Swelling is possible due to what all medical reasons and how to diagnose what will it indicate
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Swelling (Edema): Medical Causes, Diagnosis, and Clinical Significance
Swelling - clinically called edema - is the accumulation of excess fluid in the interstitial space. It results from disruption of the normal balance of forces that govern fluid movement between capillaries, interstitium, and lymphatics. Understanding the mechanism behind swelling directly points to the underlying diagnosis.
The Four Pathophysiologic Mechanisms
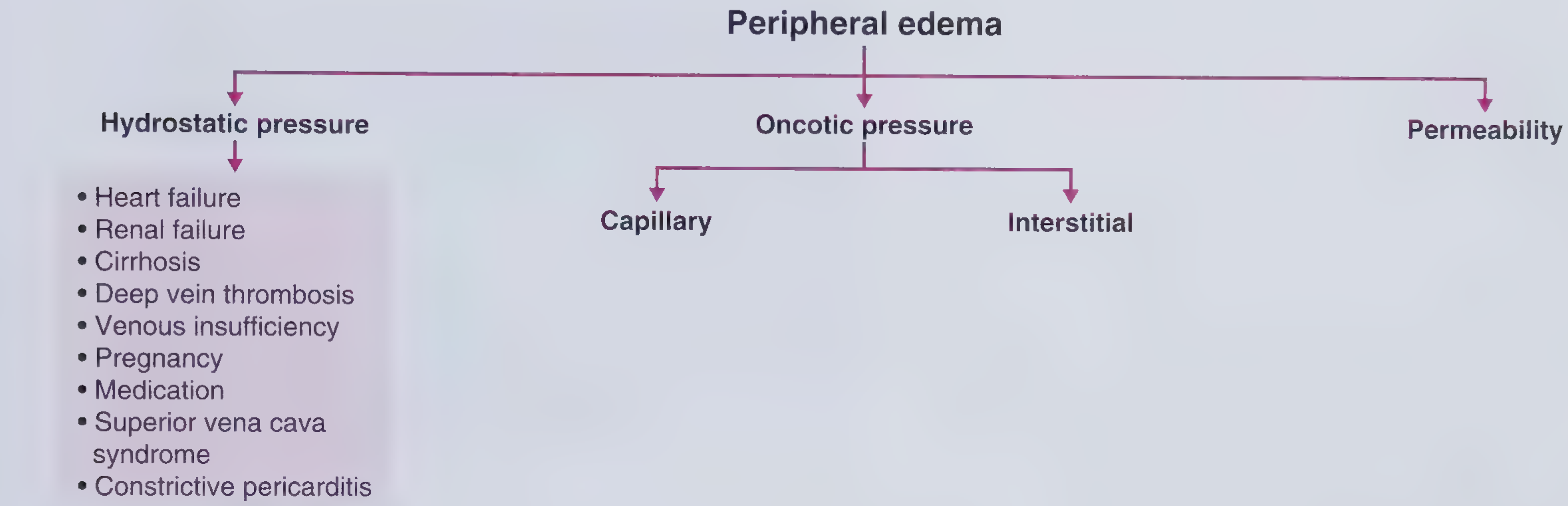
1. Increased Capillary Hydrostatic Pressure
Fluid is pushed out of capillaries into the interstitium when venous/capillary back-pressure rises.
| Cause | Key Features |
|---|---|
| Heart failure (right or congestive) | Bilateral, dependent, pitting; worsens by evening; associated with raised JVP, S3 gallop, dyspnea, orthopnea |
| Renal failure (acute or chronic) | Generalized pitting edema; associated with hypertension, uremic symptoms, elevated creatinine |
| Hepatic cirrhosis | Ascites + peripheral edema; spider angiomas, jaundice, low BP, hypoalbuminemia |
| Deep vein thrombosis (DVT) | Unilateral leg swelling, pain, erythema, warmth |
| Chronic venous insufficiency | Bilateral lower leg edema; medial malleolus ulcers; affects women of reproductive age |
| Pregnancy | Due to uterine compression of inferior vena cava + hormonal effects |
| Superior vena cava (SVC) syndrome | Edema confined to face, neck, and upper extremities; caused by central obstruction (lung cancer, thrombus) |
| Constrictive pericarditis | Elevated JVP + Kussmaul's sign + early diastolic extra heart sound |
| Medications | Calcium channel blockers (amlodipine), steroids (glucocorticoids, estrogens, anabolic steroids), vasodilators, cyclosporine |
| Paralysis / immobilization | Failure of the muscle venous pump - unilateral edema on affected side |
| Mineralocorticoid excess | Salt/water retention by kidneys |
- Frameworks for Internal Medicine, p. 307
- Guyton and Hall Textbook of Medical Physiology, p. 320
2. Decreased Capillary Oncotic Pressure (Low Plasma Proteins)
When albumin falls, less fluid is held inside capillaries - it leaks out.
| Cause | Key Features |
|---|---|
| Nephrotic syndrome | Periorbital puffiness (prominent in morning), generalized edema; proteinuria ≥3.5 g/day, hypoalbuminemia, hypercholesterolemia |
| Hepatic cirrhosis / liver failure | Reduced albumin synthesis; Terry's nails (white opacification) may be present |
| Protein-calorie malnutrition (Kwashiorkor) | Muscle atrophy, hollow temples, rib protrusion, peripheral edema in children |
| Protein-losing enteropathy | Protein lost via gut; can be due to IBD, lymphangiectasia, severe gastroenteritis |
| Burns / large wounds | Protein lost through denuded skin |
- Harrison's Principles of Internal Medicine 22E, p. 325
- Frameworks for Internal Medicine, p. 309
3. Increased Capillary Permeability
Capillary walls become "leaky" due to inflammation, immune activation, or toxins.
| Cause | Key Features |
|---|---|
| Local inflammation (trauma, cellulitis, burns, insect stings) | Localized, nonpitting edema; associated with erythema, pain, warmth |
| Allergic reaction / Anaphylaxis | Angioedema - nondependent, nonpitting; lips, tongue, periorbital, hands, genitalia; mediated by histamine |
| ACE inhibitor-induced angioedema | Bradykinin-mediated; does NOT respond to antihistamines; can be life-threatening if laryngeal |
| Preeclampsia | Hypertension + proteinuria + edema at ≥20 weeks gestation; endothelial dysfunction is the mechanism |
| Sepsis / severe infection | Cytokine storm increases permeability systemically |
| Systemic capillary leak syndrome | Rare; recurrent episodes of hypotension, hemoconcentration, edema |
| Idiopathic edema | Women; unexplained face/hand/leg swelling; diuretic misuse often complicates it |
| Vitamin C deficiency (Scurvy) | Impairs collagen in vessel walls |
| Prolonged ischemia / reperfusion injury | Tissue injury increases local capillary permeability |
- Frameworks for Internal Medicine, p. 312-313
- Guyton and Hall, p. 320
4. Lymphatic Obstruction (Increased Interstitial Oncotic Pressure)
When lymphatics are blocked, protein-rich fluid accumulates in interstitium, raising interstitial oncotic pressure - creating a self-perpetuating edema.
| Cause | Key Features |
|---|---|
| Malignant lymphatic obstruction (lymphoma, metastatic cancer) | Unilateral; ipsilateral to obstruction; skin becomes thickened/darkened over time (lymphostatic verrucosis) |
| Filariasis (Wuchereria bancrofti) | Parasitic infection; worldwide - most common infectious cause of lymphedema |
| Post-surgical lymphedema | Axillary dissection after breast cancer surgery; arm swelling |
| Radiation treatment | Lymphatic fibrosis after radiation |
| Primary (congenital) lymphedema | Absent or abnormal lymphatic vessels; intractable |
| Hypothyroidism (Myxedema) | Nonpitting bilateral lower extremity edema; glycosaminoglycan deposition; associated with dry hair, constipation, bradycardia, weight gain |
| Graves' disease (pretibial myxedema) | Bilateral, asymmetric, nonpitting, nondependent edema over pretibial region |
- Harrison's Principles of Internal Medicine 22E, p. 325
- Frameworks for Internal Medicine, p. 310-311
Distribution of Edema: A Diagnostic Clue
The location of swelling is one of the most important guides to the cause:
| Distribution | Think of |
|---|---|
| Bilateral lower extremity, dependent, worsens evening | Heart failure, venous insufficiency, bilateral DVT |
| Periorbital, facial, worst in morning | Nephrotic syndrome, renal disease, angioedema |
| Ascites + leg edema | Cirrhosis, heart failure, nephrotic syndrome |
| Unilateral leg swelling | DVT, lymphedema, cellulitis, popliteal cyst rupture |
| Face, neck, arms only | SVC syndrome |
| Pretibial only, nonpitting | Graves' dermopathy |
| Generalized nonpitting | Myxedema (hypothyroidism) |
| Localized + warm + red | Infection, inflammation, allergy |
- Harrison's Principles of Internal Medicine 22E
Diagnostic Approach
History
- Onset: Sudden (DVT, angioedema) vs. gradual (heart failure, nephrotic syndrome)
- Bilaterality: Unilateral = local cause; bilateral = systemic
- Pitting vs. nonpitting: Pitting = fluid (cardiac, renal, hepatic); nonpitting = protein/myxedema/lymphedema
- Time of day: Evening = cardiac/venous; morning = renal/nephrotic
- Associated symptoms: Dyspnea (cardiac), jaundice (hepatic), proteinuria/frothy urine (nephrotic), weight gain/hair loss (thyroid), recent DVT risk factors
- Medications: CCBs, steroids, NSAIDs, ACE inhibitors
Physical Examination
- Pitting test: Press firmly over the tibia for 5 seconds - an indentation (pit) that persists indicates pitting edema
- JVP: Elevated = cardiac or pericardial cause
- Liver size: Hepatomegaly = right heart failure or cirrhosis
- Ascites: Cirrhosis, heart failure, nephrotic syndrome
- Skin signs: Spider angiomas, jaundice, palmar erythema = liver; pretibial thickening = myxedema; erythema, warmth = inflammation
Key Investigations
| Investigation | What it tells you |
|---|---|
| Serum albumin | Low = nephrotic syndrome, cirrhosis, malnutrition |
| Urine protein (spot protein:creatinine or 24-hour) | Proteinuria ≥3.5 g/day = nephrotic syndrome |
| BNP / NT-proBNP | Elevated = heart failure |
| Serum creatinine, BUN | Elevated = renal disease |
| Liver enzymes (ALT, AST, bilirubin, PT/INR) | Abnormal = hepatic cause |
| TSH, Free T4 | Low TSH + high T4 = hyperthyroid; High TSH + low T4 = hypothyroid (myxedema) |
| ECG + Echocardiogram | Cardiac structure and function |
| Duplex ultrasound (venous) | DVT, venous insufficiency |
| CBC | Anemia can indicate chronic disease or heart failure |
| Serum electrolytes | Hyponatremia = severe heart failure; hyperkalemia = renal failure |
| Chest X-ray | Pulmonary edema, cardiomegaly, pleural effusion |
| ANA, complement, ANCA | If glomerulonephritis suspected (edema + hematuria + proteinuria) |
Quick Summary: Edema Type vs. Diagnosis
| Edema Type | Most Likely Cause |
|---|---|
| Bilateral pitting + raised JVP + dyspnea | Heart failure |
| Bilateral pitting + periorbital + frothy urine | Nephrotic syndrome |
| Bilateral pitting + jaundice + ascites + spider angiomas | Cirrhosis |
| Unilateral + acute + painful + warm | DVT or cellulitis |
| Nonpitting + bilateral + bradycardia + dry skin | Hypothyroidism |
| Unilateral + chronic + thickened skin | Lymphedema |
| Face/lips/throat swelling + urticaria | Allergic angioedema |
| Face/arm swelling + no hives + on ACE inhibitor | ACE inhibitor angioedema |
| Lower leg edema + hypertension + proteinuria in pregnancy | Preeclampsia |
Sources:
- Harrison's Principles of Internal Medicine 22E - Chapter 43: Edema
- Guyton and Hall Textbook of Medical Physiology - Chapter on Extracellular Fluid Regulation
- Frameworks for Internal Medicine - Peripheral Edema Framework (p. 307-313)
Create a diagnostic flowchart PDF for swelling workup
Reading File
Running Command
mkdir -p /home/daytona/workspace/swelling-flowchart && ls /home/daytona/workspac…
Writing File
~/swelling-flowchart/generate_flowchart.py
from reportlab.lib.pagesizes import A3, landscape
from reportlab.lib import colors
from reportlab.lib.units import mm
from reportlab.pdfgen import canvas
from reportlab.lib.utils import simpleSplit
OUTPUT = "/home/daytona/workspace/swelling-flowchart/Swelling_Diagnostic_Flowchart.pdf"
# ── palette ──────────────────────────────────────────────────────────────────
C_TITLE_BG = colors.HexColor("#1A237E") # deep navy
C_TITLE_FG = colors.white
C_START_BG = colors.HexColor("#283593") # indigo
C_STEP_BG = colors.HexColor("#1565C0") # dark blue
C_STEP_FG = colors.white
C_DIAMOND_BG = colors.HexColor("#FF6F00") # amber – decision nodes
C_DIAMOND_FG = colors.white
C_LEAF_BG = {
"cardiac": colors.HexColor("#C62828"),
"renal": colors.HexColor("#4527A0"),
"hepatic": colors.HexColor("#1B5E20"),
"nephrotic": colors.HexColor("#0D47A1"),
"thyroid": colors.HexColor("#006064"),
"lymph": colors.HexColor("#1A237E"),
"dvt": colors.HexColor("#B71C1C"),
"venous": colors.HexColor("#880E4F"),
"allergy": colors.HexColor("#E65100"),
"local": colors.HexColor("#4E342E"),
"precl": colors.HexColor("#558B2F"),
"medic": colors.HexColor("#37474F"),
}
C_ARROW = colors.HexColor("#37474F")
C_LINE = colors.HexColor("#B0BEC5")
C_BG = colors.HexColor("#F0F4FF")
C_SECTION_LINE = colors.HexColor("#90A4AE")
# ── helpers ──────────────────────────────────────────────────────────────────
def draw_rounded_box(c, x, y, w, h, fill, text_lines, font="Helvetica-Bold",
fsize=7.5, text_color=colors.white, radius=4, border_color=None):
c.setFillColor(fill)
if border_color:
c.setStrokeColor(border_color)
c.setLineWidth(1)
else:
c.setStrokeColor(fill)
c.setLineWidth(0.5)
c.roundRect(x, y, w, h, radius, fill=1, stroke=1)
c.setFillColor(text_color)
c.setFont(font, fsize)
total_h = len(text_lines) * (fsize + 1.5)
start_y = y + h/2 + total_h/2 - fsize
for i, line in enumerate(text_lines):
lw = c.stringWidth(line, font, fsize)
c.drawString(x + w/2 - lw/2, start_y - i*(fsize+1.5), line)
def draw_diamond(c, cx, cy, hw, hh, fill, lines, fsize=7):
c.setFillColor(fill)
c.setStrokeColor(colors.white)
c.setLineWidth(0.8)
path = c.beginPath()
path.moveTo(cx, cy + hh)
path.lineTo(cx + hw, cy)
path.lineTo(cx, cy - hh)
path.lineTo(cx - hw, cy)
path.close()
c.drawPath(path, fill=1, stroke=1)
c.setFillColor(colors.white)
c.setFont("Helvetica-Bold", fsize)
total_h = len(lines) * (fsize + 1.5)
sy = cy + total_h/2 - fsize
for i, line in enumerate(lines):
lw = c.stringWidth(line, "Helvetica-Bold", fsize)
c.drawString(cx - lw/2, sy - i*(fsize+1.5), line)
def arrow(c, x1, y1, x2, y2, label="", color=C_ARROW):
c.setStrokeColor(color)
c.setLineWidth(1.2)
c.line(x1, y1, x2, y2)
# arrowhead
import math
ang = math.atan2(y2-y1, x2-x1)
al = 5
aw = 3
c.setFillColor(color)
p = c.beginPath()
p.moveTo(x2, y2)
p.lineTo(x2 - al*math.cos(ang) + aw*math.sin(ang),
y2 - al*math.sin(ang) - aw*math.cos(ang))
p.lineTo(x2 - al*math.cos(ang) - aw*math.sin(ang),
y2 - al*math.sin(ang) + aw*math.cos(ang))
p.close()
c.drawPath(p, fill=1, stroke=0)
if label:
c.setFillColor(C_ARROW)
c.setFont("Helvetica-Bold", 6.5)
mx, my = (x1+x2)/2, (y1+y2)/2
c.drawString(mx+2, my+2, label)
def horiz_line(c, x1, x2, y, color=C_SECTION_LINE):
c.setStrokeColor(color)
c.setLineWidth(0.5)
c.setDash(3, 3)
c.line(x1, y, x2, y)
c.setDash()
# ── page setup ───────────────────────────────────────────────────────────────
W, H = landscape(A3) # 420 × 297 mm
c = canvas.Canvas(OUTPUT, pagesize=(W, H))
# background
c.setFillColor(C_BG)
c.rect(0, 0, W, H, fill=1, stroke=0)
# thin border
c.setStrokeColor(C_TITLE_BG)
c.setLineWidth(2)
c.rect(4, 4, W-8, H-8, fill=0, stroke=1)
# ── TITLE BAR ────────────────────────────────────────────────────────────────
c.setFillColor(C_TITLE_BG)
c.rect(4, H-38, W-8, 34, fill=1, stroke=0)
c.setFillColor(colors.white)
c.setFont("Helvetica-Bold", 17)
title = "DIAGNOSTIC FLOWCHART: SWELLING / EDEMA WORKUP"
c.drawString(W/2 - c.stringWidth(title,"Helvetica-Bold",17)/2, H-23, title)
c.setFont("Helvetica", 8)
sub = "Based on Harrison's Principles of Internal Medicine 22E | Guyton & Hall | Frameworks for Internal Medicine"
c.setFillColor(colors.HexColor("#B3C0FF"))
c.drawString(W/2 - c.stringWidth(sub,"Helvetica",8)/2, H-33, sub)
# ── LEGEND ───────────────────────────────────────────────────────────────────
LX = W - 105
LY = H - 115
c.setFillColor(colors.white)
c.setStrokeColor(C_LINE)
c.setLineWidth(0.5)
c.roundRect(LX-4, LY-6, 104, 72, 4, fill=1, stroke=1)
c.setFont("Helvetica-Bold", 7.5)
c.setFillColor(C_TITLE_BG)
c.drawString(LX+18, LY+58, "LEGEND")
legend_items = [
(C_STEP_BG, "Assessment Step"),
(C_DIAMOND_BG, "Decision / Question"),
(colors.HexColor("#C62828"), "Cardiac Diagnosis"),
(colors.HexColor("#4527A0"), "Renal Diagnosis"),
(colors.HexColor("#1B5E20"), "Hepatic Diagnosis"),
(colors.HexColor("#37474F"), "Other Diagnosis"),
]
for i,(col,label) in enumerate(legend_items):
ry = LY + 46 - i*10
c.setFillColor(col)
c.roundRect(LX, ry-5, 12, 8, 2, fill=1, stroke=0)
c.setFillColor(C_TITLE_BG)
c.setFont("Helvetica", 6.8)
c.drawString(LX+15, ry-3, label)
# ─────────────────────────────────────────────────────────────────────────────
# LAYOUT (all coords in points; A3 landscape = 841.9 × 595.3 pt)
# Row Y positions (top → bottom)
Y0 = H - 60 # START node
Y1 = Y0 - 40 # Step 1 (clinical assessment)
Y2 = Y1 - 42 # Diamond: Bilateral or Unilateral?
Y3 = Y2 - 40 # Diamond: Pitting or Nonpitting? (bilateral branch)
Y4 = Y3 - 42 # Step 2 investigations
Y5 = Y4 - 42 # Final diagnoses row
Y6 = Y5 - 36 # further diagnoses (second row)
# Centre x
CX = W/2
# ── START ────────────────────────────────────────────────────────────────────
sx, sy, sw, sh = CX-52, Y0-14, 104, 22
draw_rounded_box(c, sx, sy, sw, sh, C_START_BG,
["PATIENT PRESENTS WITH SWELLING"], "Helvetica-Bold", 8.5,
radius=11)
# arrow down
arrow(c, CX, sy, CX, Y1+22)
# ── STEP 1: Clinical Assessment ──────────────────────────────────────────────
bw, bh = 180, 38
draw_rounded_box(c, CX-bw/2, Y1-bh+22, bw, bh, C_STEP_BG,
["STEP 1: CLINICAL ASSESSMENT",
"History: onset · location · duration · medications",
"Exam: pitting test · JVP · abdomen · skin signs"],
"Helvetica-Bold", 7.2, radius=5,
border_color=colors.HexColor("#90CAF9"))
arrow(c, CX, Y1-bh+22, CX, Y2+18)
# ── DIAMOND 1: Bilateral vs Unilateral ───────────────────────────────────────
draw_diamond(c, CX, Y2, 70, 20, C_DIAMOND_BG,
["BILATERAL", "or UNILATERAL?"])
# ── LEFT BRANCH: UNILATERAL ──────────────────────────────────────────────────
UX = 130 # x-centre of unilateral column
# horizontal left
c.setStrokeColor(C_ARROW); c.setLineWidth(1.2)
c.line(CX-70, Y2, UX+60, Y2)
arrow(c, UX+60, Y2, UX+60, Y2-2) # tiny downward nub already at leaf level
# label
c.setFillColor(C_ARROW); c.setFont("Helvetica-Bold", 6.5)
c.drawString(UX+20, Y2+3, "UNILATERAL")
# Unilateral box
UBX = UX - 68
draw_rounded_box(c, UBX, Y2-56, 136, 52, C_STEP_BG,
["UNILATERAL SWELLING",
"─────────────────────",
"DVT → Doppler US (D-dimer)",
"Cellulitis → CBC, CRP, culture",
"Lymphedema → CT/MRI lymphatics",
"Hematoma → Hx trauma, US",
"Popliteal cyst → US knee"],
"Helvetica", 6.8, radius=5,
border_color=colors.HexColor("#EF9A9A"))
# ── RIGHT BRANCH: bilateral ──────────────────────────────────────────────────
RX = W - 115 # x right label area
c.setStrokeColor(C_ARROW); c.setLineWidth(1.2)
c.line(CX+70, Y2, RX-20, Y2)
c.setFillColor(C_ARROW); c.setFont("Helvetica-Bold", 6.5)
c.drawString(RX-50, Y2+3, "BILATERAL")
arrow(c, CX, Y2-20, CX, Y3+20) # down centre for bilateral
# ── DIAMOND 2: Pitting vs Nonpitting ─────────────────────────────────────────
draw_diamond(c, CX, Y3, 62, 18, C_DIAMOND_BG,
["PITTING or", "NON-PITTING?"])
# ── NONPITTING → right ──────────────────────────────────────────────────────
NPX = W - 82
c.setStrokeColor(C_ARROW); c.setLineWidth(1.2)
c.line(CX+62, Y3, NPX-50, Y3)
c.setFillColor(C_ARROW); c.setFont("Helvetica-Bold", 6.5)
c.drawString(NPX-85, Y3+3, "NON-PITTING")
draw_rounded_box(c, NPX-50, Y3-42, 128, 40, C_STEP_BG,
["NON-PITTING EDEMA",
"──────────────────────",
"Hypothyroid → TSH, Free T4",
"Lymphedema (cancer/filariasis)",
"Graves' dermopathy → T3,T4,TSH",
"Lipedema → clinical Dx"],
"Helvetica", 6.8, radius=5,
border_color=colors.HexColor("#80CBC4"))
# ── PITTING → down ───────────────────────────────────────────────────────────
arrow(c, CX, Y3-18, CX, Y4+bh-2)
c.setFillColor(C_ARROW); c.setFont("Helvetica-Bold", 6.5)
c.drawString(CX+3, Y3-10, "PITTING")
# ── STEP 2: Labs / Investigations ────────────────────────────────────────────
draw_rounded_box(c, CX-bw/2, Y4-bh+bh-2, bw, 38, C_STEP_BG,
["STEP 2: KEY INVESTIGATIONS",
"BNP · Serum albumin · Urine protein · LFTs",
"Creatinine · TSH · Echo · Chest X-ray"],
"Helvetica-Bold", 7.2, radius=5,
border_color=colors.HexColor("#90CAF9"))
arrow(c, CX, Y4-bh+bh-2, CX, Y4-bh+bh-2-6)
# ── DIAMOND 3: Which system? ──────────────────────────────────────────────────
D3Y = Y4 - bh - 8
draw_diamond(c, CX, D3Y, 80, 22, C_DIAMOND_BG,
["WHICH SYSTEM", "IS IMPLICATED?"])
# ── SIX FINAL DIAGNOSIS LEAVES ───────────────────────────────────────────────
LW, LH = 118, 56
spacing = (W - 48) / 6
leaf_y = D3Y - 70
leaves = [
("cardiac", 42, ["CARDIAC", "─────────────",
"↑ BNP/NT-proBNP",
"↑ JVP + S3 gallop",
"Echo: ↓ EF",
"Rx: Diuretics,",
"ACEi/ARB, β-blocker"]),
("renal", 160, ["RENAL FAILURE", "─────────────",
"↑ Creatinine/BUN",
"Hyperkalemia",
"Metabolic acidosis",
"Proteinuria (CKD)",
"Rx: Dialysis, diuretics"]),
("nephrotic", 279, ["NEPHROTIC SYNDROME", "──────────────",
"Protein ≥3.5 g/day",
"↓ Albumin",
"Periorbital edema",
"Rx: Treat cause,",
"diuretics, protein diet"]),
("hepatic", 398, ["HEPATIC CIRRHOSIS", "──────────────",
"↑ LFTs, ↓ albumin",
"Ascites + jaundice",
"Spider angiomas",
"Rx: Salt restrict,",
"spironolactone"]),
("allergy", 517, ["ALLERGY / ANGIOEDEMA", "──────────────",
"Hives / urticaria",
"ACEi → bradykinin",
"Preeclampsia: BP+",
"Rx: Antihistamine,",
"epi if severe"]),
("medic", 636, ["OTHER CAUSES", "──────────────",
"Medications (CCB,",
"steroids, NSAIDs)",
"Pregnancy",
"Malnutrition/kwashiorkor",
"Rx: Stop offender"]),
]
for key, lx, lines in leaves:
draw_rounded_box(c, lx, leaf_y - LH, LW, LH,
C_LEAF_BG.get(key, colors.HexColor("#37474F")),
lines, "Helvetica", 6.5, radius=5,
border_color=colors.white)
# arrow from diamond base to top of box
bx = lx + LW/2
# draw elbow: down from diamond, then over, then down to box
mid_y = D3Y - 28
c.setStrokeColor(C_ARROW); c.setLineWidth(0.9)
c.line(CX, D3Y-22, CX, mid_y)
c.line(CX, mid_y, bx, mid_y)
arrow(c, bx, mid_y, bx, leaf_y)
# ── FOOTER ───────────────────────────────────────────────────────────────────
c.setFillColor(C_TITLE_BG)
c.rect(4, 4, W-8, 14, fill=1, stroke=0)
c.setFillColor(colors.HexColor("#B3C0FF"))
c.setFont("Helvetica", 6.5)
footer = ("Sources: Harrison's Internal Medicine 22E | Guyton & Hall Medical Physiology | "
"Frameworks for Internal Medicine | For clinical use only — always apply clinical judgment")
c.drawString(W/2 - c.stringWidth(footer,"Helvetica",6.5)/2, 8, footer)
c.save()
print("PDF saved →", OUTPUT)
Running Command
cd /home/daytona/workspace/swelling-flowchart && python generate_flowchart.py 2>…
Running Command
ls -lh /home/daytona/workspace/swelling-flowchart/Swelling_Diagnostic_Flowchart.…
Your diagnostic flowchart PDF is ready:
Swelling Diagnostic Flowchart
PDF Document · PDF
What's inside the flowchart (A3 landscape, single page):
The chart walks through a structured clinical decision tree:
- Patient presents with swelling - the entry node
- Step 1 - Clinical Assessment - history (onset, location, medications) + physical exam (pitting test, JVP, skin signs)
- Decision: Bilateral or Unilateral?
- Unilateral branch - covers DVT (Doppler US), cellulitis (CBC/CRP), lymphedema, hematoma, popliteal cyst
- Bilateral path continues downward
- Decision: Pitting or Non-Pitting?
- Non-pitting branch - hypothyroidism (TSH/T4), lymphedema (cancer/filariasis), Graves' dermopathy, lipedema
- Pitting continues downward
- Step 2 - Key Investigations - BNP, albumin, urine protein, LFTs, creatinine, TSH, Echo, CXR
- Decision: Which System? - fans out into 6 color-coded diagnosis leaves:
- 🔴 Cardiac - ↑BNP, ↑JVP, S3 gallop, Echo EF; Rx: diuretics, ACEi/ARB, β-blocker
- 🟣 Renal Failure - ↑Creatinine, hyperkalemia, metabolic acidosis; Rx: dialysis/diuretics
- 🔵 Nephrotic Syndrome - Protein ≥3.5 g/day, ↓albumin, periorbital edema
- 🟢 Hepatic Cirrhosis - ↑LFTs, ascites, spider angiomas; Rx: spironolactone
- 🟠 Allergy/Angioedema/Preeclampsia - urticaria, ACEi, BP+; Rx: antihistamine/epi
- ⬛ Other Causes - medications (CCBs, steroids), pregnancy, malnutrition
Teach me thyroidism according to final year student
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have everything I need. Here is the complete, final-year-level teaching on thyroid disorders:
🩺 Thyroid Disorders - Final Year MBBS Master Guide
Sources: Robbins & Kumar Basic Pathology | Textbook of Family Medicine 9e | Harrison's Principles of Internal Medicine 22E
PART 1 - PHYSIOLOGY (Know This Cold)
The HPT Axis
Hypothalamus
↓ TRH (Thyrotropin-Releasing Hormone)
Anterior Pituitary
↓ TSH (Thyroid-Stimulating Hormone)
Thyroid Gland
↓ T3 + T4 (Thyroid Hormones)
Peripheral Tissues
↑ T3/T4 → NEGATIVE FEEDBACK on hypothalamus + pituitary
Hormone Synthesis (Step by Step)
- Iodine trapping - dietary iodine (I⁻) actively pumped into follicular cells via Na⁺/I⁻ symporter
- Oxidation - TPO (thyroid peroxidase) oxidizes I⁻ → I²
- Organification - iodine binds to tyrosine residues on thyroglobulin → MIT (monoiodotyrosine) and DIT (diiodotyrosine)
- Coupling - TPO couples MIT + DIT → T3 (MIT+DIT), T4 (DIT+DIT)
- Storage - T3/T4 stored in follicular colloid as thyroglobulin
- Release - TSH stimulates endocytosis of colloid → proteolysis → T3 + T4 secreted into blood
- Peripheral conversion - 80% of T3 comes from deiodination of T4 in liver/kidney by deiodinase
Key Facts to Memorize
| Parameter | Value |
|---|---|
| T4 : T3 secretion ratio | 20:1 |
| Biologically active form | T3 (10× more potent than T4) |
| T3 receptor affinity | 10-fold greater than T4 |
| Transport proteins | TBG (major), Transthyretin, Albumin |
| Half-life T4 | ~7 days |
| Half-life T3 | ~1 day |
Actions of thyroid hormone: Increase BMR, carbohydrate and lipid catabolism, protein synthesis, cardiac contractility, growth and development (critical for brain in fetus/neonate)
- Robbins & Kumar Basic Pathology, p. 729
PART 2 - HYPERTHYROIDISM
Definition
Elevated circulating thyroid hormones → hypermetabolic state = thyrotoxicosis
Causes (Must Know All)
| Cause | Mechanism | Key Feature |
|---|---|---|
| Graves disease (85%) | TSH-receptor stimulating antibodies (TRAb) | Diffuse goiter + exophthalmos + pretibial myxedema |
| Toxic Multinodular Goiter (Plummer disease) | Autonomous nodules overproduce T4 | Multiple palpable nodules; common in iodine-deficient areas |
| Toxic adenoma | Single autonomously functioning nodule | Solitary "hot" nodule on scan |
| Thyroiditis (transient) | Follicle destruction → hormone dump | Painful (de Quervain) or painless (postpartum) |
| TSH-secreting pituitary adenoma | Rare; TSH is HIGH (not suppressed) | Central hyperthyroidism |
| Factitious / Iatrogenic | Exogenous T4 excess | Low RAIU; suppressed TSH |
Graves Disease - The Most High-Yield
Pathogenesis:
- Autoimmune - TSH-Receptor Stimulating Antibodies (TRAb/TSH-RS Abs) bind TSH receptor on thyroid cells
- Mimic TSH → constant stimulation → excess T4 production
- TSH becomes suppressed (<0.01 mIU/L) due to negative feedback
- Associated with HLA-DR3, CTLA4 polymorphisms
Classic Triad:
- Thyrotoxicosis (diffuse goiter in >90%)
- Ophthalmopathy (exophthalmos/proptosis) - due to glycosaminoglycan deposition in retroorbital tissue
- Dermopathy (pretibial myxedema) - nonpitting, nondependent edema over shin
Histology: Diffuse hyperplasia of follicles + lymphoid infiltrates + scalloped colloid
Clinical Features of Hyperthyroidism (System by System)
| System | Features |
|---|---|
| Constitutional | Weight loss despite increased appetite, heat intolerance, sweating, warm moist skin |
| Cardiovascular | Tachycardia, palpitations, atrial fibrillation, wide pulse pressure, systolic hypertension |
| GI | Diarrhea, hypermotility, malabsorption, steatorrhea |
| Neuromuscular | Anxiety, tremor, irritability, proximal muscle weakness (thyroid myopathy ~50%) |
| Ocular | Lid lag, wide staring gaze (due to sympathetic stimulation of superior tarsal muscle) |
| Reproductive | Oligomenorrhea, infertility |
| Skin/Hair | Fine hair, onycholysis (Plummer's nails) |
Diagnosis of Hyperthyroidism
Step 1: sTSH → if SUPPRESSED (<0.1 mIU/L), proceed
Step 2: Free T4 + Free T3 → elevated confirms thyrotoxicosis
Step 3: Determine etiology:
├── TRAb (TSH-Receptor Antibodies) → Graves disease
├── RAIU (Radioactive Iodine Uptake) scan:
│ Diffuse ↑ uptake → Graves disease
│ Focal ↑ uptake → toxic adenoma
│ ↓ uptake → thyroiditis or exogenous T4
└── Anti-TPO, Anti-Tg antibodies → Hashimoto
Exam tip: TSH is the SINGLE MOST USEFUL screening test. It is suppressed even in subclinical hyperthyroidism before T4/T3 become elevated.
Treatment of Hyperthyroidism
| Option | Drug/Method | Key Detail |
|---|---|---|
| Antithyroid drugs | Propylthiouracil (PTU) or Methimazole (MMI) | Block TPO (organification). PTU also blocks peripheral T4→T3 conversion. MMI preferred (longer acting). PTU preferred in 1st trimester pregnancy |
| Beta-blockers | Propranolol | Controls sympathetic symptoms (tachycardia, tremor) - does NOT reduce hormone levels |
| Radioiodine (¹³¹I) ablation | ¹³¹I | Destroys thyroid tissue; most common definitive Rx in US; often causes hypothyroidism |
| Surgery | Subtotal/total thyroidectomy | For large goiters, suspected malignancy, ¹³¹I failure |
PART 3 - THYROID STORM ⚠️
A medical emergency. Abrupt onset of severe hyperthyroidism, most often in Graves disease.
Precipitants: Infection, surgery, trauma, stopping antithyroid meds, contrast dye
Features: Hyperpyrexia (fever >40°C), extreme tachycardia, agitation, delirium, vomiting, heart failure
Treatment (BBBBSS - mnemonic):
- Beta-blocker (propranolol IV) - control HR
- Block synthesis (PTU preferred - also blocks conversion)
- Block release (Lugol's iodine after PTU - Wolff-Chaikoff effect) - give 1 hour AFTER PTU
- Block conversion (PTU, glucocorticoids, propranolol)
- Steroids (hydrocortisone) - prevent adrenal crisis + reduce T4→T3 conversion
- Support (IV fluids, cooling, treat precipitant)
PART 4 - HYPOTHYROIDISM
Definition
Insufficient thyroid hormone to meet body needs → hypometabolic state
TSH > 10 mIU/L (primary hypothyroidism)
Causes
| Cause | Notes |
|---|---|
| Hashimoto thyroiditis | #1 cause in iodine-sufficient countries (US, UK, India urban) |
| Iodine deficiency | #1 cause worldwide (~2 billion affected); causes endemic goiter and cretinism |
| Post-radioiodine / post-surgery | Iatrogenic; permanent |
| Drugs | Lithium, amiodarone, iodides, antithyroid drugs |
| Congenital | Thyroid dysgenesis, dyshormonogenesis; detected by neonatal TSH screening |
| Central (secondary) | Pituitary failure (TSH low); hypothalamic failure (TRH low) |
| Postpartum thyroiditis | Transient; ~6 weeks postpartum |
Hashimoto Thyroiditis - The Most High-Yield
Pathogenesis:
- Breakdown of self-tolerance to thyroid antigens
- Autoimmune destruction via 3 mechanisms:
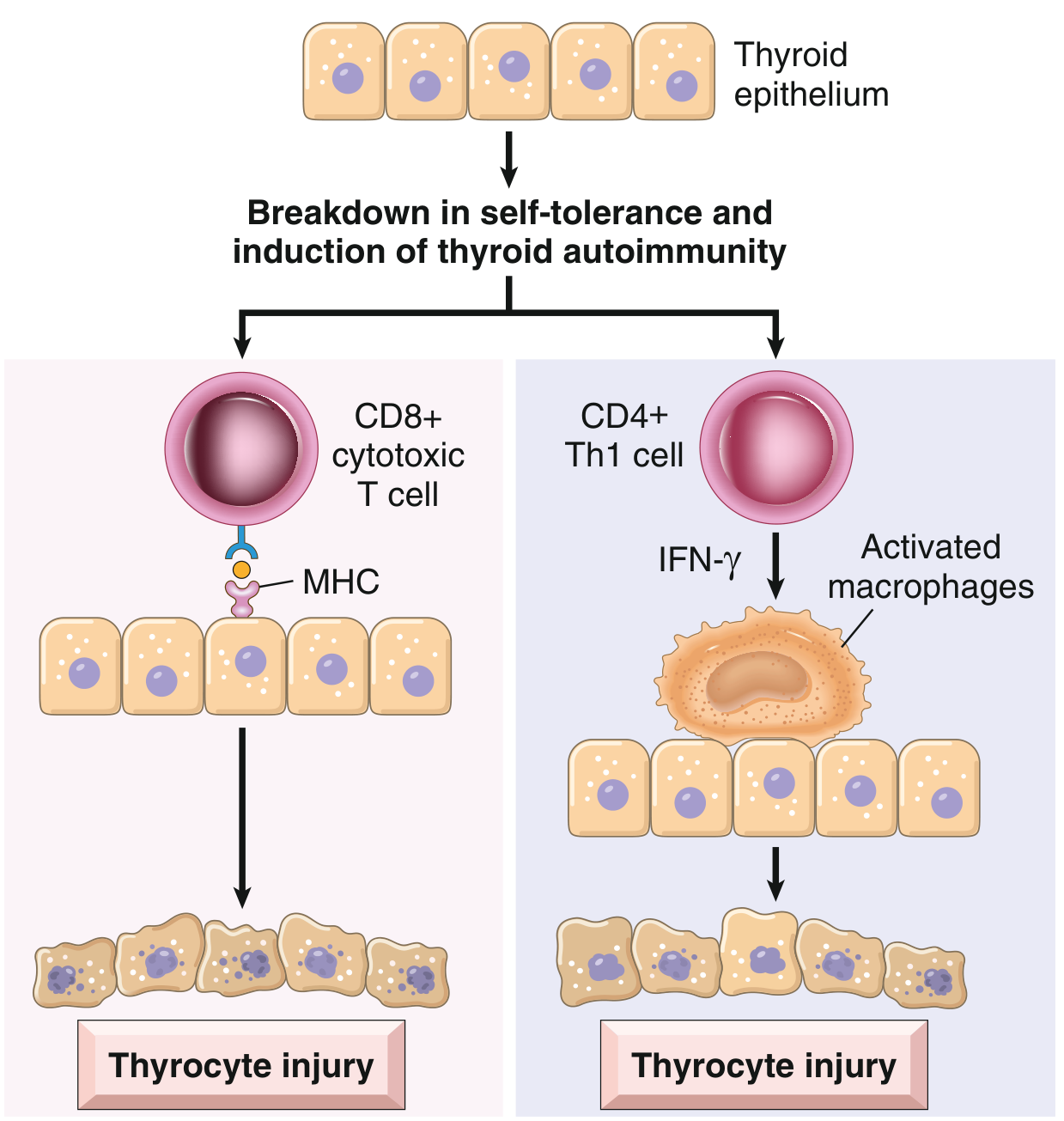
- CD8+ cytotoxic T cells directly kill thyrocytes via MHC-I
- CD4+ Th1 cells release IFN-γ → activate macrophages → follicle destruction
- Anti-TPO antibodies + Anti-Tg antibodies → complement-mediated and ADCC destruction
Genetics: CTLA4 polymorphism (T-cell inhibitor gene mutation), HLA-DR3/DR5; 40% concordance in monozygotic twins
Histology: Diffuse lymphoplasmacytic infiltrate + germinal centres + Hürthle cell (oxyphil) change + interstitial fibrosis + atrophic follicles
Hürthle cells = metaplastic follicular cells with abundant eosinophilic granular cytoplasm (packed with mitochondria) - key histological marker
Clinical course:
-
Middle-aged woman (F:M = 10-14:1)
-
Painless diffuse goiter
-
"Hashitoxicosis" first - transient thyrotoxicosis from follicle rupture releasing stored hormone
-
Then progressive hypothyroidism as gland fibroses
-
Robbins & Kumar Basic Pathology, p. 731
Clinical Features of Hypothyroidism (System by System)
| System | Features |
|---|---|
| Constitutional | Fatigue, weight gain, cold intolerance, low BMR |
| Cardiovascular | Bradycardia, diastolic hypertension, pericardial effusion, hypercholesterolemia |
| GI | Constipation, decreased gut motility |
| Neuromuscular | Lethargy, cognitive slowing ("myxedema madness"), carpal tunnel syndrome, delayed relaxation of deep tendon reflexes |
| Skin/Hair | Dry rough skin, coarse hair, hair loss, brittle nails, myxedema (non-pitting edema due to glycosaminoglycan deposition) |
| Reproductive | Menorrhagia, infertility, hyperprolactinemia (TRH stimulates PRL) |
| Eyes | Periorbital puffiness (morning), loss of outer 1/3 of eyebrows |
| Voice | Hoarseness (myxedematous infiltration of vocal cords) |
Myxedema = non-pitting, diffuse edema due to accumulation of glycosaminoglycans (hyaluronic acid) in dermis. Worst in face, hands, legs.
Diagnosis of Hypothyroidism
Primary hypothyroidism:
TSH ↑↑ + Free T4 ↓ → confirms primary hypothyroidism
+ Anti-TPO antibodies (+) → Hashimoto thyroiditis
Secondary hypothyroidism (rare):
TSH low/normal + Free T4 low → pituitary failure
→ MRI pituitary; evaluate rest of pituitary axis
Subclinical hypothyroidism:
TSH mildly ↑ (4.5-10) + Normal Free T4 → asymptomatic
→ Monitor; treat if TSH >10 or symptomatic
Treatment of Hypothyroidism
Levothyroxine (L-thyroxine / T4) is the drug of choice
- Dose: 1.6 µg/kg/day (adults)
- Elderly / cardiac patients: start low (25-50 µg/day), titrate slowly
- Monitor TSH annually; target TSH = 0.5-2.5 mIU/L
- Taken on empty stomach; interactions with calcium, iron, PPIs (reduce absorption)
T3 (Liothyronine): Some refractory patients with normal TSH but persistent symptoms may benefit from T4+T3 combination
PART 5 - MYXEDEMA COMA ⚠️
Severe life-threatening hypothyroidism (end-stage). Medical emergency.
Precipitants: Cold exposure, infection, sedatives, surgery, stopping levothyroxine
Features: Hypothermia, bradycardia, hypotension, hypoventilation, hyponatremia, altered consciousness/coma, myxedematous facies
Treatment:
- IV T3 (liothyronine) or IV T4 - rapid hormone replacement
- IV hydrocortisone (adrenal insufficiency often coexists)
- Passive rewarming (not active - risk of vasodilation)
- IV fluids, treat precipitant, mechanical ventilation if needed
PART 6 - THYROIDITIS (Summary)
| Type | Cause | Painful? | Course | Antibodies |
|---|---|---|---|---|
| Hashimoto (chronic lymphocytic) | Autoimmune | No | Progressive → hypothyroidism | Anti-TPO +++, Anti-Tg+ |
| de Quervain (subacute granulomatous) | Viral (post-URI) | YES (severe) | Self-limited; hyperthyroid → euthyroid → transient hypothyroid → recovery | ESR ↑↑, mild Anti-TPO |
| Painless/silent (subacute lymphocytic) | Autoimmune | No | Self-limited; postpartum most common | Anti-TPO+ |
| Riedel thyroiditis | Fibrous replacement | No | Rare; hard "iron thyroid"; may be IgG4-related | None specific |
| Acute suppurative | Bacterial | YES | Rare; abscess; treat with antibiotics/drainage | - |
PART 7 - THYROID NEOPLASMS (High-Yield Summary)
| Tumour | Origin | % | Key Feature | Prognosis |
|---|---|---|---|---|
| Papillary carcinoma | Follicular cells | 80% | "Orphan Annie eye" nuclei (ground-glass), nuclear grooves, pseudoinclusions; spreads via lymphatics; RET/BRAF mutations | Excellent (5yr survival >95%) |
| Follicular carcinoma | Follicular cells | 10% | Distinguished by capsular + vascular invasion (not cytology); PAX8/PPARG fusion; spreads hematogenously (lung, bone) | Good |
| Medullary carcinoma | Parafollicular C cells | 5-8% | Secretes calcitonin (tumour marker); amyloid deposits (calcitonin-derived); RET proto-oncogene mutation; 30% familial (MEN2A, MEN2B) | Intermediate |
| Anaplastic carcinoma | Dedifferentiated follicular/papillary | <1% | Uniformly lethal; TP53 loss; rapid growth, compresses trachea | Very poor (<6 months median survival) |
Exam tip: Only 1% of thyroid nodules are malignant. Fine-needle aspiration cytology (FNAC) is the primary diagnostic tool for any thyroid nodule.
PART 8 - QUICK EXAM COMPARISONS
Hyper vs. Hypo - Side-by-Side
| Feature | Hyperthyroidism | Hypothyroidism |
|---|---|---|
| Weight | ↓ (despite increased appetite) | ↑ |
| Heart rate | ↑ (tachycardia, AF) | ↓ (bradycardia) |
| Temperature | Heat intolerance, warm skin | Cold intolerance, dry cold skin |
| GI | Diarrhea | Constipation |
| Reflexes | Hyperreflexia | Delayed (slow relaxation) |
| Mood | Anxiety, irritability | Lethargy, depression |
| Menstruation | Oligomenorrhea | Menorrhagia |
| TSH | ↓ (suppressed) | ↑ |
| Free T4 | ↑ | ↓ |
| Cholesterol | ↓ | ↑ |
TSH Interpretation Cheat Sheet
| TSH | Free T4 | Diagnosis |
|---|---|---|
| ↓↓ (<0.01) | ↑ | Overt hyperthyroidism |
| ↓ (0.1-0.4) | Normal | Subclinical hyperthyroidism |
| Normal | Normal | Euthyroid |
| ↑ (4.5-10) | Normal | Subclinical hypothyroidism |
| ↑↑ (>10) | ↓ | Overt hypothyroidism |
| ↓ or normal | ↓ | Central/secondary hypothyroidism |
| ↑↑ | ↑ | TSH-secreting pituitary adenoma or thyroid hormone resistance |
PART 9 - HIGH-YIELD EXAM MNEMONICS
GRAVES (features of Graves disease):
- Goiter (diffuse)
- Retroorbital inflammation (exophthalmos)
- Autoimmune (TRAb)
- Vascularization of thyroid (bruit over gland)
- Exophthalmos + pretibial myxedema
- Suppressed TSH
Hypothyroid features - "SLOW":
- Skin (dry, coarse), Slowed reflexes
- Lethargy, weight gain, Lipids ↑
- Oedema (myxedema, periorbital)
- Weight gain, cold intolerance
Antithyroid drugs - PTU vs MMI:
- PTU = Pregnancy (1st trimester) + blocks Peripheral T4→T3 conversion
- MMI = standard choice, once-daily dosing, preferred long-term
Sources:
- Robbins & Kumar Basic Pathology - Chapter 18 (Endocrine System), pp. 729-731
- Textbook of Family Medicine 9e - Chapter 35 (Thyroid Disorders), pp. 1019-1022
- Textbook of Family Medicine 9e - Hashimoto thyroiditis and Graves treatment sections
This is a shared conversation. Sign in to Orris to start your own chat.