
explain with pathophysiology in detail
frostbite pathophysiology treatment
FROSTBITE - Detailed Pathophysiology
Definition
Normal Cold Defense: The Hunting Response (Lewis Reaction)
- Skin cooling activates the anterior hypothalamus, triggering catecholamine release, thyroid stimulation, shivering thermogenesis, and peripheral vasoconstriction.
- Cold-induced vasoconstriction at digits reduces blood flow to as low as 10% of baseline - this is the "life vs. limb" mechanism that prioritizes core temperature over extremity perfusion.
- At ~10°C, a protective Cold-Induced Vasodilation (CIVD) - the "Hunting Reaction" - kicks in: cyclic alternation between vasoconstriction and vasodilation in 5-10 minute cycles helps protect the extremity.
- Acral structures (fingers, toes, ears, nose) are rich in arteriovenous anastomoses that shut down in extreme cold, causing drastic blood flow reduction.
- As temperature continues to fall, the hunting response eventually fails, and persistent vasoconstriction takes over.
Core Pathophysiology: Three Simultaneous Pathways
Pathway 1: Ice Crystal Formation (Direct Cellular Damage)
- Frostbite begins with extracellular ice crystal formation (at around -2°C / 28°F)
- As extracellular fluid freezes, osmotic gradients develop: water is drawn out of cells to try to re-establish osmotic equilibrium
- This causes intracellular dehydration and hyperosmolality - electrolyte concentrations rise to toxic levels
- After approximately one-third of cellular volume is lost, the cell collapses and dies - even without direct ice crystal puncture of the membrane
- With rapid freezing (>10°C/min), intracellular ice crystals can also form, physically disrupting organelles and the cytoskeleton
- Extracellular crystals also compress and damage adjacent vascular structures
Pathway 2: Microvascular Injury and Ischemia
- Prefreeze phase: even before ice forms, microvascular constriction causes endothelial plasma leakage into the interstitium
- Cold increases blood viscosity, promoting RBC sludging and microthrombus formation at the capillary level
- Vascular stasis progresses - first affecting venules, then arterioles
- Endothelial cell damage leads to prostanoid release (see below) causing further vasoconstriction
- Interstitial leakage causes tissue hypertension, further compressing vessels
- The net result: cessation of capillary flow and progressive ischemia extending into surrounding tissue
Pathway 3: Inflammatory Mediator Release
| Mediator | Effect |
|---|---|
| Thromboxane A2 (TXA2) | Potent vasoconstrictor + platelet aggregator - extends thrombosis into bordering healthy tissue |
| Prostaglandin F2α | Vasoconstriction and vascular permeability |
| Bradykinin | Increases vascular permeability, edema |
| Platelet-activating factor | Platelet and leukocyte aggregation |
| Leukocyte adhesion molecules | White cell infiltration, amplifying tissue necrosis |
The Four Pathophysiologic Stages
| Stage | Phase | Physiologic Events | Clinical Findings |
|---|---|---|---|
| I | Cooling | Cyclic vasoconstriction/vasodilation → extracellular ice crystals at -2°C → intracellular crystals if rapid freeze → erythrocyte sludging and vessel occlusion | Cool extremity, blanched, numb, hard/woody texture |
| II | Thawing & Rewarming | Ice melts, dehydrated cells swell, vessel wall integrity lost, vasodilation, inflammatory mediators peak - platelet and leukocyte aggregation causes thrombosis | Erythematous to violaceous color, intense pain, blisters form |
| III | Extension of injury | TXA2 levels increase, platelet/leukocyte aggregation extends into bordering tissue, vascular compromise widens | Blisters rupture |
| IV | Resolution | Tissue either re-epithelializes OR desiccates and mummifies; vasomotor instability may persist indefinitely | Healing or amputation required |
The Freezing Injury Cascade (Sequential)
PREFREEZE PHASE
├── Superficial tissue cooling
├── Increased viscosity of vascular contents
├── Microvascular constriction
└── Endothelial plasma leakage
FREEZE-THAW PHASE
├── Extracellular fluid → ice crystal formation
├── Water movement across cell membrane (osmotic)
├── Intracellular dehydration and hyperosmolality
├── Cell membrane denaturation/disruption
└── Cell shrinkage and collapse
VASCULAR STASIS AND PROGRESSIVE ISCHEMIA
├── Vasospasticity and stasis coagulation
├── Arteriovenous shunting
├── Endothelial cell damage + prostanoid release
├── Interstitial leakage + tissue hypertension
└── Necrosis → demarcation → mummification → slough
Clinical Degrees of Frostbite
- Only skin involved; damage is reversible
- Erythema, edema, cutaneous anesthesia, transient pain
- No bleb/blister formation
- Full recovery with only mild desquamation

- Skin + subcutaneous tissue involved
- Marked hyperemia, edema, clear-fluid blisters (bullae) within 24-36 hours of thawing
- Pain subsides to paradoxical "warmth" - a sign of severe involvement
- Skin has waxy appearance; deeper tissues remain soft
- Long-term sensory neuropathy with cold sensitivity is common
- Full-thickness dermal loss
- Hemorrhagic bulla formation (blood-filled blisters) - indicates subdermal vascular plexus destruction
- Waxy, dry, mummified skin - poor prognostic indicator
- Full-thickness necrosis: skin, muscle, tendon, and bone all involved
- Leads to amputation
- Hard, solid, completely blanched extremity

Why Rewarming Phase is Particularly Dangerous
- Thawing triggers an ischemia-reperfusion injury: when blood flow returns to ischemic tissue, free radical generation causes oxidative damage
- Inflammatory mediators (TXA2, prostaglandins) peak during rewarming - causing thrombosis to extend into bordering viable tissue
- This is why field rewarming should be avoided unless refreezing can be completely prevented - a thawed-then-refrozen extremity suffers catastrophically worse injury than one left frozen during transport
Pathophysiology of Blister Types (Diagnostic Importance)
| Blister Type | Mechanism | Prognostic Significance |
|---|---|---|
| Clear / serous bullae | Injury limited to superficial dermis, subdermal vascular plexus intact | Favorable - early appearance |
| Hemorrhagic bullae | Damage to subdermal vascular plexus, blood extravasates | Poor - indicates deeper injury |
Predisposing Pathophysiologic Factors
- Windchill and moisture accelerate the freezing rate, making frostbite far more rapid
- Vasoconstriction from nicotine (smoking) or Raynaud's phenomenon reduces baseline perfusion, increasing susceptibility
- Alcohol - causes vasodilation and impairs shivering thermogenesis
- Altitude - hypoxia + cold together increase susceptibility
- Peripheral vascular disease - impaired baseline blood flow
Summary Diagram
Cold Exposure
↓
Hypothalamic Activation → Peripheral Vasoconstriction
↓
"Hunting Reaction" (cyclic vasodilation) → eventually fails
↓
Persistent Vasoconstriction → Tissue Cooling < -2°C
↓
EXTRACELLULAR ICE CRYSTAL FORMATION
↓
Osmotic efflux of water from cells → Cellular dehydration
↓ ↓
Membrane disruption Electrolyte toxicity → Cell death
↓
Vascular stasis → Sludging → Microthrombi
↓
Endothelial damage → TXA2 + PGF2α release
↓
Platelet/leukocyte aggregation → Thrombosis extends
↓
REWARMING (Ischemia-Reperfusion + Peak mediator release)
↓
Edema, blistering (clear → hemorrhagic)
↓
Gangrene / Mummification / Amputation

is this pathophysiology right?
Stage-by-Stage Assessment
✅ Stage 1: Pre-freeze Phase — Correct in concept, incomplete
"Tissues undergo cooling but have not yet reached the point of ice crystal formation"
- Tissue cooling with increased blood viscosity
- Microvascular constriction and endothelial plasma leakage
- The "Hunting Reaction" (cyclic vasoconstriction/vasodilation) that eventually fails
⚠️ Stage 2: Freeze-thaw Phase — Partially correct, but misleading
"Ice crystals form within the tissue, causing direct cellular damage and resulting in cell death"
- Extracellular ice crystals form first (at ~-2°C) - this is the primary mechanism
- Intracellular crystals only form if freezing is very rapid (>10°C/min)
- The major cause of cell death is actually osmotic - water is drawn out of cells to maintain equilibrium with the extracellular ice, causing cellular dehydration and electrolyte toxicity, not just direct crystal puncture
- Cell collapse and death can occur after losing just one-third of cellular volume, even without direct membrane disruption by crystals
⚠️ Stage 3: Vascular Stasis Phase — Correct but incomplete
"Circulatory system fails - blood coagulation or leakage of blood out of vessels"
- RBC sludging and microthrombus formation in capillaries
- Progressive failure first in venules, then arterioles
- Endothelial damage triggers release of Thromboxane A2 (TXA2) and Prostaglandin F2α - these are the key mediators causing further vasoconstriction and platelet aggregation
- Interstitial leakage causes tissue hypertension, worsening ischemia
⚠️ Stage 4: Late Ischemic Phase — Correct but the name/framing is non-standard
"Inflammatory events and ischemia leading to ultimate tissue death"
- Standard textbook classification (Dermatology 2-Volume Set, Rosen's EM) calls this the "Resolution Phase" - where tissue either re-epithelializes or mummifies/undergoes gangrene
- The "flames" visual nicely represents the ischemia-reperfusion injury that occurs during rewarming - free radical generation and peak inflammatory mediator release that can extend necrosis beyond the originally frozen zone
- This stage is also where TXA2 peaks during rewarming, explaining why repeat freeze-thaw cycles are catastrophically destructive
Summary Table
| Stage in Diagram | Accuracy | Key Gap/Error |
|---|---|---|
| Stage 1: Pre-freeze | ✅ Correct | Missing hunting reaction and AV anastomosis shutdown |
| Stage 2: Freeze-thaw | ⚠️ Misleading | Overemphasizes direct ice crystal damage; osmotic cell death (the real killer) is omitted |
| Stage 3: Vascular stasis | ⚠️ Incomplete | Missing TXA2/prostaglandins - the most therapeutically important mediators |
| Stage 4: Late ischemic | ✅ Correct | Non-standard naming; rewarming reperfusion injury not explicitly explained |
One Major Additional Omission
as u corrected the image data, can u make the same with with your correction?
A detailed medical infographic titled "The Four Stages of Frostbite Pathophysiology (Corrected)" in a wide horizontal format. Clean, professional medical illustration style with a cool blue-to-dark gradient background. Four clearly labeled stages shown left to right with connecting arrows, each with an anatomical cross-section illustration and detailed bullet points below. Stage 1 - "Pre-freeze Phase": Show a tissue cross-section with normal blood vessels. Label shows: cyclic vasoconstriction and vasodilation (Hunting Reaction of Lewis), AV anastomosis shutdown, increased blood viscosity, endothelial plasma leakage into interstitium. Skin appears pale and cool. Stage 2 - "Freeze-Thaw Phase": Show ice crystals forming OUTSIDE cells (extracellular), water arrows moving OUT of cells (osmotic efflux). Label shows: extracellular ice crystals form first at -2 degrees C, osmotic water efflux from cells, intracellular dehydration and hyperosmolality (main killer), cell membrane denaturation, cell collapse after losing 1/3 volume. Note: intracellular crystals only with rapid freeze greater than 10 C/min. Stage 3 - "Vascular Stasis Phase": Show clogged vessels with red blood cell sludging, microthrombi, leaking vessel walls. Label shows: RBC sludging and microthrombus formation, TXA2 (thromboxane A2) and PGF2-alpha release from damaged endothelium, platelet and leukocyte aggregation extends into bordering tissue, interstitial tissue hypertension worsens ischemia. Stage 4 - "Late Ischemic / Resolution Phase": Show a necrotic dark hand with flames indicating reperfusion injury and inflammation. Label shows: ischemia-reperfusion injury during rewarming, free radical generation, TXA2 peaks at rewarming, tissue either re-epithelializes or mummifies, repeat freeze-thaw cycles are catastrophic. Bottom note: "These 3 pathways occur SIMULTANEOUSLY and reinforce each other - not purely sequential." Color coded: Stage 1 blue, Stage 2 light blue/white, Stage 3 purple/red, Stage 4 dark red/black. Medical textbook quality.
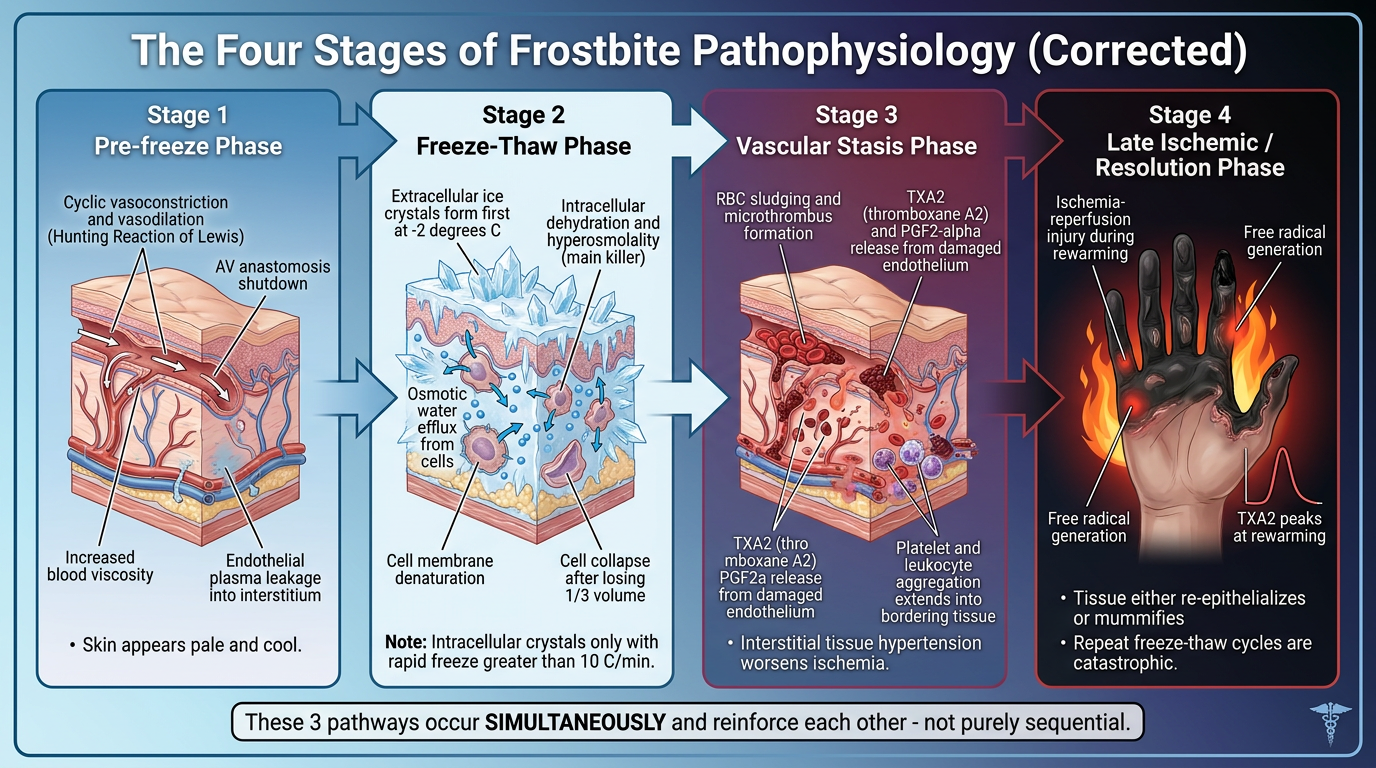
Key Corrections Made
| Original (Wrong/Incomplete) | Corrected Version |
|---|---|
| Stage 2 implied ice crystals form inside cells | Clarified that extracellular crystals form first; intracellular only with rapid freeze >10°C/min |
| Cell death attributed only to "direct crystal damage" | Added the dominant mechanism: osmotic water efflux → cellular dehydration → electrolyte toxicity → cell collapse |
| Stage 3 described only as "blood coagulation or leakage" | Added TXA2 and PGF2α (the key mediators driving vasoconstriction + platelet aggregation into bordering tissue) |
| Stage 4 labeled "Late Ischemic Phase" | Renamed to "Late Ischemic / Resolution Phase" and added ischemia-reperfusion injury during rewarming as the major mechanism |
| Stages shown as strictly sequential | Added the critical note that all 3 pathways occur simultaneously and reinforce each other |
| Missing the Hunting Reaction | Stage 1 now includes the Lewis Hunting Response (cyclic vasoconstriction/vasodilation) and AV anastomosis shutdown |
can you make another image with same information & keep a whole extremity to demonstrate like the image i have uploaded?
A detailed medical infographic titled "The Four Stages of Frostbite Pathophysiology" in wide horizontal format (landscape). Professional medical illustration style with a clean light blue-grey gradient background. The CENTRAL VISUAL is a single whole human arm and hand running horizontally across the middle of the image, from shoulder on the left to fingertips on the right. The arm is divided into 4 color-coded zones from left to right, each zone corresponding to one stage: - Zone 1 (shoulder to mid-forearm): Normal pink skin tone, healthy - Zone 2 (mid-forearm): Pale/waxy white skin, frost crystals forming on surface - Zone 3 (wrist area): Mottled purple-red skin, visible swollen vessels, early blisters - Zone 4 (hand and fingers): Dark grey-black necrotic fingers, flames around fingertips indicating reperfusion inflammation, mummified appearance Above each zone, a callout box with title and bullet points: STAGE 1 - PRE-FREEZE PHASE (blue callout, above shoulder/upper arm): • Hunting Reaction of Lewis: cyclic vasoconstriction & vasodilation • AV anastomosis shutdown — life-vs-limb response • Increased blood viscosity • Endothelial plasma leakage into interstitium • Skin: pale, cool, numb STAGE 2 - FREEZE-THAW PHASE (light blue/white callout, above mid-forearm): • Extracellular ice crystals form first (at −2°C) • Osmotic water efflux OUT of cells → intracellular dehydration • Hyperosmolality = primary cell killer (not direct crystal puncture) • Cell collapses after losing 1/3 volume • Intracellular crystals only if freeze rate >10°C/min STAGE 3 - VASCULAR STASIS PHASE (purple callout, above wrist): • RBC sludging → microthrombus formation • Endothelial damage → TXA2 + PGF2α release • Platelet & leukocyte aggregation extends into bordering tissue • Interstitial edema → tissue hypertension → more ischemia • Hemorrhagic blisters = subdermal vascular plexus destruction STAGE 4 - LATE ISCHEMIC / RESOLUTION PHASE (dark red callout, above hand): • Ischemia-reperfusion injury during rewarming • Free radical burst + TXA2 peaks at thawing • Repeat freeze-thaw cycles are catastrophic • Tissue: re-epithelializes OR mummifies/gangrenous • Amputation may be required Below the arm, a bold warning banner: "⚠ All 3 mechanisms — ice crystal injury, vasoconstriction/ischemia, and inflammatory mediators — occur SIMULTANEOUSLY and reinforce each other." Arrows between zones show disease progression. Small microscopic inset circles near each zone show cellular-level changes: Zone 1 = normal cells with vessels, Zone 2 = extracellular ice crystals with water arrows leaving cells, Zone 3 = clogged vessel with sludged RBCs and TXA2 label, Zone 4 = necrotic black cells. Medical textbook illustration quality, clean typography, color-coded stages.
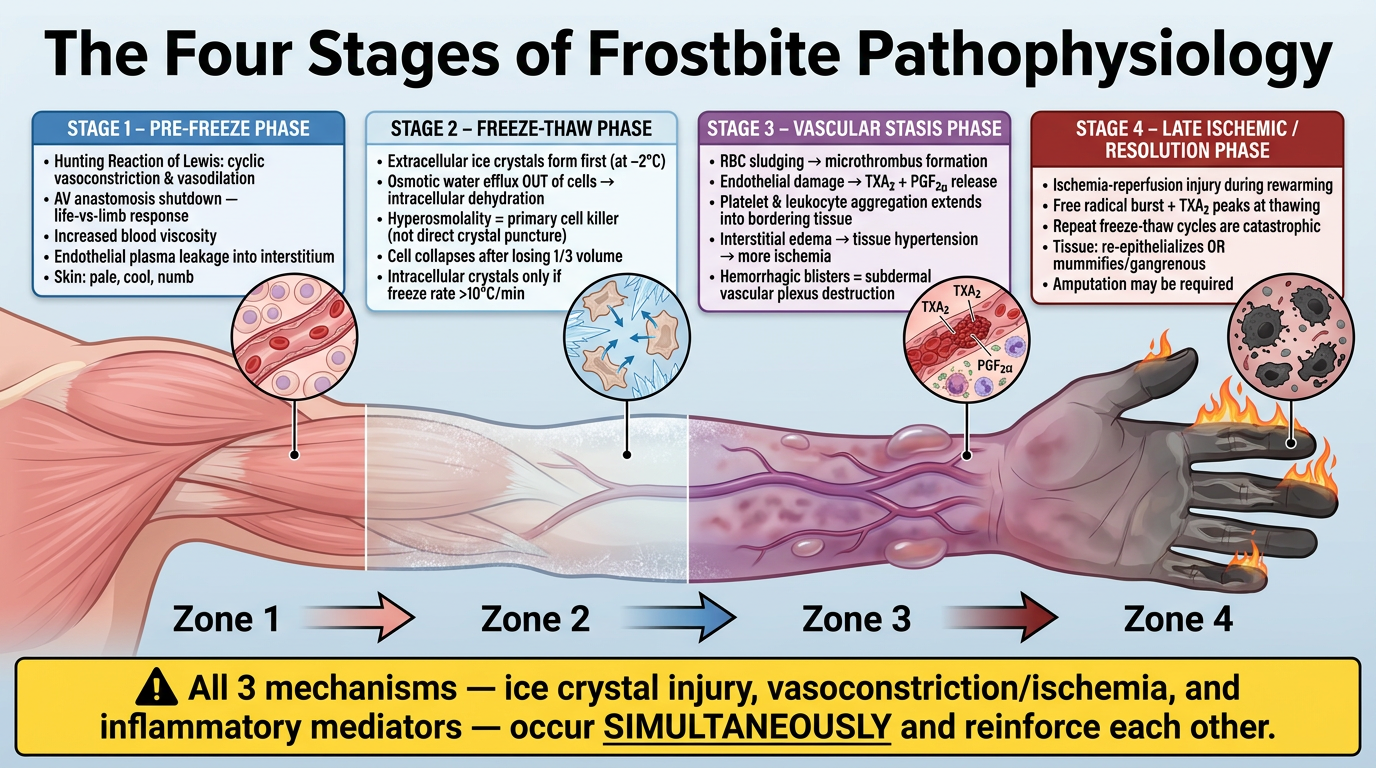
- 4 color-coded callout boxes above each arm zone with the corrected bullet points
- Microscopic inset circles showing cellular-level changes per stage (extracellular ice, osmotic water efflux, RBC sludging with TXA2 label, necrotic cells)
- Flames at the fingertips representing reperfusion injury during rewarming
- Warning banner at the bottom emphasizing that all 3 mechanisms are simultaneous, not sequential - the biggest correction from your original diagram
why osmotic gradient changes after Extracellular ice crystals formation?
Why Extracellular Ice Formation Changes the Osmotic Gradient
The Core Principle: Ice Excludes Solutes
Extracellular fluid (water + solutes)
↓ freezing
Ice crystal (pure H₂O) + concentrated solute residue
Step-by-Step Mechanism
- Intracellular osmolarity ≈ 300 mOsm/L
- Extracellular osmolarity ≈ 300 mOsm/L
- System is in osmotic equilibrium → no net water movement
| Compartment | What happens | Result |
|---|---|---|
| Extracellular | Water molecules are locked into ice crystals | Remaining liquid becomes hyperosmolar (e.g. 400, 500, 600+ mOsm/L) |
| Intracellular | Solutes unchanged, water still liquid | Remains ~300 mOsm/L |
Extracellular osmolarity >> Intracellular osmolarity
The Osmotic Response: Water Leaves the Cell
CELL (300 mOsm) ──water exits──→ Extracellular ice zone (500+ mOsm)
- Further concentrates extracellular solutes even more
- Drives even more water out of the cell
- Creates a self-amplifying cycle
What This Does to the Cell
- Cell shrinks and dehydrates - the cytoplasm becomes concentrated
- Intracellular electrolytes rise to toxic levels - especially Na⁺, Ca²⁺, H⁺ - disrupting enzyme function and membrane potentials
- Proteins denature - high ionic strength unfolds proteins
- Cell membrane buckles - the lipid bilayer loses structural integrity under physical stress of shrinkage
- Cell death occurs after losing approximately one-third of its volume - even if no ice crystal ever physically pierced the membrane
Analogy to Make It Intuitive
When seawater freezes, the ice is nearly fresh water - the salt is expelled into the remaining liquid. The ocean water under Arctic ice is therefore saltier and denser than normal seawater. The same principle applies at the cellular level - freezing the extracellular fluid "salts out" the remaining liquid, drawing water out of nearby cells by osmosis.
Why This Matters Clinically
| Freeze Rate | Ice Formation | Osmotic Injury | Net Result |
|---|---|---|---|
| Slow (e.g. frostbite) | Extracellular only → solute concentration → prolonged osmotic stress | Severe - cells dehydrate progressively | Osmotic cell death |
| Ultra-rapid (e.g. cryopreservation with liquid nitrogen) | Intracellular water vitrifies (glass state) before it can exit | Minimal osmotic time | Less solution-effect injury (but mechanical crystal damage instead) |
Remaining liquid becomes hyperosmolar menas?
What "Remaining Liquid Becomes Hyperosmolar" Means
Start with a Simple Example
10 molecules of water + 2 molecules of salt
Osmolarity = 2 salt / 10 water = 0.2 (relatively low)
ICE (5 water molecules, zero salt)
+
REMAINING LIQUID (5 water molecules + 2 salt molecules still)
Osmolarity = 2 salt / 5 water = 0.4 (DOUBLED!)
The Word Itself
| Term | Meaning |
|---|---|
| Osmolar | related to osmolarity = concentration of solute particles per liter of solution |
| Hyper- | above normal / higher than |
| Hyperosmolar | more concentrated than normal (more solute particles per unit of water than the reference point) |
- 350 mOsm/L → mildly hyperosmolar
- 500 mOsm/L → severely hyperosmolar
- 600+ mOsm/L → lethal to nearby cells
Visualized at the Cellular Level
BEFORE FREEZING:
┌─────────────────────────────────┐
│ Extracellular fluid │
│ 🧂🧂 💧💧💧💧💧💧💧💧 │ ← 300 mOsm (normal)
│ (2 solute, 8 water) │
└─────────────────────────────────┘
AFTER EXTRACELLULAR ICE FORMS:
┌──────────────┐ ┌──────────────┐
│ ICE crystal │ │ Remaining │
│ 💧💧💧💧 │ │ liquid │
│ (pure H₂O) │ │ 🧂🧂 💧💧💧💧 │ ← 500 mOsm (HYPEROSMOLAR)
│ no solutes │ │(2 solute, │
└──────────────┘ │ 4 water) │
└──────────────┘
Why This Pulls Water Out of the Cell
CELL (300 mOsm) ──── water rushes out ────→ Extracellular (500 mOsm)
↓
Cell shrinks, dehydrates, intracellular solutes rise
↓
Cell dies
One-Line Summary
Hyperosmolar = too many solute particles per unit of water. When extracellular water freezes into ice, the solutes that can't enter the ice get left behind in less water, making that remaining liquid abnormally concentrated - which then sucks water out of adjacent cells by osmosis.
The "blood leakage" shown refers to this interstitial plasma/RBC extravasation leading to edema and eventually hemorrhagic blisters. why the blood is leaking?
Why Does Blood Leak Out of Vessels in Frostbite?
Normal Vessel Wall — Quick Recap
- Endothelial cells tightly joined together by proteins called tight junctions and adherens junctions
- These junctions act like a sealed wall — water, large proteins, and RBCs cannot pass through
- Only small molecules (O₂, CO₂, nutrients) cross normally
NORMAL:
Blood inside vessel | Endothelial cell wall (sealed) | Tissue outside
RBCs, plasma | ████████████████████████████ | (dry, no blood)
proteins stay inside | tight junctions intact |
Reason 1: Direct Endothelial Cell Damage by Ice Crystals
- Extracellular ice crystals form inside the vessel wall tissue and surrounding the endothelial cells
- The same osmotic mechanism that kills other cells also dehydrates and kills endothelial cells
- Dead or injured endothelial cells shrink and pull apart from each other
- The tight junctions between them break open - creating physical gaps in the vessel wall
ICE CRYSTALS FORM HERE:
↓↓↓
████ GAP ████ GAP ████ ← endothelial cells separating
↑↑↑
Blood leaks through gaps
Reason 2: Inflammatory Mediators Directly Destroy Tight Junctions
- They activate phospholipase inside endothelial cells
- This triggers actin-myosin contraction within the endothelial cell cytoskeleton
- The cell physically contracts and rounds up - like a fist clenching
- This pulls the cell body away from its neighbors, ripping tight junctions apart
- Directly bind receptors on endothelial cells
- Cause the same cytoskeletal contraction
- Open intercellular gaps within seconds to minutes
Normal endothelial cell: Inflamed endothelial cell:
┌──────────────┐ ┌────┐ ┌────┐
│ flat, spread│ │ │ GAP │ │
│ tight fit │ → │ │◄────►│ │
│ no gaps │ │ │ │ │
└──────────────┘ └────┘ └────┘
Actin contracts → cell rounds up → gap opens
Reason 3: Ischemia Weakens the Endothelial Cell Barrier
- Vasoconstriction cuts off blood supply to the vessel wall itself (vessels have their own tiny feeding vessels - vasa vasorum)
- Hypoxia causes ATP depletion inside endothelial cells
- Without ATP:
- Ion pumps (Na⁺/K⁺ ATPase) fail → cells swell
- Cytoskeletal proteins can't be maintained
- Tight junction proteins (occludin, claudins, ZO-1) degrade
- Swollen, ATP-depleted cells lose their architecture and barrier function collapses
Reason 4: Reperfusion - The Burst That Breaks the Dam
- A sudden burst of reactive oxygen species (ROS) / free radicals is generated
- ROS directly oxidize and degrade tight junction proteins
- They also activate matrix metalloproteinases (MMPs) - enzymes that digest the basement membrane under the endothelial cells
- Without the basement membrane anchor, cells detach and the vessel wall literally falls apart
What Leaks Out and Why It Matters
| What leaks | Why it happens | Clinical result |
|---|---|---|
| Plasma (water + proteins) | Small gap openings, hydrostatic pressure pushes fluid out | Edema - swelling of tissue |
| RBCs | Larger gap openings when damage is severe | Hemorrhagic (blood-filled) blisters |
| Platelets | Leak out and activate in the interstitium | Worsen clotting and mediator release |
Why Clear Blisters vs. Hemorrhagic Blisters?
SUPERFICIAL INJURY (2nd degree):
Small gaps → only plasma (water + proteins) leaks
→ CLEAR / SEROUS blisters
Subdermal vascular plexus INTACT
DEEP INJURY (3rd/4th degree):
Large gaps + basement membrane destruction → RBCs also leak
→ HEMORRHAGIC (blood-filled) blisters
Subdermal vascular plexus DESTROYED
→ Poor prognosis
Summary in One Flow
Cold → Ice crystals form in vessel wall
↓
Endothelial cells dehydrate + die → tight junctions break
+
TXA2/Bradykinin/Histamine → actin contraction → gaps open
+
Hypoxia → ATP depletion → barrier proteins degrade
+
Reperfusion → ROS burst → basement membrane digested
↓
VESSEL WALL INTEGRITY LOST
↓
Plasma leaks → Edema + Clear blisters
RBCs leak → Hemorrhagic blisters (= deep injury marker)
Extracellular ice crystals form inside the vessel wall tissue?
What "Extracellular" Actually Means
VESSEL WALL CROSS-SECTION:
│ Blood │ Endothelial │←Basement→│ Smooth muscle │ Adventitia │
│inside │ cells │ membrane │ cells │ (outside) │
│ │ ┌──┐ ┌──┐ │ │ ┌──┐ ┌──┐ │ │
│ │ │EC│~~~│EC│ │ │ │SM│~~~~│SM│ │ │
│ │ └──┘ └──┘ │ │ └──┘ └──┘ │ │
│ │ ↑ │ ↑ │ │
│ │ ECF here │ ECF here │ │
│ │ (between │ (between │ │
│ │ cells) │ cells) │ │
So Where Exactly Does the Ice Form?
Location 1: Interstitial space of the vessel wall itself
- Ice crystals nucleate in the interstitial spaces between endothelial cells
- Also between smooth muscle cells in the tunica media
- The crystals grow in these spaces, physically pushing cells apart
Location 2: The interstitium surrounding the vessel (perivascular space)
Tissue outside vessel:
Fibroblast [Ice crystal] Collagen fiber
↑ ↑
[Ice crystal] Endothelial cell (vessel wall) [Ice crystal]
Ice forms in ALL the fluid spaces surrounding the vessel
→ compresses the vessel from outside
Location 3: Inside the blood (intravascular)
- Plasma water can begin to freeze inside the vessel lumen
- This is called intravascular ice formation
- It directly causes RBC sludging because ice crystals mechanically trap and aggregate red blood cells
The Key Distinction - "Extracellular" is a Compartment, Not a Location
| Term | Meaning | Where physically |
|---|---|---|
| Intracellular | Inside the cell membrane | Inside any cell - endothelial, muscle, skin, RBC |
| Extracellular | Outside cell membranes | The fluid-filled gaps between cells - everywhere in the tissue |
| Intravascular | Inside the blood vessel lumen | Inside the tube itself, where blood flows |
Ice forms in the fluid-filled spaces between the cells that make up the vessel wall - not inside those cells, and not (initially) inside the blood vessel lumen.
Visual Summary
BEFORE FREEZING (vessel wall, zoomed in):
┌─────┐ fluid ┌─────┐ fluid ┌─────┐
│ EC │ ~~~~~ │ EC │ ~~~~~ │ EC │
│cell │ │cell │ │cell │
└─────┘ └─────┘ └─────┘
Tight junctions connecting them, fluid between them
AFTER EXTRACELLULAR FREEZING:
┌─────┐ ❄ICE❄ ┌─────┐ ❄ICE❄ ┌─────┐
│ EC │ │ EC │ │ EC │
│cell │◄pushed► │cell │◄pushed► │cell │
└─────┘ apart └─────┘ apart └─────┘
Ice in the spaces physically pushes cells apart
+ osmotic dehydration shrinks each cell
= tight junctions torn open = vessel leaks
One-Line Answer
free radical generation?
What is a Free Radical?
Normal molecule: ●● ●● ●● (all electrons paired, stable)
Free radical: ●● ●● ● (one unpaired, UNSTABLE → attacks neighbors)
Where Do Free Radicals Come From in Frostbite?
Step 1: During Ischemia (while tissue is frozen/no blood flow)
- Oxygen runs out → cells switch to anaerobic metabolism
- ATP falls → the enzyme xanthine dehydrogenase (XDH) gets converted to a different form: xanthine oxidase (XO)
- This conversion is driven by calcium flooding into cells (because ATP-dependent calcium pumps fail)
- Xanthine oxidase accumulates silently during ischemia, waiting
During ischemia, two things build up quietly:
1. Xanthine oxidase enzyme (XO) ← the loaded gun
2. Hypoxanthine substrate ← the ammunition
Step 2: Reperfusion - Oxygen Returns (thawing, blood flow resumes)
Hypoxanthine + O₂ + Xanthine Oxidase
↓
Xanthine + O₂•⁻ (superoxide radical) + H₂O₂
The Free Radical Cascade
O₂•⁻ (superoxide)
↓ superoxide dismutase (SOD)
H₂O₂ (hydrogen peroxide) ← not a radical but still reactive
↓ + Fe²⁺ (Fenton reaction)
•OH (hydroxyl radical) ← THE MOST DANGEROUS
↓
Attacks everything nearby
The Fenton Reaction (key step)
Fe²⁺ + H₂O₂ → Fe³⁺ + •OH + OH⁻
What Do Free Radicals Attack?
1. Cell Membranes - Lipid Peroxidation
•OH attacks membrane phospholipid (has double bonds)
↓
Lipid radical formed → steals from next lipid
↓
Chain reaction through the entire membrane
↓
Membrane loses integrity → cell lyses
2. Proteins - Oxidation
- Enzyme active sites oxidized → enzymes stop working
- Structural proteins (collagen, actin) cross-link and stiffen
- Tight junction proteins (occludin, claudins) oxidized and degraded → vessel leaks
3. DNA - Strand Breaks
- •OH directly attacks DNA bases
- Single and double strand breaks
- If not repaired → cell death (apoptosis or necrosis)
4. Mitochondria
- ROS attack the mitochondrial membrane
- This releases cytochrome C into the cytoplasm
- Cytochrome C triggers apoptosis (programmed cell death)
Why is This Worse Than the Original Injury?
- The burst is massive - weeks of XO and hypoxanthine release all at once
- The chain reaction amplifies damage far beyond the original frozen zone
- Normal antioxidant defenses (glutathione, catalase, SOD) are already depleted by ischemia and cannot cope
The Antioxidant Defense That Fails
| Antioxidant | What it does |
|---|---|
| Superoxide dismutase (SOD) | Converts O₂•⁻ → H₂O₂ (less reactive) |
| Catalase | Converts H₂O₂ → H₂O + O₂ (harmless) |
| Glutathione peroxidase | Neutralizes H₂O₂ and lipid peroxides |
| Vitamin C, E | Donate electrons to quench radicals |
Summary Flow
ISCHEMIA (frozen tissue):
ATP depletion → Ca²⁺ floods in → XDH converts to XO
Anaerobic metabolism → Hypoxanthine accumulates
(XO + Hypoxanthine sit loaded, waiting for O₂)
REPERFUSION (thawing, blood returns):
O₂ arrives → XO + Hypoxanthine → Superoxide burst (O₂•⁻)
↓
H₂O₂ formed
↓ + Fe²⁺ (Fenton)
•OH (hydroxyl radical) — most destructive
↓
Lipid peroxidation → membrane destruction
Protein oxidation → tight junctions fail → vessel leaks
DNA damage → apoptosis
Mitochondrial damage → more cell death
↓
Tissue necrosis EXTENDS BEYOND originally frozen zone
Can you please simplify stage 4?
Stage 4 - Late Ischemic / Resolution Phase (Simplified)
What's happening at this point?
Thing 1: The Damage Gets Worse When Blood Comes Back
During the frozen period, the cells were starving (no oxygen, no blood). They built up toxic waste products. The moment blood rushes back in with oxygen, those waste products react with the oxygen and produce free radicals - basically chemical fire inside the tissue.
Frozen (no blood) → cells damaged but some still alive
↓
Blood returns → chemical fire (free radicals) kills the rest
↓
MORE tissue dies than the cold alone caused
Thing 2: The Inflammatory System Overreacts
- More TXA2 released → more blood vessel constriction → less blood to the already struggling tissue
- Swelling worsens
- The border between dead and living tissue slowly becomes clearer
The Two Possible Outcomes
Stage 4 ends one of two ways:
MILD/MODERATE DAMAGE SEVERE DAMAGE
↓ ↓
Tissue heals Tissue turns black
Re-grows skin Dries out and shrinks
(re-epithelialization) (mummification)
↓
Amputation needed
One Simple Analogy
Think of Stage 4 like a house fire that's been put out. The fire (freezing) caused damage - but when the firefighters flood the building with water (reperfusion), some remaining structural parts that survived the fire collapse from the water damage. The final state of the building depends on how much was damaged total - either it can be repaired, or it has to be demolished.
Key Takeaway
can u create a small image to fit in above mentioned pathophysiology?
A compact, clean medical diagram for Stage 4 of frostbite pathophysiology titled "Stage 4: Late Ischemic / Resolution Phase". Square format, white background, professional medical illustration style. Left half shows: A blood vessel with red arrows indicating blood rushing back in (labeled "Reperfusion - blood returns"), inside the vessel sparks and orange chemical symbols representing free radicals (labeled "Free radical burst - chemical fire"), surrounding tissue cells turning dark/dying. Center shows a bold downward arrow labeled "Two outcomes" Right half splits into two boxes: TOP BOX (green border): Shows pink healthy regenerating skin cells with label "Healing - re-epithelialization" with a small checkmark BOTTOM BOX (dark red/black border): Shows black dried mummified fingers/tissue labeled "Mummification → Gangrene → Amputation" with a warning symbol Small text at bottom: "Reperfusion damage often worse than original freeze" Clean, minimal, easy to read, suitable as a small inline teaching image.
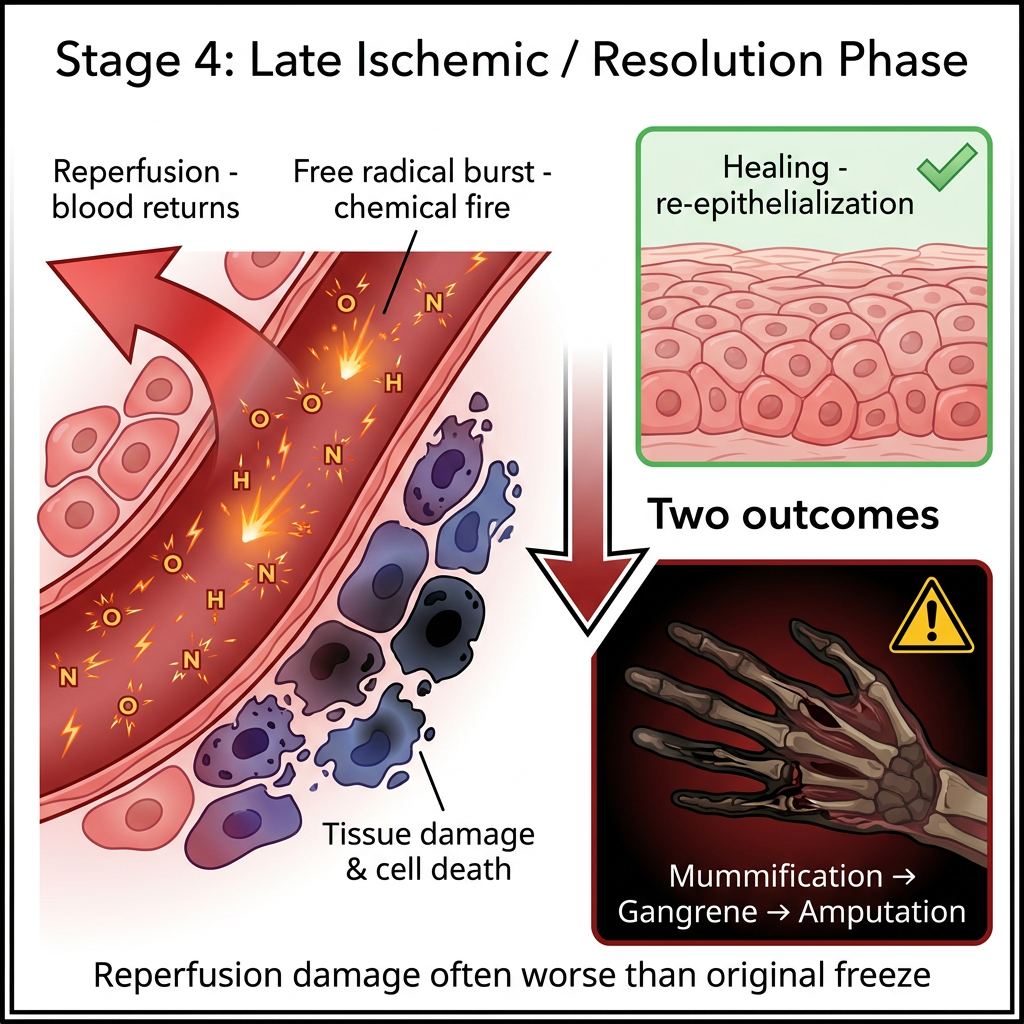
- Left - Blood rushing back into the vessel (reperfusion) triggering the free radical burst
- Center - The two-outcome split arrow
- Top right - Green box showing healing/re-epithelialization (good outcome)
- Bottom right - Dark box showing mummification → gangrene → amputation (bad outcome)
- Bottom note - The key teaching point that reperfusion damage often exceeds the original freeze injury