Connective tissue, Function of connective tissue, Connective tissue cells, resident cells of the connective tissue, extracellular matrix of the connective tissue, Ground substance of the connective tissue, connective tissue fibers, Embryonic connective tissue
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed for a comprehensive, well-illustrated response. Here is the full organized answer:
Connective Tissue - Complete Overview
1. What Is Connective Tissue?
Connective tissue is one of the four basic tissue types of the body. Unlike epithelium, muscle, and nerve - which consist mainly of cells - connective tissue is defined by very large amounts of extracellular matrix (ECM). The cells are conspicuously separated from one another; the intervening spaces are occupied by ECM produced by the cells themselves.
Connective tissue forms a vast and continuous compartment throughout the body, bounded by the basal laminae of various epithelia and by the external/basal laminae of muscle cells and nerve-supporting cells. It connects and supports all other tissues and organs.
Classification is primarily based on the composition, organization, and relative amount of its extracellular components:
- Embryonic connective tissue (mesenchyme; mucous connective tissue)
- Connective tissue proper (loose/areolar; dense irregular; dense regular)
- Specialized connective tissue (reticular tissue; adipose tissue; cartilage; bone; blood)
2. Functions of Connective Tissue
The functions vary based on cell types, fiber composition, and ground substance, but include:
| Function | Example |
|---|---|
| Structural support | Tendons, ligaments, bone - provide mechanical framework |
| Physical connection | Connects organs, muscles, and epithelia |
| Metabolic support | Interstitial fluid serves as medium for nutrient/waste diffusion between cells and blood |
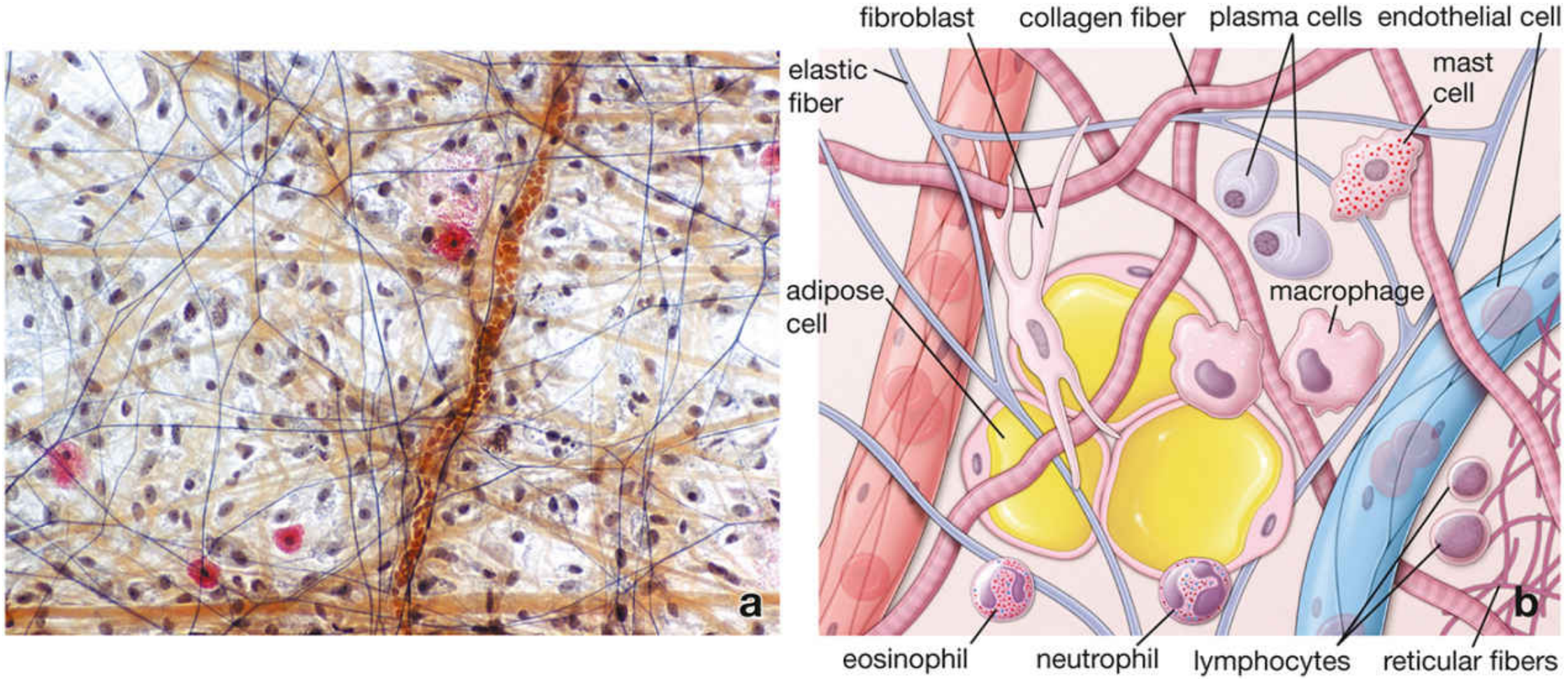
| Defense/immunity | Macrophages, plasma cells, lymphocytes, neutrophils, and eosinophils operate within the ECM |
| Energy storage | Adipocytes store neutral fats |
| Repair | Fibroblasts migrate and synthesize new matrix during wound healing |
| Filtration barrier | Type IV collagen in kidney glomerular basal lamina |
| Insulation | Adipose tissue provides thermal insulation |
"The functions of the various connective tissues are reflected in the types of cells and fibers present within the tissue and the composition of the ground substance in the ECM." - Histology A Text and Atlas, 7e
3. Connective Tissue Cells
Connective tissue cells are divided into two populations:
A. Resident Cells (Permanent Population)
These cells are relatively stable with little movement; they are regarded as permanent residents of the tissue.
1. Fibroblasts (Principal Cell)
The most numerous cell in connective tissue proper. Fibroblasts:
- Originate from embryonic mesenchymal cells and become permanent residents
- Synthesize and secrete collagen (most abundant protein in the body), elastin, and reticular fibers
- Produce complex carbohydrates of the ground substance (GAGs, proteoglycans, multiadhesive glycoproteins)
- Have large, pale-staining nuclei with prominent nucleoli when active (fibroblast); when inactive, the cell is called a fibrocyte with smaller, darker nuclei and reduced synthetic activity
Myofibroblasts - a closely related cell type with properties intermediate between fibroblasts and smooth muscle cells; important in wound contraction.
2. Macrophages
- Derived from two origins: (a) yolk sac erythro-myeloid progenitors (embryonic, tissue-resident self-renewing pool) and (b) bone marrow hematopoietic stem cells via blood monocytes
- Functions: phagocytosis of ECM debris, bacteria, and aging cells; antigen processing and presentation; secretion of growth factors and cytokines
- Tissue-specific macrophages include: microglia (CNS), Kupffer cells (liver), alveolar macrophages (lungs), Langerhans cells (skin), mesangial cells (kidney), Hofbauer cells (placenta)
3. Mast Cells
- Found along blood vessels throughout loose connective tissue
- Large cells with numerous metachromatic granules containing:
- Histamine - vasodilator; increases vascular permeability
- Heparin - anticoagulant
- Tryptase, chymase (serine proteases)
- Leukotrienes and prostaglandins (synthesized de novo on activation)
- Play key roles in allergic/hypersensitivity reactions (type I) and defense against parasites
4. Adipocytes (Fat Cells)
- Specialize in storing neutral lipids (triglycerides)
- Found singly or in clusters in loose connective tissue, or massively aggregated as adipose tissue
- Two types: white adipose tissue (unilocular, energy storage) and brown adipose tissue (multilocular, thermogenesis)
5. Adult Stem Cells
- Mesenchyme-like cells remain present in some adult connective tissues, including tooth pulp and some adipose tissue
- Being investigated as sources for therapeutic repair and organ regeneration
B. Wandering (Transient) Cells
These cells migrate into connective tissue from blood in response to specific stimuli:
| Cell | Primary Function |
|---|---|
| Lymphocytes | Immune surveillance and adaptive immunity |
| Plasma cells | Antibody secretion (differentiated B lymphocytes) |
| Neutrophils | Phagocytosis of bacteria; first responders to acute infection |
| Eosinophils | Modulate allergic/vasoactive reactions; defense against helminths |
| Basophils | Pharmacologically active molecules (histamine); similar to mast cells |
| Monocytes | Differentiate into macrophages in tissue |
4. Extracellular Matrix (ECM) of Connective Tissue
The ECM has two major components:
- Protein fibers (collagen, reticular, elastic)
- Ground substance (amorphous component - GAGs, proteoglycans, multiadhesive glycoproteins)
"Unlike epithelial cells, connective tissue cells are conspicuously separated from one another. The intervening spaces are occupied by material produced by the cells. This extracellular material is called the extracellular matrix." - Histology A Text and Atlas, 7e
In all types of connective tissue, the extracellular volume exceeds that of the cells. The ECM determines the structural, mechanical, and functional properties of each connective tissue type.
5. Ground Substance
Ground substance is a highly hydrated, transparent, gel-like complex that fills all spaces between cells and fibers. It appears amorphous (structureless) in routine H&E sections due to its aqueous nature. It has three classes of macromolecules:
A. Glycosaminoglycans (GAGs)
Long, unbranched polysaccharide chains of repeating disaccharide units. They are strongly anionic (negatively charged) and highly hydrophilic - they bind water and cations, forming a gel:
| GAG | Features |
|---|---|
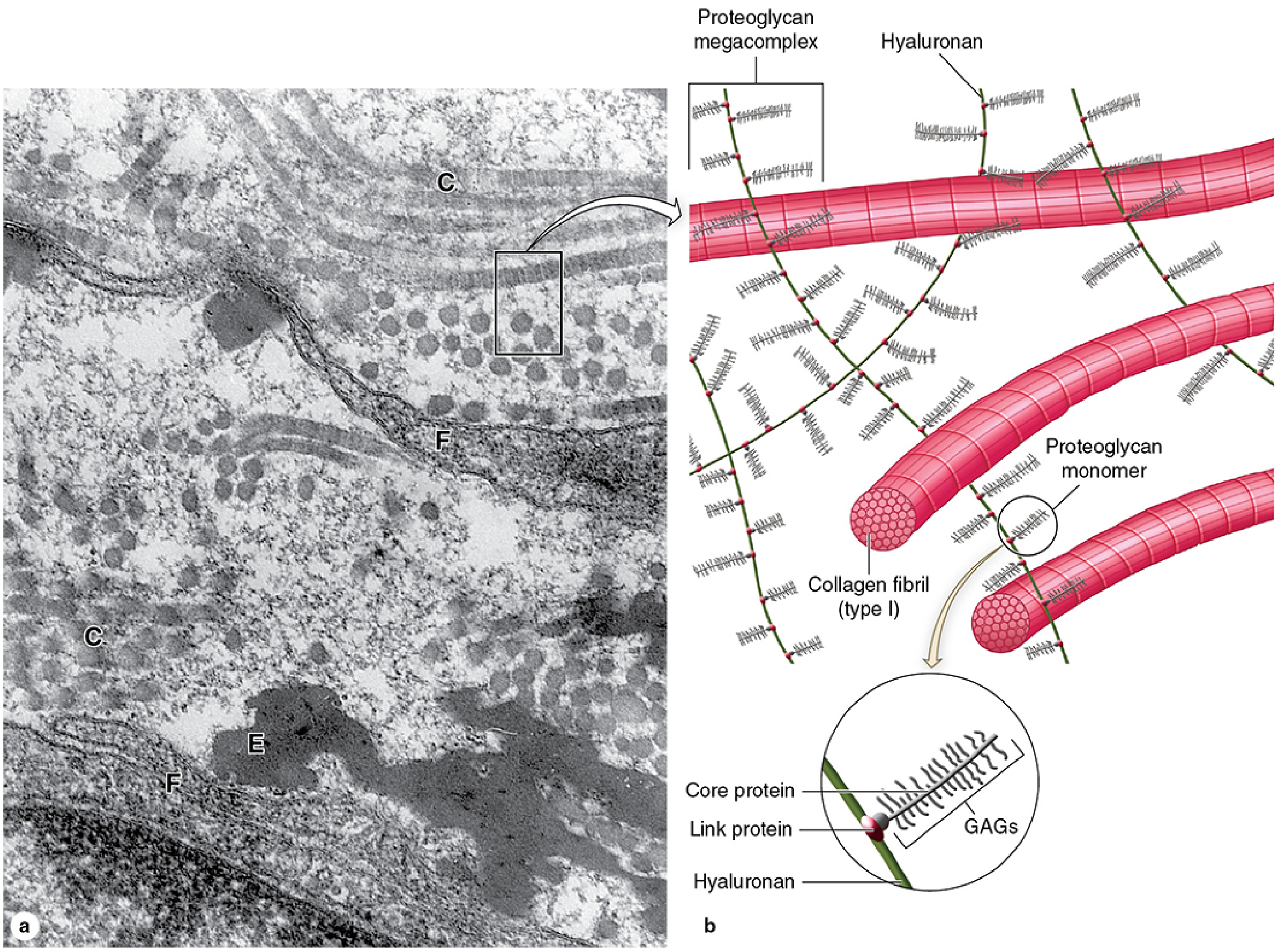
| Hyaluronan (hyaluronic acid) | Very long polymer of glucosamine-glucuronate; NOT sulfated; not covalently linked to protein; forms backbone for proteoglycan megacomplexes; most abundant in embryonic tissue |
| Chondroitin sulfate | Sulfated; bound to proteoglycan core proteins; abundant in cartilage |
| Dermatan sulfate | Sulfated; in skin, tendons, vessels |
| Heparan sulfate | Sulfated; in basal laminae |
| Heparin | Highly sulfated; in mast cell granules; anticoagulant |
| Keratan sulfate | Sulfated; in cartilage and cornea |
B. Proteoglycans
Core proteins with multiple covalently attached sulfated GAG chains. They bind to hyaluronan via linker proteins to form enormous proteoglycan megacomplexes that bind vast amounts of water and regulate the diffusion of molecules through the matrix. Key proteoglycans include:
- Aggrecan - most abundant in articular cartilage; core protein with ~100 chondroitin sulfate chains
- Perlecan - in basal laminae
- Syndecan - transmembrane; mediates cell attachment to ECM
- Versican, decorin, biglycan - in connective tissue proper
C. Multiadhesive Glycoproteins
These link cells to each other and to the ECM via binding sites for integrins, collagens, and other matrix molecules:
| Protein | MW | Location | Function |
|---|---|---|---|
| Fibronectin | 250-280 kDa | ECM of many tissues | Cell adhesion and migration; binds integrins, type IV collagen, heparin, fibrin |
| Laminin | 140-400 kDa | All basal laminae, external laminae | Anchors cells to basal lamina; binds collagen IV, heparan sulfate, entactin |
| Tenascin | 1,680 kDa | Embryonic mesenchyme, wounds, tumors | Modulates cell attachments; binds fibronectin, integrins |
| Entactin/Nidogen | 150 kDa | Basal lamina | Links laminin and type IV collagen |
| Osteopontin | 44 kDa | Bone | Binds osteoclasts, hydroxyapatite |
Functions of ground substance:
- Allows diffusion of small molecules (nutrients, metabolic wastes, hormones)
- Acts as a lubricant due to its viscosity
- Acts as a barrier to penetration of microorganisms (especially hyaluronan)
- Profoundly influences cellular activities - proliferation, differentiation, migration
6. Connective Tissue Fibers
There are three principal types:
A. Collagen Fibers
The most abundant structural components of connective tissue - collagen is the most abundant protein in the entire body.
Properties:
- Flexible yet have high tensile strength
- Appear as long, straight, unbranched profiles in H&E (pink/eosinophilic)
- Exhibit characteristic 67-nm (D-period) banding visible by TEM
- Stain green with Masson trichrome, blue with Mallory trichrome
Structure: Collagen fibrils → collagen fibers → fiber bundles
- Each fibril is assembled from triple-helical collagen molecules (tropocollagen: 300 nm long, 1.5 nm wide)
- Three alpha chains wind together in a right-handed helix; requires glycine at every third position (Gly-X-Y) and hydroxyproline/hydroxylysine (from proline/lysine by vitamin C-dependent hydroxylation)
Biosynthesis (intracellular steps):
- Transcription and translation of alpha-chain preprocollagen
- Hydroxylation of proline and lysine residues in RER (requires vitamin C)
- Glycosylation and triple-helix formation → procollagen
- Secretion via exocytosis
Biosynthesis (extracellular steps):
5. Cleavage of N- and C-terminal propeptides by procollagen peptidases → tropocollagen
6. Self-assembly of tropocollagen into collagen fibrils
7. Cross-linking by lysyl oxidase (enzyme, requires copper)
Major collagen types:
| Type | Composition | Location | Function |
|---|---|---|---|
| I | [α1(I)]₂α2(I) | Skin, bone, tendon, ligaments, dentin - 90% of body collagen | Resistance to tension and stretch |
| II | [α1(II)]₃ | Hyaline cartilage, intervertebral disc, notochord | Resistance to intermittent pressure |
| III | [α1(III)]₃ | Loose CT, uterus, liver, spleen, blood vessels, fetal skin | Forms reticular fibers; supportive scaffolding in expansible organs |
| IV | Complex heterotrimers | All basal and external laminae | Support of epithelial cells; filtration barrier |
| V | Various | Fetal tissues, skin, bone, placenta | Modulates biomechanical properties of type I fibrils |
| VII | [α1(VII)]₃ | Anchoring fibrils of skin, eye, uterus | Secures basal lamina to underlying reticular lamina |
Clinical note: Vitamin C deficiency impairs hydroxylation of proline/lysine → weak, unstable collagen → scurvy (bleeding gums, poor wound healing, perifollicular hemorrhages).
B. Reticular Fibers
- Composed of type III collagen
- Much thinner than collagen fibers (0.5-2 μm); form a delicate meshwork, not thick bundles
- Argyrophilic - stain black with silver impregnation (NOT with routine H&E)
- PAS positive (due to glycoprotein coat)
- Provide supportive scaffolding for cells in: lymph nodes, spleen, liver, bone marrow, kidney, endocrine glands
- Produced by: reticular cells (specialized fibroblasts) in lymphoid/hematopoietic tissues; fibroblasts in other tissues
- Also produced by smooth muscle cells (around vessels) and Schwann cells (around nerve fibers)
C. Elastic Fibers
- Allow tissues to respond to stretch and distension - can be stretched to 150% of their resting length and return to original shape
- Appear as thin, branching threads; stain with resorcin-fuchsin, aldehyde fuchsin, or Verhoeff hematoxylin
Composition:
- Elastin core - amorphous component; cross-linked elastin molecules
- Rich in hydrophobic amino acids (glycine, valine, proline, leucine) arranged in repetitive motifs → random coiling → elasticity
- Contains unique amino acids desmosine and isodesmosine (formed from 4 lysine residues) responsible for covalent cross-linking
- Rich in proline and glycine but POOR in hydroxyproline (unlike collagen) and completely LACKS hydroxylysine
- Fibrillin microfibrils - form scaffolding for elastin deposition; made of fibrillin-1, fibrillin-2, EMILINs, and MAGPs
Produced by: fibroblasts, chondrocytes, endothelial cells, and smooth muscle cells
Location examples:
- Elastic ligaments (ligamenta flava, ligamentum nuchae)
- Fenestrated elastic lamellae of elastic arteries (produced by smooth muscle cells, not fibroblasts)
- Elastic fibers of skin and lung
Clinical note: Mutations in fibrillin-1 (FBN1) cause Marfan syndrome - lack of structural resistance in elastic fiber-rich tissues, leading to aortic aneurysm, lens dislocation, tall stature with long limbs.
7. Embryonic Connective Tissue
Two forms of embryonic connective tissue exist:
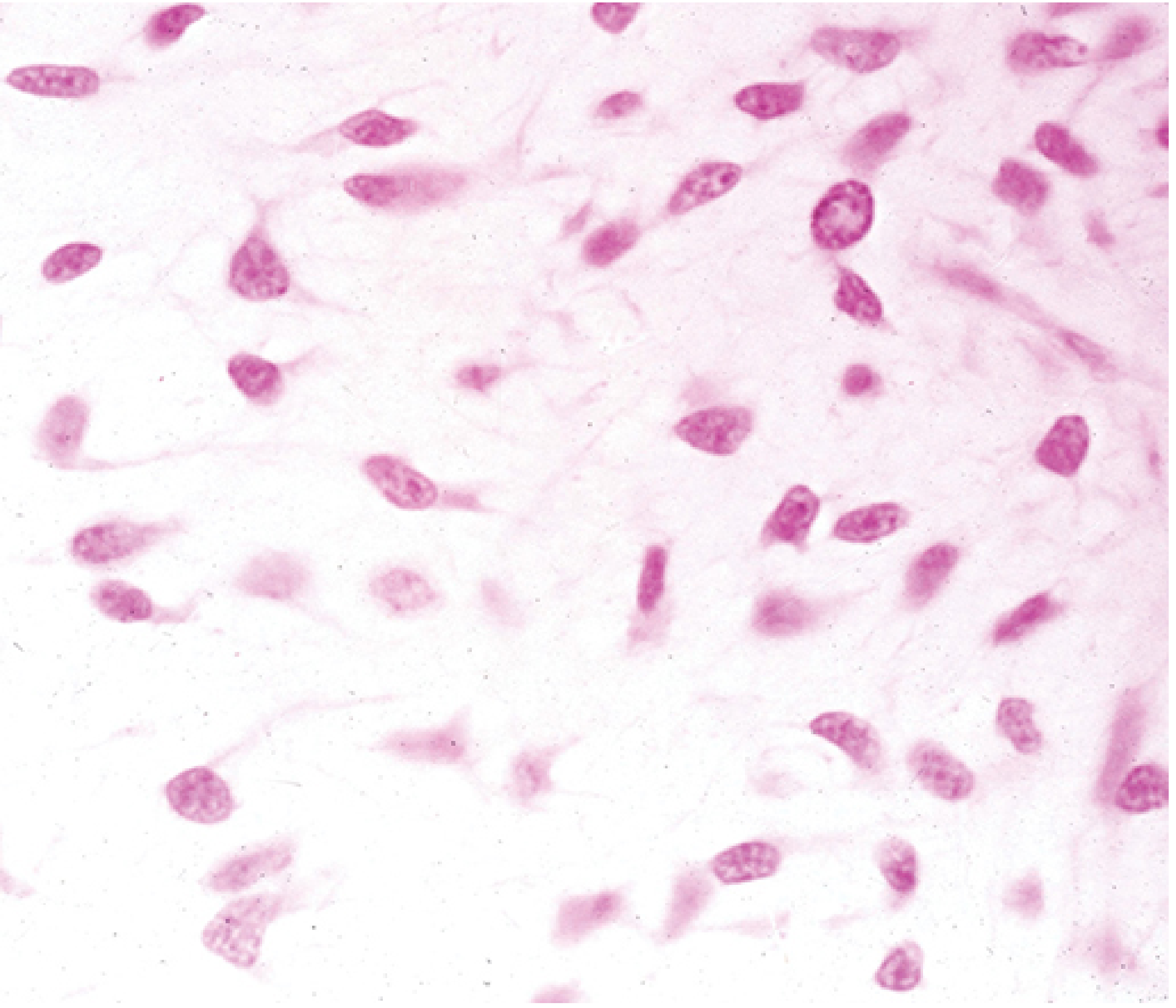
A. Mesenchyme
- The primary embryonic connective tissue, derived mainly from embryonic mesoderm (middle germ layer)
- Small contributions from neural crest cells (ectoderm-derived) to form craniofacial connective tissues
- Morphology:
- Sparsely distributed, undifferentiated cells
- Cells are generally elongated ("spindle-shaped") with cytoplasmic processes giving a stellate appearance
- Large euchromatic nuclei with prominent nucleoli - indicating high synthetic activity
- ECM consists largely of simple ground substance rich in hyaluronan with very little collagen
- Fate: Mesenchymal stem cells differentiate into all types of connective tissue proper and specialized connective tissues: bone, cartilage, blood cells, vascular endothelium, and muscle
Medical relevance: Mesenchyme-like cells (multipotent stem cells) persist in some adult connective tissues (tooth pulp, adipose tissue) and are under investigation for regenerative medicine.
B. Mucous (Mucoid) Connective Tissue
- Present primarily in the umbilical cord (also called Wharton's jelly)
- Contains widely separated, spindle-shaped fibroblasts embedded in a gelatin-like, hyaluronan-rich ECM
- The ground substance (Wharton's jelly) is extremely rich in hyaluronic acid - gives the cord its turgid, protective consistency that prevents compression of umbilical vessels
- Random collagen fibers are present but sparse
Summary Table: Classification of Connective Tissues
| Type | Key Features | Examples |
|---|---|---|
| Mesenchyme | Undifferentiated spindle cells in sparse collagen/hyaluronan ECM | Embryonic mesodermal layer |
| Mucous CT | Spindle cells in hyaluronan-rich gel (Wharton's jelly) | Umbilical cord |
| Loose (areolar) CT | Many cell types, abundant ground substance, loosely arranged fibers | Lamina propria, around vessels/glands |
| Dense irregular CT | Few cells, random collagen bundles, little ground substance | Dermis, organ capsules, submucosa |
| Dense regular CT | Parallel collagen bundles, aligned tendinocytes | Tendons, ligaments, aponeuroses |
| Reticular CT | Type III collagen meshwork + reticular cells | Bone marrow, liver, lymph nodes, spleen |
| Adipose tissue | Adipocytes dominant | White/brown fat |
| Cartilage | Chondrocytes in rigid ECM | Hyaline, elastic, fibrocartilage |
| Bone | Osteocytes in calcified ECM | Cortical/cancellous bone |
| Blood | Cells in liquid ECM (plasma) | Circulatory system |
Sources:
- Histology A Text and Atlas With Correlated Cell and Molecular Biology, 7e (Pawlina), pp. 434-535
- Junqueira's Basic Histology - Text and Atlas, 17e, pp. 257-310
Give me complete overview on Connective tissue Proper
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have everything needed for a complete, well-illustrated answer. Here it is:
Connective Tissue Proper - Complete Overview
Definition and Scope
Connective tissue proper is the broad category of soft, supportive connective tissue that excludes the specialized forms (cartilage, bone, blood, and lymph). It contains the same fundamental components as all connective tissue - cells, protein fibers, and ground substance - but in varying proportions that define its two major subtypes.
Connective tissue proper is classified into:
- Loose (areolar) connective tissue
- Dense connective tissue
- Dense irregular connective tissue
- Dense regular connective tissue
General Components
All types of connective tissue proper contain:
| Component | Details |
|---|---|
| Cells | Fibroblasts (predominant); macrophages, mast cells, adipocytes, plasma cells, lymphocytes, etc. |
| Collagen fibers | Type I (main); type III (reticular); provide tensile strength |
| Elastic fibers | Elastin + fibrillin; provide elasticity/recoil |
| Ground substance | GAGs, proteoglycans, multiadhesive glycoproteins; gel-like, hydrated |
| Blood vessels and nerves | Course through loose CT; sparse in dense CT |
Type 1: Loose (Areolar) Connective Tissue
Definition
Also called areolar tissue. Characterized by loosely arranged fibers, abundant ground substance, and a high diversity of cell types. It is the most widely distributed connective tissue in the body.
"Loose connective tissue is a cellular connective tissue with thin and relatively sparse collagen fibers. The ground substance, however, is abundant; in fact, it occupies more volume than the fibers do." - Histology A Text and Atlas, 7e
Histological Features
- Many cell nuclei visible at low magnification (high cellularity)
- Thin, wispy collagen fibers loosely arranged - not packed into thick bundles
- Abundant pale ground substance between fibers and cells
- Elastic fibers present but delicate
- Small blood vessels are common
- Stains: collagen = pink (H&E) / green (Masson trichrome) / blue (Mallory trichrome)
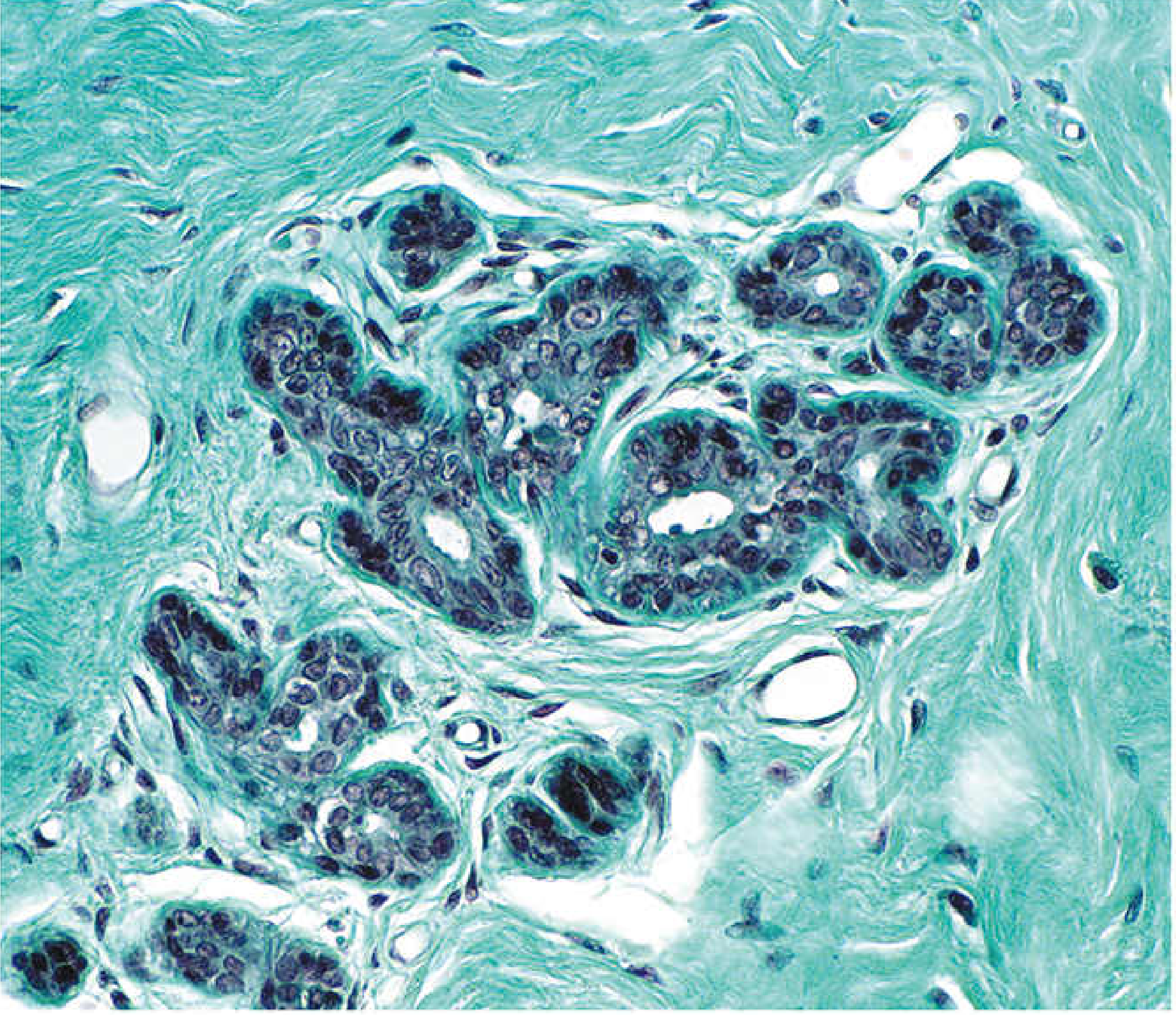
Fig. 1 - Mammary gland: loose CT (center, many cells, thin collagen) vs. dense irregular CT (periphery, thick bundles, few cells) - Masson trichrome. Histology A Text and Atlas, 7e
Cellular Composition
Loose CT is unique in having the greatest diversity of cell types of any connective tissue. Most transient cells migrate in from local blood vessels in response to stimuli:
| Cell Type | Role |
|---|---|
| Fibroblasts | Synthesize and maintain ECM fibers and ground substance |
| Macrophages | Phagocytosis; antigen presentation; cytokine secretion |
| Mast cells | Allergic/immune responses (histamine, heparin) |
| Plasma cells | Antibody secretion |
| Lymphocytes | Immune surveillance |
| Eosinophils | Anti-parasitic; modulate allergic reactions |
| Neutrophils | Bacterial phagocytosis; acute inflammation |
| Adipocytes | Scattered fat storage |
Functional Roles
- Metabolic support - abundant ground substance allows diffusion of O₂, nutrients, CO₂, and metabolic wastes between cells and the microvasculature
- First line of defense - the initial site where bacteria and pathogens that breach an epithelial surface are challenged and destroyed by immune cells
- Site of inflammation and immune reactions - can swell considerably during inflammatory episodes
- Structural support for microvasculature, nerves, and epithelial structures
Locations
- Lamina propria - loose CT of all mucous membranes (GI, respiratory, urogenital tracts); maintains large populations of immune cells because of continuous antigen exposure
- Beneath the epithelium covering all internal and external body surfaces
- Around glands and their ducts
- Surrounds the smallest blood vessels (capillaries and venules)
- Fills spaces between muscle fibers (endomysium)
- Surrounds peripheral nerves (endoneurium)
- Hypodermis (subcutaneous tissue)
Type 2: Dense Irregular Connective Tissue
Definition
Contains abundant collagen fibers arranged in random (irregular) bundles, with few cells (primarily fibroblasts) and relatively little ground substance.
"Dense irregular connective tissue contains mostly collagen fibers. Cells are sparse and typically of a single type, the fibroblast... Because of its high proportion of collagen fibers, dense irregular connective tissue provides significant strength. Typically, the fibers are arranged in bundles oriented in various directions (thus, the term Irregular) that can withstand stresses on organs or structures." - Histology A Text and Atlas, 7e
Histological Features
- Very thick, eosinophilic collagen bundles randomly interwoven in all directions
- Sparse cell nuclei at low magnification (compared to loose CT)
- Little ground substance
- Elastic fibers are present but less prominent
- Stains densely pink on H&E; intensely blue/green on trichrome stains
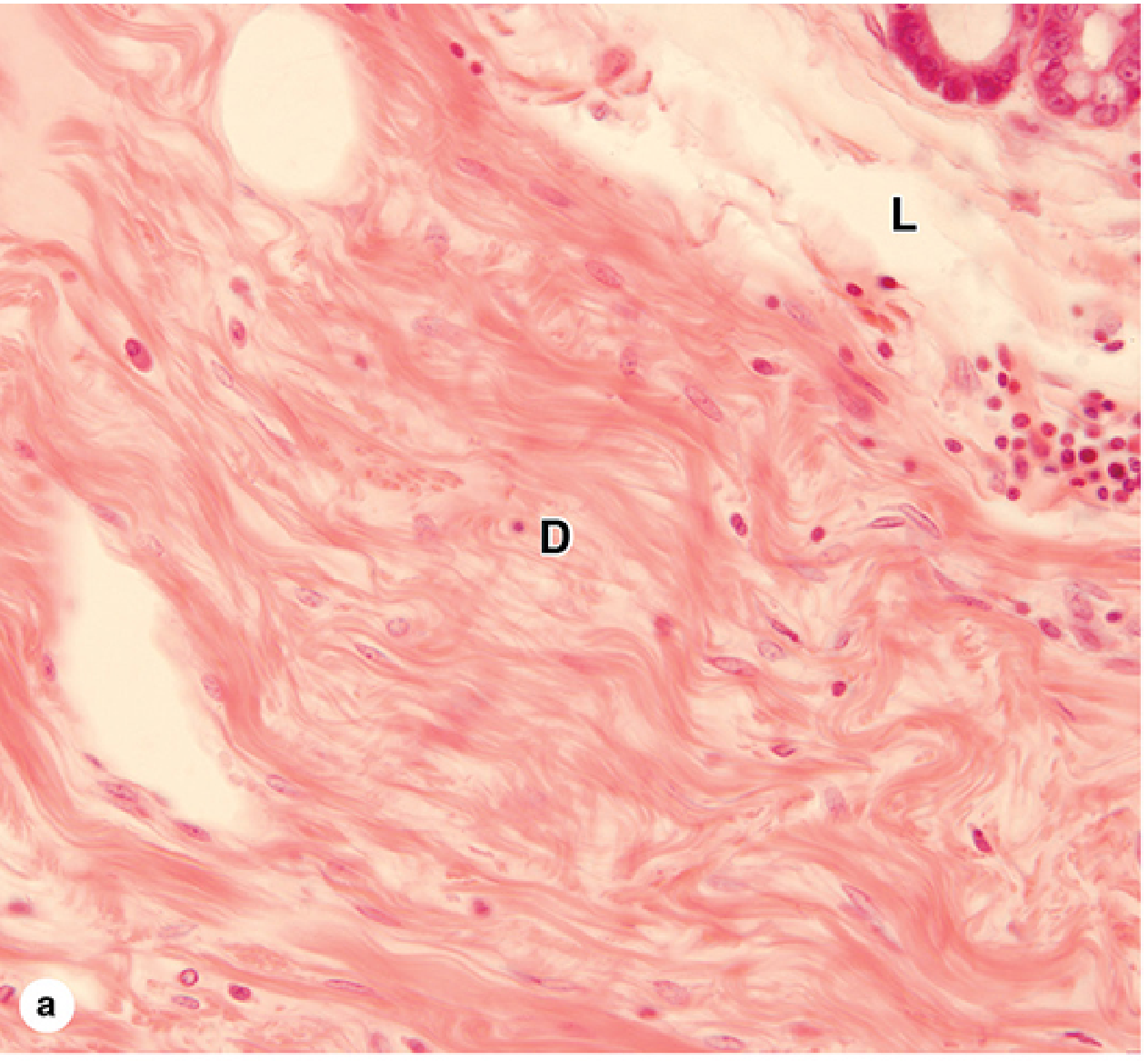
Fig. 2 - Dense irregular (D) and loose (L) CT adjacent in a gland. Junqueira's Basic Histology, 17e (H&E, ×100)
Functional Role
- Provides strength in multiple directions - resists tearing, compression, and stretching forces from all directions simultaneously
- Protects and supports organs
- Resists excessive distension and tearing
Locations
- Reticular layer (deep layer) of the dermis - thick zone providing skin with resistance to tearing
- Organ capsules - surrounds and protects organs (spleen, lymph nodes, testis, liver capsule)
- Submucosa of the GI tract - the distinct dense irregular layer beneath the mucosa
- Periosteum and perichondrium - fibrous outer layer of bone and cartilage
- Sclera of the eye
- Tendon sheaths (epitendineum)
- Fibrous pericardium, dura mater, aponeuroses of the scalp
Type 3: Dense Regular Connective Tissue
Definition
Characterized by densely packed, parallel arrays of collagen fibers with cells (tendinocytes/fibrocytes) aligned between the fiber bundles. The main functional component of tendons, ligaments, and aponeuroses.
"Dense regular connective tissue consists mostly of type I collagen bundles and fibroblasts aligned in parallel for great resistance to prolonged or repeated stresses from the same direction." - Junqueira's Basic Histology, 17e
Histological Features
- Very tightly packed, parallel collagen bundles (all oriented in the same direction) - no ground substance between them
- Cells appear as rows of elongated, flattened (basophilic) nuclei between fiber bundles
- In TEM, tendinocytes show thin cytoplasmic sheets extending between fibrils
- In cross-section, tendinocytes appear stellate
- Almost avascular - appears glistening white in the fresh state
- Very little ground substance
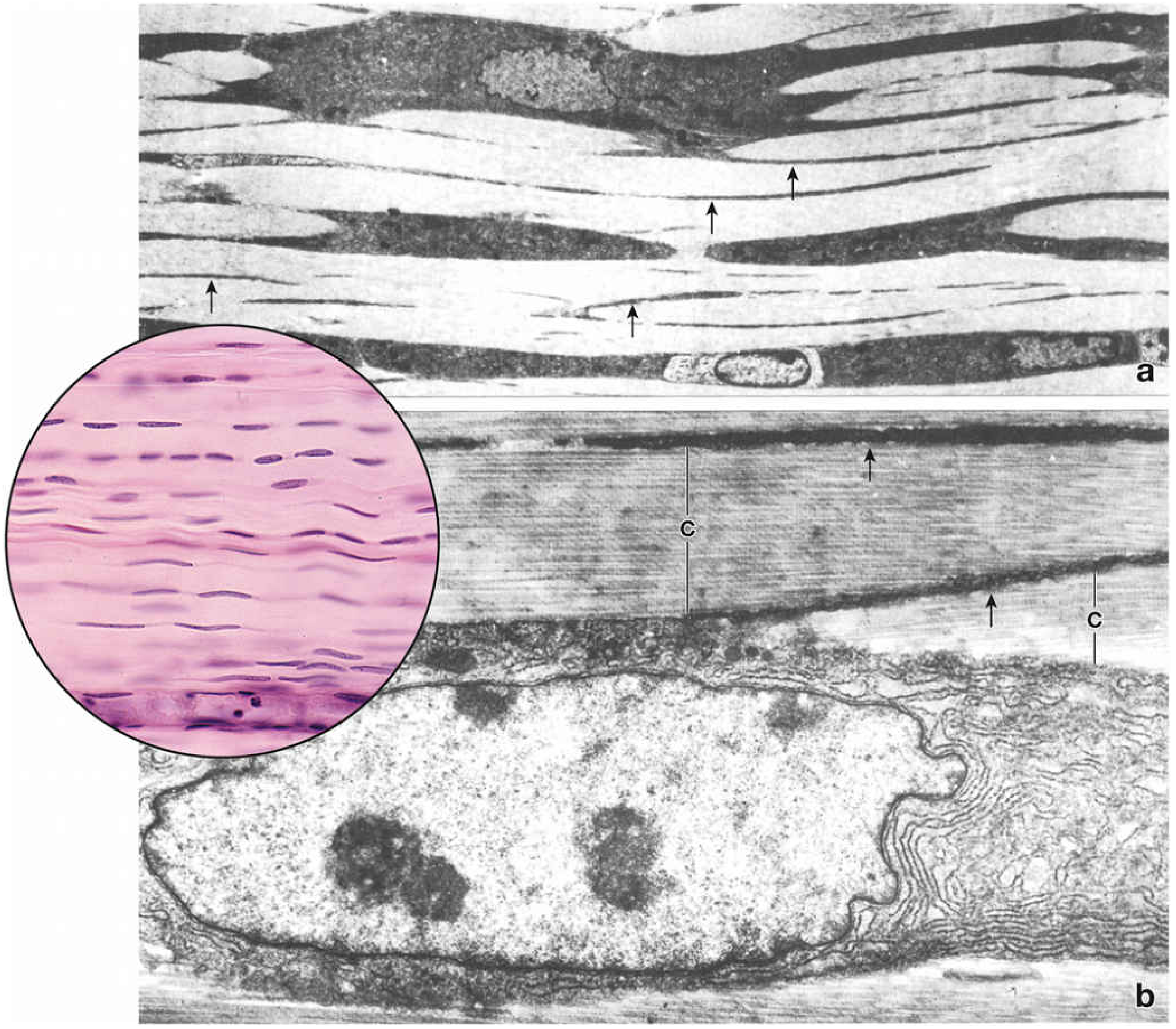
Fig. 3 - Dense regular CT (tendon): EM longitudinal section (top) and TEM cross-section (bottom) showing tendinocyte cytoplasm wrapped around collagen bundles (C). Histology A Text and Atlas, 7e
Functional Role
- Provides maximum tensile strength in one direction
- Transmits the force of muscle contraction to bone (tendons)
- Binds bone to bone (ligaments)
- The quarter-stagger arrangement of collagen molecules + covalent cross-linking gives tensile strength comparable to steel on a per-weight basis
Specific Structures
Tendons
- Cord-like structures attaching muscle to bone
- Consist of parallel bundles of type I collagen
- Cells = tendinocytes (specialized fibroblasts/fibrocytes) in rows between bundles
- Epitendineum - thin dense CT capsule surrounding the tendon
- Endotendineum - connective tissue extensions that subdivide tendon into fascicles, carrying blood vessels and nerves
- Poorly vascularized → slow healing after injury
Ligaments
- Band/sheet-like structures joining bone to bone
- Fibers less strictly parallel than tendons; allow some more flexibility
- Most are predominantly type I collagen ligaments
- Elastic ligaments (e.g., ligamenta flava of vertebral column, ligamentum nuchae) - contain many parallel elastic fiber bundles plus collagen; these require elasticity to allow spinal flexion/extension
Aponeuroses
- Broad, flattened sheet-like tendons
- Collagen bundles are organized in multiple layers at 90° (orthogonal) angles to one another
- Each layer is a regular array, so aponeurosis is still considered dense regular CT
- The same orthogonal arrangement is found in the corneal stroma and is responsible for corneal transparency
Comparative Summary Table
| Feature | Loose CT | Dense Irregular CT | Dense Regular CT |
|---|---|---|---|
| Collagen amount | Sparse, thin | Abundant, thick | Very abundant, parallel |
| Fiber arrangement | Random, loosely scattered | Random bundles (multidirectional) | Strict parallel arrays |
| Cells | Many types, numerous | Few (mainly fibroblasts) | Rows of fibrocytes/tendinocytes |
| Ground substance | Abundant | Little | Minimal |
| Vascularity | Well vascularized | Moderate | Poorly vascularized |
| Main fiber type | Type I, III, elastic | Type I collagen dominant | Type I collagen dominant |
| Mechanical property | Flexibility; metabolic support | Resistance to stress from all directions | Maximum strength in one direction |
| Key locations | Lamina propria, around vessels/glands | Dermis, organ capsules, submucosa | Tendons, ligaments, aponeuroses |
| Staining (H&E) | Pale, many nuclei | Dense pink, few nuclei | Very dense, nuclei in rows |
Clinical Correlations
| Condition | Mechanism | Connective Tissue Relevance |
|---|---|---|
| Scurvy (Vitamin C deficiency) | Impaired hydroxylation of proline/lysine → unstable collagen | Defective collagen synthesis by fibroblasts → bleeding gums, perifollicular hemorrhage, poor wound healing |
| Tendinitis | Overuse of tendon-muscle units → inflammation | Dense regular CT of tendon; poorly vascularized → slow repair; treated with anti-inflammatory agents |
| Marfan syndrome (FBN1 mutation) | Defective fibrillin → poor elastic fiber scaffold | Affects elastic ligaments, aorta; aortic aneurysm, lens dislocation |
| Ehlers-Danlos syndrome | Mutations in collagen genes or processing enzymes | Hyperextensible skin and joints, tissue fragility, poor wound healing |
| Menkes syndrome (ATP7A mutation) | Copper deficiency → lysyl oxidase dysfunction | Defective collagen and elastin cross-linking; arterial aneurysms, loose skin and joints, brittle hair |
| Keloid/hypertrophic scar | Excessive fibroblast activity after injury | Overproduction of type I collagen in dense irregular CT of dermis |
Sources:
- Histology A Text and Atlas With Correlated Cell and Molecular Biology, 7e (Pawlina), pp. 440-535
- Junqueira's Basic Histology - Text and Atlas, 17e, pp. 257-310
This is a shared conversation. Sign in to Orris to start your own chat.