Define cardiac output. Factors effecting cardiac output
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed for a thorough, well-cited answer. Here it is:
Cardiac Output
Definition
Cardiac output (CO) is the total volume of blood ejected by each ventricle per unit time. It reflects the overall pumping capacity of the heart.
"The total volume of blood ejected per unit time is the cardiac output. Thus cardiac output depends on the volume ejected on a single beat (stroke volume) and the number of beats per minute (heart rate)."
- Costanzo Physiology, 7th Ed.
Formula
CO = Stroke Volume (SV) × Heart Rate (HR)
- Normal resting values (70-kg man): SV ~70 mL × HR ~72 beats/min = ~5,000 mL/min (5 L/min)
- Normal range: 4-8 L/min at rest
Related Measures
| Parameter | Formula | Normal Value |
|---|---|---|
| Stroke Volume (SV) | EDV - ESV | ~70 mL |
| Ejection Fraction (EF) | SV / EDV | ~55-65% |
| Cardiac Index (CI) | CO / BSA | 2.5-4.0 L/min/m² |
(EDV = end-diastolic volume; ESV = end-systolic volume; BSA = body surface area)
Factors Affecting Cardiac Output
CO is governed by four major determinants - two intrinsic to the heart and two extrinsic (vascular coupling):
"Cardiac output is determined by four factors: two factors that are intrinsic to the heart (heart rate and myocardial contractility) and two factors that are extrinsic to the heart but functionally couple the heart and the vasculature (preload and afterload)."
- Miller's Anesthesia, 10th Ed.
1. Heart Rate (Chronotropy)
When SV is constant, CO is directly proportional to HR. HR is intrinsically set by the SA node (~90-100 beats/min in young adults) but is continuously modified:
| Influence | Effect on HR |
|---|---|
| Sympathetic (β1 stimulation) | ↑ HR |
| Vagal (M2 stimulation) | ↓ HR |
| Circulating catecholamines | ↑ HR |
| Hyperthermia, hypoxia | ↑ HR |
| Hypothyroidism, beta-blockers | ↓ HR |
| Very high HR (>120 bpm) | ↓ CO (inadequate diastolic filling) |
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
Important caveat: At very high heart rates, diastolic filling time is shortened, reducing EDV and therefore SV - so CO may actually fall despite a high HR.
2. Preload (Frank-Starling Mechanism)
Preload = ventricular end-diastolic volume (EDV) - the stretch on myocardial fibers just before systole. It is the main determinant of stroke volume through the Frank-Starling law.
"The Frank-Starling law of the heart states that the volume of blood ejected by the ventricle depends on the volume present in the ventricle at the end of diastole... Stroke volume and cardiac output correlate directly with end-diastolic volume, which correlates with venous return."
- Costanzo Physiology, 7th Ed.
Factors that increase preload (and thus CO):
| Factor | Mechanism |
|---|---|
| ↑ Blood volume (e.g., IV fluids) | ↑ Venous return |
| Venoconstriction (sympathetic) | ↑ Venous return |
| Supine posture / leg raising | ↑ Venous return |
| Slow heart rate | More diastolic filling time |
| Normal atrial contraction | Boosts EDV by 20-30% ("atrial kick") |
Factors that decrease preload:
- Hemorrhage/dehydration
- Positive-pressure ventilation (impairs venous return)
- Pericardial tamponade / constrictive pericarditis
- Atrial fibrillation (loss of atrial kick)
- Tachycardia
"The heart cannot pump what the heart does not receive; therefore, venous return normally equals cardiac output."
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
3. Afterload
Afterload = the resistance against which the ventricle must eject blood - for the left ventricle, this is primarily aortic pressure and systemic vascular resistance (SVR).
"Afterload is the resistance against which the heart must pump blood and is the result of aortic impedance and systemic vascular resistance. Systolic blood pressure is the clinically accessible measure of afterload."
- Katzung's Basic & Clinical Pharmacology, 16th Ed.
- ↑ Afterload (e.g., hypertension, aortic stenosis) → ↑ wall stress → ↓ fiber shortening → ↓ SV → ↓ CO
- ↓ Afterload (e.g., vasodilators) → ↑ SV → ↑ CO
Afterload is formally described by Laplace's Law:
Wall tension = (Intraventricular pressure × Ventricular radius) / (2 × Wall thickness)
So a dilated ventricle faces higher afterload at the same aortic pressure - explaining why cardiac dilation in heart failure further reduces CO.
| ↑ Afterload causes | ↓ Afterload causes |
|---|---|
| Hypertension, aortic stenosis | Vasodilators (nitroprusside, ACEi) |
| Vasoconstriction (septic shock compensation) | Septic shock (distributive phase) |
| Aortic cross-clamping | Neuraxial anesthesia |
4. Myocardial Contractility (Inotropy)
Contractility = the intrinsic ability of the myocardium to generate force, independent of preload and afterload. It reflects the vigor of Ca²⁺-mediated cross-bridge cycling.
"Agents that increase contractility have a positive inotropic effect... produce increases in stroke volume and cardiac output for a given end-diastolic volume. The result is that a larger fraction of the end-diastolic volume is ejected per beat and there is an increase in ejection fraction."
- Costanzo Physiology, 7th Ed.
Factors affecting contractility (from Harrison's, 22nd Ed.):
| ↑ Contractility (Positive Inotropes) | ↓ Contractility (Negative Inotropes) |
|---|---|
| Sympathetic stimulation (β1) | Myocardial ischemia / infarction |
| Circulating catecholamines | Beta-blockers, calcium channel blockers |
| Digoxin, dopamine, dobutamine | Acidosis, hypoxia |
| ↑ Heart rate (Bowditch/treppe effect) | Cardiomyopathy |
| Hypercalcemia | Myocardial fibrosis |
Frank-Starling Curves and Contractility Interaction
The figure below shows how all these factors interact. Each curve represents a different contractile state. For any given preload (EDV on x-axis), higher contractility shifts the curve upward (more CO). Heart failure patients operate on lower, flatter curves.
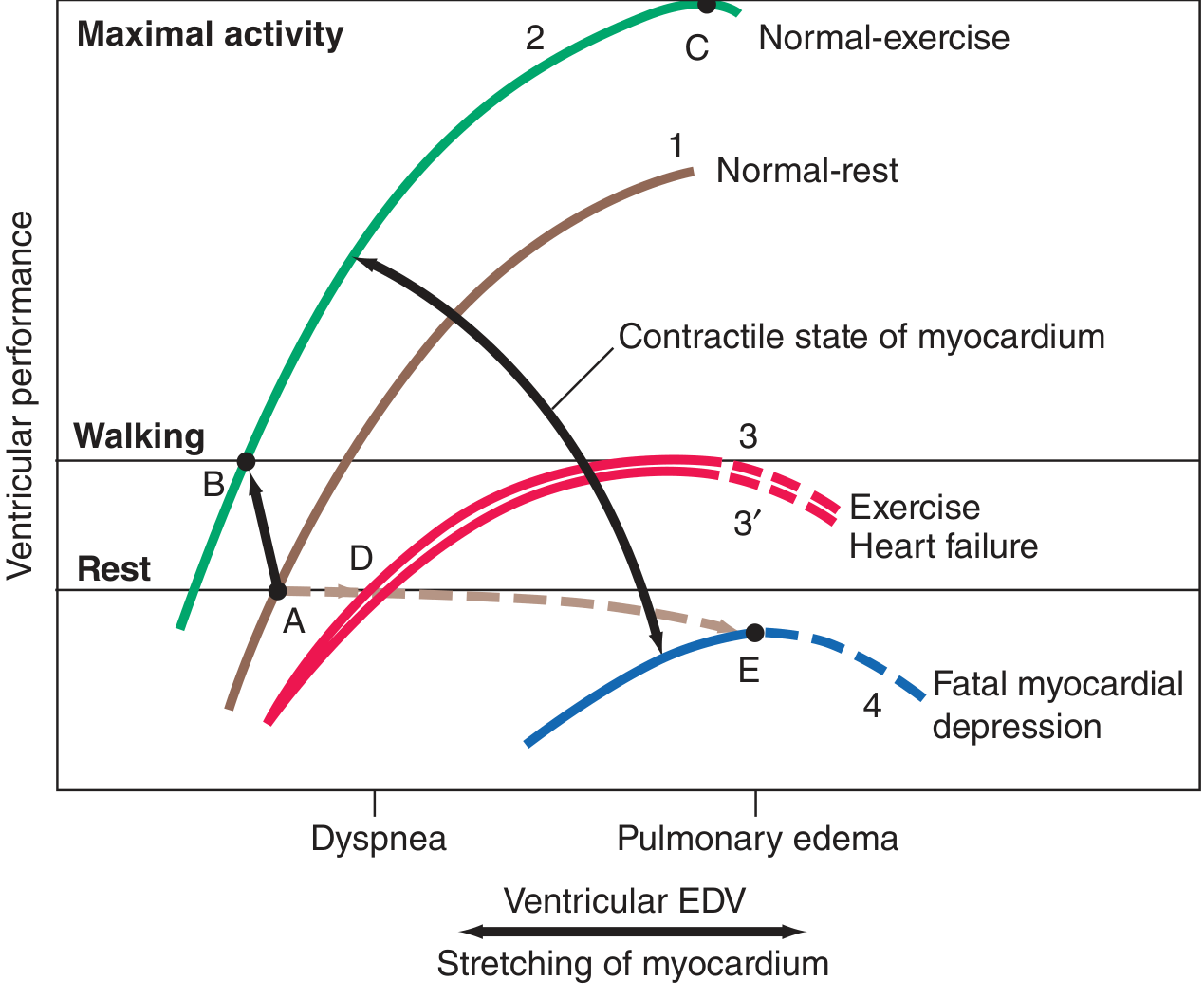
Frank-Starling curves showing ventricular performance vs. EDV across different myocardial states - Harrison's Principles, 22nd Ed.
Summary Table
| Factor | Effect on CO if Increased | Key Modifier |
|---|---|---|
| Heart Rate | ↑ (up to ~120 bpm, then ↓) | ANS, catecholamines |
| Preload (EDV) | ↑ (via Frank-Starling) | Venous return, blood volume |
| Afterload (SVR/aortic pressure) | ↓ | Vascular resistance |
| Contractility | ↑ | Sympathetics, inotropes, Ca²⁺ |
Sources: Costanzo Physiology 7th Ed. · Morgan & Mikhail's Clinical Anesthesiology 7th Ed. · Miller's Anesthesia 10th Ed. · Harrison's Principles of Internal Medicine 22nd Ed. · Katzung's Basic & Clinical Pharmacology 16th Ed.
Explain methods of cardiac output
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.