Write me about rectus sheath for mbbs exam long answer and also give diagrams if possible.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Let me compose the comprehensive MBBS long answer on the rectus sheath.
Rectus Sheath
Introduction
The rectus sheath is an aponeurotic compartment on the anterior abdominal wall that encloses the rectus abdominis and pyramidalis muscles. It is formed by the interlacing aponeuroses of the three flat muscles of the lateral abdominal wall (external oblique, internal oblique, and transversus abdominis) and has a composition that differs characteristically above and below the arcuate line. Its understanding is fundamental to abdominal surgery, hernia repair, and regional anaesthesia.
Formation of the Rectus Sheath
The sheath is formed by the aponeuroses of:
- External oblique
- Internal oblique (splits into anterior and posterior lamellae at the lateral edge of rectus abdominis)
- Transversus abdominis
Above the Arcuate Line (Upper 3/4)
| Wall | Composition |
|---|---|
| Anterior wall | Aponeurosis of external oblique + anterior lamella of internal oblique aponeurosis |
| Posterior wall | Posterior lamella of internal oblique aponeurosis + aponeurosis of transversus abdominis |
Below the Arcuate Line (Lower 1/4)
At a point midway between the umbilicus and the pubic symphysis, all three aponeuroses pass anterior to the rectus abdominis:
| Wall | Composition |
|---|---|
| Anterior wall | Aponeuroses of all three muscles (external oblique + internal oblique + transversus abdominis) |
| Posterior wall | Absent - rectus abdominis lies directly on transversalis fascia |
Key point: The aponeuroses of the three lateral abdominal muscles contribute equally to the anterior and posterior layers of the sheath above the umbilicus. The two layers blend together approximately 3-5 cm below the umbilicus (at the arcuate line) to form a single, more stable anterior sheet.
Diagram 1 - Cross-sections of the Rectus Sheath (Gray's Anatomy for Students, Fig. 4.33)
(A) = Above arcuate line | (B) = Below arcuate line
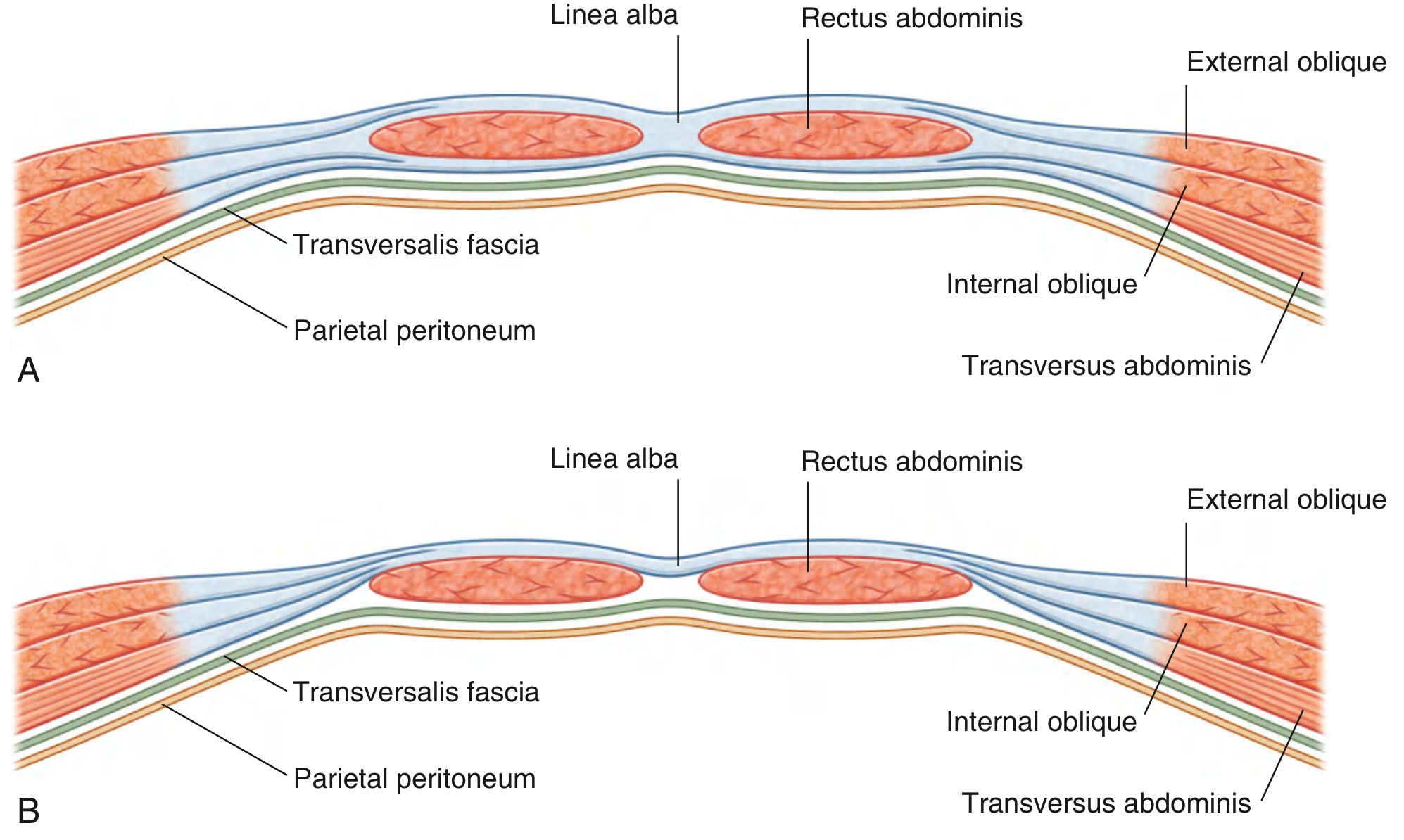
Diagram 2 - Thieme Atlas Cross-Section (showing all named layers)
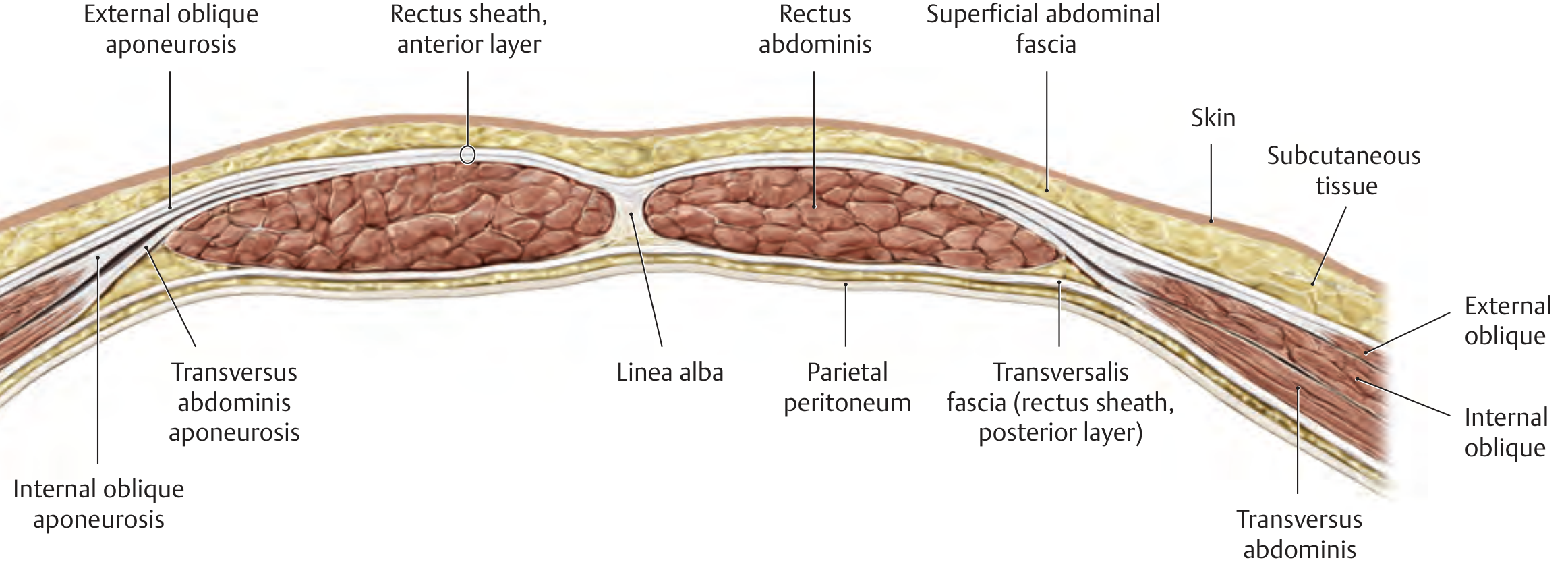
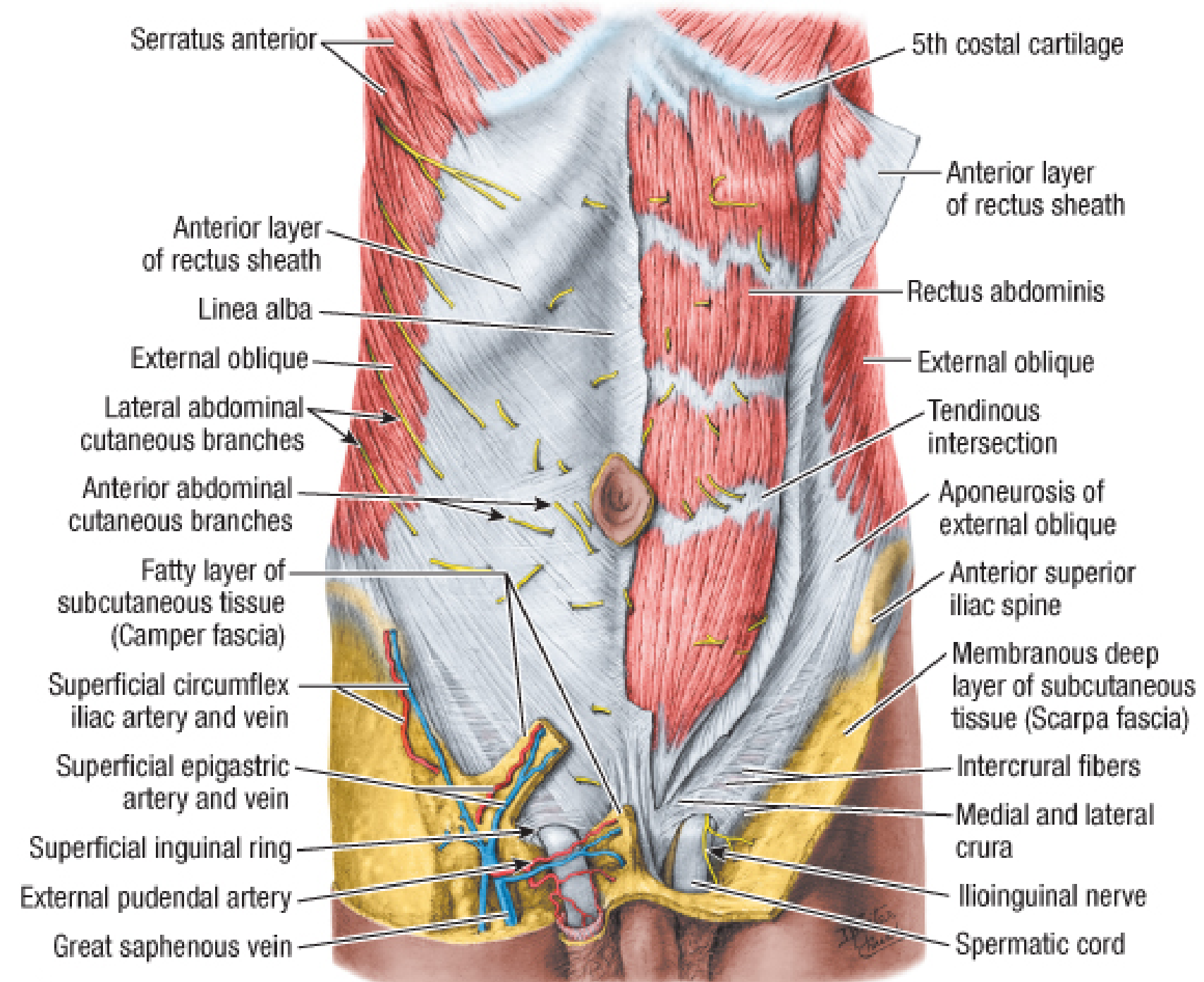
Diagram 3 - Anterior Abdominal Wall with Anterior Layer of Rectus Sheath (Fischer's Mastery of Surgery)
The Arcuate Line (Linea Semicircularis / Line of Douglas)
- Lies midway between the umbilicus and pubic symphysis
- Marks the lower free border of the posterior rectus sheath
- Below this line, the posterior sheath is absent
- The inferior epigastric vessels and their branches are relatively fixed at this level, making them vulnerable to shearing forces
- It is the site of Spigelian hernia when combined with the linea semilunaris
The Linea Semilunaris
- The lateral edge of the rectus sheath
- Visible on the anterior abdominal wall as a curved linear depression lateral to each rectus abdominis
- Formed by the fusion of the aponeuroses at the lateral border of the rectus abdominis muscle
- Clinically important as the site of Spigelian hernia (hernia through the aponeurosis lateral to the rectus at the level of the arcuate line)
Contents of the Rectus Sheath
The rectus sheath encloses the following structures:
- Rectus abdominis muscle (paired, longitudinal)
- Pyramidalis muscle (small triangular muscle, may be absent; anterior to rectus abdominis, base on pubis, apex attached to linea alba)
- Superior epigastric artery and veins - terminal branch of internal thoracic artery; enters the sheath below the costal margin
- Inferior epigastric artery and veins - branch of external iliac artery; enters the sheath below the arcuate line
- Anastomosis between superior and inferior epigastric vessels within the sheath
- Lymphatic vessels
- Thoracoabdominal and subcostal nerves - anterior rami of spinal nerves T7 to T12 (lower intercostal nerves enter the sheath laterally and supply segmental innervation)
Blood Supply of Rectus Abdominis (Within the Sheath)
- Superior epigastric artery: terminal branch of internal thoracic artery; enters sheath by passing posterior to the 7th costal cartilage
- Inferior epigastric artery: branch of external iliac artery; enters the sheath below the arcuate line from laterally
- The two arteries anastomose within the substance of the rectus abdominis, providing a rich blood supply
- This anastomosis is used in the TRAM (Transverse Rectus Abdominis Myocutaneous) flap for breast reconstruction
Nerve Supply (Within the Sheath)
- Anterior rami of T7-T12 (thoracoabdominal nerves) and the subcostal nerve (T12)
- They enter the lateral aspect of the sheath by piercing the posterior layer and run between the rectus abdominis and the posterior wall of the sheath
- They supply motor innervation to the rectus and pyramidalis and provide segmental cutaneous supply to the overlying skin
Related Structures
| Structure | Relation |
|---|---|
| Linea alba | Medial fusion of the two sheaths at the midline |
| Transversalis fascia | Forms the posterior "wall" below the arcuate line |
| Preperitoneal fat | Between transversalis fascia and parietal peritoneum |
| Parietal peritoneum | Deep to preperitoneal fat |
Clinical Significance
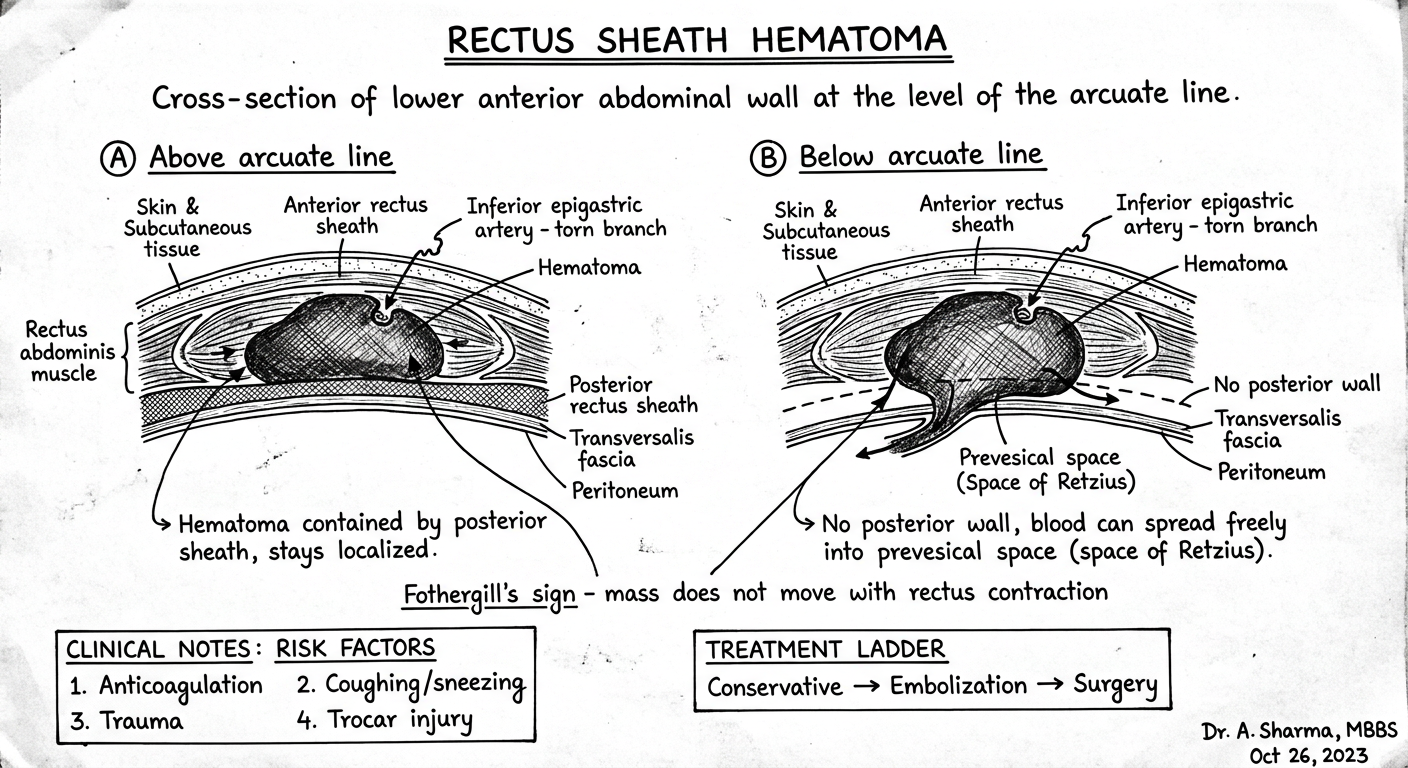
1. Rectus Sheath Hematoma
- Caused by disruption of branches of the inferior epigastric artery
- Most common around the arcuate line, where the artery and its branches are relatively fixed and vulnerable to shearing forces
- Risk factors: Trauma, vigorous coughing/sneezing, exercise, anticoagulation therapy, chronic pulmonary disease (coughing fits), laparoscopic trocar injury
- Presentation: Acute abdominal pain + palpable abdominal wall mass
- May mimic intraperitoneal pathology (e.g., appendicitis on the right)
- Fothergill's sign: A mass that does not change in position with contraction of the rectus muscle (distinguishes from intraperitoneal masses)
- Diagnosis: Ultrasound or CT scan with IV contrast
- Management:
- Small/stable hematoma: conservative (bed rest, compression, reverse anticoagulation)
- Expanding or large hematoma: hospitalization, serial Hb/Hct
- Hemodynamic instability: aggressive resuscitation + angiographic embolization
- Surgical evacuation + vessel ligation if angiography fails
2. Spigelian Hernia
- Hernia through the Spigelian fascia at the junction of the arcuate line and linea semilunaris
- Typically presents as an intermittent lateral abdominal mass
- Diagnosis by USS or CT; treated surgically
3. Rectus Abdominis Diastasis (Diastasis Recti)
- Abnormal separation of the rectus muscles with laxity of the linea alba (>2 cm is abnormal)
- Not a true hernia (fascia is intact; no strangulation risk)
- Risk factors: obesity, pregnancy, connective tissue disorders
- Presents as a fusiform midline bulge that worsens with Valsalva maneuver
- Management: weight loss, exercise; surgery (plication of sheath) for symptomatic cases
4. Surgical Access
- The rectus sheath is opened in paramedian incisions and Pfannenstiel incisions
- Knowledge of the sheath's layers guides safe entry into the peritoneal cavity and avoids injury to the epigastric vessels
5. TRAM Flap and DIEP Flap
- The superior epigastric artery pedicle within the sheath is used for the TRAM flap in breast reconstruction
- The DIEP (Deep Inferior Epigastric Perforator) flap preserves the rectus muscle by using perforators of the inferior epigastric artery
6. Rectus Sheath Block (Regional Anaesthesia)
- Local anaesthetic is deposited between the rectus abdominis and the posterior rectus sheath under ultrasound guidance
- Provides analgesia for midline abdominal incisions by blocking the anterior rami of T7-T12
Summary Table
| Feature | Above Arcuate Line | Below Arcuate Line |
|---|---|---|
| Anterior wall | External oblique + ant. lamella of internal oblique | All three aponeuroses |
| Posterior wall | Post. lamella of internal oblique + transversus abdominis | Absent |
| Posterior covering | Posterior rectus sheath | Transversalis fascia only |
| Location | Upper 3/4 of rectus | Lower 1/4 of rectus |
Exam Tip
The single most commonly tested fact is the difference in composition above vs. below the arcuate line. Remember: below the arcuate line, all aponeuroses go to the front and the posterior wall of the sheath is absent - leaving only transversalis fascia covering the posterior surface of rectus abdominis. This also explains why rectus sheath hematomas tend to be larger and more dangerous below the arcuate line (no posterior wall to limit spread).
Sources: Gray's Anatomy for Students (Fig. 4.33); THIEME Atlas of General Anatomy and Musculoskeletal System; Fischer's Mastery of Surgery, 8e; Schwartz's Principles of Surgery, 11e; Sabiston Textbook of Surgery
Can you give some handwritten diagrams for better representation in exam.
Generating Image
Generating Image
Generating Image
Generating Image
Generating Image
Here are all 5 handwritten-style diagrams for your MBBS exam:
Diagram 1 - Cross-section: Above the Arcuate Line
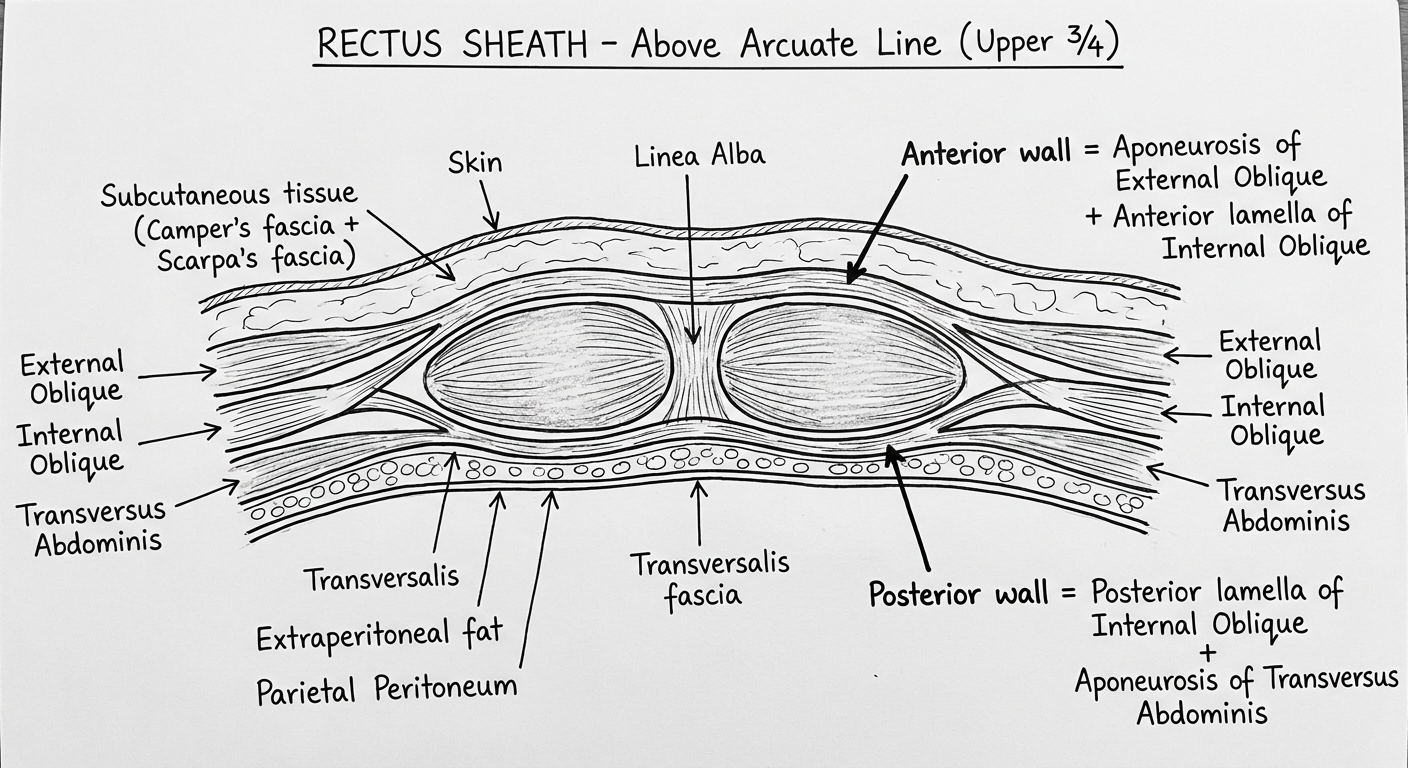
Diagram 2 - Cross-section: Below the Arcuate Line
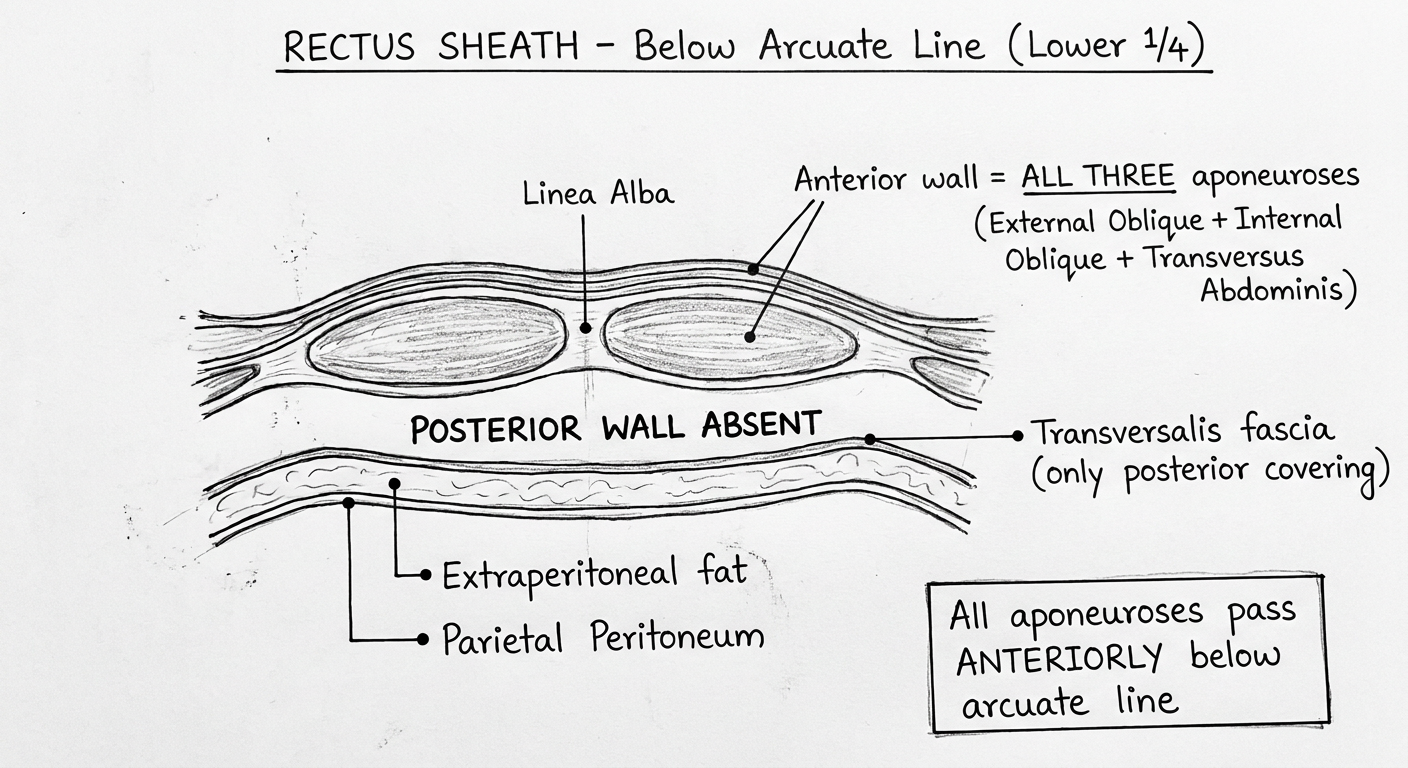
Diagram 3 - Anterior View: Rectus Sheath & Related Structures
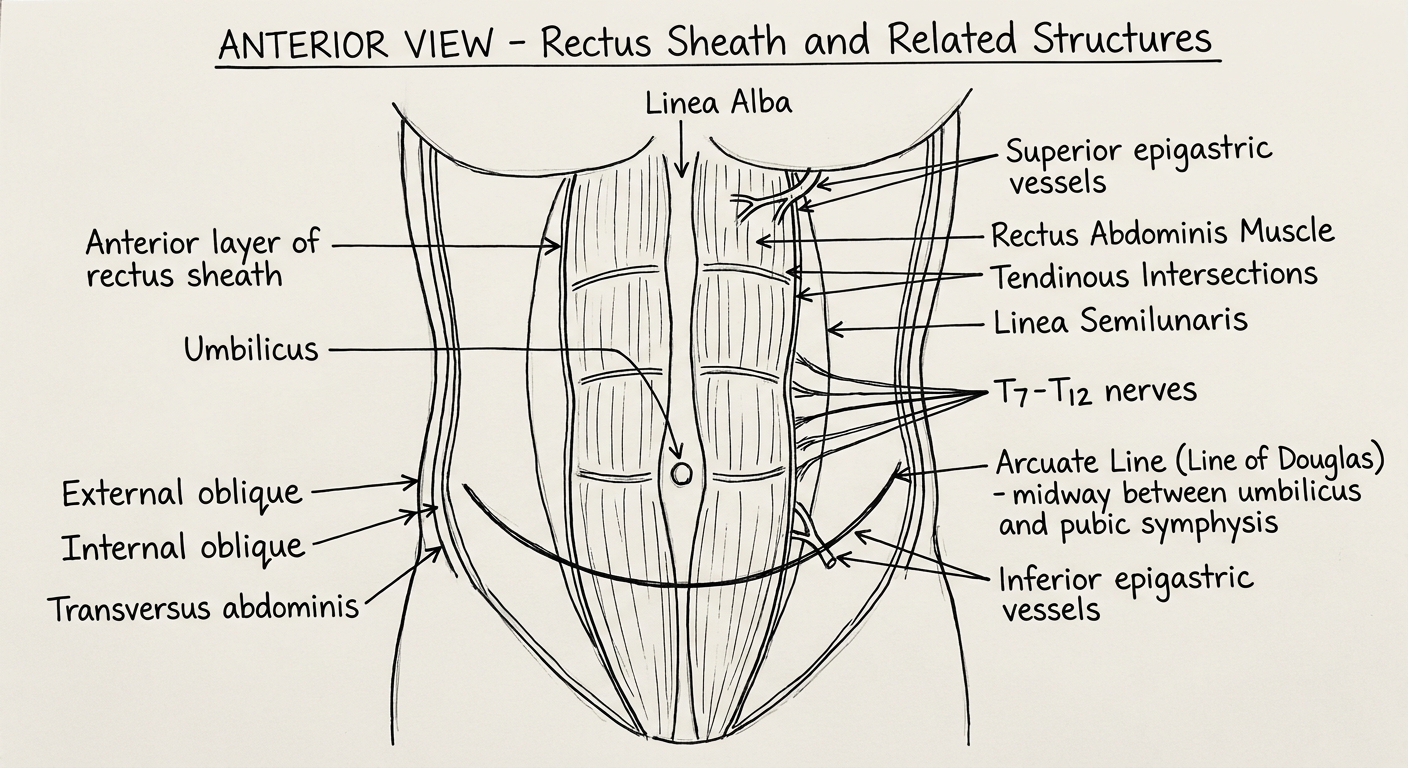
Diagram 4 - Comparison Table: Above vs Below Arcuate Line
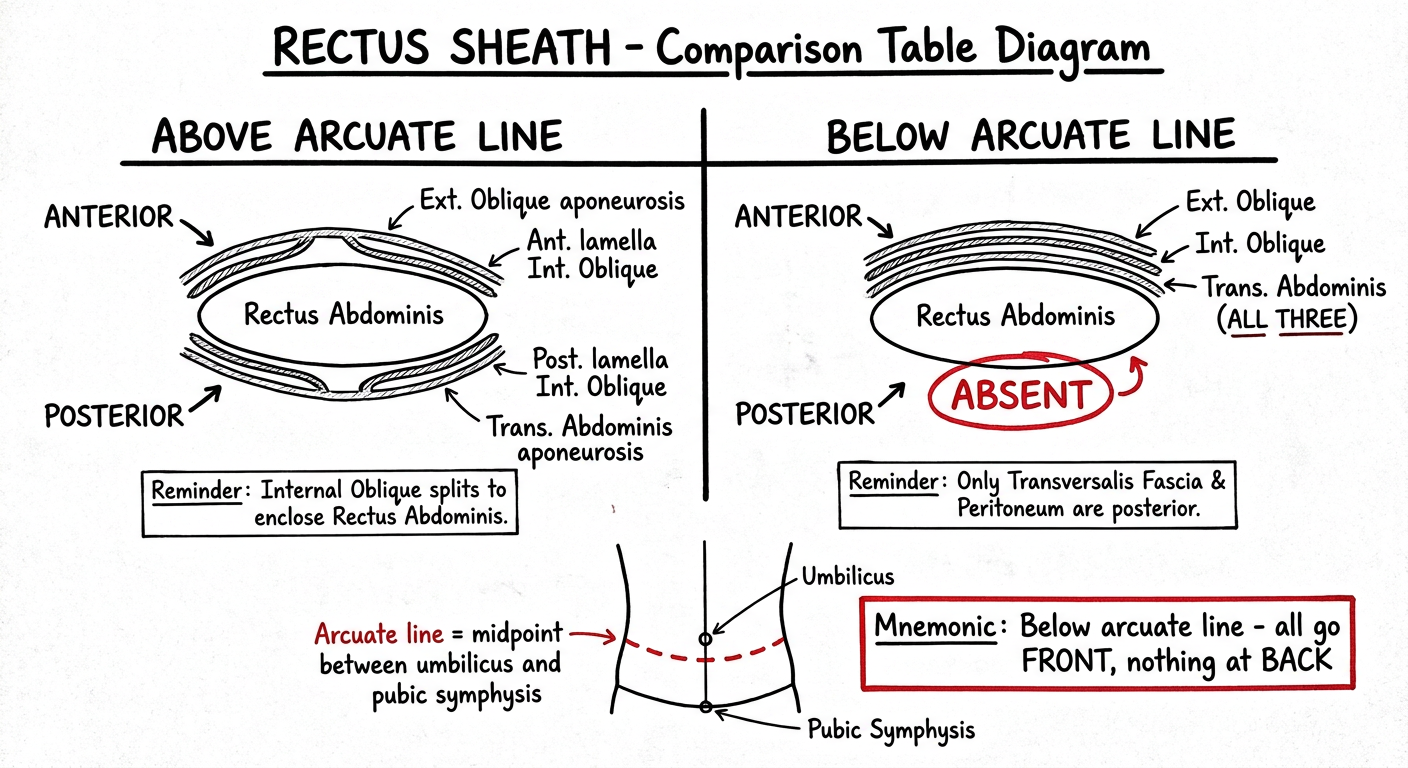
Diagram 5 - Clinical: Rectus Sheath Hematoma
How to Use These in Exams
| Diagram | When to Draw |
|---|---|
| Diagrams 1 & 2 | For any question on formation/composition of sheath |
| Diagram 3 | For questions on contents, arcuate line, linea semilunaris |
| Diagram 4 | Quick reference table within the answer |
| Diagram 5 | If the question asks clinical importance or applied anatomy |
Exam tip: In a long answer, always draw Diagram 1+2 together (above and below arcuate line side by side) - examiners love seeing that comparison. Then draw Diagram 3 for contents and follow it with clinical significance. That structure alone will fetch you maximum marks.
This is a shared conversation. Sign in to Orris to start your own chat.