Give me last 10 previous exam sheet of community health nursing of bfuhs
Searching the Web
BFUHS community health nursing previous year question papers
Searching the Web
Baba Farid University Health Sciences nursing exam papers community health nursing PDF
I'm unable to run web searches at the moment due to a temporary API issue. Let me share what I know and point you in the right directions.
BFUHS Community Health Nursing - Previous Exam Papers
Unfortunately, I was unable to retrieve live search results right now. However, here is a practical guide to finding the last 10 previous exam question papers for Community Health Nursing (CHN) from Baba Farid University of Health Sciences (BFUHS), Faridkot, Punjab:
Official Sources
-
BFUHS Official Website Visit: www.bfuhs.ac.in
- Go to Examination section
- Look for "Previous Year Question Papers" or "Old Papers"
- Select the B.Sc Nursing / GNM / Post Basic B.Sc Nursing programme as applicable
-
BFUHS Examination Cell
- Contact the university examination cell directly at 0164-2300477 or email via the official website
- They can provide official copies of past papers
Reliable Third-Party Sources (to try manually)
These websites regularly host BFUHS nursing question papers:
- ExamYou / NursingExam.in - Search "BFUHS CHN question paper"
- NurseInfo.in - Has BFUHS B.Sc Nursing subject-wise papers
- Previouspapers.co.in
- AglaSem - nursing section
- Scribd / Studocu - Search "BFUHS community health nursing"
- Telegram groups for BFUHS nursing students (many share scanned PDFs)
Topics Typically Covered in BFUHS CHN Exams
Based on the standard BFUHS B.Sc Nursing syllabus (INC-aligned), CHN papers generally include:
| Unit | Topic |
|---|---|
| 1 | Concepts of community health, epidemiology |
| 2 | Health planning, national health programs |
| 3 | Family health nursing, MCH, RCH program |
| 4 | Communicable disease control |
| 5 | School health, occupational health |
| 6 | Environmental sanitation, water supply |
| 7 | Health statistics, vital statistics |
| 8 | Rural health services, PHC |
| 9 | Community health nursing process |
| 10 | Disaster management, rehabilitation |
Direct Search Tips
Try these Google search terms for best results:
"BFUHS" "community health nursing" "question paper" filetype:pdfsite:bfuhs.ac.in question paper nursingBFUHS BSc nursing 2nd year CHN paper 2023 2022 2021 2020
Note: I was unable to directly fetch or display the actual PDF exam sheets in this session due to a web search service outage. I strongly recommend visiting the official BFUHS website or the third-party sources listed above to download the papers directly. If you share a specific link or PDF, I can read and summarize its contents for you.
Define demography
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I have enough context from the library and my knowledge to give a thorough, well-structured answer on demography, especially in the context of community health nursing as taught in Park's Preventive and Social Medicine.
Demography
Definition
Demography is the scientific and statistical study of human populations - their size, structure, distribution, density, and the processes that change them over time, namely births (fertility), deaths (mortality), and migration.
The word "demography" is derived from two Greek words:
- "Demos" = people
- "Graphos" = to write/describe
So literally, demography means "description of the people."
Several authorities have defined demography as follows:
- Multilingual Demographic Dictionary (UN, 1958): "Demography is the scientific study of human populations, primarily with respect to their size, their structure, and their development."
- Donald Bogue: "Demography is the statistical and mathematical study of the size, composition, and spatial distribution of human populations, and of changes over time in these aspects through the operation of five processes - fertility, mortality, marriage, migration and social mobility."
- Philip Hauser and Otis Duncan: "Demography is the study of the size, territorial distribution, and composition of populations, and of changes therein, and the components of such changes."
Types of Demography
| Type | Description |
|---|---|
| Formal (Pure) Demography | Purely quantitative - deals with statistical measurement of population (size, growth, mortality, fertility) |
| Social Demography | Studies the relationship between population and social, economic, and environmental factors |
Scope of Demography
Demography covers five major areas:
- Population size - total number of people in a defined area
- Population composition - age, sex, marital status, literacy, occupation
- Population distribution - geographic spread, density (urban vs. rural)
- Population change - growth or decline over time
- Determinants and consequences - causes and effects of population changes
Demographic Processes (Components of Population Change)
The population at any time is determined by:
P₂ = P₁ + B - D + I - E
Where:
- P₁ = Population at start of period
- P₂ = Population at end of period
- B = Births
- D = Deaths
- I = In-migration (immigration)
- E = Out-migration (emigration)
Sources of Demographic Data
- Census - complete enumeration of population (in India, every 10 years)
- Vital registration - continuous recording of births, deaths, marriages
- Sample surveys - e.g., National Family Health Survey (NFHS), Sample Registration System (SRS)
- Health Management Information System (HMIS)
Key Demographic Indicators
| Indicator | Definition |
|---|---|
| Crude Birth Rate (CBR) | Births per 1,000 population per year |
| Crude Death Rate (CDR) | Deaths per 1,000 population per year |
| Infant Mortality Rate (IMR) | Deaths under 1 year per 1,000 live births |
| Maternal Mortality Rate (MMR) | Maternal deaths per 1,00,000 live births |
| Total Fertility Rate (TFR) | Average children born per woman over her lifetime |
| Sex Ratio | Number of females per 1,000 males |
| Dependency Ratio | Non-working to working population ratio |
| Life Expectancy | Average years a person is expected to live |
Importance of Demography in Community Health Nursing
- Health planning - helps nurses and planners identify the health needs of a community based on population size and structure
- Priority setting - a high proportion of children signals need for MCH/immunization programs; elderly population signals need for geriatric care
- Evaluation of health programs - changes in IMR, MMR, and life expectancy reflect program effectiveness
- Epidemiological studies - population data forms the denominator for calculating disease rates
- Resource allocation - guides deployment of health workers, clinics, and beds
- National health programs - demographic data drives programs like Reproductive and Child Health (RCH), Family Welfare, and Universal Immunization
Demographic Transition Theory
This theory describes how populations evolve through stages as countries develop:
| Stage | Birth Rate | Death Rate | Population Growth |
|---|---|---|---|
| Stage I - Pre-industrial | High | High | Stable/slow |
| Stage II - Early developing | High | Falling | Rapid growth |
| Stage III - Late developing | Falling | Low | Slowing growth |
| Stage IV - Developed | Low | Low | Stable/declining |
India is currently in Stage III of demographic transition.
Source: Park's Textbook of Preventive and Social Medicine (authoritative reference for community health nursing exams)
Reason for intense pain in chest
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from the textbooks. Here is the full, well-organized answer:
Causes of Intense Chest Pain
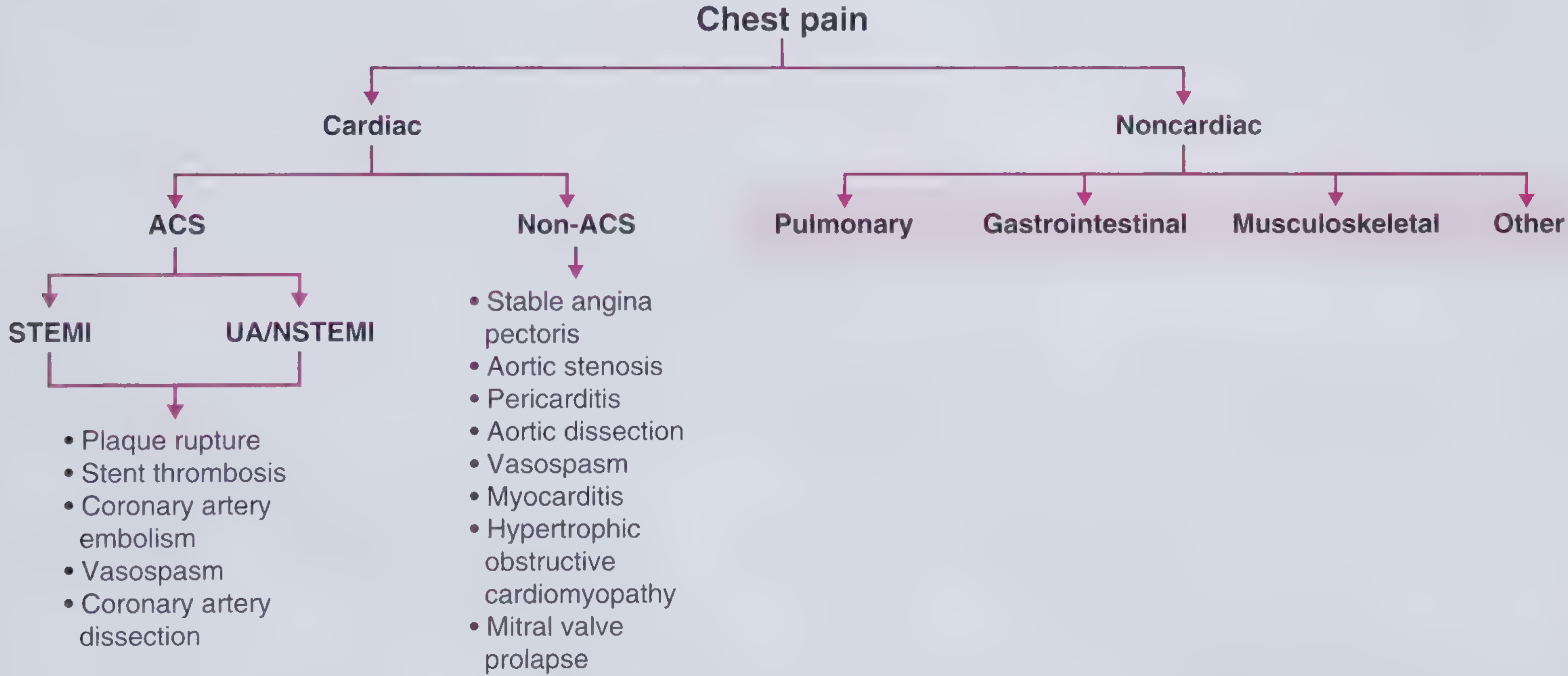
Chest pain is broadly divided into Cardiac and Noncardiac causes.
A. CARDIAC CAUSES
1. Acute Coronary Syndrome (ACS) - Most Dangerous
ACS describes a spectrum of conditions resulting in myocardial ischemia with or without infarction. It is caused by reduced blood flow to the heart muscle.
| Subtype | Description |
|---|---|
| STEMI (ST-elevation MI) | Complete blockage of a coronary artery; most severe; requires urgent reperfusion |
| NSTEMI (Non-ST-elevation MI) | Partial blockage with myocardial necrosis; elevated troponin |
| Unstable Angina (UA) | Partial blockage without necrosis; troponin normal |
Mechanism of ACS:
- Plaque rupture - atherosclerotic plaque tears open, triggering clot formation
- Stent thrombosis - clot forms on a previously placed coronary stent
- Coronary artery embolism
- Vasospasm (including Prinzmetal's angina)
- Coronary artery dissection
Character of pain: Heavy, crushing, squeezing substernal pressure; may radiate to left arm, jaw, neck, or back; lasts >20 minutes; associated with sweating, nausea, and breathlessness.
2. Non-ACS Cardiac Causes
| Condition | Character of Pain | Key Feature |
|---|---|---|
| Stable angina | Substernal pressure on exertion, relieved by rest | Due to fixed atherosclerotic plaque causing supply-demand mismatch |
| Aortic dissection | Sudden, tearing/ripping pain radiating to the back | Pulse discrepancy between limbs; widened mediastinum on X-ray |
| Acute pericarditis | Sharp, pleuritic pain - relieved by leaning forward | Diffuse ST elevation on ECG; friction rub |
| Aortic stenosis | Chest pain on exertion | Pulsus parvus et tardus; systolic ejection murmur |
| Myocarditis | Chest pain, often after viral infection | May progress to dilated cardiomyopathy |
| Hypertrophic Obstructive Cardiomyopathy (HOCM) | Exertional chest pain + syncope | Murmur intensifies with Valsalva |
| Mitral Valve Prolapse (MVP) | Recurrent chest pain + palpitations | Mid-systolic click on auscultation |
| Coronary artery vasospasm | Rest pain, often at night/early morning | Normal stress test; responds to nitrates |
B. NONCARDIAC CAUSES
1. Pulmonary Causes
| Condition | Character of Pain | Key Feature |
|---|---|---|
| Pulmonary Embolism (PE) | Sudden-onset pleuritic chest pain + dyspnea | Risk factors: cancer, immobility, post-surgery |
| Pneumonia | Pleuritic pain + fever + purulent cough | Dullness on percussion, increased tactile fremitus |
| Pleurisy | Sharp pain worsened by deep breathing, coughing, or sneezing | Inflammation of the pleural lining |
| Pneumothorax | Sudden sharp pain + dyspnea | Hyperresonance on percussion; absent breath sounds |
| Tension Pneumothorax | Severe pain + hemodynamic collapse | Emergency - requires immediate needle decompression |
| Pulmonary Hypertension | Exertional chest pain + dyspnea | Elevated JVP, loud P2, right ventricular heave |
| Acute Chest Syndrome | Sudden chest pain in sickle cell disease | Pulmonary infiltrates on imaging |
2. Gastrointestinal Causes
| Condition | Character of Pain |
|---|---|
| GERD (Acid Reflux) | Burning retrosternal pain, worsened after meals, relieved by antacids |
| Esophageal Spasm | Severe squeezing chest pain, mimics cardiac pain; may respond to nitrates |
| Peptic Ulcer / Gastritis | Epigastric burning pain |
| Esophageal Rupture (Boerhaave) | Sudden severe chest pain after vomiting |
| Hiatus Hernia | Burning retrosternal discomfort |
Note: GERD and esophageal causes are the most common non-cardiac causes of chest pain seen in emergency departments.
3. Musculoskeletal Causes
| Condition | Character of Pain |
|---|---|
| Costochondritis | Sharp, localized pain - reproducible with chest wall palpation; responds to NSAIDs |
| Rib Fracture | Localized chest pain after trauma; worse with breathing |
| Chest Wall Trauma | Similar to above |
| Cervical Angina (Radiculopathy) | Chest pain from C4-C8 nerve root compression (disc disease); associated with neck pain |
| Chest Wall Tumor | Most common primary malignant type is soft tissue sarcoma |
4. Other Causes
| Condition | Character of Pain |
|---|---|
| Herpes Zoster (Shingles) | Burning, dermatomal chest pain; followed by vesicular rash on erythematous base |
| Panic Disorder / Anxiety | Chest tightness + palpitations; associated with agoraphobia and depression |
| Referred pain | From gallbladder disease (right shoulder tip), spleen, subphrenic abscess |
Quick Clinical Memory Aid: "CARDIAC PLAN"
| Letter | Cause |
|---|---|
| C | Coronary artery disease / ACS |
| A | Aortic dissection / Angina |
| R | Reflux (GERD) / Esophageal spasm |
| D | Dissection (aortic) |
| I | Ischemia / Infarction |
| A | Anxiety / Arrhythmia |
| C | Costochondritis / Chest wall |
| P | Pulmonary embolism / Pneumothorax / Pericarditis |
| L | Lung conditions (pneumonia, pleuritis) |
| A | Aortic stenosis |
| N | Nerve root (cervical radiculopathy) |
Emergency Red Flags - Any chest pain with the following features requires immediate emergency care:
- Tearing/ripping quality (think aortic dissection)
- Crushing pain + diaphoresis (think MI)
- Sudden onset + breathlessness (think PE or pneumothorax)
- Hemodynamic instability (shock, hypotension, collapse)
Source: Frameworks for Internal Medicine (Lippincott); Tintinalli's Emergency Medicine

1000560859.jpg
Give me answer
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
BFUHS B.Sc.(N) 3rd Year - Child Health Nursing (BNN302) - Complete Answers
QUESTION 1(i)(a) - Behavioural Disorders & Management of Temper Tantrums [7.5]
Behavioural Disorders in Children
Behavioural disorders are patterns of emotional and behavioural problems that deviate from age-appropriate norms and interfere with a child's daily functioning.
Classification of Behavioural Disorders:
| Type | Description |
|---|---|
| Temper Tantrums | Explosive outbursts of anger, crying, screaming, common in 1-3 years |
| Enuresis | Involuntary bedwetting beyond 5 years of age |
| Encopresis | Fecal soiling after bowel control should be established |
| Thumb Sucking | Persistent sucking beyond infancy |
| Nail Biting | Biting nails due to anxiety/stress |
| Breath Holding Spells | Child holds breath when upset until cyanotic |
| School Phobia | Extreme anxiety about going to school |
| Attention Deficit Hyperactivity Disorder (ADHD) | Inattention, hyperactivity, impulsivity |
| Conduct Disorder | Persistent antisocial behaviour |
| Autism Spectrum Disorder | Social communication deficits |
Management of a Child with Temper Tantrums
Definition: Temper tantrums are intense emotional outbursts characterized by crying, screaming, kicking, breath-holding, and throwing objects. Common in children aged 1-4 years.
Causes:
- Frustration when unable to communicate needs
- Fatigue, hunger, or illness
- Over-stimulation
- Seeking attention
- Inability to get desired objects/activities
Nursing/Management Strategies:
1. Prevention:
- Maintain consistent daily routines (sleep, meals, play)
- Avoid situations known to trigger tantrums (overtiredness, hunger)
- Offer choices within limits (e.g., "Do you want red shirt or blue shirt?")
- Give advance warning before transitions ("5 more minutes, then bath time")
2. During a Tantrum:
- Stay calm - do not lose temper yourself
- Ensure the child is safe - remove hazards
- Ignore the behaviour (if safe) - do not give attention as reward
- Do NOT give in to demands - this reinforces the behaviour
- Do not reason or argue during the outburst
- Use a calm, firm voice
3. After the Tantrum:
- Comfort the child once calm
- Briefly discuss the behaviour in simple words
- Do not humiliate or punish
- Praise positive behaviour immediately when it occurs
4. Parental Guidance:
- Educate parents that tantrums are a normal developmental phase
- Teach parents positive reinforcement techniques
- Advise parents to model calm behaviour
- Advise against physical punishment
5. Medical Management (if severe):
- Rule out organic causes (pain, illness)
- Refer to child psychologist if behaviour is extreme or persists beyond age 5
Q1(i)(b) - Nursing Care of Infant and Child with HIV/AIDS [7.5]
Overview: HIV/AIDS in children is most commonly acquired through mother-to-child transmission (vertical transmission) during pregnancy, delivery, or breastfeeding.
Clinical Features in Children:
- Failure to thrive, poor weight gain
- Recurrent infections (bacterial, viral, fungal)
- Lymphadenopathy, hepatosplenomegaly
- Chronic diarrhoea
- Developmental delays
- Opportunistic infections (PCP pneumonia, oral candidiasis, CMV)
- Parotid swelling
Nursing Care:
1. Assessment:
- Monitor weight, height, head circumference regularly
- Assess nutritional status
- Record CD4 count and viral load results
- Monitor for signs of opportunistic infections
- Assess developmental milestones
2. Infection Prevention and Control:
- Follow Standard Precautions (gloves, mask, gown as needed)
- Prevent exposure to communicable diseases
- Ensure complete immunization (note: live vaccines with caution in symptomatic children)
- Maintain strict hand hygiene
- Isolate from infectious patients
3. Nutritional Support:
- Provide high-calorie, high-protein diet
- Support breastfeeding decisions (per WHO guidelines and PMTCT protocol)
- Treat oral candidiasis to allow feeding
- Monitor for failure to thrive
4. Medication Administration:
- Administer Antiretroviral Therapy (ART) as prescribed - e.g., Zidovudine (AZT), Lamivudine, Nevirapine
- Give Cotrimoxazole prophylaxis for PCP prevention
- Administer antifungals for candidiasis
- Ensure medication adherence - use appropriate formulations (syrups for infants)
5. Psychosocial Support:
- Maintain confidentiality
- Support parents and caregivers emotionally
- Refer to counselling services
- Address stigma and discrimination
- Age-appropriate disclosure to older children
6. Developmental Support:
- Monitor and stimulate developmental milestones
- Refer to early intervention programs if developmental delay is noted
- Encourage school attendance in stable children
7. Discharge Teaching:
- Medication schedule and adherence
- Signs of deterioration requiring re-admission
- Follow-up schedule for CD4 monitoring
- Nutritional guidance
- Safe sex education for adolescents
QUESTION 1(ii)(a) - OR: Wilm's Tumor [7.5]
Definition
Wilm's tumor (Nephroblastoma) is the most common primary malignant renal tumor of childhood, usually occurring in children under 5 years of age. It arises from embryonic renal tissue (metanephric blastema) and is associated with mutations in the WT1 gene on chromosome 11.
Epidemiology:
- Peak age: 3-4 years
- Can be unilateral (most common) or bilateral (5-10%)
- Associated with WAGR syndrome (Wilm's, Aniridia, Genitourinary abnormalities, intellectual disability/Retardation)
Clinical Features:
- Abdominal mass - most common presenting sign (firm, smooth, non-tender)
- Abdominal pain
- Haematuria (blood in urine)
- Hypertension (due to renin secretion)
- Fever, weight loss, anorexia
- Anemia
Diagnosis:
- Ultrasound abdomen - first investigation
- CT scan / MRI abdomen - staging
- Chest X-ray - check for lung metastasis
- Urinalysis and serum creatinine
- Biopsy (confirmatory)
Staging (National Wilm's Tumor Study - NWTS):
| Stage | Description |
|---|---|
| I | Tumor limited to kidney, completely resected |
| II | Extends beyond kidney, completely resected |
| III | Residual non-hematogenous tumor in abdomen |
| IV | Haematogenous metastases (lung, liver, bone) |
| V | Bilateral renal involvement |
Medical Treatment: Surgery (nephrectomy) + Chemotherapy (Vincristine, Actinomycin-D, Doxorubicin) + Radiotherapy (Stage III onwards)
Nursing Care of Child with Wilm's Tumor
Pre-operative Nursing Care:
- Do NOT palpate the abdomen vigorously - risk of tumor rupture and spreading malignant cells
- Post "DO NOT PALPATE ABDOMEN" sign at bedside
- Monitor BP regularly (hypertension is common)
- Prepare child and family emotionally for surgery
- Pre-operative investigations: CBC, BUN, creatinine, urine analysis
- Maintain IV access; keep child NPO before surgery
- Administer pre-operative medications as prescribed
Post-operative Nursing Care:
- Monitor vital signs every 2-4 hours
- Assess wound site for bleeding, infection
- Monitor urine output hourly (ensure remaining kidney is functioning)
- Maintain fluid balance chart
- Pain management - analgesics as prescribed
- Encourage early ambulation
- NGT care if needed
Chemotherapy/Radiotherapy Nursing Care:
- Monitor for nausea, vomiting - administer antiemetics
- Monitor for bone marrow suppression - CBC monitoring
- Maintain strict infection precautions (neutropenia)
- Ensure adequate nutrition and hydration
- Monitor mouth sores (mucositis) - oral hygiene care
- Protect child from radiation exposure to caregivers
Psychosocial Care:
- Provide age-appropriate explanations to the child
- Support parents through grief and fear
- Encourage therapeutic play
- Facilitate school re-integration when appropriate
Discharge Teaching:
- Follow-up chemotherapy schedule
- Signs of infection (fever, chills)
- Dietary and activity restrictions
- Contact sports avoidance (protect remaining kidney)
- Importance of long-term renal function monitoring
QUESTION 1(ii)(b) - OR: Hydrocephalus [7.5]
Definition
Hydrocephalus is an abnormal increase in the volume of CSF (cerebrospinal fluid) within the ventricular system of the brain, resulting from impaired flow, decreased resorption, or rarely overproduction of CSF. In infants (before cranial suture fusion), it causes head enlargement; after suture fusion, it causes raised intracranial pressure (ICP).
Types:
- Non-communicating (Obstructive): Blockage within ventricular system (e.g., aqueduct stenosis, tumor, hemorrhage)
- Communicating: CSF flows freely but absorption is impaired (e.g., post-meningitis, post-hemorrhage)
- Normal Pressure Hydrocephalus (NPH): Seen in elderly - triad of dementia, gait disturbance, urinary incontinence
- Hydrocephalus ex vacuo: Compensatory increase due to brain tissue loss
Causes:
- Congenital (aqueductal stenosis, myelomeningocele, Dandy-Walker malformation)
- Post-hemorrhagic (intraventricular hemorrhage in premature infants)
- Post-meningitis (adhesions block CSF flow)
- Brain tumor
- Arnold-Chiari malformation
Clinical Features (Infant):
- Rapidly increasing head circumference
- Bulging anterior fontanelle
- Dilated scalp veins
- "Sunset sign" (eyes deviated downward)
- Irritability, high-pitched cry
- Vomiting, poor feeding
- Shiny scalp skin
Diagnosis:
- Head circumference measurement
- Cranial ultrasound (in infants with open fontanelle)
- CT / MRI brain - gold standard
- Transillumination of skull
Treatment:
- Ventriculo-Peritoneal (VP) Shunt - most common surgical treatment; CSF drained from ventricle to peritoneum
- Ventriculo-Atrial (VA) shunt - alternative
- Endoscopic Third Ventriculostomy (ETV) - for obstructive hydrocephalus
- Acetazolamide (reduces CSF production temporarily)
Nursing Care of Child with Hydrocephalus
Pre-operative:
- Measure and record head circumference daily using same tape
- Assess fontanelle - bulging or tense indicates raised ICP
- Elevate head of bed 15-30 degrees to reduce ICP
- Monitor neurological status - level of consciousness, pupil reactions
- Handle head gently - support head when lifting
- Prevent skin breakdown on scalp (reposition frequently)
- Monitor for signs of raised ICP: vomiting, irritability, sunset sign
- Prepare child and family for surgery
Post-operative (VP Shunt):
- Position child on the non-operated side initially
- Monitor for shunt malfunction: return of symptoms (headache, vomiting, drowsiness)
- Assess for shunt infection (fever, redness along shunt tract, neck stiffness)
- Measure head circumference daily
- Monitor fontanelle (should become softer post-operatively)
- Maintain skin integrity of scalp
- Strict neurological observations
General Nursing Care:
- Provide small, frequent feedings (large feeds can trigger vomiting)
- Protect eyes if exophthalmos present (use eye drops/patch)
- Encourage developmental stimulation within limitations
- Physiotherapy for motor delays
- Psychosocial support for family
Discharge Teaching:
- Signs of shunt malfunction or infection
- When to come to hospital immediately
- Developmental follow-up
- Head circumference monitoring at home
- Safe play activities; avoid contact sports
QUESTION 2 - Burns [3+5+7 = 15]
(a) Definition of Burns [3]
Burns are injuries to the skin and underlying tissues caused by thermal, chemical, electrical, or radiation agents. They result in cell death, protein denaturation, and disruption of the skin barrier, leading to fluid loss, infection risk, and metabolic derangements.
(b) Classification of Burns [5]
1. By Depth (Degree Classification):
| Degree | Depth | Appearance | Sensation | Healing |
|---|---|---|---|---|
| 1st Degree (Superficial) | Epidermis only | Red, dry, no blisters | Painful | 3-7 days, no scar |
| 2nd Degree Superficial | Epidermis + superficial dermis | Blisters, moist, pink | Very painful | 10-21 days, minimal scar |
| 2nd Degree Deep | Epidermis + deep dermis | Blisters, pale/red, wet | Less painful | 21-35 days, scarring |
| 3rd Degree (Full Thickness) | All skin layers | Dry, leathery, white/brown/black | Painless (nerve destruction) | Requires skin grafting |
| 4th Degree | Skin + muscle, bone, tendon | Charred, black | Painless | Amputation may be needed |
2. By Cause:
- Thermal (flame, scald, contact)
- Chemical (acid, alkali)
- Electrical (low/high voltage)
- Radiation (sunburn, X-ray)
3. By Extent - Rule of Nines (Modified for Children using Lund & Browder Chart):
| Body Part | Adult % | Infant modification |
|---|---|---|
| Head | 9% | 18% (larger head) |
| Each Arm | 9% | 9% |
| Chest/Abdomen | 18% | 18% |
| Back | 18% | 18% |
| Each Leg | 18% | 14% (smaller legs) |
| Perineum | 1% | 1% |
4. Severity Classification:
- Minor: <10% BSA, 2nd degree or <2% 3rd degree
- Moderate: 10-20% BSA
- Major/Critical: >20% BSA, or any 3rd degree, or burns to face, hands, feet, perineum, or circumferential burns
(c) Nursing Management of a Child with Burns [7]
Emergency/Immediate Phase:
- Stop the burning process - remove child from source, remove clothing/jewelry
- Cool the burn - cool (not cold/ice) running water for 10-20 minutes
- Airway management - assess for inhalation injury (singed eyebrows, hoarse voice); prepare for intubation if needed
- IV access - two large bore IV lines
- Fluid resuscitation (Parkland Formula): 4 ml × weight (kg) × % BSA burned of Ringer's Lactate in first 24 hours (half in first 8 hours, half in next 16 hours)
- Pain management - IV morphine or opioid analgesia
- Wound assessment - calculate BSA burned using Lund & Browder chart
Nursing Assessment:
- Vital signs monitoring every 1-4 hours
- Urine output monitoring (target 1 ml/kg/hr in children)
- Neurological status
- Depth and extent of burn
- Signs of infection at wound site
Wound Care:
- Clean wound with chlorhexidine or saline
- Apply topical antimicrobial agents (silver sulfadiazine, bacitracin)
- Non-adherent dressings
- Change dressings as prescribed (every 24-48 hours)
- Prevent infection - strict aseptic technique
- Prepare for skin grafting if 3rd degree burns
Nutritional Support:
- High-calorie, high-protein diet (burn patients have massively increased metabolic needs)
- Nasogastric tube feeding if oral intake insufficient
- Monitor weight daily
Pain Management:
- Scheduled analgesics (not PRN only)
- Procedural analgesia before dressing changes
- Non-pharmacological: distraction, play therapy
Infection Prevention:
- Isolation precautions
- Strict hand hygiene
- Monitor for signs of sepsis (fever, tachycardia, high WBC)
- Wound culture as needed
Psychological Care:
- Explain all procedures to child in age-appropriate language
- Therapeutic play
- Support parents
- Refer to psychologist for severe burns
Rehabilitation:
- Physiotherapy and occupational therapy to prevent contractures
- Pressure garments to reduce scarring
- Splinting of joints
- Scar management
QUESTION 3 - Hirschsprung's Disease [2+8 = 10]
(a) Definition [2]
Hirschsprung's disease (congenital aganglionic megacolon) is a congenital condition in which there is an absence of ganglion cells (aganglionosis) in the myenteric (Auerbach's) and submucosal (Meissner's) plexuses of the distal colon and rectum. This occurs due to failure of neural crest cell migration during embryogenesis, resulting in a non-peristaltic distal segment and functional intestinal obstruction.
- Incidence: 1 in 5,000 live births
- More common in males
- Associated with Down syndrome (Trisomy 21)
- Most cases involve rectum and sigmoid colon
(b) Management of Child with Hirschsprung's Disease [8]
Clinical Presentation:
- Neonates: failure to pass meconium within 48 hours of birth
- Abdominal distension
- Bilious vomiting
- Chronic constipation
- Poor feeding and weight gain
- In older children: ribbon-like stools, failure to thrive
Diagnosis:
- Barium enema - shows narrow aganglionic segment and dilated proximal colon (transition zone)
- Anorectal manometry - absent recto-anal inhibitory reflex
- Rectal biopsy - gold standard; shows absence of ganglion cells and hypertrophied nerve trunks
Medical Management (Pre-operative stabilization):
- NGT decompression
- IV fluids and correction of electrolyte imbalances
- Rectal irrigations (saline washouts) to decompress the bowel
- Antibiotics if enterocolitis present
- Nutritional support
Surgical Management (Definitive Treatment):
- Staged procedure (traditional):
- Stage 1: Colostomy (temporary) - to divert stool from obstructed segment
- Stage 2: Pull-through operation (Swenson, Soave, or Duhamel procedure) - resection of aganglionic segment and anastomosis of normal colon to rectum
- Stage 3: Colostomy closure
- Single-stage pull-through - now more commonly done (all in one operation)
Nursing Management:
Pre-operative:
- Monitor vital signs and abdominal girth
- Maintain NPO status; IV fluids
- Perform rectal irrigations as prescribed
- Bowel preparation
- Skin preparation
- Psychological preparation of child and parents
Post-operative:
- Monitor vital signs, wound site, abdominal distension
- Maintain IV fluids; advance to oral feeds gradually
- Stoma care if colostomy created (skin protection, bag changes, teaching parents)
- Monitor for complications: wound infection, anastomotic leak, enterocolitis
- Pain management
- Monitor bowel function - passage of stool, continence
Discharge Teaching:
- Stoma care (if applicable) and signs of problems
- Dietary modifications - high-fibre diet long-term
- Signs of Hirschsprung-associated enterocolitis (fever, explosive diarrhoea, distension - emergency)
- Long-term bowel habit training
- Follow-up appointments
QUESTION 4 - Malnutrition [3+7 = 10]
(a) Definition of Malnutrition [3]
Malnutrition is a state of nutritional imbalance in which the body does not receive adequate nutrients (undernutrition) or receives excessive nutrients (overnutrition) for normal growth, development, and physiological functioning.
In the context of child health, malnutrition most commonly refers to undernutrition, which includes:
- Wasting - low weight for height (acute malnutrition)
- Stunting - low height for age (chronic malnutrition)
- Underweight - low weight for age
- Micronutrient deficiencies - vitamin A, iron, zinc, iodine deficiencies
Clinical forms: Kwashiorkor (protein deficiency), Marasmus (calorie deficiency), Marasmic-Kwashiorkor (mixed)
(b) Nutritional Assessment in Children and Causes of Malnutrition [7]
Nutritional Assessment:
1. Anthropometric Measurements:
- Weight for Age - underweight indicator (Z-score < -2 SD = underweight)
- Height/Length for Age - stunting indicator
- Weight for Height - wasting indicator
- Mid-Upper Arm Circumference (MUAC):
-
12.5 cm = Normal
- 11.5-12.5 cm = Moderate Acute Malnutrition (MAM)
- <11.5 cm = Severe Acute Malnutrition (SAM)
-
- BMI for age (in older children)
- Head circumference (reflects brain growth in infants)
2. Clinical Assessment:
- Hair: sparse, dull, easily pluckable, flag sign (Kwashiorkor)
- Skin: loose skin (Marasmus), edema (Kwashiorkor), dermatosis
- Eyes: Bitot's spots, xerophthalmia (Vit A deficiency)
- Mouth: angular stomatitis, cheilosis (Vit B2), glossitis
- Nails: koilonychia (iron deficiency)
- Abdomen: distension, hepatomegaly (Kwashiorkor)
- Muscles: wasting, reduced strength
- Edema: pitting edema of legs/face in Kwashiorkor
3. Dietary Assessment:
- 24-hour dietary recall
- Food frequency questionnaire
- Dietary history from parents
- Breastfeeding history
4. Biochemical Assessment:
- Serum albumin (low in Kwashiorkor - <3.5 g/dL)
- Hemoglobin (anemia)
- Serum electrolytes (hypokalemia, hyponatremia)
- Blood glucose (hypoglycemia in SAM)
- Serum ferritin (iron stores)
- Serum Vitamin A levels
5. Functional Assessment:
- Developmental milestones
- Activity level and play
- Immune function (susceptibility to infections)
Causes of Malnutrition in Children:
1. Dietary Causes:
- Inadequate food intake - poverty, food insecurity
- Early cessation of breastfeeding
- Inappropriate complementary feeding (too early, too late, or wrong foods)
- Poor dietary diversity
- Food taboos and cultural practices
2. Disease-related Causes:
- Recurrent infections (diarrhoea, pneumonia, measles) - increase metabolic demand and reduce absorption
- Intestinal parasites (worms)
- HIV/AIDS
- Tuberculosis
- Malabsorption syndromes (celiac disease, cystic fibrosis)
- Congenital heart disease (increased caloric needs)
3. Socioeconomic Causes:
- Poverty and low household income
- Poor maternal education
- Unemployment
- Large family size
- Lack of access to healthcare
4. Environmental Causes:
- Poor sanitation and water supply
- Unhygienic food preparation
- Poor storage of food (aflatoxin contamination)
- Natural disasters, conflict zones
5. Maternal Causes:
- Maternal malnutrition (low birth weight infants)
- Teenage pregnancy
- Short birth intervals
- Poor antenatal care
6. Health System Causes:
- Lack of growth monitoring programs
- Poor immunization coverage
- Inadequate micronutrient supplementation (Vit A, iron, zinc)
QUESTION 5 - Short Notes (Any Five) [5×5 = 25]
(a) Role of Child Health Nurse in Caring for a Hospitalized Child
The child health nurse plays a multi-dimensional role:
- Care Provider - Administers medications, performs procedures, monitors vital signs, wound care
- Advocate - Ensures the child's rights and best interests are protected; speaks for the child who cannot speak for themselves
- Educator - Teaches child (age-appropriately) and parents about the illness, medications, and home care
- Communicator - Uses therapeutic communication and play techniques to gain child's trust
- Supporter - Provides emotional support to child and family; addresses fear and anxiety
- Coordinator - Coordinates with doctors, physiotherapists, dietitians, social workers
- Promoter of Family-Centered Care - Encourages parents to stay and participate in care (rooming-in)
- Infection Controller - Maintains aseptic technique, prevents hospital-acquired infections
- Developmental Facilitator - Provides age-appropriate stimulation and play to support development during hospitalization
- Researcher - Participates in evidence-based practice to improve pediatric outcomes
(b) Preventive Paediatrics
Preventive paediatrics focuses on preventing disease and promoting optimal health in children.
Levels of Prevention:
| Level | Examples |
|---|---|
| Primordial | Healthy maternal nutrition, safe environment |
| Primary | Immunization, health education, nutrition supplementation, accident prevention |
| Secondary | Growth monitoring, newborn screening, early diagnosis and treatment |
| Tertiary | Rehabilitation, preventing complications of established disease |
Key Preventive Activities:
- Immunization - following national immunization schedule (BCG, OPV, DPT, MMR, Hepatitis B, etc.)
- Breastfeeding promotion - exclusive breastfeeding for 6 months
- Nutritional supplementation - Vitamin A, iron-folic acid, zinc
- Growth monitoring - regular weight/height measurements, plotting on growth chart
- IMNCI (Integrated Management of Neonatal and Childhood Illness) - identifies and manages common childhood illnesses
- Safe water and sanitation - preventing diarrhoeal disease
- School health programs - physical examination, vision screening, dental care
- Adolescent health - reproductive health education, mental health support
(c) Organisation of Neonatal Unit
A Neonatal Unit (NICU/SNCU/NBSU) is a specialized unit caring for sick or preterm newborns.
Levels of Neonatal Care:
- Level I (NBSU): Basic newborn care, healthy term babies
- Level II (SNCU): Special newborn care; gestational age >32 weeks, weight >1500 g
- Level III (NICU): Intensive care; very preterm, <1500 g, critically ill neonates
Physical Organisation:
- Reception/Admission area - initial assessment and stabilization
- Intensive care bay - radiant warmers, incubators, ventilators, cardiac monitors
- Step-down bay - less intensive monitoring, Kangaroo Mother Care (KMC)
- Isolation area - for infants with infections
- Parents' room - for rooming-in and KMC
- Milk bank / expressed breast milk area
- Procedure room - for intubation, lumbar puncture, surgeries
Equipment:
- Radiant warmers and incubators (thermoregulation)
- Neonatal ventilators, CPAP machines
- Pulse oximeters, cardiorespiratory monitors
- Infusion pumps
- Phototherapy units (for jaundice)
- Emergency resuscitation equipment
Staffing:
- Neonatologist/Pediatrician
- Trained neonatal nurses (ratio: 1:2 in NICU, 1:4 in step-down)
- Physiotherapist, dietitian
- Social worker
(d) Prevention of Accidents in Children
Accidents are the leading cause of death in children over 1 year of age.
Common Accidents by Age Group:
| Age | Common Accidents |
|---|---|
| Infant (0-1 yr) | Suffocation, falls, burns/scalds |
| Toddler (1-3 yr) | Falls, drowning, poisoning, foreign body ingestion |
| Pre-school (3-5 yr) | Road accidents, drowning, burns |
| School age (6-12 yr) | Road accidents, sports injuries, drowning |
| Adolescent | Road accidents, sports injuries, violence |
Prevention Strategies:
-
Home Safety:
- Use stair gates, window guards, cabinet locks
- Keep medicines, cleaning agents out of reach (child-proof containers)
- Never leave infant/toddler unattended in bath
- Cover electrical sockets
- Use smoke detectors and fire extinguishers
-
Road Safety:
- Car seats and seatbelts for age-appropriate groups
- Cycle helmets
- Teach road crossing rules
- Supervised crossing near schools
-
Water Safety:
- Never leave child unattended near water
- Swimming lessons from age 4+
- Life jackets near open water
- Fence around home swimming pools
-
Playground Safety:
- Age-appropriate equipment
- Soft surfaces under equipment
- Supervision
-
School:
- Safety education as part of curriculum
- First aid training for teachers
(e) Signs and Symptoms of Rheumatic Heart Disease
Rheumatic Heart Disease (RHD) is a complication of acute rheumatic fever (ARF), caused by Group A beta-hemolytic Streptococcal infection, resulting in permanent damage to heart valves.
Signs and Symptoms:
Acute Rheumatic Fever (Jones Criteria):
Major Criteria:
- Carditis - tachycardia, new murmur, cardiomegaly, pericardial friction rub
- Migratory polyarthritis - hot, swollen joints moving from joint to joint
- Sydenham's chorea - involuntary, irregular movements (St. Vitus dance)
- Erythema marginatum - pink ring-shaped rash on trunk
- Subcutaneous nodules - painless nodules over bony prominences
Minor Criteria:
- Fever (38.5°C+)
- Elevated ESR/CRP
- Prolonged PR interval on ECG
- Arthralgia (if arthritis not counted as major)
Chronic Rheumatic Heart Disease:
- Mitral stenosis - most common valve lesion; dyspnea, orthopnea, haemoptysis
- Mitral regurgitation - systolic murmur at apex
- Aortic stenosis/regurgitation - exertional dyspnea, angina, syncope
- Heart failure symptoms - edema, breathlessness, fatigue
- Atrial fibrillation - irregular pulse
- Embolic events - stroke from clots forming in fibrillating atria
(f) Juvenile Diabetes Management
Juvenile Diabetes (Type 1 Diabetes Mellitus) is an autoimmune condition in which the beta cells of the pancreas are destroyed, resulting in absolute insulin deficiency.
Management:
1. Insulin Therapy:
- Multiple daily injections (basal-bolus regimen):
- Long-acting insulin (glargine/detemir) once/twice daily
- Rapid-acting insulin (aspart/lispro) before meals
- Insulin pump (CSII) - continuous subcutaneous insulin infusion
- Injection sites: abdomen, thighs, upper arm - rotate sites
2. Blood Glucose Monitoring:
- Self-monitoring blood glucose (SMBG) - 4-6 times daily
- Continuous Glucose Monitor (CGM) - preferred in children
- Target HbA1c: <7% (individualized)
3. Dietary Management:
- Consistent carbohydrate counting
- Three main meals + snacks
- Avoid simple sugars, refined carbohydrates
- High fibre diet
- Consistent meal timing
4. Exercise:
- Regular physical activity encouraged
- Monitor blood glucose before and after exercise
- Carry fast-acting glucose (juice, glucose tablets) during activity
- Adjust insulin or carbohydrate intake for planned exercise
5. Hypoglycemia Management:
- Recognition: sweating, trembling, confusion, pallor
- Treatment: 15 g fast-acting carbohydrate (glucose tablets, juice)
- Rule of 15: give 15 g carbs, recheck in 15 minutes; if still low, repeat
- Severe hypoglycemia: glucagon injection/IV dextrose
6. Education (Diabetes Self-Management Education - DSME):
- Insulin administration technique
- Blood glucose monitoring
- Sick day rules (continue insulin even if not eating)
- Signs of hypo/hyperglycemia
- School management plan
- Emotional/psychological support
(g) Hemophilia
Definition: Hemophilia is a hereditary bleeding disorder caused by a deficiency of clotting factors - Factor VIII deficiency = Hemophilia A (most common), Factor IX deficiency = Hemophilia B (Christmas disease).
Inheritance: X-linked recessive - affects males predominantly; females are carriers.
Classification:
| Type | Factor Level | Severity |
|---|---|---|
| Mild | 5-40% | Bleeds with major trauma/surgery |
| Moderate | 1-5% | Bleeds with minor trauma |
| Severe | <1% | Spontaneous bleeds |
Clinical Features:
- Prolonged bleeding after cuts, injections, surgery, dental extraction
- Haemarthrosis - bleeding into joints (knees, elbows, ankles most common); painful, swollen joint
- Deep muscle haematomas
- Spontaneous bruising
- Intracranial haemorrhage (life-threatening)
- Hematuria
Diagnosis:
- Prolonged aPTT (activated partial thromboplastin time)
- Normal PT, platelet count, bleeding time
- Factor VIII or IX assay - confirms diagnosis
Management:
-
Factor Replacement Therapy:
- Hemophilia A: recombinant Factor VIII concentrate
- Hemophilia B: recombinant Factor IX concentrate
- Desmopressin (DDAVP) - for mild Hemophilia A (releases stored Factor VIII)
- On-demand treatment: when bleeding occurs
- Prophylaxis: regular infusions 2-3 times/week to prevent bleeds
-
RICE for acute haemarthrosis:
- Rest - keep joint immobile
- Ice - reduce swelling
- Compression - gentle bandaging
- Elevation - raise affected limb
- Give Factor concentrate immediately
-
Avoid:
- Aspirin and NSAIDs (impair platelet function)
- IM injections (use SC or IV instead)
- Contact sports
-
Nursing Care:
- Handle child gently - avoid unnecessary trauma
- Apply prolonged pressure after injections
- Teach parents and child to recognize and manage bleeds
- Medical alert bracelet
- School alert plan
- Regular dental care (with Factor coverage before procedures)
- Physiotherapy for joint rehabilitation after haemarthrosis
- Genetic counselling for family
All answers are exam-ready for BFUHS B.Sc.(N) 3rd Year Child Health Nursing. Sources: Robbins & Kumar Basic Pathology; Frameworks for Internal Medicine; standard pediatric nursing curriculum aligned with INC syllabus.
This is a shared conversation. Sign in to Orris to start your own chat.