Headache management
Reading File
Finding Sources
Searching PubMed
"headache" AND "management"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Headache Management
A structured, evidence-based overview covering classification, acute treatment, prophylaxis, and special headache types.
1. Classification - Red Flags First
Before managing headache, exclude secondary (dangerous) causes. The key warning signs are:
- "Thunderclap" - sudden, worst-ever headache (subarachnoid hemorrhage until proven otherwise)
- New headache in age >50 (giant cell arteritis, mass lesion)
- Fever + neck stiffness (meningitis)
- Headache with focal neurologic signs or papilloedema
- Progressive worsening over days/weeks
- Headache in a cancer or immunocompromised patient
90% of patients presenting to primary care with headache have migraine. - Harrison's Principles of Internal Medicine 22E, 2025
2. Primary Headache Types & Their Management
A. Migraine
Acute (Abortive) Treatment
Step up based on attack severity:
Step 1 - Mild attacks:
- Aspirin, acetaminophen, or NSAIDs (ibuprofen, naproxen)
- Combination: acetaminophen + aspirin + caffeine (FDA-approved)
- Add a dopamine antagonist (metoclopramide 10 mg, prochlorperazine 10 mg) if nausea is present - also enhances GI absorption
Step 2 - Moderate-to-severe attacks (after NSAID failure):
| Drug | Route | Dose |
|---|---|---|
| Sumatriptan | PO | 50-100 mg |
| Rizatriptan | PO | 10 mg |
| Eletriptan | PO | 40 mg |
| Almotriptan | PO | 12.5 mg |
| Zolmitriptan | PO/nasal | 2.5 mg / 5 mg nasal |
| Sumatriptan | SC | 6 mg (fastest onset) |
| Sumatriptan | Nasal | 20 mg |
| Rimegepant (CGRP antagonist) | PO | 75 mg |
| Ubrogepant (CGRP antagonist) | PO | 50-100 mg |
| Lasmiditan (5-HT1F agonist) | PO | 50-200 mg |
Triptans are selective 5-HT1B/1D receptor agonists. Rizatriptan and eletriptan are the most efficacious on a population basis. Sumatriptan and zolmitriptan offer multiple formulations. - Harrison's
Triptan timing is key: Give oral/nasal forms at aura onset; SC at headache onset. Do NOT give during aura to prevent headache - they are ineffective in the aura phase but safe if given then.
Triptan contraindications: Ischemic heart disease, uncontrolled hypertension, basilar or hemiplegic migraine, concurrent MAOIs.
Special clinical situations (from Harrison's treatment table):
| Situation | Preferred Option |
|---|---|
| Early vomiting | Zolmitriptan 5 mg nasal / Sumatriptan 6 mg SC |
| Rapid onset headache | SC or nasal triptans / DHE IM |
| Headache recurrence | Ergotamine 2 mg PR / Naratriptan 2.5 mg / Eletriptan 40 mg |
| Poor tolerance of acute therapy | Naratriptan, Almotriptan, Rimegepant, neuromodulation |
| Menstrual migraine prevention | Frovatriptan, Rimegepant, or estrogen patches during menses |
Dihydroergotamine (DHE): 1 mg IV (over 3 min) or IM, or 2 mg nasal spray. Pretreat with antiemetic. Contraindicated in pregnancy, ischemic heart disease, within 24h of triptan use.
ED/Parenteral setting:
- IV prochlorperazine 5-10 mg (superior to opioids in RCTs)
- IV metoclopramide 10 mg
- IV ketorolac 15-30 mg
- IV mixture: prochlorperazine 5 mg + DHE 0.5 mg over 2 min (common protocol)
- Dexamethasone 6-10 mg IV as adjunct to reduce recurrence
- Magnesium sulfate 2 g IV over 30 min (nonvalidated)
- Opioids: Only for severe infrequent headache unresponsive to other therapies; avoid routine use as they worsen long-term outcomes and decrease future triptan responsiveness
Tintinalli's Emergency Medicine, Table 165-7
Neuromodulation (non-pharmacologic acute options):
- Single-pulse transcranial magnetic stimulation (sTMS) - FDA cleared
- Noninvasive vagus nerve stimulator (nVNS) - FDA cleared
- Remote electrical neuromodulation (arm device)
- Transcutaneous supraorbital nerve stimulation
Migraine Prophylaxis (Preventive Treatment)
Indicated when: ≥4 headache days/month, attacks significantly impairing function, failure/contraindication to acute therapies, medication overuse headache risk, or patient preference.
Established preventive agents:
| Drug Class | Agents | Notes |
|---|---|---|
| Beta-blockers | Propranolol, metoprolol, timolol | First-line; avoid in asthma, depression |
| Anticonvulsants | Topiramate, valproate | FDA-approved; valproate teratogenic |
| TCAs | Amitriptyline | Also treats comorbid depression/sleep |
| Calcium channel blockers | Verapamil | More evidence for cluster headache |
| CGRP monoclonal antibodies | Erenumab, fremanezumab, galcanezumab, eptinezumab | New class; SC/IV monthly; very effective |
| CGRP receptor antagonists | Rimegepant (also used acutely) | Oral, twice-weekly for prevention |
| Supplements | Magnesium, riboflavin (B2), CoQ10, feverfew | Modest evidence, good safety |
B. Tension-Type Headache (TTH)
Characteristics: Bilateral, pressing/tightening (non-pulsating), mild-to-moderate, no vomiting, no significant nausea, no aggravation by activity.
Acute treatment:
- Simple analgesics: aspirin, acetaminophen, NSAIDs (first-line for episodic TTH)
- More severe headaches may require prescription analgesics, but no specific preparation has proven superior
- Avoid opioids and barbiturate-containing combinations due to dependence and medication overuse risk
Prevention/chronic TTH:
- Amitriptyline (single bedtime dose) - treatment of choice when anxiety/depression comorbid
- Some evidence for calcium channel blockers, phenelzine, cyproheptadine
- Propranolol and ergotamine are ineffective unless migraine features co-exist
- Biofeedback, relaxation techniques, massage for anxious/stressed patients
- Medication overuse is a key concern - gradual analgesic withdrawal is essential in chronic daily headache
Adams and Victor's Principles of Neurology, 12th Ed.
C. Cluster Headache
Characteristics: Unilateral periorbital/temporal, excruciating (15-180 min), autonomic features (lacrimation, conjunctival injection, nasal congestion, ptosis), episodic or chronic, M > F.
Acute treatment:
- 100% oxygen via mask for 10-15 min at attack onset (highly effective, no side effects)
- Sumatriptan 6 mg SC or zolmitriptan 5 mg nasal spray
- Intranasal lidocaine (adjunct)
- Ergotamine 2 mg orally at bedtime (for predictable nocturnal attacks)
Preventive/transitional treatment:
- Verapamil (up to 480 mg/d) - first-line; requires ECG monitoring in older patients
- Prednisone 75 mg/d tapering over ~3 weeks (short-term bridge)
- Lithium 600-900 mg/d (chronic cluster; monitor for toxicity)
- Galcanezumab (anti-CGRP monoclonal antibody) - halved weekly cluster frequency in clinical trials
- Topiramate, melatonin as alternatives
Adams and Victor's Principles of Neurology, 12th Ed.; Harrison's 22E
D. Trigeminal Autonomic Cephalalgias (TACs) Comparison
| Feature | Cluster | Paroxysmal Hemicrania | SUNCT/SUNA |
|---|---|---|---|
| Duration | 15-180 min | 2-30 min | 5-240 sec |
| Frequency | 1-8/day | 1-20/day | 3-200/day |
| Abortive Rx | O2, sumatriptan SC | Indomethacin (diagnostic) | IV lidocaine |
| Prevention | Verapamil, galcanezumab | Indomethacin | Lamotrigine |
Paroxysmal hemicrania: Complete, absolute response to indomethacin is pathognomonic - start at 25 mg TID, titrate to 75 mg TID.
SUNCT/SUNA: Best prevented with lamotrigine 200-400 mg/d. Topiramate and gabapentin are alternatives.
Hemicrania continua: Unilateral continuous pain + autonomic features; complete response to indomethacin is diagnostic and therapeutic.
E. Medication Overuse Headache (MOH)
- Occurs when acute medications are used >10-15 days/month
- Highest risk: opioids and barbiturates > triptans > NSAIDs
- Treatment: gradual withdrawal of the offending medication (can be done abruptly for triptans/NSAIDs; slower for opioids/barbiturates)
- Preventive therapy should be started during withdrawal
- Multidisciplinary support improves outcomes
3. When to Refer
Per Harrison's 22E: Refer to a headache specialist when:
- No clear diagnosis
- Primary headache other than migraine or TTH
- Unresponsive to two or more standard therapies for the diagnosed type
- Any suspected secondary headache requiring specialist workup
Recent Evidence Note
A 2024 BMJ network meta-analysis (PMID 39293828) on acute migraine management confirmed triptans as effective first-line agents and provided comparative efficacy data across drug classes - consistent with current guideline recommendations.
Abdominal koch’s pain abdomen mana
Reading File
Finding Sources
Searching PubMed
"abdominal tuberculosis" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Now I have all the data needed. Here is the comprehensive answer:
Abdominal Tuberculosis (Koch's) - Pain Abdomen Management
Overview
Abdominal TB (Koch's abdomen) refers to TB involvement of the gastrointestinal tract, peritoneum, mesenteric lymph nodes, and/or solid organs. The abdomen is involved in ~11% of extrapulmonary TB cases. 50-80% of abdominal TB patients have peritoneal involvement. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Forms of Abdominal TB
| Form | Features |
|---|---|
| Intestinal TB | Terminal ileum/ileocaecal region most common (75%), ulcerative/hypertrophic/ulcerohypertrophic |
| Tuberculous peritonitis | Wet ascitic type (90%), dry fibrotic type (rare) |
| Mesenteric lymphadenitis | Enlarged nodes, central caseation - can be seen on CT |
| Solid organ | Liver, spleen involvement less common |
Clinical Presentation - Pain Abdomen in Abdominal TB
Chronic/Subacute:
- Abdominal pain - nonspecific, chronic; most common complaint (80-90% of patients)
- Weight loss, evening fever, malaise, night sweats
- Alternating diarrhoea and constipation
- Palpable RIF mass in 25-50% (ileocaecal involvement)
- Ascites and abdominal distension (peritoneal TB)
- "Doughy feel" of abdomen on palpation - a classical sign
Acute (Emergency presentation):
- Features of acute distal small bowel obstruction - colicky pain, abdominal distension, bilious/faeculent vomiting, absolute constipation
- Rarely: peritonitis from perforation of a tuberculous ulcer
- Acute-on-chronic: superimposed obstruction on longstanding disease
These patients are often extremely ill - dehydrated, malnourished, anaemic, often with active pulmonary TB. - Bailey & Love
Investigations
Bloods:
- FBC - mild anaemia, normal or mildly elevated WBC
- Raised ESR/CRP
- LFTs (especially with hepatic involvement)
- Urea and electrolytes (dehydration in obstruction)
Microbiological:
- Sputum AFB smear and culture (even without pulmonary symptoms, CXR is essential)
- IGRA (Interferon-Gamma Release Assay) - Quantiferon or T-SPOT
- Ascitic fluid analysis: straw-coloured exudate, protein >25-30 g/L, WBC >500/mL with lymphocytes >40%, AFB smear often negative, culture takes 4-8 weeks
- Adenosine deaminase (ADA) in ascitic fluid - high sensitivity and specificity for peritoneal TB
- Xpert MTB/RIF assay (on tissue, stool, or fluid) - more sensitive than AFB smear (~65%)
- Tissue biopsy: granulomas with caseation on histology (seen in 50-80% of cases)
Imaging:
- Plain AXR in obstruction: dilated small bowel loops, valvulae conniventes (concertina effect), fluid levels, featureless ileum
- CXR: pulmonary infiltrates/TB lesions (may be normal)
- USS abdomen: ascites (may be loculated), lymphadenopathy, bowel wall thickening
- CT abdomen: ileocaecal valve thickening, asymmetric bowel wall thickening, massive lymphadenopathy with central necrosis (characteristic), cecal contraction, Stierlin sign
- Barium meal/small bowel follow-through: multiple ileal strictures, subhepatic caecum (caecum pulled up by fibrosis - pathognomonic), ileum entering caecum in a straight line from below (Figure 6.38)
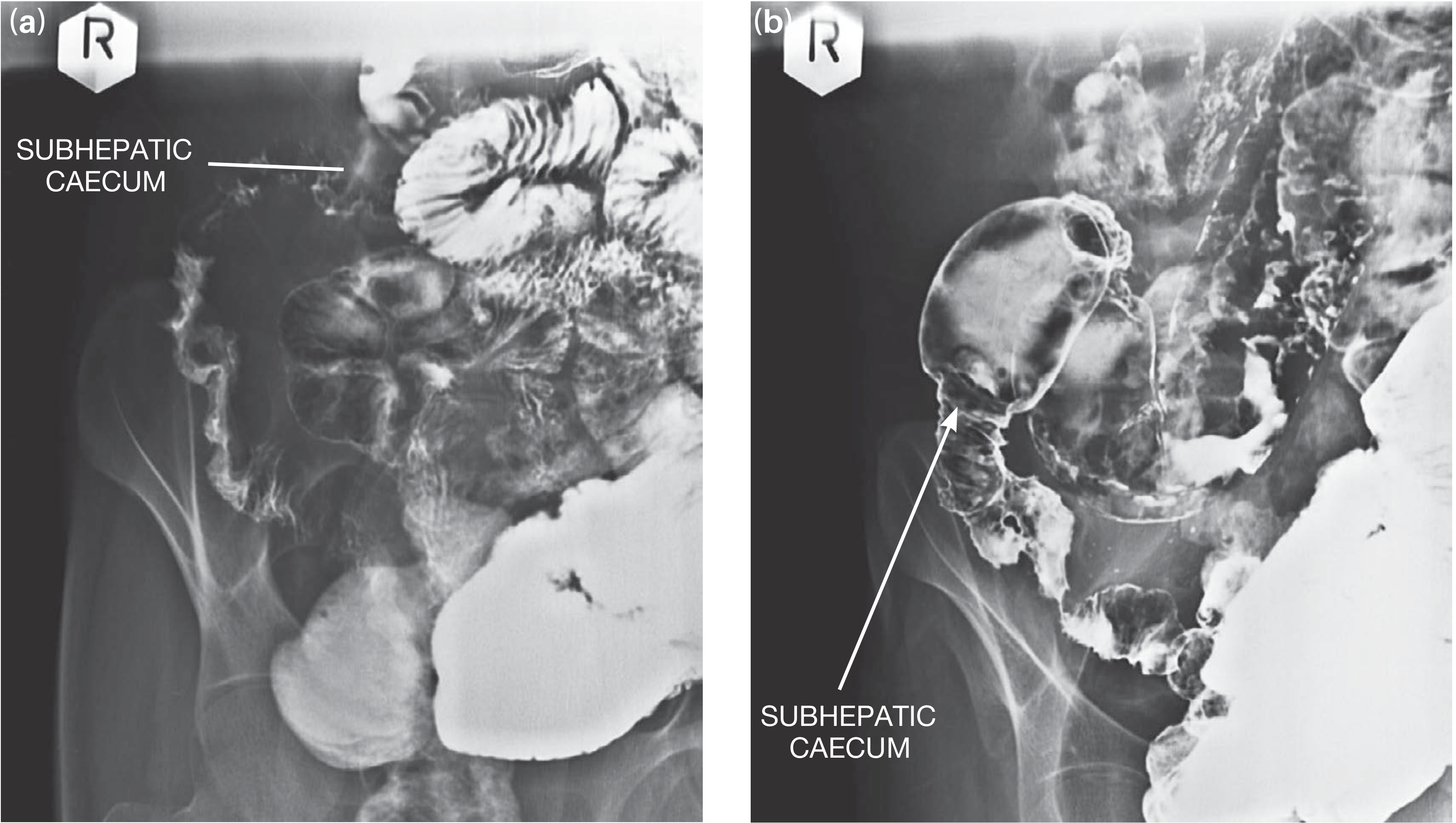
Barium follow-through showing ileal strictures with the caecum in a subhepatic position - Bailey & Love, 28th Ed.
Endoscopy:
- Colonoscopy with biopsy from ileocaecal region - most useful diagnostic procedure
- AFB staining, PCR, and culture on biopsy tissue (with drug sensitivity testing)
- Wear isolation masks when performing
Laparoscopy: Tubercles on bowel serosa, multiple strictures, high caecum, caseous lymph nodes, ascites - useful when biopsy via colonoscopy is inconclusive
Management
A. General Supportive Measures (All Patients)
- Nutrition - correct malnutrition; nasogastric or parenteral nutrition if required
- Hydration/fluid resuscitation - IV fluids for dehydration, especially in obstruction
- NGT decompression - in obstruction/ileus
- Anaemia correction - transfusion if Hb critically low pre-operatively
- Notify public health authorities - TB is a reportable disease; contact tracing
B. Medical Management - Anti-TB Therapy (MAINSTAY)
Abdominal TB is treated identically to pulmonary TB with standard short-course chemotherapy. A high index of suspicion warrants starting empirical therapy even before culture results - clinical response often occurs within 2 weeks. However, masses, hyperplasia, and strictures respond more slowly.
Standard Regimen (Drug-Sensitive TB):
| Phase | Duration | Drugs | Abbreviation |
|---|---|---|---|
| Intensive phase | 2 months | Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) | 2HRZE |
| Continuation phase | 4 months | Isoniazid (H) + Rifampicin (R) | 4HR |
| Total | 6 months |
For extrapulmonary TB including abdominal TB, a total duration of 12-18 months may be preferred in some guidelines/settings due to the depth of tissue penetration and risk of relapse. - Bailey & Love
Important notes:
- Send drug sensitivity testing (DST) from cultures - MDR-TB may be more prevalent in abdominal than pulmonary TB
- Add pyridoxine (Vitamin B6) 10-25 mg/day with isoniazid (prevents peripheral neuropathy)
- In HIV co-infection, ART should be initiated; standard TB regimens are used but with close monitoring for drug interactions (rifampicin and antiretrovirals)
- Adjunctive corticosteroids (prednisolone) may be considered in peritoneal TB with ascites to reduce inflammation and adhesion formation (though evidence is limited)
- Engage a TB specialist for management guidance
C. Surgical Management
Surgery is reserved for complications - it is NOT the primary treatment.
Indications for Surgery:
| Indication | Notes |
|---|---|
| Intestinal obstruction not responding to medical therapy | Most common surgical indication |
| Intestinal perforation | Emergency - peritoneal contamination |
| Intestinal hemorrhage | Uncontrolled bleeding |
| Abdominal abscess | Drainage required |
| Diagnostic uncertainty | Biopsy when endoscopic diagnosis not possible |
| Fistula formation | Entero-enteric or entero-cutaneous |
Key principle: Many cases of intestinal obstruction from TB will respond to anti-TB treatment without surgery. Always give adequate medical therapy before deciding on surgical intervention. - Bailey & Love, Summary Box 65.6
Surgical Options (Elective / Post-Medical Treatment):
After completion of medical treatment, re-image the small bowel. If significant strictures remain causing subacute obstruction:
| Surgical Procedure | Indication |
|---|---|
| Limited ileocolic resection + anastomosis | Terminal ileal/ileocolic hyperplastic disease |
| Strictureplasty | Single ileal stricture (bowel-conserving) |
| Bowel resection | Multiple closely placed strictures |
| Right hemicolectomy | Extensive ileocolic disease precluding limited resection |
Surgical principles are similar to Crohn's disease - resections should be kept as conservative as possible to prevent short bowel syndrome. - Bailey & Love, 28th Ed.
Emergency Surgery (Acute Obstruction/Perforation):
These patients present in extremis - dehydrated, malnourished, anaemic, often with active pulmonary TB.
Pre-operative resuscitation is mandatory:
- IV fluids - vigorous fluid resuscitation
- NGT decompression
- Correct electrolytes
- Blood transfusion if severely anaemic
- Broad-spectrum antibiotics (for perforation/secondary peritonitis)
At laparotomy - minimum life-saving procedure:
- Resection of the diseased segment + proximal ileostomy + distal ileal or colonic mucus fistula (preferred)
- This avoids primary anastomosis, which has a high leak rate in the presence of active infection and poor general condition
- One-stage resection and anastomosis is only performed if the patient's general condition permits (rare in the emergency setting)
Peritoneal TB - Specific Management
- Primarily medical (anti-TB chemotherapy as above)
- Therapeutic paracentesis for tense ascites causing respiratory compromise
- Laparoscopy + peritoneal biopsy if diagnosis in doubt
- Distinguish from peritoneal metastases (CT-guided biopsy or laparoscopy)
- Intestinal obstruction in peritoneal TB (fibrous "dry" type - matted loops) may respond to anti-TB therapy + corticosteroids alone before considering surgery
TB vs Crohn's Disease - Differential Diagnosis Points
| Feature | Intestinal TB | Crohn's Disease |
|---|---|---|
| Ileocaecal valve | Incompetent (both sides involved) | Usually competent |
| Ulcer orientation | Transverse, circumferential | Longitudinal (along bowel axis) |
| Lymph nodes | Large (>1 cm), hypodense (caseous) | Small, non-necrotic |
| Stierlin sign | Present | Absent |
| Granulomas | Caseating | Non-caseating |
| AFB/PCR | Positive | Negative |
Summary Algorithm
Suspected Abdominal Koch's (Pain abdomen)
↓
Red flags? (Obstruction / Perforation / Haemorrhage)
↓ ↓
YES NO
↓ ↓
Emergency resuscitation Confirm diagnosis
+ surgery if required (Colonoscopy + biopsy, CT, ADA)
↓
START ANTI-TB THERAPY
(2HRZE → 4HR, 6-18 months)
↓
Clinical response within 2 weeks?
↓ ↓
YES NO
↓ ↓
Continue ATT Re-evaluate diagnosis
↓ Consider MDR-TB / biopsy
Post-treatment imaging
↓
Residual stricture/obstruction?
↓
ELECTIVE SURGERY
(Strictureplasty / Limited resection)
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Bailey and Love's Short Practice of Surgery, 28th Ed.; Goldman-Cecil Medicine
Recent evidence note: A 2025 systematic review on abdominal TB in children (PMID 40533676) and a 2025 diagnostic evaluation and management review (PMID 40023548) confirm that standard 6-month HRZE/HR regimens remain the backbone of treatment, with surgical intervention reserved for complications unresponsive to medical therapy.
This is a shared conversation. Sign in to Orris to start your own chat.