Extrapyramidal pathway functions
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of extrapyramidal pathway functions drawn from multiple authoritative textbooks:
Extrapyramidal Pathway - Functions
Definition and Scope
The term "extrapyramidal" refers to all descending motor pathways other than the corticospinal (pyramidal) tract - i.e., every tract that does NOT pass through the medullary pyramids. This includes both the brainstem tracts (bulbospinal system) and the basal ganglia circuits that modulate cortical motor output.
- Harrison's Principles of Internal Medicine, 22E: "The bulbospinal system is sometimes referred to as the extrapyramidal upper motor neuron system."
- Costanzo Physiology, 7th Ed: "Pyramidal tracts are corticospinal and corticobulbar tracts... All others are extrapyramidal tracts."
Core Functions of the Extrapyramidal System
| Function | Details |
|---|---|
| Muscle tone regulation | Adjusts background tone in postural muscles |
| Postural control | Maintains body position against gravity |
| Automatic/involuntary movement | Controls habitual, reflexive, and automatic motor acts |
| Modulating voluntary movement | Influences the automatic component of skilled voluntary movement |
| Axial and proximal limb control | Most tracts target trunk and girdle muscles |
Lesions of the extrapyramidal system cause involuntary movements, changes in muscle tone, and slowness of movement - contrasting with pyramidal lesions which cause spasticity and paralysis (Kaplan & Sadock's Comprehensive Textbook of Psychiatry).
The Individual Extrapyramidal Tracts
All of these originate in the brainstem, not the cortex directly:
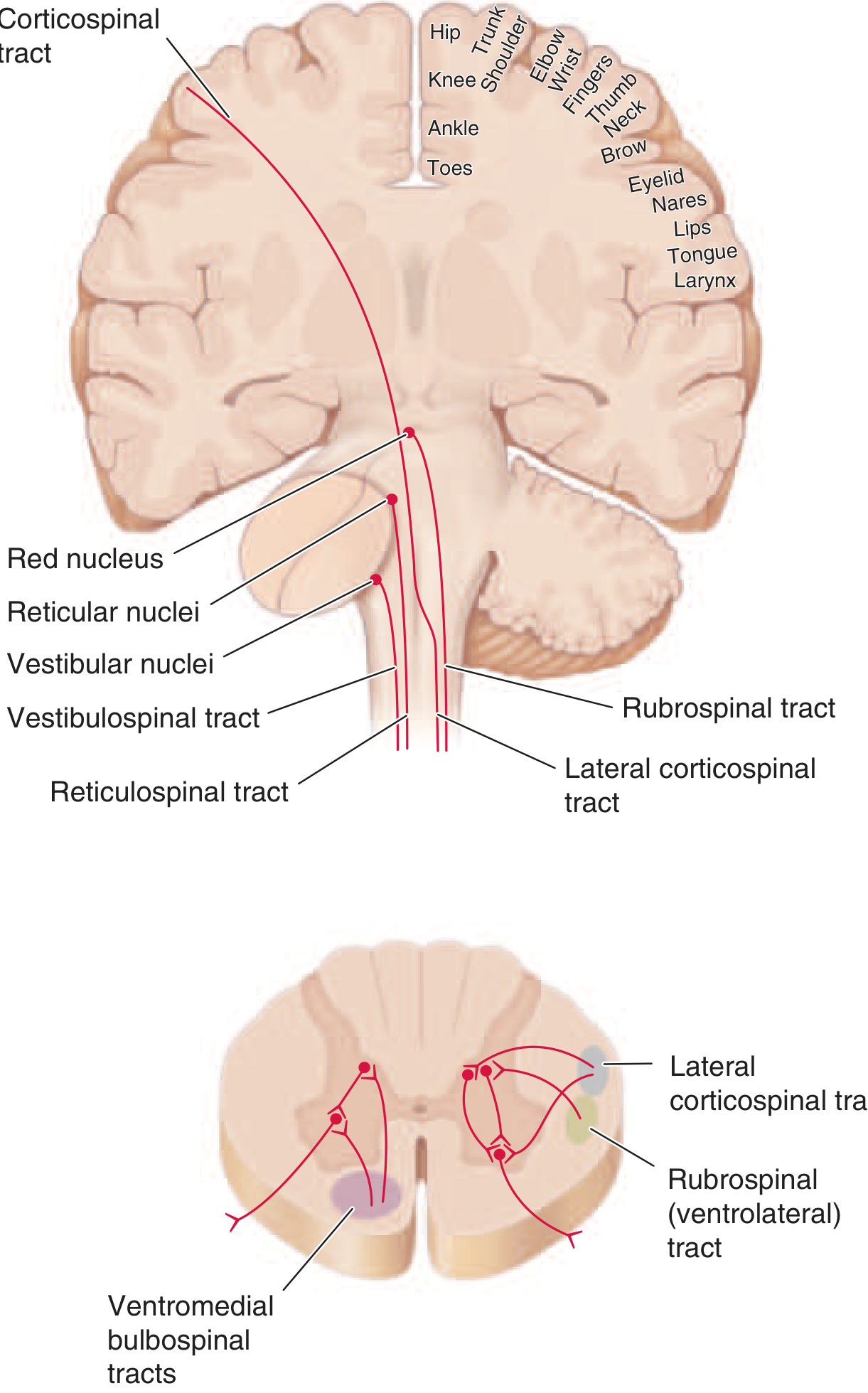
1. Rubrospinal Tract
- Origin: Red nucleus (midbrain tegmentum)
- Projection: Lateral spinal cord, contralateral
- Function: Activates flexor muscles, inhibits extensors; facilitates distal limb movements
- Classified as a ventrolateral bulbospinal pathway
2. Pontine Reticulospinal Tract
- Origin: Pontine reticular formation
- Projection: Ventromedial spinal cord
- Function: Generalized activating effect on both flexors and extensors; predominantly excites extensors - important for upright posture
3. Medullary Reticulospinal Tract
- Origin: Medullary reticular formation
- Projection: Spinal cord
- Function: Generalized inhibitory effect, predominantly on extensors; modulates tone and reflexes
4. Lateral Vestibulospinal Tract
- Origin: Lateral vestibular nucleus (Deiters nucleus)
- Projection: Ipsilateral motoneurons throughout the cord
- Function: Activates extensors, inhibits flexors - critical for gravitational posture and balance
5. Tectospinal Tract
- Origin: Superior colliculus (midbrain tectum)
- Projection: Cervical spinal cord only
- Function: Controls neck muscle movements in response to visual stimuli; coordinates head-eye orientation
Clinical note: The pontine reticular formation and lateral vestibular nucleus both powerfully excite extensor muscles. Lesions above these structures (but below the midbrain) release their activity, producing decerebrate rigidity (dramatic extensor hypertonicity). - Costanzo Physiology, 7th Ed
The Basal Ganglia Component
The basal ganglia are the other major extrapyramidal component. They operate via five parallel cortico-striato-thalamo-cortical loops:
| Loop | Striatal Input | Terminal Cortex | Function |
|---|---|---|---|
| Sensorimotor | Motor cortex | Putamen → Premotor/SMA/Motor cortex | Movement control |
| Associative | Frontal/parietal cortex | Dorsal caudate → Prefrontal cortex | Cognition |
| Limbic | Hippocampus/amygdala/cingulate | Ventral striatum → Anterior cingulate/orbitofrontal | Emotion, motivation |
| Oculomotor | Frontal eye fields | Caudate → FEF | Eye movements |
| Lateral orbitofrontal | Orbitofrontal cortex | Caudate → Orbitofrontal | Behavioral flexibility |
(Bradley and Daroff's Neurology in Clinical Practice)
Direct vs. Indirect Pathway
The basal ganglia regulate movement through two opposing pathways:
Direct pathway (movement-promoting):
- Cortex → Striatum (D1 receptors, substance P) → GPi/SNr (inhibited) → Thalamus (disinhibited) → Motor cortex (excited)
- Net result: facilitates ongoing motor activity
Indirect pathway (movement-suppressing):
- Cortex → Striatum (D2 receptors, enkephalin) → GPe (inhibited) → STN (disinhibited) → GPi/SNr (excited) → Thalamus (inhibited) → Motor cortex (suppressed)
- Net result: suppresses competing or unwanted movements
Dopamine from the substantia nigra pars compacta (SNc) facilitates the direct pathway (via D1 receptors) and inhibits the indirect pathway (via D2 receptors) - thus dopamine acts as a net motor facilitator. Loss of dopaminergic neurons (as in Parkinson disease) tips the balance toward the indirect pathway, producing hypokinesia, rigidity, and tremor.
(Eric Kandel - Principles of Neural Science, 6th Ed; Bradley and Daroff's Neurology)
Summary: Pyramidal vs. Extrapyramidal Comparison
| Feature | Pyramidal | Extrapyramidal |
|---|---|---|
| Main tract | Corticospinal | Rubrospinal, reticulospinal, vestibulospinal, tectospinal |
| Passes through medullary pyramids | Yes | No |
| Primary target muscles | Distal limb (fine movement) | Axial, proximal (posture, tone) |
| Type of movement | Voluntary, precise, skilled | Automatic, postural, background |
| Lesion effects | Spasticity, paralysis, Babinski sign | Rigidity/hypotonia, involuntary movements (tremor, chorea, athetosis), bradykinesia |
The division is now understood to be not absolute - the pyramidal and extrapyramidal systems are extensively interconnected, and the basal ganglia influence motor output through the cortex, which then acts via the corticospinal tract. The cerebellum adds a third layer of motor regulation, controlling synergy, timing, and force of movement.
- Costanzo Physiology, 7th Ed | Bradley and Daroff's Neurology | Harrison's Principles of Internal Medicine, 22E | Eric Kandel - Principles of Neural Science, 6th Ed | Kaplan & Sadock's Comprehensive Textbook of Psychiatry
How do hepatic excretion ratio calculated
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Excellent sources found. Here is the complete answer:
Hepatic Extraction Ratio (E) - How It Is Calculated
Core Definition
The hepatic extraction ratio (E) is the fraction of drug removed from the blood in a single pass through the liver. It is a dimensionless number ranging from 0 to 1 (or 0% to 100%).
Primary Formula (Direct Measurement)
$$E = \frac{C_a - C_v}{C_a}$$
| Variable | Meaning |
|---|---|
| C_a | Drug concentration in arterial/portal venous blood entering the liver (mixed hepatic arterial + portal venous inflow) |
| C_v | Drug concentration in hepatic venous blood leaving the liver |
This is the most direct experimental calculation - you measure what goes in and what comes out.
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
- Tietz Textbook of Laboratory Medicine, 7th Ed: E = C_a / C_e (same formula, different notation)
Derived from Clearance (Calculated Formula)
When you have clearance data instead of blood concentration measurements:
$$E = \frac{Cl_H}{Q}$$
Where:
- Cl_H = hepatic blood clearance (L/h or L/min)
- Q = hepatic blood flow (~1.5 L/min or ~90 L/h in a 70 kg person)
Example - Morphine:
- Morphine blood clearance = 50 L/h/70 kg
- Hepatic blood flow = 90 L/h/70 kg
- ER = 50/90 = 0.67 (high extraction)
- Therefore oral bioavailability ≈ 1 - 0.67 = ~33%
(Katzung's Basic and Clinical Pharmacology, 16th Ed)
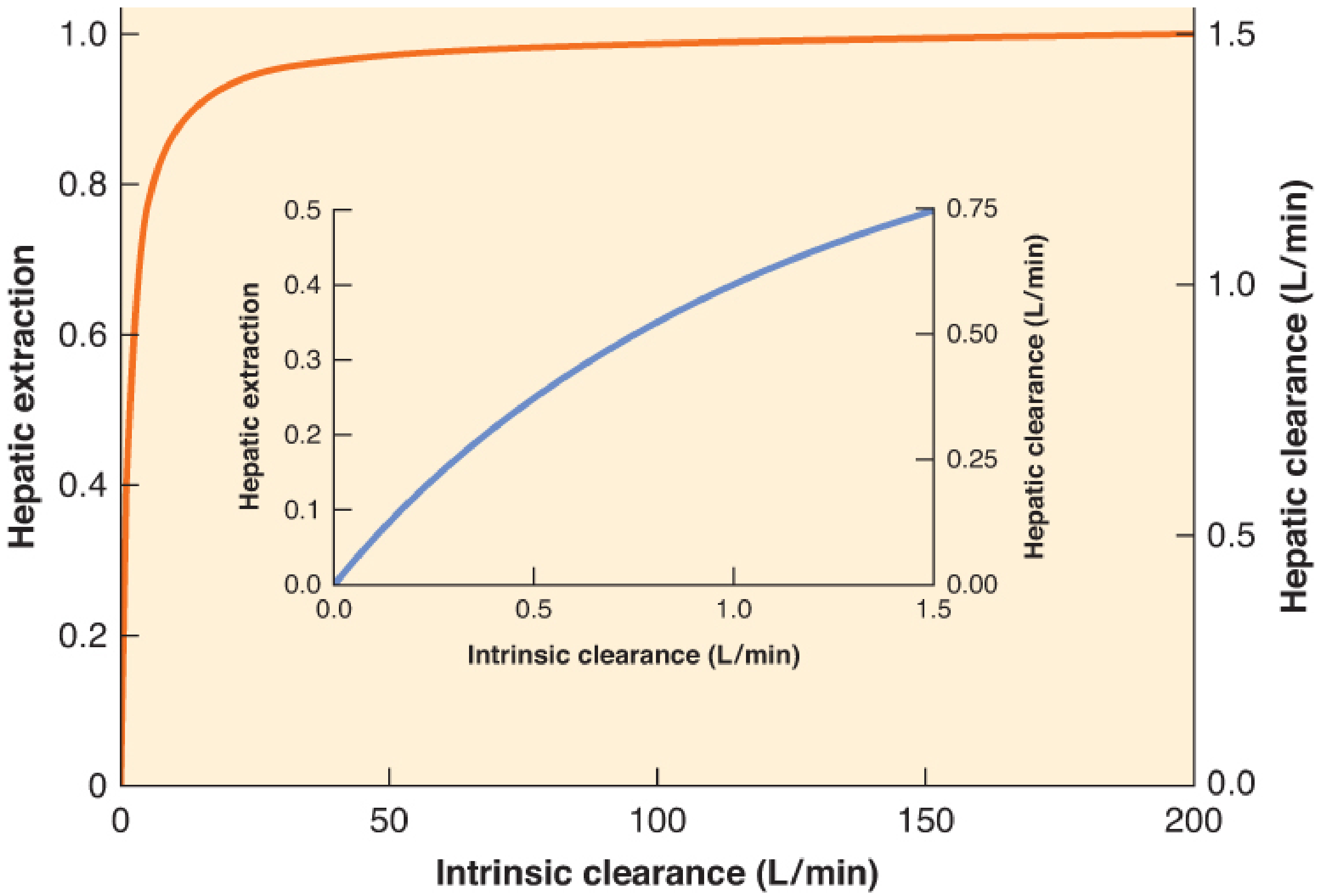
Full Physiologic Model (Intrinsic Clearance Formula)
A more mechanistic calculation incorporates intrinsic clearance (Cl_i) - the liver's inherent metabolic capacity independent of blood flow or protein binding:
$$E = \frac{Cl_i}{Q + Cl_i}$$
This shows two important limiting scenarios:
When intrinsic clearance is very HIGH (Cl_i >> Q):
$$E \approx 1 \quad \text{(flow-limited drugs)}$$
- Hepatic clearance approaches hepatic blood flow
- Changes in enzyme activity have minimal effect; changes in blood flow directly change clearance
When intrinsic clearance is very LOW (Cl_i << Q):
$$E \approx \frac{Cl_i}{Q} \ll 1 \quad \text{(capacity-limited drugs)}$$
- Hepatic clearance is nearly equal to intrinsic clearance
- Clearance is sensitive to enzyme inducers/inhibitors but NOT blood flow
(Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e)
Relationship to Hepatic Clearance
$$Cl_H = Q \times E$$
So:
$$Cl_H = Q \times \frac{Cl_i}{Q + Cl_i}$$
Relationship to Oral Bioavailability (First-Pass Effect)
After oral dosing, drug absorbed from the gut passes through the portal circulation to the liver before reaching systemic blood. The fraction that survives this first pass gives bioavailability (F):
$$F = f \times (1 - E)$$
Where f = fraction absorbed from the gut (accounting for gut wall metabolism).
Classification of Drugs by Extraction Ratio
| Category | E Value | Examples | Key Feature |
|---|---|---|---|
| Low | < 0.3 | Diazepam, lorazepam, phenytoin, theophylline, thiopental | Clearance depends on enzyme activity and protein binding; NOT affected by blood flow |
| Intermediate | 0.3 - 0.7 | Midazolam, alfentanil, methohexital, vecuronium | Both blood flow and enzyme activity matter |
| High | > 0.7 | Morphine, lidocaine, propofol, fentanyl, ketamine, propranolol, morphine, meperidine | Clearance is flow-limited; reduced cardiac output (e.g., shock, heart failure) directly reduces hepatic clearance |
(Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Table 11-3)
Clinical Implications
- High-extraction drugs (morphine, propranolol, lidocaine): oral bioavailability is low due to heavy first-pass metabolism; IV dose is much smaller than oral equivalent dose. In liver disease with portosystemic shunting, bioavailability of these drugs increases 2-10 fold - oral doses must be substantially reduced.
- Low-extraction drugs (diazepam, phenytoin): bioavailability is relatively preserved orally; clearance is sensitive to enzyme inducers/inhibitors (CYP450 interactions) and changes in protein binding.
- Reduced cardiac output states (heart failure, shock, spinal anesthesia): high-extraction drugs will accumulate because hepatic blood flow drops directly - but low-extraction drugs are largely unaffected.
This is a shared conversation. Sign in to Orris to start your own chat.