opioid Phramacology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"opioid" AND "pharmacology"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from four authoritative textbooks. Let me compile the full, detailed response.
Opioid Pharmacology
1. Terminology and Classification
The term opioid refers broadly to any agent that binds to the orthosteric (ligand-binding) site of opioid receptors - this includes natural plant-derived compounds, semisynthetic derivatives, fully synthetic drugs, and endogenous peptides. The narrower term opiate specifically refers to morphine, codeine, and structurally related compounds derived from opium (the dried resin of Papaver somniferum), along with semisynthetic derivatives like oxycodone.
Opium contains: morphine (~10%), codeine (~0.5%), thebaine (a precursor with no opioid activity), papaverine (1%, smooth muscle relaxant), and noscapine (6%, antitussive).
Origin-Based Classification
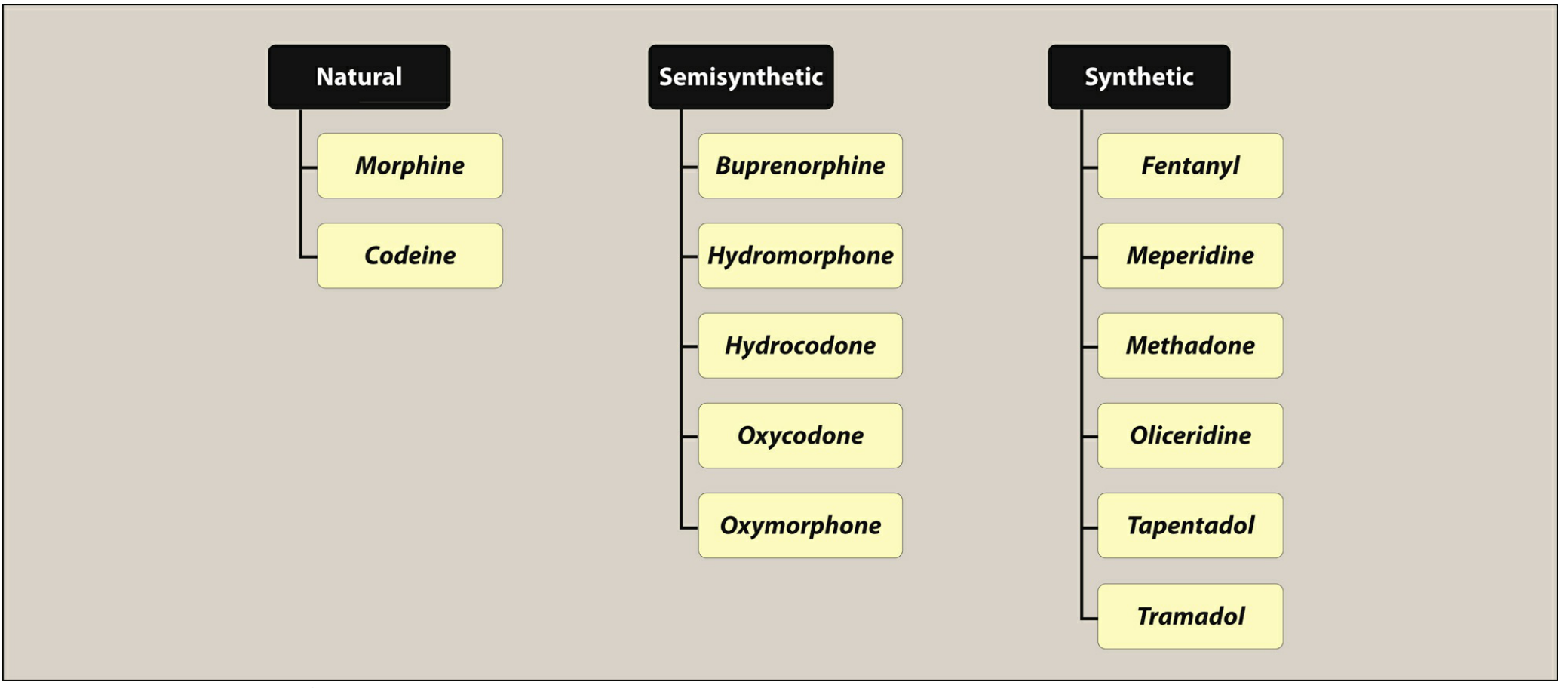
| Category | Examples |
|---|---|
| Natural | Morphine, Codeine |
| Semisynthetic | Buprenorphine, Hydromorphone, Hydrocodone, Oxycodone, Oxymorphone |
| Synthetic | Fentanyl, Meperidine, Methadone, Tramadol, Tapentadol, Remifentanil |
Receptor Activity Classification
| Class | Examples |
|---|---|
| Full agonists | Morphine, codeine, fentanyl, methadone, oxycodone, meperidine |
| Partial agonist | Buprenorphine (μ partial agonist, κ/δ antagonist) |
| Mixed agonist-antagonist | Pentazocine, nalbuphine, butorphanol |
| Pure antagonists | Naloxone, naltrexone, nalmefene |
- Lippincott Illustrated Reviews: Pharmacology, p. 700-702
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 463
2. Opioid Receptors
There are four receptor families, all belonging to the Class A (rhodopsin-type) G protein-coupled receptors (GPCRs), sharing 48-58% sequence homology:
| Receptor | Symbol | Key Endogenous Ligands | Primary Actions |
|---|---|---|---|
| Mu | μ (MOP) | β-Endorphin, endomorphins | Analgesia, euphoria, respiratory depression, constipation, miosis, physical dependence |
| Kappa | κ (KOP) | Dynorphins | Analgesia, sedation, dysphoria, diuresis, miosis, minimal respiratory depression |
| Delta | δ (DOP) | Enkephalins | Analgesia, mood modulation, less respiratory depression |
| Nociceptin/ORL1 | NOP (NOPr) | Nociceptin/Orphanin FQ | Pain modulation, anxiety, stress, memory, feeding; NOT activated by classical opioids |
Key point: The mu receptor is the primary target mediating both the analgesic benefits AND the unwanted effects (respiratory depression, addiction) of all clinically used opioids.
Receptor Distribution
- μ receptors: Neocortex, caudate-putamen, nucleus accumbens, ventral tegmental area (VTA), thalamus, hippocampus, amygdala, raphe nucleus, periaqueductal gray (PAG), medulla/pons, spinal cord dorsal horn
- κ receptors: Caudate-putamen, nucleus accumbens, amygdala, hypothalamus, pituitary, PAG, dorsal horn
- δ receptors: Olfactory areas, neocortex, caudate-putamen, nucleus accumbens, amygdala (low levels in spinal cord)
- NOPr: Most widely distributed - found throughout brain and spinal cord
Opioid receptors also reside on non-neuronal cells: macrophages, microglia, astrocytes, and enteric neurons of the GI tract.
- Goodman & Gilman's, p. 463-464
3. Receptor Signaling Mechanism
All opioid receptors signal through Gi/o heterotrimeric G proteins. Agonist binding activates the receptor, and both the α subunit and βγ dimer drive downstream effects:
α subunit effects:
- Directly inhibits adenylyl cyclase (AC) → ↓ cAMP → ↓ PKA activity → reduced phosphorylation of downstream targets
- Reduced cAMP-dependent Ca²⁺ influx
βγ dimer effects:
- Inhibits voltage-gated Ca²⁺ channels on presynaptic terminals → ↓ Ca²⁺ influx → ↓ neurotransmitter release (e.g., inhibits GABA release in the PAG, activating descending antinociceptive pathways; enhances dopamine release in nucleus accumbens via disinhibition - the reward pathway)
- Opens GIRK (G protein-coupled inwardly rectifying K⁺) channels → K⁺ efflux → membrane hyperpolarization → reduced neuronal firing
- Activates MAPK (mitogen-activated protein kinase) pathways
Net result: Decreased neuronal excitability, reduced neurotransmitter release, and analgesia.
Chronic agonist exposure leads to AC supersensitivity - when the opioid is removed, there is a rebound "overshoot" of cAMP production, contributing to withdrawal.
- Goodman & Gilman's, p. 464-465
4. Sites of Analgesic Action
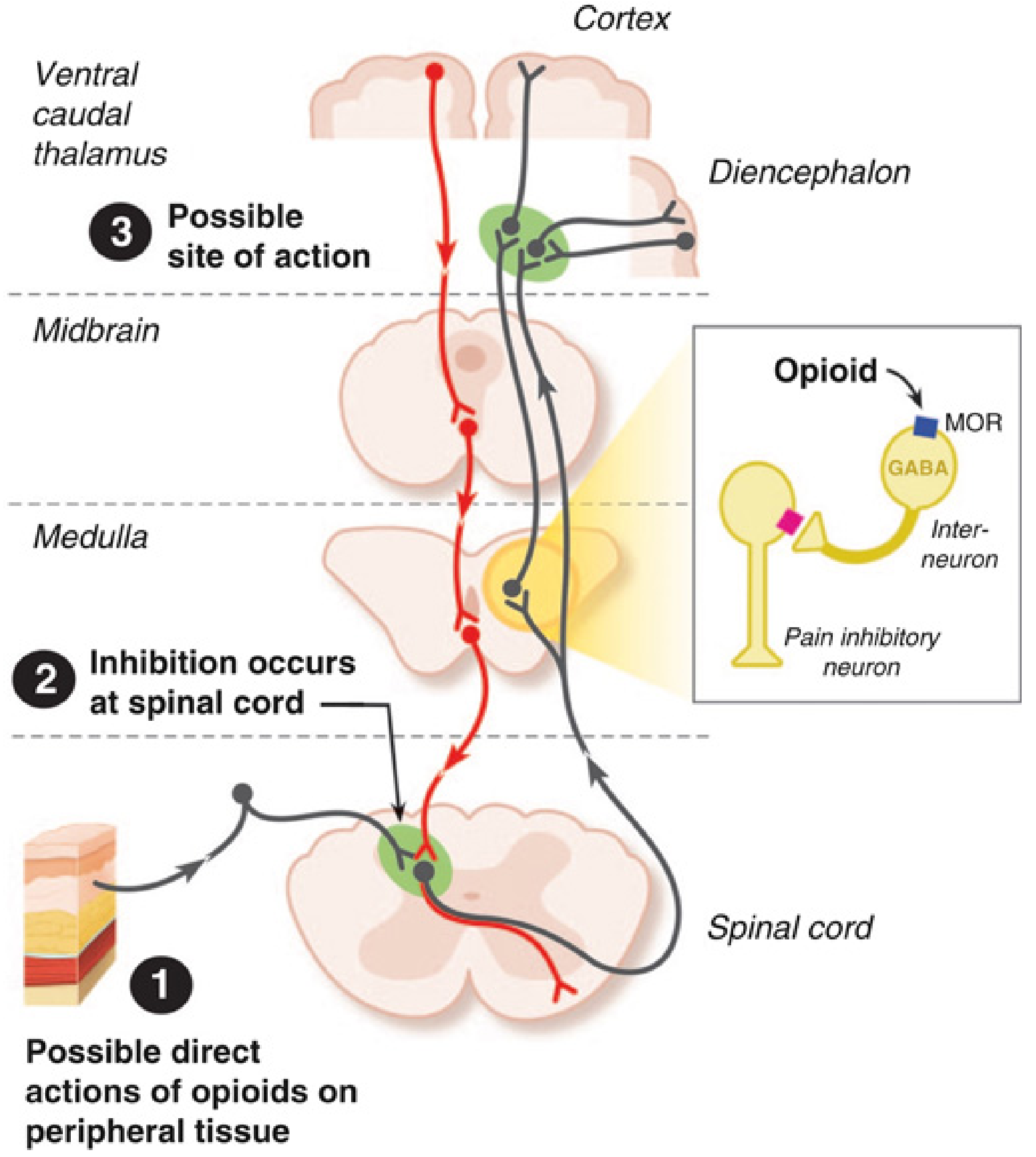
Opioids produce analgesia at three levels:
(1) Peripheral
- Dorsal root ganglion neurons express μ, κ, and δ receptors
- Inflammatory mediators upregulate peripheral opioid receptors
- Clinically relevant for intra-articular and local opioid administration
(2) Spinal Cord
- Opioid receptors are abundantly expressed in the substantia gelatinosa of the dorsal horn
- Opioids inhibit the release of glutamate and substance P from primary afferent terminals (presynaptic)
- Act both pre- and postsynaptically
- Systemic morphine also activates descending inhibitory pathways to increase serotonin and norepinephrine release in the dorsal horn
(3) Supraspinal (Brain)
-
Periaqueductal gray (PAG): Opioids disinhibit descending pain-modulating neurons by inhibiting GABAergic interneurons
-
Rostral ventromedial medulla (RVM): Relay of descending inhibition
-
Limbic structures (amygdala, anterior cingulate): Modulate the affective/emotional component of pain
-
Thalamus and cortex: Alter pain perception and consciousness
-
Miller's Anesthesia, 10th Edition, p. 2702-2703
5. Endogenous Opioid Peptides
Three main families of endogenous opioids, all derived from precursor proteins:
| Peptide Family | Precursor | Receptor Preference |
|---|---|---|
| Enkephalins (met- and leu-) | Proenkephalin | δ > μ |
| Endorphins (β-endorphin) | Proopiomelanocortin (POMC) | μ > δ |
| Dynorphins | Prodynorphin | κ >> μ, δ |
6. Pharmacological Effects of Opioids (Prototype: Morphine)
CNS Effects
- Analgesia: Selective relief of pain without loss of consciousness; patients report pain is still present but they feel "more comfortable" - this reflects modulation of the affective component of pain
- Euphoria/Dysphoria: μ agonists cause euphoria; κ agonists cause dysphoria
- Sedation and drowsiness: Mental clouding
- Respiratory depression: Most dangerous effect - depression of brainstem respiratory centers, reducing sensitivity to CO₂. Tolerance develops with repeated use
- Antitussive effect: Suppression of cough reflex (medulla)
- Miosis (pinpoint pupils): Stimulation of Edinger-Westphal nucleus; NO tolerance develops - a useful sign in overdose
- Truncal rigidity ("wooden chest"): Seen with high-dose fentanyl and rapid IV administration
GI Effects
- Constipation: ↑ circular smooth muscle tone, ↓ intestinal propulsion, ↑ anal sphincter tone - minimal tolerance develops to this effect
- Nausea and vomiting: Direct stimulation of the chemoreceptor trigger zone (CTZ) in the area postrema
- ↑ Biliary pressure: Contraction of gallbladder, constriction of biliary sphincter (Oddi's sphincter)
Cardiovascular Effects
- Minimal at therapeutic doses; at higher doses: hypotension and bradycardia
- CO₂ retention → cerebral vasodilation → ↑ ICP - contraindicated in head trauma
Urinary
- Inhibits voiding reflex, increases sphincter tone → urinary retention (common postoperatively)
Histamine Release (Morphine-specific)
- Triggers mast cell degranulation → urticaria, sweating, bronchoconstriction, vasodilation
- Use with caution in asthma; fentanyl is preferred (minimal histamine release)
Hormonal
- Prolonged use → opioid-induced androgen deficiency (OPIAD) via suppression of the hypothalamic-pituitary-gonadal (HPG) axis → ↓ testosterone → fatigue, decreased libido, mood changes, sexual dysfunction
Labor
-
Morphine may prolong the second stage of labor (transiently decreases uterine contraction strength and frequency)
-
Lippincott Illustrated Reviews: Pharmacology, pp. 712-714; Miller's Anesthesia, p. 2714
7. Pharmacokinetics of Morphine (Prototype)
| Parameter | Detail |
|---|---|
| Absorption | Oral absorption is slow and erratic; significant first-pass hepatic metabolism; IV and SC are most reliable |
| Distribution | Enters all tissues including fetus; least lipophilic of common opioids - only a small fraction crosses the BBB |
| Metabolism | Hepatic glucuronidation → morphine-6-glucuronide (M6G) (potent analgesic, active) + morphine-3-glucuronide (M3G, no analgesia, may cause neuroexcitatory effects) |
| Elimination | Renal; accumulates in renal failure |
| Half-life | ~2-3 hours; extended-release forms (MS Contin) for chronic dosing |
Fentanyl and methadone are highly lipophilic and readily penetrate the CNS; they are the preferred agents when rapid CNS action is needed or in patients with poor oral bioavailability.
8. Individual Opioid Drug Profiles
Full Agonists
| Drug | Key Features |
|---|---|
| Morphine | Prototype; oral/IV/epidural; M6G active metabolite; histamine release; least lipophilic |
| Codeine | Prodrug - converted to morphine by CYP2D6; also antitussive; weak analgesic (10% potency of morphine) |
| Oxycodone | Oral; ~1.5x potency of oral morphine; OxyContin (extended release) - associated with opioid crisis |
| Hydromorphone | 5-10x potency of morphine; good oral bioavailability |
| Fentanyl | 100x potency of morphine; highly lipophilic; rapid onset; transdermal, IV, buccal, intranasal; minimal histamine release; preferred in asthma and hemodynamically unstable patients |
| Remifentanil | Ultra-short acting; metabolized by non-specific plasma esterases (not CYP); useful in anesthesia |
| Methadone | Long t½ (24-36 h); NMDA receptor antagonist (additional mechanism); oral; used for chronic pain and OUD maintenance; QT prolongation risk |
| Meperidine | κ agonist with some μ activity; active metabolite normeperidine (neurotoxic, accumulates in renal failure - seizures, myoclonus); anticholinergic effects; no miosis; serotonin syndrome with SSRIs/MAOIs; short-term use only (≤48 h) |
| Tramadol | Weak μ agonist + SNRI (serotonin and norepinephrine reuptake inhibitor); ceiling effect; serotonin syndrome risk |
| Tapentadol | μ agonist + norepinephrine reuptake inhibitor; fewer GI side effects than morphine |
Partial Agonists / Mixed Agonist-Antagonists
Buprenorphine:
- Partial μ agonist + κ/δ antagonist + ORL-1 agonist
- Very high receptor affinity (25-100x potency of morphine)
- Ceiling effect on respiratory depression (lower abuse potential)
- Can precipitate withdrawal in opioid-dependent patients (high affinity displaces full agonists)
- Formulations: Suboxone (buprenorphine + naloxone), transdermal patches, subdermal implant
- Approved for office-based OUD treatment (unlike methadone)
- Shorter, less severe withdrawal than methadone; but methadone has higher patient retention rates
Pentazocine, Nalbuphine, Butorphanol:
-
Mixed agonist-antagonists; κ agonist / μ antagonist or partial μ agonist
-
Can precipitate withdrawal in opioid-dependent patients
-
Dysphoria, hallucinations (κ effects)
-
Lippincott Illustrated Reviews: Pharmacology, pp. 720-723; Katzung's Basic and Clinical Pharmacology, p. 884
9. Opioid Antagonists
| Drug | Key Points |
|---|---|
| Naloxone | Short-acting (30-90 min); IV/IM/intranasal; reverses opioid overdose; given with buprenorphine in Suboxone to deter IV misuse (poor oral bioavailability means it doesn't antagonize SL buprenorphine) |
| Naltrexone | Longer acting; oral; used for OUD and alcohol use disorder; hepatotoxicity at high doses |
| Nalmefene | Similar to naltrexone; longer half-life |
Antagonists bind the receptor but have zero intrinsic activity - they compete with agonists for binding. In opioid-dependent patients, they precipitate acute withdrawal.
10. Tolerance and Dependence
Tolerance: Reduced response to the same dose with repeated exposure. Mechanisms include:
- Receptor desensitization (uncoupling from G protein)
- Receptor internalization/downregulation
- AC supersensitivity (upregulation of cAMP pathway)
- Neuroadaptive changes in downstream circuits
Tolerance develops to: analgesia, euphoria, sedation, respiratory depression, emesis
No tolerance develops to: Miosis, constipation
Physical Dependence: Physiological adaptation requiring continued drug to prevent withdrawal. Withdrawal is characterized by:
- Anxiety, agitation, insomnia, yawning
- Piloerection ("gooseflesh"), diaphoresis, lacrimation, rhinorrhea
- Tachycardia, hypertension, hyperthermia
- Nausea, vomiting, diarrhea
- Myalgias, abdominal cramps
Mechanism: rebound cAMP overshoot when opioid removed → noradrenergic hyperactivation (explains why clonidine, an α₂ agonist, reduces withdrawal symptoms by suppressing norepinephrine release).
11. Opioid Overdose Toxidrome
Classic triad:
- Coma / unconsciousness
- Respiratory depression (slow, shallow breathing; apnea)
- Miosis (pinpoint pupils)
Management: Naloxone (0.4-2 mg IV/IM/IN; repeat every 2-3 minutes as needed; may need infusion for long-acting opioids like methadone)
12. Special Considerations
- Renal failure: Avoid morphine (M6G accumulates), meperidine (normeperidine accumulates - seizures); prefer hydromorphone, fentanyl
- Asthma: Avoid morphine/codeine (histamine release); prefer fentanyl
- Head injury: Avoid (CO₂ retention → ↑ ICP)
- Pregnancy: Neonatal opioid withdrawal syndrome (NOWS) with chronic exposure; buprenorphine or methadone for OUD in pregnancy
- Elderly: Avoid meperidine (delirium risk); reduce doses of all opioids
- MAOIs: Meperidine + MAOIs = potentially fatal serotonin syndrome or opioid toxicity; tramadol + MAOIs also dangerous
Sources:
- Goodman & Gilman's The Pharmacological Basis of Therapeutics - Chapter 23 (Opioid Analgesics)
- Lippincott Illustrated Reviews: Pharmacology - Chapter 21 (Opioid Analgesics)
- Katzung's Basic and Clinical Pharmacology, 16th Edition - Chapter 31
- Miller's Anesthesia, 10th Edition - Chapter 22
This is a shared conversation. Sign in to Orris to start your own chat.