Leukemoid reaction verses CML
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Excellent - I now have all the information needed for a thorough comparison. Here is the full answer:
Leukemoid Reaction vs. Chronic Myeloid Leukemia (CML)
Both conditions present with markedly elevated WBC counts (often >50,000/μL) and a left shift in the myeloid series on peripheral smear, making them a classic diagnostic challenge. The distinction is critical because one is benign and self-limiting, while the other is a malignant clonal disorder.
Definition
| Feature | Leukemoid Reaction | CML |
|---|---|---|
| Nature | Benign, reactive leukocytosis | Clonal myeloproliferative neoplasm |
| WBC count | Usually >50,000/μL | Often 50,000 - >300,000/μL |
| Cause | External trigger (infection, inflammation, malignancy, drugs) | BCR::ABL1 fusion gene (Philadelphia chromosome) |
Etiology & Pathogenesis
Leukemoid reaction is a physiologic, exaggerated bone marrow response to stimuli such as:
- Bacterial infections (e.g., diphtheria)
- Malignancy (e.g., Hodgkin disease)
- Rebound granulocytosis
- Corticosteroid administration
The granulocytic type is most common and shows reactive neutrophils with a left shift (bands, metamyelocytes, myelocytes), along with toxic granulation and Döhle bodies - morphologic signs of cellular stress.
CML is driven by the Philadelphia chromosome - a reciprocal translocation t(9;22)(q34;q11) between chromosomes 9 and 22, producing the BCR::ABL1 fusion gene. This encodes a constitutively active tyrosine kinase (p210 protein in most cases) that drives uncontrolled myeloid proliferation. Basophilia is an independent adverse prognostic factor in CML. - Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 132
Peripheral Blood Findings
| Feature | Leukemoid Reaction | CML |
|---|---|---|
| Left shift | Present (bands, metas, myelocytes) | Present (full spectrum of maturation) |
| Myelocyte "bulge" | Not characteristic | Characteristic - myelocytes exceed other immature forms |
| Basophilia | Absent or minimal | Prominent - hallmark feature |
| Eosinophilia | Absent or mild | Often present |
| Thrombocytosis | Absent | Often present |
| Toxic granulation / Döhle bodies | Present | Absent (cells appear relatively normal) |
| Blasts | Absent | <10% in chronic phase |
CML Microscopy
The peripheral blood and bone marrow findings in CML:
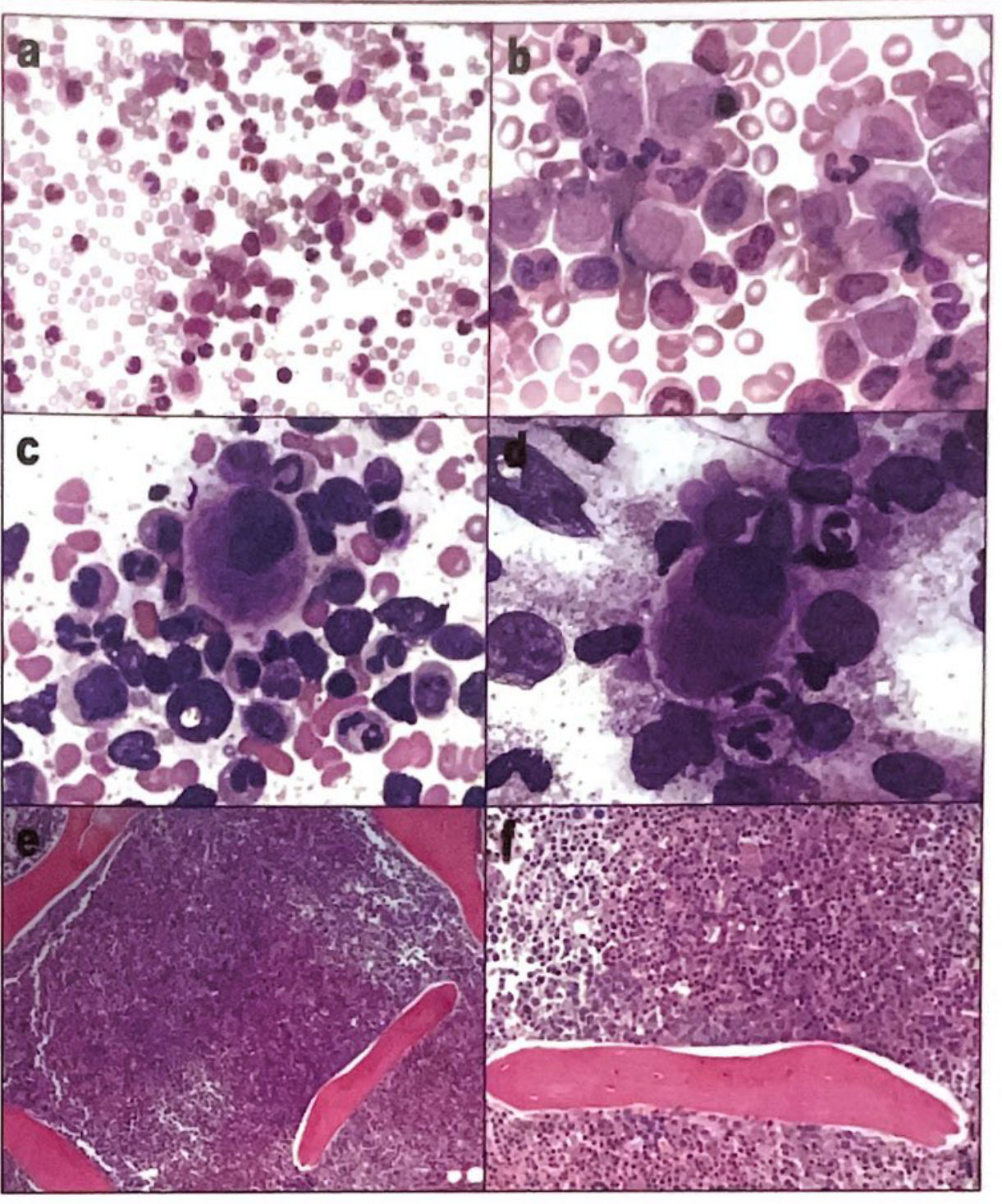
CML: (a,b) Peripheral blood shows leukocytosis with a range of myeloid progenitors, pronounced myelocytes, increased basophils and eosinophils, and thrombocytosis. (c,d) Marrow aspirate shows small mononuclear "dwarf" megakaryocytes alongside myeloid precursors. (e,f) Marrow biopsy demonstrates hypercellularity with a thickened regenerative zone. - Quick Compendium of Clinical Pathology, 5th ed.
The Key Differentiator: LAP Score (Leukocyte Alkaline Phosphatase)
The LAP score is scored visually on 100 bands and neutrophils (0-4+ per cell), then summed:
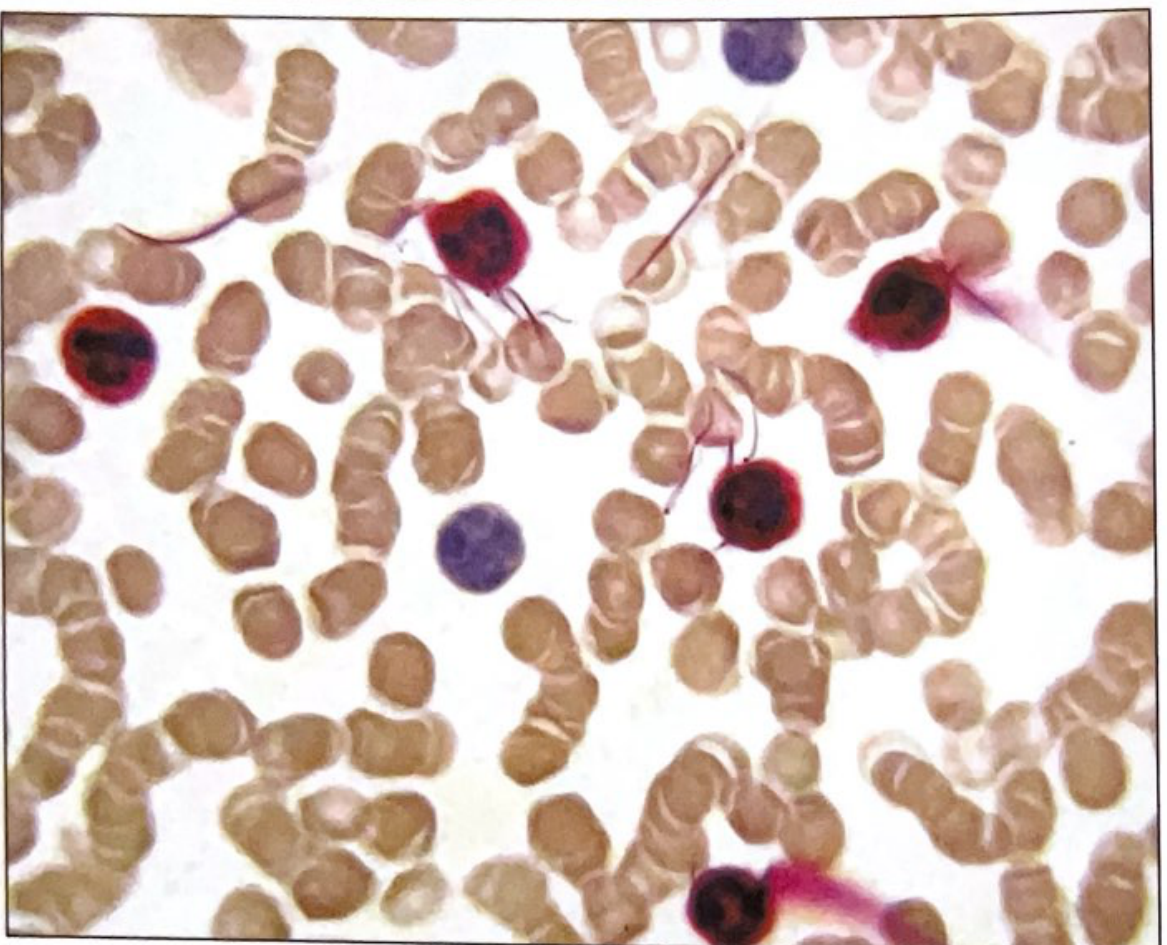
LAP stain: Positive (red-stained) neutrophils are scored 1-4+. Lymphocyte (blue, center) is negative.
| Condition | LAP Score |
|---|---|
| Normal adults | 40 - 120 |
| Leukemoid reaction | Elevated (>120) |
| CML | Low (0 - 15) |
| PNH | Low |
| MDS | Low |
| Polycythemia vera | Elevated |
| Glucocorticoid use | Elevated |
| 3rd trimester pregnancy | Elevated |
The neutrophil alkaline phosphatase (NAP/LAP) is normal or elevated in a leukemoid reaction but decreased in CML - this is a historically important and still clinically useful test. - Henry's Clinical Diagnosis and Management, p. 132; Quick Compendium of Clinical Pathology 5th ed., p. 297
Definitive Diagnosis of CML
| Test | CML | Leukemoid Reaction |
|---|---|---|
| BCR::ABL1 FISH / PCR | Positive | Negative |
| Philadelphia chromosome (cytogenetics) | Present - t(9;22)(q34;q11) | Absent |
| LAP score | Low (0-15) | High |
| Bone marrow biopsy | Hypercellular; myeloid hyperplasia; dwarf megakaryocytes | Reactive changes; no clonal abnormality |
| Splenomegaly | Common at presentation | Absent (unless due to underlying cause) |
| Basophilia | Prominent | Absent |
Molecular testing by quantitative PCR for BCR::ABL1 is also used to monitor treatment response to tyrosine kinase inhibitors (e.g., imatinib) in CML. - Henry's Clinical Diagnosis and Management, p. 132
CML Phases (Chronic Phase Features)
In the chronic phase of CML:
- Leukocytosis due to increased neutrophils at all stages of maturation
- The proportion of myelocytes exceeds other immature forms (the classic "myelocyte bulge")
- Basophilia + eosinophilia + thrombocytosis
- Blasts <10%
- Platelet aggregation defect: impaired response to epinephrine
The p210 BCR::ABL1 fusion protein is the most common; the rare p230 variant is associated with marked thrombocytosis and neutrophil maturation, and p190 (the m-BCR breakpoint) is associated with monocytosis and is also the breakpoint seen in Ph+ ALL. - Quick Compendium of Clinical Pathology 5th ed., p. 269
Summary Mnemonic
Think "CML = low LAP + basophilia + BCR-ABL + splenomegaly" vs. "Leukemoid = high LAP + toxic granulation + Döhle bodies + reactive cause"
This is a shared conversation. Sign in to Orris to start your own chat.