JUNCTIONAL RHYTHM
Comprehensive MD Medicine Notes
Sources: Tintinalli's Emergency Medicine | Harrison's Principles of Internal Medicine 22E | Braunwald's Heart Disease | Goldman-Cecil Medicine | Rosen's Emergency Medicine | Katzung's Basic & Clinical Pharmacology | Harriet Lane Handbook | Frameworks for Internal Medicine
SECTION 1: DEFINITION
1.1 Definition of Junctional Rhythm
A junctional rhythm is any cardiac rhythm that originates from the AV junction (AV node or His bundle region) rather than the SA node. It results from either:
- Escape mechanism: the SA node fires too slowly or fails, and the AV junction assumes pacemaker function
- Enhanced automaticity: the AV junction fires faster than the SA node, overriding it
"Under normal circumstances, the SA node discharges at a faster rate than the AV node, so the pacemaker function of the AV node and all other slower pacemakers are suppressed." - Tintinalli's Emergency Medicine
1.2 Anatomy and Physiology of the AV Junction
The AV junction comprises:
Atrial myocardium
|
[AV Node] ← compact node, located in Koch's triangle
| (bounded by: tendon of Todaro, tricuspid annulus,
| orifice of coronary sinus)
[Bundle of His] ← penetrates the central fibrous body
|
[Bundle Branches] → Left + Right
|
[Purkinje fibers]
Koch's Triangle Boundaries:
| Boundary | Structure |
|---|
| Anterior-superior | Tendon of Todaro |
| Inferior | Tricuspid valve annulus |
| Base | Opening of coronary sinus |
Blood supply of AV node:
- 90%: Right coronary artery (posterior descending branch) - hence inferior MI affects it
- 10%: Left circumflex artery
Innervation:
- Rich autonomic innervation: parasympathetic (vagal) slows, sympathetic speeds
- Intrinsic rate of AV junction: 40-60 bpm
1.3 Normal Pacemaker Hierarchy
┌─────────────────────────────────────────────────────────┐
│ NORMAL PACEMAKER HIERARCHY │
├──────────────────┬────────────────┬─────────────────────┤
│ Pacemaker │ Location │ Intrinsic Rate │
├──────────────────┼────────────────┼─────────────────────┤
│ SA Node │ Right atrium │ 60-100 bpm ← BOSS │
│ AV Junction │ AV node/His │ 40-60 bpm │
│ Purkinje/Vent. │ Ventricles │ 20-40 bpm │
└──────────────────┴────────────────┴─────────────────────┘
- The SA node is primary pacemaker because it has the fastest spontaneous depolarization
- Subsidiary pacemakers are suppressed by overdrive suppression - when a faster pacemaker depolarizes them, they reset
- If the SA node slows or fails, the AV junction "escapes" and becomes the dominant pacemaker
1.4 Escape Rhythm vs Accelerated Rhythm
| Feature | Escape Rhythm | Accelerated Rhythm |
|---|
| Mechanism | Passive - SA node fails | Active - AV junction fires faster than SA node |
| Rate | 40-60 bpm (at intrinsic rate) | 60-100 bpm (faster than intrinsic, slower than tachycardia) |
| Clinical context | SA node disease, high vagal tone | Digoxin toxicity, inferior MI, post-surgery |
| Significance | Protective mechanism | May indicate pathology |
| SA node firing? | No (or too slow) | Yes, but "outrun" by junction |
Pearl: Junctional escape is a life-saving protective response. Never suppress it without ensuring another pacemaker is present.
SECTION 2: ELECTROPHYSIOLOGY
2.1 Automaticity of the AV Junction
- Automaticity = ability of cardiac cells to spontaneously depolarize during phase 4 of the action potential (slow diastolic depolarization via the "funny current" - If)
- AV nodal cells have less steep phase 4 slope compared to SA node → slower intrinsic rate (40-60 bpm)
- AV nodal cells use L-type calcium channels for phase 0 (slow action potential) unlike atrial/ventricular cells (fast Na+ channels)
Ion currents in AV junction automaticity:
| Current | Role |
|---|
| If (funny/pacemaker current) | Phase 4 slow depolarization |
| ICa-L (L-type Ca2+) | Phase 0 upstroke |
| IK (delayed rectifier K+) | Phase 3 repolarization |
| INa | Minimal role in nodal cells |
2.2 Escape Mechanism
When the SA node fails or fires too slowly:
- AV junction cells are no longer suppressed by overdrive
- They complete their own intrinsic phase 4 depolarization
- An escape beat fires at 40-60 bpm
- If this continues: junctional escape rhythm
Escape interval = the interval from the last sinus beat to the first junctional escape beat (typically 1000-1500 ms)
2.3 Enhanced Automaticity
- Catecholamines, ischemia, digoxin toxicity, or electrolyte disturbances steepen phase 4 slope of AV junction cells
- This causes the junction to fire faster than the SA node
- Results in: accelerated junctional rhythm (60-100 bpm) or junctional tachycardia (>100 bpm)
- Mechanism: increased If current, enhanced Ca2+ influx, or decreased K+ efflux
2.4 Re-entry Mechanism
Some junctional tachycardias (notably AVNRT) are re-entrant:
ATRIUM
|
┌──────┴──────┐
│ FAST pathway │ (alpha, short refractory)
│ │
│ SLOW pathway│ (beta, long refractory)
└──────┬──────┘
|
VENTRICLE
In typical AVNRT:
- Anterograde: down slow pathway
- Retrograde: up fast pathway
- Creates a rapid circuit → P wave buried in or just after QRS
Note: True junctional tachycardia (focal JT) is automatic, NOT re-entrant - this distinguishes it from AVNRT.
2.5 Influence of Autonomic Tone
| Autonomic Tone | Effect on AV Junction | Mechanism |
|---|
| Parasympathetic (vagal) | Slows rate, may cause junctional escape | Acetylcholine → M2 receptors → ↑ IK-Ach → hyperpolarization + ↓ If |
| Sympathetic | Speeds rate, may trigger accelerated JR or JT | Catecholamines → β1 receptors → ↑ cAMP → ↑ If and ICa-L |
| High vagal tone (athletes, sleep) | Promotes junctional escape at rest | - |
| Sympathetic surge (fever, surgery, catecholamines) | Promotes accelerated JR/JT | - |
SECTION 3: CLASSIFICATION
3.1 Overview Table
| Type | Rate | Mechanism | Clinical Setting |
|---|
| Junctional Escape Rhythm | 40-60 bpm | Passive escape | SA node failure, high vagal tone |
| Accelerated Junctional Rhythm | 60-100 bpm | Enhanced automaticity | Digoxin toxicity, inferior MI, post-cardiac surgery |
| Junctional Tachycardia | >100 bpm | Enhanced automaticity | Digoxin tox, myocarditis, post-surgery |
| Non-paroxysmal JT (NPJT) | 70-130 bpm | Enhanced automaticity | Digoxin toxicity (classic), acute inferior MI |
| Congenital JET | >200 bpm | Enhanced automaticity | Infants <6 months, structural CHD |
| Postoperative JET | 170-260 bpm | Enhanced automaticity | After congenital heart surgery |
3.2 Junctional Escape Rhythm (40-60 bpm)
ECG Pattern:
Lead II:
___ ___ ___
/ \ / \ / \
________/ \_____/ \_____/ \____
No P wave No P wave
Rate: 40-60 bpm | Regular | Narrow QRS | No preceding P wave
ECG Features:
- Rate: 40-60 bpm
- Regular rhythm
- Narrow QRS (<120 ms) unless aberrant conduction
- No P wave before QRS, or inverted P in inferior leads (retrograde)
- If retrograde: P wave immediately BEFORE QRS (very short PR, <120 ms) OR AFTER QRS
Clinical significance: Protective escape in the setting of SA node failure, sinus bradycardia, complete heart block
ECG from Textbook of Family Medicine (Junctional rhythm - junctional rate dominates):
Lead II: Regular narrow QRS complexes at ~50 bpm with no clear upright P waves preceding each complex - classic junctional escape rhythm
3.3 Accelerated Junctional Rhythm (60-100 bpm)
ECG Pattern:
Lead II:
P' P' P' P' P' P'
/\_ /\_ /\_
__/ \__________/ \__________/ \__
(inverted/retrograde P waves near QRS)
Rate: 60-100 bpm | Regular | Narrow QRS
ECG Features:
- Rate: 60-100 bpm (faster than normal junctional escape, but not tachycardia)
- Regular
- Narrow QRS
- P waves: inverted in II, III, aVF; may be before, within, or after QRS
- AV dissociation may be present if SA node continues firing independently
Defining feature per Harrison's 22E: "Paroxysmal regular rhythm with P waves visible at the end of the QRS complex or not visible at all."
Clinical: Digoxin toxicity, inferior wall MI, post-cardiac surgery, reperfusion arrhythmia, rheumatic fever
3.4 Junctional Tachycardia (>100 bpm)
ECG Pattern:
Lead II:
P'P'P'P'P'P'P'P'P'
|__|__|__|__|__|__|
[narrow QRS complexes, ~120-130 bpm]
P' = inverted/buried, retrograde
Rate: >100 bpm | Regular | Narrow QRS
From Braunwald's Heart Disease:
"Junctional tachycardia (ectopic junctional tachycardia) is a rare form of SVT in which the ECG resembles AVNRT but is distinct in that (1) the mechanism is automatic, not reentrant, and (2) the atrium is clearly not involved in the tachycardia. This disorder is most often observed in young healthy individuals, in women more often than in men, and is usually catecholamine dependent."
From Rosen's Emergency Medicine:
"JT shows sustained ventricular rates but rarely exceeds 130 bpm. JT is associated with structural heart disease, metabolic disturbances, or drug toxicity."
ECG differential from AVNRT:
- AVNRT: re-entrant, onset/offset paroxysmal, adenosine terminates
- JT: automatic, gradual onset (warm-up), adenosine may transiently suppress but does NOT terminate
3.5 Non-Paroxysmal Junctional Tachycardia (NPJT)
- Rate: 70-130 bpm (most commonly 70-130)
- Onset and termination: gradual (not abrupt - "warm up/cool down" pattern)
- Mechanism: enhanced automaticity
- Classic cause: digitalis toxicity (especially when combined with atrial fibrillation - fibrillatory baseline with regular QRS = NPJT)
- Also: inferior MI, acute rheumatic fever, myocarditis, post-cardiac surgery
- ECG: regular narrow QRS, retrograde P waves, AV dissociation possible
- Treatment: remove offending drug (digoxin), treat underlying cause
3.6 Congenital Junctional Ectopic Tachycardia (Congenital JET)
| Feature | Details |
|---|
| Age | Infants, usually <6 months |
| Rate | Often >200 bpm |
| Mechanism | Enhanced automaticity (possibly genetic channelopathy) |
| ECG | Narrow QRS, retrograde or AV dissociation, "warm-up" pattern |
| Clinical | Heart failure, hydrops, cardiomegaly |
| Prognosis | Poor without treatment; may resolve spontaneously in some |
| Treatment | Amiodarone, propafenone; cooling (mild hypothermia); catheter ablation (high risk near His bundle) |
3.7 Postoperative Junctional Ectopic Tachycardia (Postoperative JET)
| Feature | Details |
|---|
| Setting | Pediatric congenital heart surgery (VSD repair, TOF repair, Fontan) |
| Timing | Within 24-48 hours post-op |
| Rate | 170-260 bpm |
| Mechanism | Enhanced automaticity due to trauma/edema near His bundle |
| ECG | Narrow QRS (usually), AV dissociation, more V's than A's |
| Hemodynamics | Often severely hemodynamically compromising |
| Treatment | Cooling (36°C), amiodarone, dexmedetomidine, procainamide, atrial pacing faster than JET rate (to restore AV synchrony) |
Recent Evidence: A 2026 systematic review and meta-analysis (PMID: 41845224) found that ivabradine may be effective for postoperative JET by blocking the If current, reducing the junctional rate. This is an emerging therapeutic option.
SECTION 4: ETIOLOGY
4.1 Comprehensive Etiologic Classification Table
| Category | Cause | Mechanism | Pearl |
|---|
| Physiological | Athletes, sleep, vagal tone | High resting vagal tone | Often asymptomatic, benign |
| SA Node Disease | Sick sinus syndrome | SA node fails → junctional escape | May need pacemaker |
| Sinus arrest | Prolonged sinus pause | Escape rhythm is protective |
| SA exit block | SA impulse blocked from leaving | P-P pause is multiple of basic cycle |
| AV Conduction | Complete AV block (3rd degree) | No AV conduction → junctional escape | Wide QRS if below His |
| Ischemia | Inferior wall MI (RCA territory) | AV node ischemia (RCA supplies node in 90%) | Transient, usually resolves |
| Reperfusion arrhythmia | Enhanced automaticity post-reperfusion | Self-limiting |
| Inflammatory | Myocarditis | Inflammatory damage to conduction system | May be severe |
| Acute rheumatic fever | Carditis affecting AV node | Classic teaching |
| Endocarditis | Direct invasion | Rare |
| Post-surgical | Cardiac surgery | Trauma/edema near His bundle | Commonest post-op arrhythmia in pediatric CHD surgery |
| Drug-induced | Digoxin toxicity | Enhanced AV junctional automaticity | Classic NPJT at 70-130 bpm over AF baseline |
| Beta-blockers | SA suppression → junctional escape | Rate-related, dose-related |
| Calcium channel blockers (diltiazem, verapamil) | SA/AV node suppression | Non-dihydropyridines |
| Amiodarone | SA suppression | Chronic use |
| Ivabradine | If channel blockade | At high doses |
| Adenosine | Transient AV block → escape | Expected; transient |
| Electrolyte | Hypokalemia | Increased automaticity | Also with digoxin - synergistic toxicity |
| Hyperkalemia | SA arrest → junctional escape | Life-threatening |
| Hypomagnesemia | Arrhythmogenesis | Often coexists with hypokalemia |
| Hypocalcemia | Arrhythmias | Rare |
| Metabolic | Hypoxia | Enhanced automaticity | ICU, respiratory failure |
| Acidosis | Cellular dysfunction | Multifactorial |
| Structural | Congenital heart disease | Structural anomalies of conduction | Post-surgical especially |
| Sleep | Sleep apnea | Vagal surges during apnea | Nocturnal bradycardia/junctional escape |
| Athlete's heart | Enhanced vagal tone | Resting junctional rhythm - benign |
| Idiopathic | No identifiable cause | Unknown | Often young women (catecholamine-dependent JT) |
4.2 Memory Aid - "DISCHARGE" Mnemonic for Junctional Rhythm Causes
D - Digitalis toxicity
I - Ischemia (inferior MI), Idiopathic
S - Sick sinus syndrome, Surgery (cardiac), Sleep apnea
C - Calcium channel blockers, Congenital HD
H - Hyperkalemia, Hypokalemia, Hypoxia
A - Athletes (physiological), Amiodarone
R - Rheumatic fever, Reperfusion
G - (vagal) Greater vagal tone
E - Electrolyte abnormalities
SECTION 5: ECG DIAGNOSIS (DETAILED)
5.1 Stepwise ECG Interpretation
STEP 1: RATE
├── Count QRS complexes in 6-second strip × 10
├── OR 300 ÷ (large boxes between QRS)
└── Junctional: 40-60 (escape), 60-100 (accelerated), >100 (JT)
STEP 2: RHYTHM REGULARITY
├── Measure R-R intervals
└── Junctional rhythm = REGULAR (unlike AF)
STEP 3: P WAVE ANALYSIS (KEY!)
├── Is there a P wave?
├── Is P wave UPRIGHT in leads I, II, aVF? → Sinus origin
├── Is P wave INVERTED in II, III, aVF? → Retrograde (junctional)
├── Where is P relative to QRS?
│ ├── BEFORE QRS (PR < 120 ms) → Junctional with retrograde atrial activation
│ ├── WITHIN QRS (buried) → P not visible; QRS appears P-waveless
│ └── AFTER QRS (RP < 200 ms) → Junctional with retrograde conduction after ventricles
└── No P wave visible at all → Buried or absent retrograde conduction
STEP 4: PR INTERVAL
├── Normal sinus: 120-200 ms
├── Junctional: If P before QRS → PR <120 ms (retrograde)
└── AV dissociation: Variable PR (no fixed relationship)
STEP 5: QRS DURATION
├── Narrow (<120 ms) = Junctional (supraventricular)
└── Wide (>120 ms) = Aberrant conduction OR ventricular origin
STEP 6: LOOK FOR AV DISSOCIATION
└── P waves and QRS independent, with junctional rate > atrial rate
STEP 7: CAPTURE AND FUSION BEATS
├── Capture beat: occasional sinus impulse "captures" ventricle → normal-looking QRS
└── Fusion beat: simultaneous activation from SA and junctional → hybrid QRS morphology
5.2 ECG Diagrams - All P Wave Patterns
Pattern A: No P Wave (P buried in QRS)
Lead II
| | | |
─────────|─────────|─────────|─────────|──────
/|\ /|\ /|\ /|\
/ | \ / | \ / | \ / | \
──────/ | \───/ | \───/ | \───/ | \──
QRS (no P visible - buried inside QRS)
Rate: ~50 bpm | No P waves discernible | Narrow QRS
DIAGNOSIS: Junctional rhythm with P wave buried in QRS
Pattern B: Inverted P BEFORE QRS (short PR)
Lead II
P' P' P' P'
| | | |
─v──|──/\─v──|──/\─v──|──/\─v──|──/\──
QRS QRS QRS QRS
P' = inverted (negative) in II, III, aVF
PR interval < 120 ms (retrograde fast conduction)
DIAGNOSIS: Junctional with retrograde P before QRS
Pattern C: Inverted P AFTER QRS (short RP)
Lead II
/\ P' /\ P' /\ P' /\ P'
──/ \─\──v─/ \─\──v─/ \─\──v─/ \─\──v─
QRS QRS QRS QRS
RP interval < 200 ms
DIAGNOSIS: Junctional rhythm with retrograde P after QRS (most common pattern)
Pattern D: P Wave Simultaneous with QRS (P in QRS)
↕P merged with QRS
─────/\/\──────/\/\──────/\/\───
QRS+P QRS+P QRS+P
Cannot see P wave on surface ECG
DIAGNOSIS: Synchronous retrograde activation - P hidden in QRS
Pattern E: AV Dissociation (P waves walking through QRS)
Lead II showing AV dissociation:
P P P P P P P P P P P (atrial rate: 60 bpm - slower)
| | | | | | | | | | |
| | | | | |
J J J J J (junctional rate: 80 bpm - faster)
/\ /\ /\ /\ /\
P waves march THROUGH QRS complexes
P-QRS relationship constantly changing
DIAGNOSIS: Accelerated junctional rhythm with AV dissociation
↑
Capture beat here (P happens to precede
QRS with appropriate PR → normal-looking beat)
5.3 Key ECG Parameters Summary Table
| Parameter | Junctional Escape | Accelerated JR | Junctional Tachycardia | AVNRT (for comparison) |
|---|
| Rate | 40-60 bpm | 60-100 bpm | >100 bpm | 150-250 bpm |
| Rhythm | Regular | Regular | Regular | Regular |
| P wave | Absent/retrograde | Absent/retrograde | Absent/retrograde | Retrograde (in/after QRS) |
| PR interval | <120 ms if present | <120 ms if present | <120 ms if present | N/A (retrograde) |
| RP interval | Variable | Variable | <70 ms | <70 ms (typical AVNRT) |
| QRS duration | Narrow | Narrow | Narrow | Narrow |
| AV dissociation | Sometimes | Sometimes | Sometimes | No |
| Capture beats | Sometimes | Yes | Yes | No |
| Fusion beats | Rare | Yes | Yes | No |
| Onset | Gradual | Gradual | Gradual | Abrupt (paroxysmal) |
| Adenosine | Temporary slowing | Temporary slowing | Temporary slowing | Terminates |
5.4 Retrograde Atrial Activation
- AV junction impulse travels RETROGRADE from AV node up to atria
- Atria activated from below upward (inferior to superior)
- Results in:
- Lead II, III, aVF: Inverted P wave (negative)
- Lead aVR: Positive P wave
- Lead I: Usually isoelectric or slightly negative
Normal sinus: Retrograde:
+P in II -P in II
↓ ↑
Atria activate Atria activate
top → bottom bottom → top
(SA node high) (AV node low)
5.5 Capture and Fusion Beats
Capture Beat:
- During AV dissociation, an occasional sinus P wave arrives at the ventricles at just the right time (outside junctional refractory period)
- The sinus impulse "captures" the ventricles → produces a normal-looking narrow QRS
- Confirms AV dissociation is NOT complete
- Importance: Capture beats PROVE that the rhythm is ventricular (if in VT) or junctional (if in accelerated JR)
Fusion Beat:
- Simultaneous activation of ventricles from BOTH the junctional pacemaker AND a descending sinus impulse
- Produces a QRS morphology intermediate between normal sinus QRS and junctional QRS
- Confirms: two competing pacemakers
Fusion beat morphology:
Sinus alone: Normal QRS
Junctional alone: Also narrow QRS (same morphology in junctional)
Fusion: Hybrid - often subtle difference in morphology
5.6 Diagnostic Flowchart for ECG Interpretation
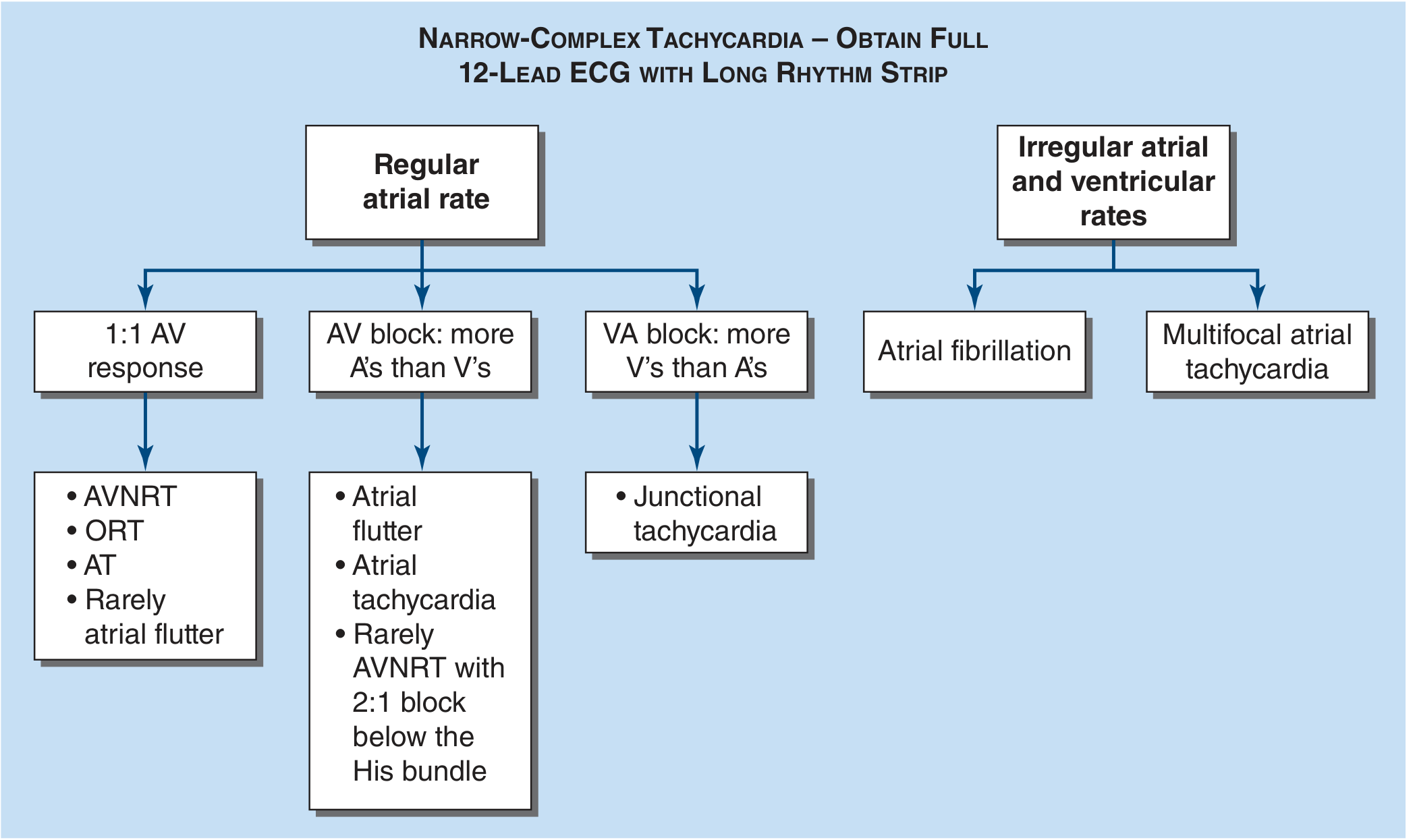
Here is the diagnostic approach based on Harrison's SVT flowchart (from the textbook):
FIGURE: Diagnostic approach to SVT. Junctional tachycardia characteristically shows more V's than A's (VA block: more ventricles than atria), distinguishing it from AVNRT and AT. (Harrison's Principles of Internal Medicine 22E)
SECTION 6: ECG DIFFERENTIAL DIAGNOSIS
6.1 Master Differential Comparison Table
| Feature | Sinus Brady | Junctional Escape | Low Atrial Rhythm | AVNRT | JT (Focal) | Ventricular Escape | AIVR | Complete HB |
|---|
| Rate | <60 | 40-60 | 40-100 | 150-250 | >100 | 20-40 | 50-110 | Variable |
| P wave | Normal upright | Absent/retrograde | Different morphology | Retrograde | Absent/retrograde | Absent/dissociated | Absent/dissociated | Upright, dissociated |
| PR interval | Normal (120-200) | <120 or none | Short-normal | N/A | <120 or none | None | None | Variable, no fixed |
| QRS | Narrow | Narrow | Narrow | Narrow | Narrow | Wide | Wide | Narrow or Wide |
| Onset | Gradual | Gradual | Gradual | Abrupt | Gradual | Gradual | Gradual | May be sudden |
| Adenosine | Slight slowing | Temporary slowing | Variable | Terminates | Temporary slowing | No effect | No effect | No effect |
| Key differentiator | P upright, normal PR | No P or retrograde | Abnormal P axis | Paroxysmal, retrograde short RP | Gradual, automatic | Wide QRS | Wide QRS, accelerated | P-QRS dissociation, wide escape |
6.2 Junctional vs Sinus Bradycardia
| Feature | Sinus Bradycardia | Junctional Escape |
|---|
| P wave | Upright in I, II, aVF | Absent, or inverted in II/III/aVF |
| PR interval | Normal (>120 ms) | Short (<120 ms) if P present |
| Atropine response | Increases rate | May increase if SA node responds |
| Cause | Vagal tone, hypothyroidism, athletes | SA node failure |
6.3 Junctional vs Complete Heart Block
| Feature | Junctional Escape in CHB | Ventricular Escape in CHB |
|---|
| QRS morphology | Narrow | Wide (>120 ms) |
| Rate | 40-60 bpm | 20-40 bpm |
| P waves | Dissociated, upright, faster | Dissociated, upright, faster |
| Stability | More stable | Less stable, more symptomatic |
6.4 Junctional Tachycardia vs AVNRT
This is the most important and clinically challenging differential:
| Feature | Focal Junctional Tachycardia | AVNRT |
|---|
| Mechanism | Enhanced automaticity | Re-entry |
| Onset | Gradual (warm-up) | Abrupt (paroxysmal) |
| Termination | Gradual (cool-down) | Abrupt |
| Adenosine | Temporarily slows, then resumes | Terminates |
| Vagal maneuvers | May slow transiently | May terminate |
| AV dissociation | May occur | Never (atrium required) |
| P wave | Retrograde or AV dissociation | Retrograde, very short RP |
| Atrium required? | NO | YES |
| Catecholamine sensitivity | Yes (isoproterenol provokes) | Variable |
| Rate | Usually <130 bpm | 150-250 bpm |
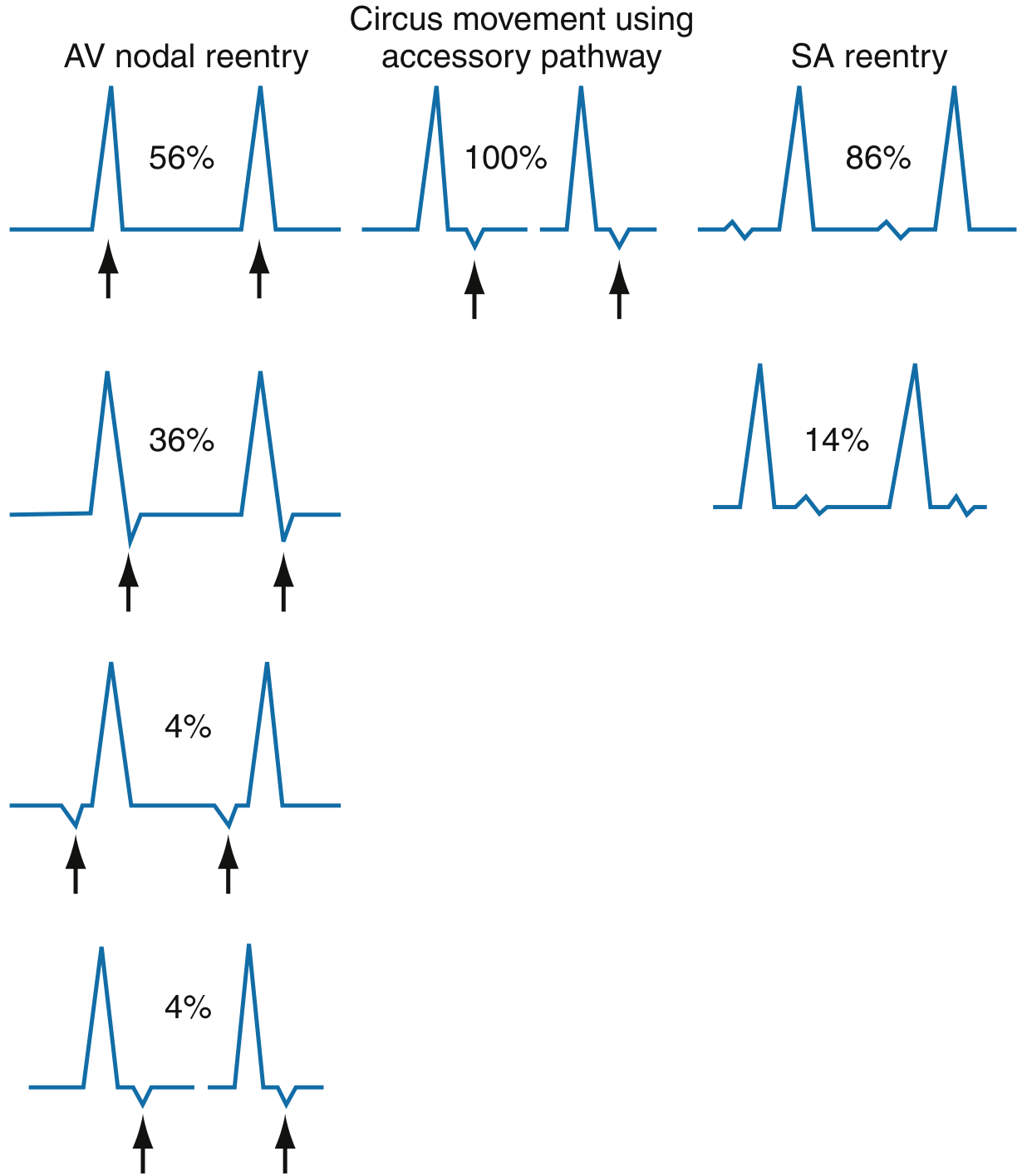
P wave location diagram (from Rosen's Emergency Medicine):
P wave location patterns in various SVT subtypes. In AVNRT: P buried within or just after QRS (56-36% patterns shown). In accessory pathway tachycardia: P clearly after QRS. In focal JT: P may show AV dissociation (more V's than A's).
6.5 Junctional vs Accelerated Idioventricular Rhythm (AIVR)
| Feature | Accelerated Junctional | AIVR |
|---|
| QRS duration | Narrow (<120 ms) | Wide (>120 ms) |
| Rate | 60-100 bpm | 50-110 bpm |
| P wave | May be retrograde | Absent or dissociated |
| Clinical | Digoxin, inferior MI | Reperfusion, inferior MI |
| Treatment | Treat cause | Usually no treatment needed |
SECTION 7: CLINICAL FEATURES
7.1 Symptoms
| Symptom | Mechanism | When present |
|---|
| Asymptomatic | Well-tolerated if rate adequate | Common in escape rhythms |
| Palpitations | Awareness of irregular/slow beat | Any junctional rhythm |
| Presyncope/Lightheadedness | Reduced cardiac output | Slow escape rhythm |
| Syncope | Severe reduction in cardiac output | Slow junctional escape in CHB |
| Dyspnea/Fatigue | Reduced CO, AV dyssynchrony | Accelerated JR, JT |
| Chest discomfort | Reduced coronary perfusion | JT with rapid rate |
| Heart failure symptoms | AV dyssynchrony, reduced CO | Sustained JT, post-surgical JET |
| Cardiogenic shock | Severe CO reduction | JET in post-surgical infants |
7.2 Signs
| Sign | Mechanism | Clinical Note |
|---|
| Bradycardia | Slow junctional escape | Check pulse: regular vs irregular |
| Cannon A waves | Atrial contraction against closed tricuspid valve | Seen in AV dissociation; intermittent large jugular pulsations |
| Variable S1 intensity | Changing PR interval in AV dissociation | Correlates with P-QRS relationship |
| Hypotension | Reduced CO | More severe with fast JT in structural disease |
| Signs of heart failure | Sustained arrhythmia | Edema, elevated JVP, crackles |
| Signs of underlying cause | e.g., inferior MI (diaphoresis), digoxin toxicity (xanthopsia, GI symptoms) | Guide etiology |
7.3 Hemodynamic Effects and Cannon A Waves
Normal cardiac physiology: Atrial contraction (P wave) → atrial kick → increases ventricular preload → enhances CO by ~20-30%
AV Dyssynchrony in junctional rhythm:
- When P and QRS are dissociated, atria may contract AGAINST CLOSED AV VALVES
- This produces: Cannon A waves in JVP (visible neck pulsation)
- Loss of atrial kick → reduces CO by 20-30% in patients with poor LV function
Cannon A Wave Physiology:
Atrium contracts ──→ Tricuspid CLOSED (ventricle already contracting)
──→ Blood forced BACKWARD into vena cava
──→ Giant pulsation in jugular vein = CANNON A WAVE
Classic causes of cannon A waves:
• AV dissociation (junctional rhythm, VT, CHB)
• Tricuspid stenosis
• Right heart failure (giant "a" waves)
SECTION 8: DIAGNOSTIC EVALUATION
8.1 History
Key questions:
- Onset (gradual vs sudden), duration, triggers
- Associated symptoms (syncope, chest pain, dyspnea)
- Drug history: digoxin, beta-blockers, CCBs, amiodarone
- Cardiac history: previous MI (especially inferior), CHD, cardiac surgery
- Symptoms of hypothyroidism, electrolyte disorders
- Family history (congenital JET)
- Athletic history
8.2 Physical Examination
- Vital signs: HR, BP, SpO2, RR
- Pulse: rate, rhythm (regular in junctional)
- JVP: cannon A waves (AV dissociation), elevated (heart failure)
- Carotid sinus massage (CSM): may slow or reveal underlying atrial activity
- Cardiac auscultation: variable S1 intensity (AV dissociation), S3/S4 (heart failure)
- Signs of digoxin toxicity: GI, neurological (yellow-green vision)
8.3 Laboratory Investigations
| Test | Rationale |
|---|
| Serum electrolytes (Na, K, Cl, HCO3) | Hypo/hyperkalemia, hypomagnesemia |
| Serum calcium | Hypocalcemia |
| Serum magnesium | Hypomagnesemia (potentiates arrhythmia) |
| Digoxin level | Toxicity threshold generally >2 ng/mL (therapeutic 0.5-2 ng/mL) |
| Thyroid function (TSH, fT4) | Hypothyroidism (bradycardia) or hyperthyroidism (tachycardia) |
| Troponin I/T | Myocardial injury (inferior MI, myocarditis) |
| CBC | Anemia (compensatory tachycardia), infection |
| ABG | Hypoxia, acidosis |
| BMP/CMP | Renal function (affects drug clearance) |
| CRP, ESR | Myocarditis, rheumatic fever |
| ASO titer | Acute rheumatic fever |
8.4 Cardiac Investigations
| Investigation | Indication | Findings |
|---|
| 12-lead ECG | First test always | Rate, rhythm, P-QRS relationships, ST changes |
| Continuous monitoring/Telemetry | Inpatient monitoring, ICU | Dynamic rhythm changes, capture beats |
| Holter monitor (24-48h) | Intermittent/symptomatic rhythm | Frequency, correlation with symptoms |
| Event recorder | Infrequent episodes | Patient-triggered recording |
| Exercise ECG | Rate-dependent arrhythmia | Response to catecholamines |
| Echocardiography | Structural disease, function | LV/RV function, valvular disease, CHD |
| Electrophysiology study (EPS) | Confirm mechanism, ablation planning | Confirms enhanced automaticity vs re-entry |
| Cardiac MRI | Myocarditis, structural disease | Myocardial edema, fibrosis (late gadolinium enhancement) |
| Coronary angiography | Suspected ischemic cause | CAD assessment |
SECTION 9: APPROACH TO JUNCTIONAL RHYTHM
9.1 Clinical Algorithm / Flowchart
┌─────────────────────────────────────────────────────────────────┐
│ PATIENT PRESENTING WITH JUNCTIONAL RHYTHM │
└──────────────────────────┬──────────────────────────────────────┘
↓
┌────────────────────────┐
│ 12-LEAD ECG + VITALS │
└────────────┬───────────┘
↓
┌────────────────┴────────────────┐
↓ ↓
UNSTABLE PATIENT STABLE PATIENT
(SBP <90, altered MS, (Alert, BP adequate,
chest pain, severe HF) no shock)
│ │
↓ ↓
IMMEDIATE: IDENTIFY SUBTYPE:
• IV access • Escape (40-60 bpm)?
• O2 supplementation • Accelerated (60-100)?
• Monitoring • JT (>100 bpm)?
• Atropine 0.5mg IV │
• If no response: IDENTIFY CAUSE:
Transcutaneous pacing • Check digoxin level
• Prepare for transvenous • Electrolytes
pacing • Troponin
│ • Echocardiogram
↓ │
TREAT CAUSE TREAT REVERSIBLE CAUSE
(adjust/stop offending (stop drug, correct electrolyte,
drugs, reperfuse if MI) treat ischemia/infection)
│ │
↓ ↓
PERSISTENT SYMPTOMATIC REASSESS:
BRADYCARDIA? • Rhythm resolved? → Follow-up
│ • Persists symptomatically? →
↓ Consider permanent pacemaker
PERMANENT PACEMAKER • Ablation if JT refractory
(see indications below)
SECTION 10: ACUTE MANAGEMENT
10.1 ACC/AHA/ESC Guideline-Based Management
Stable Patient
STABLE JUNCTIONAL RHYTHM
↓
Is the rate adequate (>40 bpm with no symptoms)?
|
YES → Monitor, identify cause, no immediate treatment
|
NO (symptomatic bradycardia from escape rhythm)
↓
┌──────────────────────────────────┐
│ 1. O2 (maintain SpO2 >94%) │
│ 2. IV access │
│ 3. Cardiac monitoring │
│ 4. 12-lead ECG, labs │
│ 5. TREAT UNDERLYING CAUSE │
│ • Stop digoxin │
│ • Correct hypokalemia │
│ • Treat inferior MI │
└──────────────────────────────────┘
↓
If symptomatic (lightheaded, low BP):
ATROPINE 0.5 mg IV → repeat q3-5 min → max 3 mg
↓
Response? → Observe, monitor
No response? → Consider temporary pacing
Unstable Patient
UNSTABLE PATIENT (hypotension, syncope, altered consciousness,
angina, acute pulmonary edema)
↓
┌──────────────────────────────────────────┐
│ IMMEDIATE STABILIZATION │
│ 1. O2 via face mask / intubate if needed │
│ 2. IV access (large bore, bilateral) │
│ 3. Continuous ECG monitoring │
│ 4. 12-lead ECG │
└──────────────────────┬───────────────────┘
↓
ATROPINE 0.5 mg IV
Repeat every 3-5 min, max 3 mg
↓
Response?
YES ─────────────────→ Monitor, treat cause
NO
↓
┌─────────────────────────────────────┐
│ TRANSCUTANEOUS PACING (TCP) │
│ • Start immediately while │
│ arranging transvenous pacing │
│ • Rate: 60-80 bpm initially │
│ • Output: start at 60 mA, │
│ increase to capture │
│ • Analgesia/sedation essential │
└──────────────────┬──────────────────┘
↓
While awaiting pacing or if TCP ineffective:
┌──────────────────────────────────────────┐
│ PHARMACOLOGICAL BRIDGE │
│ • DOPAMINE 2-10 mcg/kg/min IV infusion │
│ • EPINEPHRINE 2-10 mcg/min IV infusion │
│ • ISOPROTERENOL (rare, for beta-blocker │
│ or CCB overdose) 2-10 mcg/min │
└──────────────────────────────────────────┘
↓
TRANSVENOUS PACING (TVP)
- Definitive emergency pacing
- Via right internal jugular or subclavian vein
- Float electrode to RV apex
- Confirm capture on ECG
10.2 Drug Summary Table
| Drug | Dose | Mechanism | Indication | Contraindication |
|---|
| Atropine | 0.5 mg IV q3-5 min, max 3 mg | Blocks muscarinic receptors → ↑ SA/AV automaticity | Symptomatic junctional bradycardia | Heart transplant (ineffective), 2nd degree Mobitz II, CHB (may worsen) |
| Dopamine | 2-10 mcg/kg/min IV | β1 stimulation → ↑ HR and contractility | Hemodynamically unstable, atropine failure | Tachyarrhythmias, VF |
| Epinephrine | 2-10 mcg/min IV | α + β1 stimulation | Severe hemodynamic compromise | Ventricular arrhythmias |
| Isoproterenol | 2-10 mcg/min IV | Pure β1+β2 → ↑ HR | Beta-blocker/CCB toxicity, temporary bridge | Acute MI, hypertension |
| Glucagon | 3-10 mg IV bolus | Bypasses beta receptor; ↑ cAMP | Beta-blocker or CCB overdose | - |
| Digoxin Fab fragments | Weight/level based | Binds free digoxin | Digoxin toxicity with serious arrhythmia | Allergy to ovine proteins |
10.3 Pacing Indications and Technique
Transcutaneous Pacing (TCP)
- Indication: Hemodynamically unstable symptomatic bradycardia not responding to atropine
- Technique: Anterior-posterior pad placement, rate 60-80, increase output until capture
- Limitation: Painful, not for long-term use, may fail to capture
Transvenous Pacing (TVP)
- Indication: Persistent symptomatic bradycardia, TCP failure, high-degree AV block
- Route: Right internal jugular, right subclavian, femoral
- Target: RV apex (float-through or fluoroscopy guided)
- Confirm capture: Paced spike → wide QRS in ECG, pulse corresponding to pacing
Permanent Pacemaker Indications (ACC/AHA Class I)
- Symptomatic sinus bradycardia (including junctional escape as secondary pacemaker)
- Sick sinus syndrome with symptomatic bradycardia
- Complete (3rd degree) AV block at any anatomic level
- Symptomatic Mobitz II 2nd degree AV block
- Symptomatic bradycardia not responding to other treatments
- Drug-induced bradycardia when drug cannot be stopped
SECTION 11: LONG-TERM TREATMENT
11.1 Treat Underlying Cause
| Cause | Specific Treatment |
|---|
| Digoxin toxicity | Stop digoxin; digoxin-specific Fab if severe |
| Beta-blocker toxicity | Glucagon, high-dose insulin, calcium; stop drug |
| CCB toxicity | Calcium gluconate/chloride; glucagon; high-dose insulin; stop drug |
| Inferior MI | Urgent reperfusion (PCI); AV block usually transient |
| Myocarditis | Anti-inflammatory, immunosuppression if indicated; steroids |
| Hypokalemia | IV/PO potassium replacement |
| Hyperkalemia | Calcium gluconate, insulin+dextrose, bicarb, dialysis |
| Hypothyroidism | Thyroid hormone replacement |
| Sleep apnea | CPAP/BiPAP |
| Rheumatic fever | Penicillin, aspirin/steroids |
11.2 Permanent Pacemaker Decision
SYMPTOMATIC JUNCTIONAL RHYTHM / ESCAPE RHYTHM
↓
Is the cause reversible?
YES → Treat cause, re-evaluate
NO → Is the patient symptomatic with bradycardia?
↓
YES
↓
PERMANENT PACEMAKER IMPLANTATION
• VVIR (single chamber) - sufficient for isolated junctional escape
• DDDR (dual chamber) - preferred if AV synchrony beneficial
• Consider CRT if LVEF <35% and LBBB pattern
11.3 Catheter Ablation for Junctional Tachycardia
- Reserved for drug-refractory symptomatic JT
- Target: focus near His bundle / AV node
- Risk: Complete heart block requiring pacemaker >5% (Braunwald's)
- Success rate: lower than for AVNRT (~80-85%)
- Preferred approach: careful mapping with His potential monitoring
SECTION 12: DRUG-INDUCED JUNCTIONAL RHYTHM
12.1 Detailed Drug Table
| Drug | Mechanism | ECG Pattern | Treatment |
|---|
| Digoxin | Inhibits Na/K-ATPase → ↑ intracellular Ca2+ → enhanced automaticity. Also: ↑ vagal tone → SA suppression | NPJT (70-130 bpm) over AF baseline, bidirectional VT in severe toxicity | Stop digoxin; Digoxin Fab for severe toxicity; correct K+ (hypoK worsens toxicity) |
| Beta-blockers | Block β1 receptors → suppress SA automaticity → junctional escape | Sinus bradycardia → junctional escape | Stop if severe; Glucagon 3-10 mg IV; High-dose insulin euglycemic therapy; Atropine (limited); TCP |
| Diltiazem/Verapamil | Block L-type Ca2+ channels in SA and AV node → suppress pacemaker | SA/AV block → junctional escape; may cause complete AV block | Stop drug; Calcium gluconate IV; Glucagon; Isoproterenol; TCP/TVP |
| Amiodarone | Blocks Na+, K+, Ca2+ channels; β-blocker effects → marked SA suppression | Sinus bradycardia → junctional escape; prolonged QT; also can cause JT | Reduce dose or stop; Thyroid effects may contribute |
| Ivabradine | Blocks If (funny current) in SA node → slows sinus rate | Sinus bradycardia → junctional escape | Reduce dose; If current also present in AV node so junction also slowed |
| Adenosine | Activates A1 receptors → ↑ IK-Ach → hyperpolarization of SA/AV | Transient sinus arrest → brief junctional escape (expected) | Expected, transient - typically resolves in <30 seconds |
12.2 Digoxin Toxicity - Special Emphasis
Mechanism: Digoxin inhibits Na-K-ATPase → ↑ intracellular Na+ → ↑ Ca2+ via Na-Ca exchanger → enhanced automaticity in AV junction. Simultaneously increases vagal tone → suppresses SA node.
Classic ECG pattern in digoxin toxicity:
- Atrial fibrillation with REGULAR QRS complexes (NPJT + AF = "regularized AF")
- Bidirectional ventricular tachycardia (pathognomonic)
- PAT with block (atrial tachycardia at 150-250 bpm with 2:1 AV block)
Management Algorithm:
Digoxin Toxicity + Junctional Rhythm
↓
STOP DIGOXIN
Monitor K+ (correct hypokalemia to K+ >4 mEq/L)
↓
Mild (NPJT, asymptomatic): Monitor, hold digoxin
↓
Moderate (hemodynamically unstable): Digoxin-specific Fab fragments
↓
Severe (life-threatening arrhythmia, K+ >5 in acute overdose):
Digoxin-specific Fab, AVOID cardioversion (risk of VF),
AVOID calcium (can worsen stone heart)
SECTION 13: JUNCTIONAL RHYTHM IN SPECIAL SITUATIONS
13.1 Inferior Wall MI
- AV node supplied by posterior descending artery (PDA) from RCA in 90% of people
- Inferior MI (ST elevation in II, III, aVF) → ischemia of AV node → junctional escape
- Features:
- Usually transient (hours to days)
- Narrow QRS junctional escape if below bundle of His not involved
- May progress to Mobitz I (Wenckebach) → complete AV block
- Management: PCI/reperfusion (primary treatment); atropine if hemodynamically compromised; temporary pacing rarely needed
- Prognosis: usually resolves after reperfusion; rarely needs permanent pacemaker
13.2 Digoxin Toxicity
(See Section 12.2 above for full details)
Key pearl: The combination of atrial fibrillation + regular ventricular rhythm = junctional tachycardia from digoxin toxicity until proven otherwise.
13.3 Post-Cardiac Surgery
- Common in first 24-48 hours post-cardiac surgery (especially in children)
- Mechanism: edema and trauma to His bundle during VSD repair, Tetralogy of Fallot repair, Fontan procedure
- Management:
- Avoid catecholamines if possible (worsen automaticity)
- Hypothermia (36°C): reduces automaticity
- Amiodarone IV loading dose
- Atrial pacing faster than JET rate to restore AV synchrony
- Dexmedetomidine (alpha-2 agonist) - reduces sympathetic tone
- Usually transient (resolves in 24-72 hours)
13.4 Athletes
- Sinus bradycardia (40-55 bpm) very common
- High resting vagal tone → junctional escape (benign)
- ECG: absent P waves at rest, HR 45-55 bpm, narrow QRS
- Rate increases normally with exercise (distinguishes from pathological SA node disease)
- No treatment required - this is a normal physiological variant
- Reassurance is key
13.5 Pregnancy
- Pregnancy generally causes sinus tachycardia (↑ sympathetic tone)
- Junctional rhythm in pregnancy: consider inferior MI, peripartum cardiomyopathy, drug effect
- Management: treat underlying cause; atropine safe for acute use; avoid isoproterenol (uteroplacental effects); temporary pacing if severely symptomatic
13.6 Pediatric Patients
- Congenital JET: most important; see Section 3.6
- Junctional escape common after cardiac surgery
- Normal range for pediatric HR higher than adults; junctional rhythm diagnosed relative to age-appropriate normal rates
13.7 ICU Patients
- Multiple contributing factors: sedatives, electrolytes, hypoxia, cardiac ischemia, sepsis
- Strategy:
- Correct electrolytes first (K+, Mg2+, Ca2+)
- Review all medications
- Treat underlying critical illness
- Continuous telemetry monitoring
13.8 Electrolyte Abnormalities
| Electrolyte | Disturbance | Effect on Junctional Rhythm |
|---|
| Potassium | Hypokalemia | Increases automaticity → accelerated JR / JT; potentiates digoxin toxicity |
| Potassium | Hyperkalemia | Depresses SA node → junctional escape; risk of asystole |
| Magnesium | Hypomagnesemia | Arrhythmogenesis; often co-occurs with hypokalemia |
| Calcium | Hypocalcemia | Prolonged QT; rare arrhythmias |
| Calcium | Hypercalcemia | SA acceleration usually; rarely junctional rhythm |
SECTION 14: COMPLICATIONS
| Complication | Mechanism | Clinical Consequence |
|---|
| Syncope / Near-syncope | Cerebral hypoperfusion from low CO | Fall, injury, sudden cardiac arrest |
| Heart failure | AV dyssynchrony + loss of atrial kick | Dyspnea, edema, reduced exercise tolerance |
| Hypotension | Low cardiac output, reduced preload | Organ hypoperfusion, syncope |
| AV Dyssynchrony | Loss of coordinated atrial-ventricular contraction | Reduces CO 20-30%, cannon A waves |
| Reduced Cardiac Output | Bradycardia + dyssynchrony | Worsened in structural heart disease |
| Progression to Complete Heart Block | Worsening conduction system disease | Life-threatening if no escape pacemaker |
| Pacemaker syndrome | If VVI pacing used without AV synchrony | Persistent symptoms despite pacing |
| Cardiogenic shock | Severe rapid JET in infants with CHD | Emergency; very high mortality without treatment |
SECTION 15: PROGNOSIS
15.1 Benign vs Pathological Junctional Rhythm
| Feature | Benign | Potentially Pathological |
|---|
| Rate | 40-60 bpm, adequate | <40 or >100 bpm |
| Setting | Athletes, sleep, high vagal tone | Structural heart disease, drug toxicity, ischemia |
| Symptoms | None | Syncope, HF, angina |
| Hemodynamics | Stable | Unstable |
| ECG | Junctional escape only | AV dissociation, AV block, capture beats |
| Response to exercise | Rate increases normally | May not respond |
| Structural disease | Absent | Present |
15.2 Prognostic Factors
| Good Prognosis | Poor Prognosis |
|---|
| Isolated junctional escape in athletes | Complete heart block with ventricular escape |
| Transient junctional rhythm after inferior MI reperfusion | Postoperative JET in CHD (mortality up to 5% historically) |
| Drug-induced (reversible after drug removal) | Congenital JET with refractory tachycardia |
| Asymptomatic accelerated junctional rhythm | Junctional rhythm with cardiogenic shock |
| Normal cardiac structure | Severe structural heart disease |
| Preserved LV function | Reduced EF (<35%) |
15.3 Specific Prognostic Scenarios
Inferior MI + Junctional Rhythm:
- With successful PCI: AV conduction usually recovers within 24-72 hours
- Rarely progresses to permanent complete heart block
- Prognosis determined by infarct size, not the rhythm itself
Congenital JET:
- High mortality if untreated (heart failure, hydrops in infants)
- With amiodarone ± ablation: most survive but risk of complete heart block from ablation
Postoperative JET:
- Historically 10-15% mortality; modern management (cooling, amiodarone) reduces this
- Usually transient (24-48 hours)
- Recurrence rare after healing
Digoxin-induced NPJT:
- Excellent prognosis after drug withdrawal and Fab treatment
- Recurrence prevented by avoiding digoxin
CLINICAL PEARLS SUMMARY
Pearl 1: Junctional rhythm is NARROW QRS (unless bundle branch block coexists). If you see a wide-complex escape rhythm, think ventricular escape.
Pearl 2: In AV dissociation with junctional rhythm, look for cannon A waves in JVP - they are pathognomonic of atria contracting against closed tricuspid.
Pearl 3: NEVER suppress a junctional escape rhythm without ensuring another adequate pacemaker is present. It may be the only thing keeping the patient alive.
Pearl 4: "Regularized AF" (AF with regular R-R intervals) = junctional tachycardia from digoxin toxicity until proven otherwise.
Pearl 5: Focal junctional tachycardia has GRADUAL onset (warm-up), while AVNRT starts ABRUPTLY. Adenosine terminates AVNRT but only transiently slows JT.
Pearl 6: Inferior MI affects the AV node (RCA supplies in 90%) → transient junctional escape expected. Reperfuse first; most will resolve without pacing.
Pearl 7: Atropine is ineffective in heart transplant recipients (denervated heart) and may paradoxically worsen Mobitz II or CHB.
Pearl 8: Postoperative JET treatment priorities: cooling > amiodarone > atrial pacing (faster than JET to restore AV synchrony). Emerging evidence: ivabradine (
PMID: 41845224) may reduce JET rate.
Pearl 9: In complete heart block, narrow QRS escape = junctional escape (above bifurcation, 40-60 bpm, more stable). Wide QRS escape = ventricular escape (below bifurcation, 20-40 bpm, less stable, needs urgent pacing).
Pearl 10: ECG hallmark of junctional rhythm: inverted P waves in II, III, aVF (retrograde) either before QRS (PR < 120 ms), within QRS (not visible), or after QRS (RP < 200 ms).
KEY ECG SUMMARY DIAGRAM
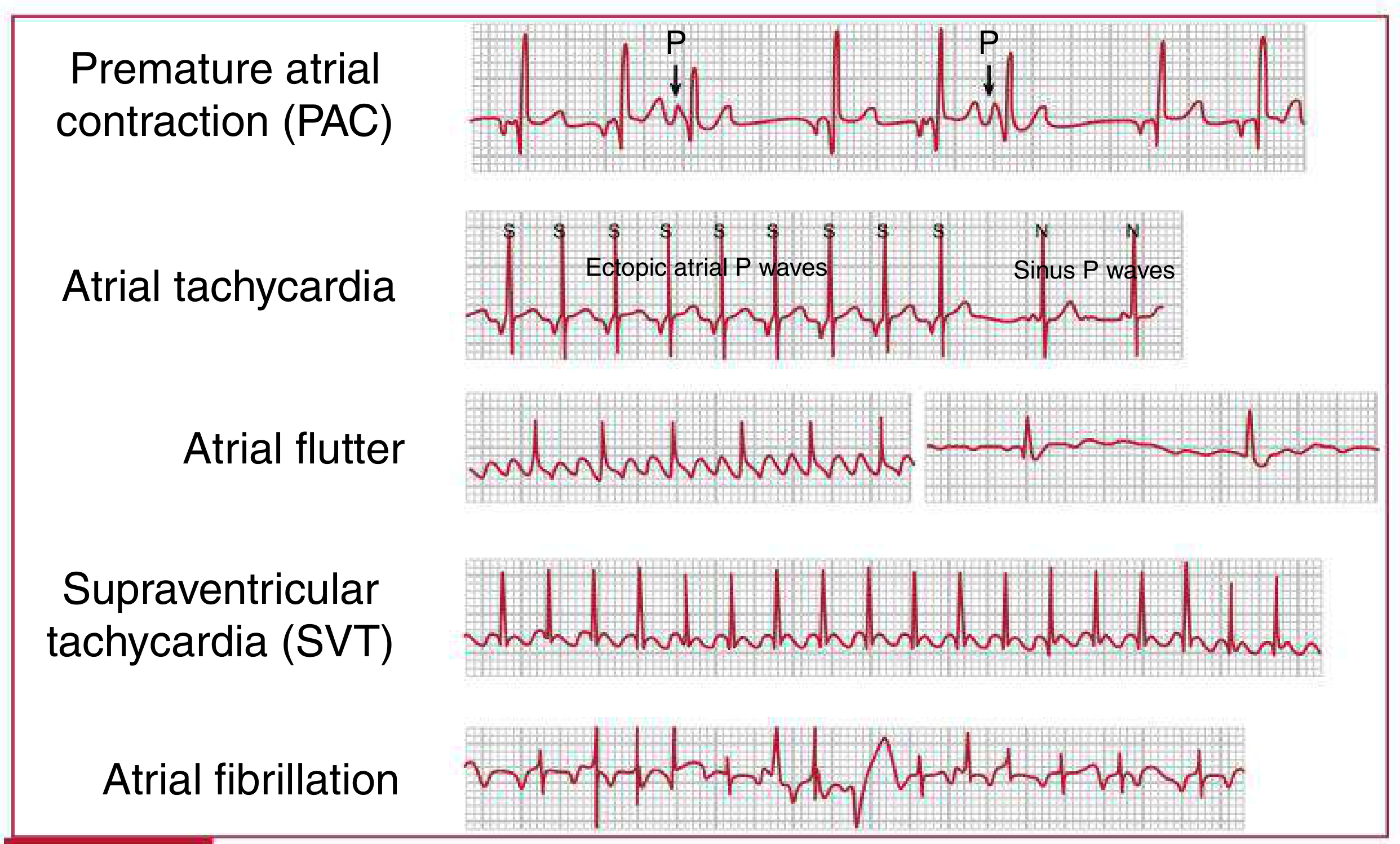
Supraventricular arrhythmia comparison panel (from Harriet Lane Handbook):
Key differential: Junctional rhythm differs from all above patterns by its characteristic inverted/absent P waves, narrow regular QRS at 40-60 bpm (escape) or 60-100 bpm (accelerated). SVT pattern resembles junctional tachycardia but starts/stops abruptly and terminates with adenosine.
REFERENCES
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th ed. - Chapter 18: Dysrhythmia Management
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 253: Supraventricular Arrhythmias
- Braunwald's Heart Disease, 2 Vol Set - Chapter on Catheter Ablation of Arrhythmias
- Goldman-Cecil Medicine International Edition - Chapter 52: Junctional Tachycardia
- Rosen's Emergency Medicine, 9th ed. - Chapter 65: Arrhythmias
- Katzung's Basic and Clinical Pharmacology, 16th Edition - Chapter on Digoxin
- Harriet Lane Handbook, 23rd ed. - Chapter 7: Arrhythmias
- Frameworks for Internal Medicine - Junctional Escape Rhythm
- Balweel H et al. Potential use of ivabradine in postoperative junctional ectopic tachycardia: a systematic review and meta-analysis. BMC Cardiovasc Disord. 2026 (PMID: 41845224)
- Carmona-Puerta R et al. Junctional ectopic tachycardia revisited. Postgrad Med. 2025 (PMID: 40143746)