Tabulate differences in CSF examination in Pyogenic, Tuberculous*, Viral Meningitis; CSF findings in Meningitis 2. Meningioma** - gross, microscopic features ( 3. Acute (purulent) Leptomeningitis - morphology, CSF findings 1. Pyogenic Meningitis - aetiology, indication of CSF examination, CSF findings in Pyogenic and Tuberculous Meningitis (answer in detail covering imp points as welll in exaam point of view 2mbbs pathology refer harsh moham add diagrams as well cover required points for muhs exam Add histo pathology diagram and gross as well FOR EXAM drawing point of view
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
I now have all the key textbook content. Let me compile a comprehensive, exam-oriented answer.
CNS Infections & Meningioma - Pathology Notes (2nd MBBS / MUHS Exam)
Source: Robbins & Cotran Pathologic Basis of Disease | Robbins & Kumar Basic Pathology | Bradley & Daroff's Neurology
PART 1: MENINGITIS - CLASSIFICATION & OVERVIEW
Meningitis = inflammation of the leptomeninges (pia + arachnoid) and CSF within the subarachnoid space, usually infectious.
Three broad types:
| Type | Etiology | Course |
|---|---|---|
| Acute Pyogenic (Bacterial) | Bacteria | Acute, fulminant |
| Aseptic (Viral) | Viruses (enteroviruses 80%) | Subacute, self-limited |
| Chronic | TB, fungi, spirochetes | Weeks-months |
PART 2: ACUTE PYOGENIC (BACTERIAL / PURULENT) MENINGITIS
2A. Aetiology (Age-based - Exam Favourite)
| Age Group | Common Organisms |
|---|---|
| Neonates (<1 month) | Escherichia coli, Group B Streptococci |
| Infants / Children | Haemophilus influenzae (now rare with vaccination) |
| Adolescents / Young Adults | Neisseria meningitidis (meningococcus) |
| Older Adults (>60) | Streptococcus pneumoniae, Listeria monocytogenes |
| Immunosuppressed | Klebsiella, anaerobic organisms, fungi |
Exam tip: The most common organism overall = S. pneumoniae. Meningococcal meningitis clusters in young adults and raises public health concerns. Vaccination against H. influenzae has markedly reduced its incidence.
2B. Indications for CSF Examination (Lumbar Puncture)
- Suspected meningitis (bacterial, viral, TB, fungal)
- Subarachnoid haemorrhage (xanthochromia)
- Encephalitis
- Unexplained altered consciousness with fever
- Neurosyphilis, cryptococcal infection
- Intracranial pressure assessment
- Intrathecal drug administration
Contraindications to LP: Raised ICP with papilloedema (risk of herniation), bleeding disorders, infection at LP site.
2C. Clinical Features
- Systemic signs: fever, rigors, malaise
- Meningeal irritation: severe headache, photophobia, neck stiffness (nuchal rigidity)
- Kernig's sign (+), Brudzinski's sign (+)
- Clouding of consciousness, irritability
- Elevated CSF pressure on LP (cloudy/frankly purulent fluid)
PART 3: MORPHOLOGY OF ACUTE PURULENT LEPTOMENINGITIS
3A. Gross Features
- Meningeal vessels are congested/engorged and stand out prominently
- Exudate within the leptomeninges over the brain surface - cloudy to frankly purulent
- Distribution varies with organism:
- H. influenzae - basal distribution
- S. pneumoniae - over cerebral convexities near the sagittal sinus
- Tracts of pus follow blood vessels on brain surface
- In fulminant cases: ventriculitis (extension to ventricles)
- Complications: leptomeningeal fibrosis → hydrocephalus; pneumococcal: chronic adhesive arachnoiditis (due to capsular polysaccharide)
Gross photo - Pyogenic meningitis:
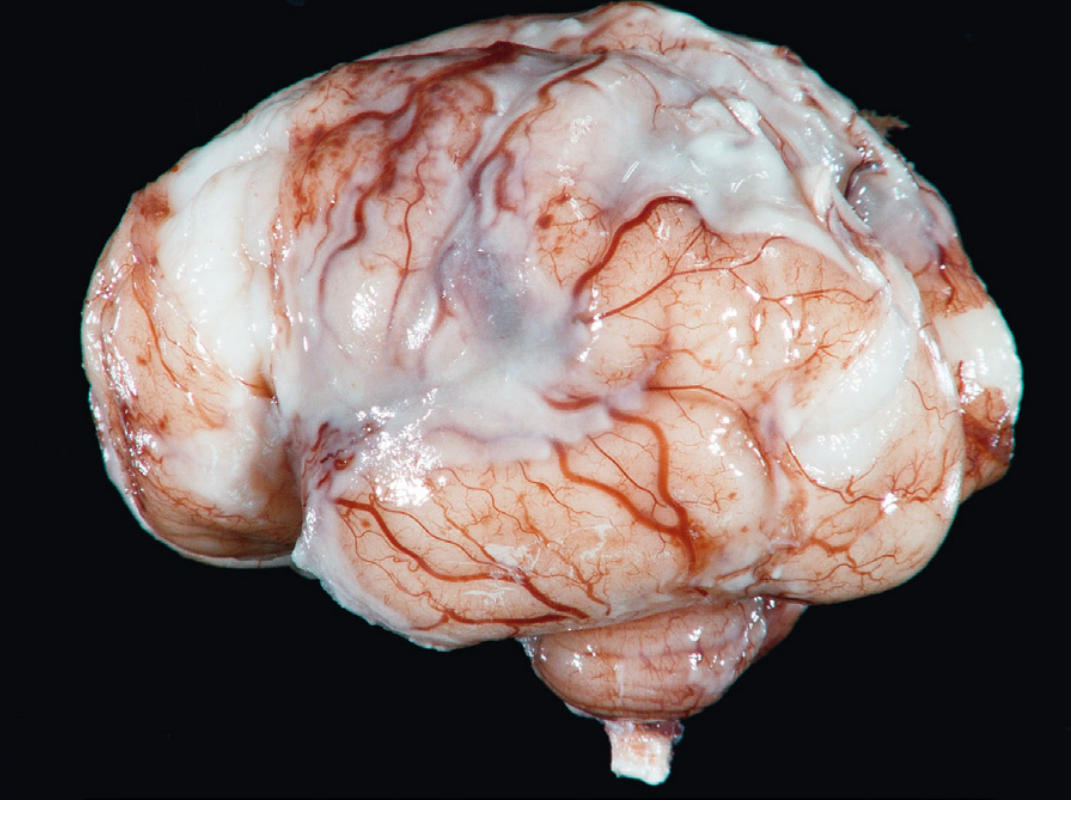
Gross appearance: Thick suppurative exudate covering the brain surface, thickening the leptomeninges. Meningeal vessels are engorged and prominent.
3B. Microscopic Features
- Neutrophils fill the subarachnoid space in severely affected areas
- Neutrophils predominantly around leptomeningeal blood vessels in less severe cases
- Gram stain: reveals variable numbers of bacteria
- In fulminant cases: inflammatory cells infiltrate walls of leptomeningeal veins and extend into brain parenchyma (cerebritis)
- Secondary vasculitis and venous thrombosis → haemorrhagic cerebral infarction
- Pia rarely breached in typical bacterial meningitis
Exam drawing tip: Draw subarachnoid space filled with neutrophils (PMNs), engorged blood vessels in meninges, brain surface intact, and bacteria visible on Gram stain between cells.
3C. Waterhouse-Friderichsen Syndrome (Important Complication)
- Meningitis-associated septicaemia + haemorrhagic infarction of adrenal glands
- Occurs most often with meningococcal and pneumococcal meningitis
- Results in adrenal insufficiency + septic shock
PART 4: CSF EXAMINATION - COMPARISON TABLE
CSF Findings in Meningitis (Most Important Exam Table)
| Parameter | Normal | Pyogenic (Bacterial) | Tuberculous | Viral (Aseptic) |
|---|---|---|---|---|
| Appearance | Clear, colourless | Turbid / Purulent / Cloudy | Clear / Xanthochromic / Cobweb clot | Clear |
| Pressure | 70-180 mmH₂O | Markedly elevated | Elevated (moderate) | Normal / Mildly elevated |
| Cell count | 0-5 cells/mm³ | 200-20,000 cells/mm³ | 100-500 cells/mm³ | 10-500 cells/mm³ |
| Predominant cell type | Lymphocytes | Neutrophils (PMNs) | Lymphocytes | Lymphocytes |
| Protein | 15-45 mg/dL | Markedly elevated (100-500 mg/dL) | Elevated (100-400 mg/dL) | Mildly elevated (50-100 mg/dL) |
| Glucose | 50-80 mg/dL (2/3 of blood glucose) | Markedly reduced (<40 mg/dL) | Reduced (moderately) | Normal |
| CSF:Blood glucose ratio | >0.6 | <0.4 (very low) | 0.4-0.5 (low) | Normal (>0.6) |
| Organisms on smear | Absent | Gram stain positive in ~60-80% | AFB smear (ZN stain) - positive in ~25-40%; culture gold standard | Not seen (viral, no bacteria) |
| Culture | Sterile | Positive for bacteria | Positive for MTB (slow, weeks) | Viral culture / PCR |
| Special features | - | Neutrophilic pleocytosis; may clot | Cobweb/pellicle formation (fibrin web); AFB ZN stain | Self-limited; enterovirus most common |
| Chloride | 120-130 mEq/L | Reduced | Markedly reduced (<120 mEq/L) | Normal |
| Clinical course | - | Acute, fulminant; fatal if untreated | Subacute-chronic; weeks | Mild, self-limiting |
Memory Aid (MUHS favourite):
- Pyogenic = Pus (PMNs), Protein up, glucose Down dramatically
- TB = Lymphocytes, low glucose (not as low as pyogenic), cobweb clot, AFB
- Viral = Lymphocytes, normal glucose, mild protein rise
Cobweb Clot (TB - Exam Point)
In TB meningitis, when CSF is allowed to stand, a fine fibrinous "cobweb" or "pellicle" forms in the test tube - a classic finding. This is due to the high fibrin content. AFB can be found in this cobweb clot.
PART 5: MENINGIOMA
5A. Introduction
- Most common intracranial extraaxial tumor (>1/3 of newly diagnosed CNS tumors)
- Arises from arachnoidal (meningothelial) cap cells - hence extraaxial, dural-based
- More common in females (progesterone receptor positive in >50%)
- Can enlarge dramatically with pregnancy and regress after delivery
- Associated with NF2 gene mutation (chromosome 22q12) in >50% of cases
- Other mutations: TRAF7, KLF4, AKT1, SMO
5B. Gross Features
- Well-demarcated, lobulated, firm mass attached to the dura
- Compresses but does NOT invade adjacent brain / spinal cord (pushes brain aside)
- Gritty consistency due to sand-like calcifications (psammoma bodies)
- Often shows a dural tail sign on imaging / gross specimen
- May invade bone (hyperostosis) - does NOT constitute malignancy
- Meningioma en plaque = diffuse carpet-like spread along dural surface
- Cut surface: grey-white, lobulated, firm to rubbery
- Common locations: parasagittal (falcine), sphenoid wing, olfactory groove, parasellar, spinal canal
Exam drawing tip (gross): Draw a well-encapsulated, lobulated, firm mass attached to dura/falx with a broad dural base. The brain is pushed/compressed to one side. Mark the attachment to dura clearly.
5C. Microscopic Features (Histopathology)
Three major histological patterns:
| Pattern | Features |
|---|---|
| Meningothelial (Syncytial) | Arachnoidal epithelioid cells in lobules with prominent whorls and psammoma bodies |
| Fibroblastic | Spindle cells in fascicular or storiform pattern; abundant collagen |
| Transitional | Mixed features of both above |
Key Microscopic Features to Know:
- Meningothelial whorls - concentric spiral arrangements of tumour cells (pathognomonic appearance)
- Psammoma bodies - concentrically laminated calcifications formed from degenerated meningothelial whorls (appear as basophilic laminated concentric rings)
- Cells have pale vesicular nuclei with central clearing (nuclear pseudoinclusions)
- EMA (Epithelial Membrane Antigen) - positive in vast majority (key IHC marker for meningothelial differentiation)
- Progesterone receptor - positive in >50%
- No mitoses / very rare in Grade I (benign)
Histopathology diagram - Meningioma (Whorls & Psammoma bodies):
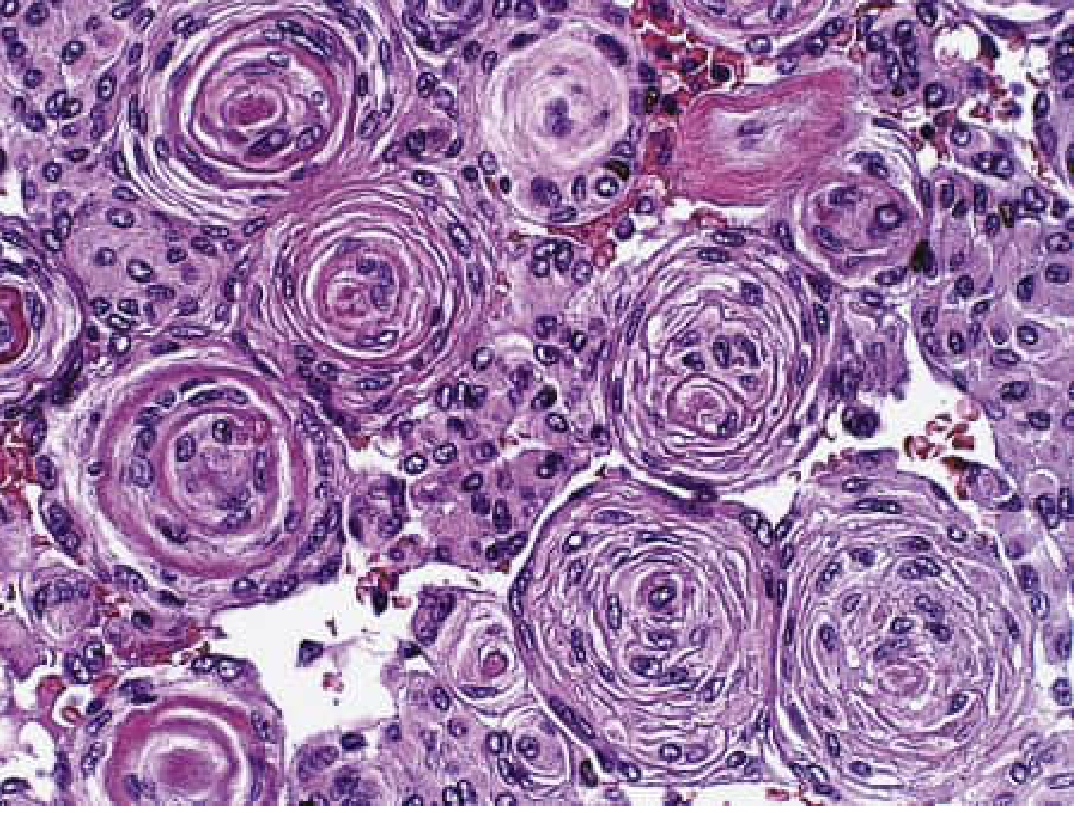
H&E x400: Multiple concentric meningothelial whorls with psammoma bodies (laminated calcifications). This is the classic "storiform" pattern.
Exam drawing (microscopic): Draw 3-4 concentric whorls of cells. In the centre of some whorls, draw a pink/basophilic laminated structure (psammoma body). Cells have pale oval nuclei. Label: meningothelial cells, whorls, psammoma body.
5D. WHO Grading of Meningioma
| Grade | Type | Features |
|---|---|---|
| Grade I | Benign | Most common; <4 mitoses/10 HPF |
| Grade II | Atypical | ≥4 mitoses/10 HPF or 3 of 5 criteria (sheeting, hypercellularity, macronucleoli, small cells, necrosis); higher recurrence |
| Grade III | Anaplastic/Malignant | Frank malignancy; rare (2%); brain invasion |
Special aggressive variants: Clear cell (II), Chordoid (II), Papillary (III), Rhabdoid (III).
QUICK REVISION BOX - MUHS EXAM KEY POINTS
Pyogenic Meningitis
- Aetiology: age-based (E. coli/GBS in neonates → N. meningitidis in young adults → S. pneumoniae in elderly)
- CSF: purulent, ↑↑pressure, neutrophils (PMNs), ↑↑protein, ↓↓glucose, Gram stain +ve
- Gross: exudate over brain surface, engorged vessels
- Micro: neutrophils in subarachnoid space, bacteria on Gram stain
- Complication: Waterhouse-Friderichsen syndrome, hydrocephalus, cerebritis
TB Meningitis
- CSF: clear/xanthochromic, cobweb clot, lymphocytes, ↑ protein, ↓ glucose and chloride, ZN stain for AFB
- Base of brain predominantly affected (basal exudate)
Viral Meningitis
- CSF: clear, lymphocytes, mildly ↑ protein, normal glucose (KEY differentiator)
- Self-limited; enteroviruses (80%)
Meningioma
- Gross: firm, lobulated, dural-attached, gritty (psammoma bodies), compresses but does not invade brain
- Micro: meningothelial whorls + psammoma bodies; EMA positive; PR positive
- Grade I = benign; excellent prognosis with total resection
Sources: Robbins & Cotran Pathologic Basis of Disease (10th ed.), Robbins & Kumar Basic Pathology (11th ed.), Bradley & Daroff's Neurology in Clinical Practice.
This is a shared conversation. Sign in to Orris to start your own chat.