Hypokalemia and hyponatremia in detail with proper understanding with photos medicine mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Searching the Web
hypokalemia hyponatremia ECG changes clinical features MBBS medicine
Loading Image
Loading Image
I now have all the information needed to compose a thorough, well-illustrated MBBS-level guide on both conditions. Let me write the comprehensive answer.
Hypokalemia and Hyponatremia - Complete MBBS Guide
PART 1: HYPOKALEMIA
Definition & Normal Values
Potassium (K+) normal range: 3.5 - 5.0 mEq/L (mmol/L)
| Grade | Serum K+ |
|---|---|
| Mild hypokalemia | 3.0 - 3.5 mEq/L |
| Moderate hypokalemia | 2.5 - 3.0 mEq/L |
| Severe hypokalemia | < 2.5 mEq/L |
Key fact: ~98% of total body potassium is intracellular. The ratio of intracellular to extracellular K+ (approximately 140:4 mEq/L) determines the resting membrane potential of excitable cells. Even small changes in serum K+ have large effects on this ratio.
Pathophysiology of K+ Homeostasis
K+ balance involves two processes:
- Internal balance - distribution between ICF and ECF (regulated by insulin, catecholamines, acid-base status)
- External balance - intake vs. renal excretion (regulated by aldosterone, distal tubular flow, AVP)
The kidney is the primary regulator - the distal convoluted tubule and cortical collecting duct (principal cells) secrete K+ via ROMK channels (basal secretion) and BK channels (flow-dependent secretion), both regulated by aldosterone.
Causes of Hypokalemia
1. Transcellular Shift (Redistribution) - K+ moves INTO cells
| Cause | Mechanism |
|---|---|
| Insulin (exogenous/endogenous) | Stimulates Na+/K+-ATPase |
| Beta-2 agonists (salbutamol, terbutaline) | cAMP-dependent Na+/K+-ATPase activation |
| Alkalosis (metabolic/respiratory) | K+ moves into cells in exchange for H+ |
| Theophylline/caffeine overdose | cAMP activation |
| Hypokalemic periodic paralysis | Abnormal gating pore current (Ca/Na channel mutations) |
| Thyrotoxic periodic paralysis | Direct + indirect Na+/K+-ATPase activation |
MBBS pearl: In thyrotoxic periodic paralysis, high-dose propranolol (3 mg/kg) rapidly reverses hypokalemia by blocking the adrenergic drive to Na+/K+-ATPase - Harrison's Principles of Internal Medicine 22E
2. Renal Losses (Urine K+ > 20 mEq/L or TTKG > 4)
A. With Metabolic Alkalosis + Hypertension:
- Primary hyperaldosteronism (Conn's syndrome)
- Secondary hyperaldosteronism (RAS, CHF, cirrhosis)
- Cushing's syndrome (cortisol has mineralocorticoid activity)
- Liddle syndrome (gain-of-function ENaC mutation)
- 11β-HSD deficiency (apparent mineralocorticoid excess)
B. With Metabolic Alkalosis, NO Hypertension:
- Diuretics (thiazides, loop diuretics) - most common cause
- Vomiting/NG suction (alkalosis → bicarbonaturia → urinary K+ loss)
- Bartter syndrome (loop diuretic-like defects)
- Gitelman syndrome (thiazide-like defect - NCC mutation)
C. With Metabolic Acidosis:
- Renal tubular acidosis type 1 and 2
- Diabetic ketoacidosis (total body K+ depleted despite possibly normal serum K+)
- Amphotericin B toxicity
3. Extrarenal (GI) Losses (Urine K+ < 20 mEq/L)
- Diarrhea (large intestinal secretions rich in K+)
- Laxative abuse
- Malnutrition / poor dietary intake (rare alone)
- Excessive sweating (K+ in sweat is ~5-10 mEq/L)
- Fistulae, ileostomy
Clinical Features
Neuromuscular
- Weakness (especially proximal muscles, lower limbs)
- Fatigue, cramps, myalgia
- Hypo/areflexia
- Ascending paralysis (severe)
- Rhabdomyolysis (K+ < 2.5 mEq/L)
Cardiac (most dangerous)
- Palpitations, arrhythmias
- Increased risk of digitalis toxicity
- Ventricular tachycardia/fibrillation in severe cases
Renal
- Polyuria, polydipsia (hypokalemic nephropathy - impairs urinary concentrating ability)
- Metabolic alkalosis (K+ depletion promotes H+ secretion and HCO3- reabsorption)
GI
- Constipation, ileus (smooth muscle hypo-excitability)
- Nausea
ECG Changes in Hypokalemia
The ECG is a window into K+-related cardiac toxicity. Changes occur due to delayed ventricular repolarization.
Progressive ECG changes with falling K+:


| ECG Finding | Significance |
|---|---|
| Flattening/inversion of T wave | First sign; delayed repolarization |
| Prominent U wave (>1 mm, taller than T wave) | Most characteristic - represents delayed M-cell repolarization |
| ST depression | Ischemia-like pattern |
| Prolonged QU interval | (Often misread as QT prolongation) |
| Increased P-wave amplitude + PR prolongation | With more severe hypokalemia |
| Arrhythmias | PACs, PVCs, atrial/ventricular tachycardia |
Mnemonic: "No pot, no T" - flattening of T wave is the hallmark of hypokalemia Barash Clinical Anesthesia 9e - "ECG manifestations include flattened T waves, prominent U waves, ST depression, prolonged QU interval - a prodysrhythmic state"
Mechanisms of Diuretic-Induced Hypokalemia
This flowchart from Brenner and Rector's The Kidney shows the 4 mechanisms:
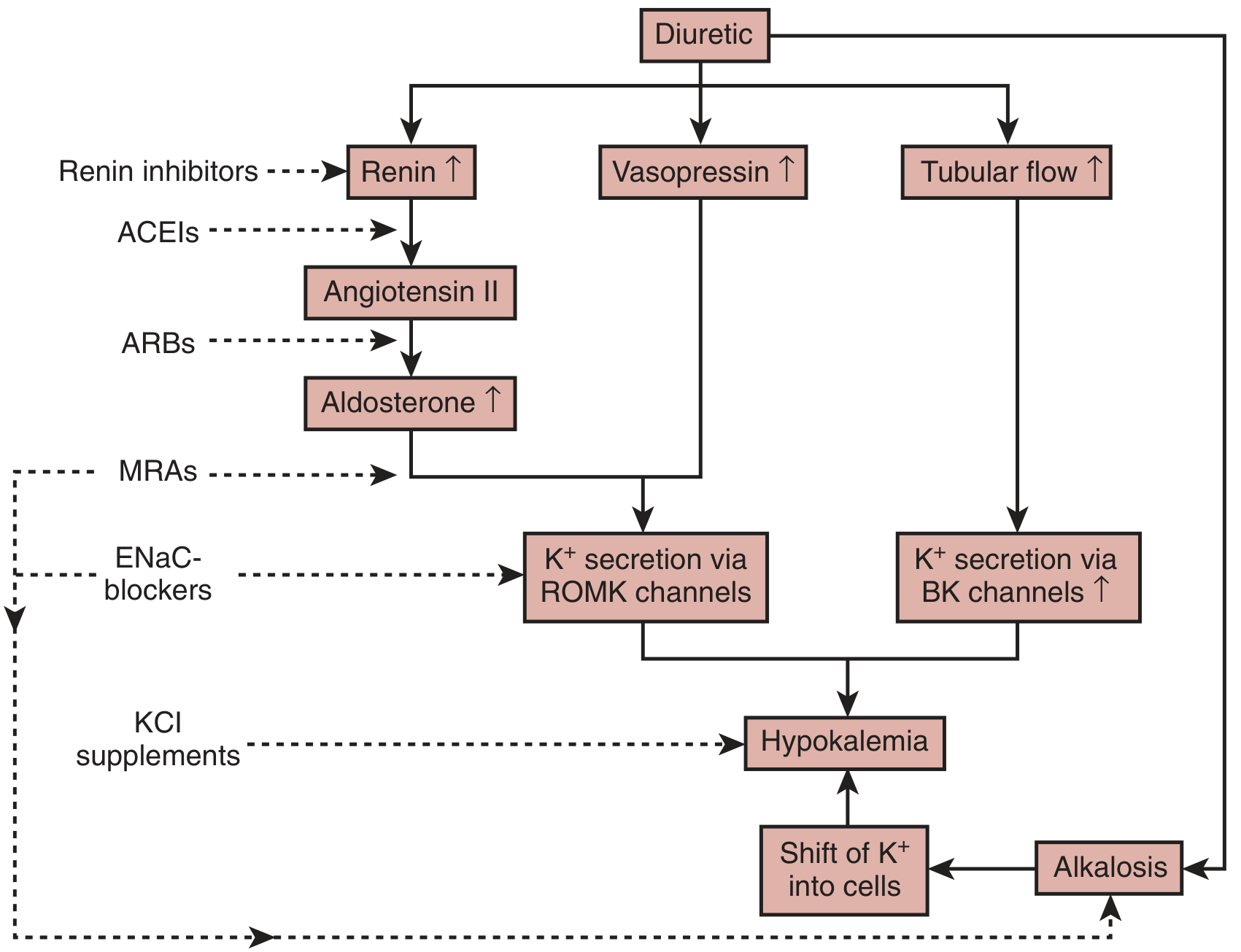
Four mechanisms operate simultaneously:
- Increased distal tubular flow - BK channel-mediated K+ secretion
- AVP stimulation (nonosmotic) - ROMK-mediated secretion
- Aldosterone secretion (RAAS activation) - ENaC/ROMK activation
- Metabolic alkalosis - K+ shift into cells + increased distal K+ secretion
Investigation of Hypokalemia
Step 1 - Rule out pseudohypokalemia (leukemia with very high WBC count consumes K+ in vitro)
Step 2 - Assess acid-base status (metabolic alkalosis vs acidosis guides etiology)
Step 3 - Measure urine K+:
- Urine K+ < 20 mEq/L or TTKG < 3: Extrarenal loss or poor intake
- Urine K+ > 20 mEq/L or TTKG > 4: Renal wasting
Step 4 - Measure blood pressure + urine electrolytes:
- Hypertension + high urine K+ → hyperaldosteronism, Cushing's, Liddle syndrome
- Normotension + metabolic alkalosis + low urine Cl- → vomiting/bulimia
- Normotension + metabolic alkalosis + high urine Cl- → diuretics, Bartter/Gitelman
Useful ratios:
- TTKG (transtubular K+ gradient) < 3 = appropriate renal conservation
- Urine K+/creatinine > 13 mmol/g = inappropriate renal wasting
- Plasma aldosterone:PRA ratio > 50 → primary hyperaldosteronism
Treatment of Hypokalemia
(Harrison's Principles of Internal Medicine 22E)
General Principles
- Determine urgency based on: severity, cardiac disease, digoxin use, rate of fall
- Patients with prolonged QT or arrhythmia require continuous cardiac monitoring
- Always correct hypomagnesemia first - hypomagnesemic patients are refractory to K+ replacement because Mg2+ is needed for Na+/K+-ATPase function
Oral Replacement (Preferred)
- KCl is the first choice - corrects both K+ and Cl- deficit (important in metabolic alkalosis)
- Potassium bicarbonate/citrate for those with concomitant metabolic acidosis
- Potassium phosphate if hypophosphatemia coexists
IV Replacement (When oral not feasible, severe hypokalemia, arrhythmias)
- Standard rate: 10-20 mEq/hr via peripheral vein
- Maximum rate: 40 mEq/hr (only with continuous cardiac monitoring, central line)
- Concentration: ≤ 40 mEq/L via peripheral IV (higher concentrations are painful and sclerotic)
- Do NOT use dextrose solutions (glucose stimulates insulin → drives K+ into cells, worsening hypokalemia)
Special Situations
- Redistributive hypokalemia (TPP, theophylline): High-dose propranolol (3 mg/kg) - corrects without rebound hyperkalemia risk
- DKA: K+ replacement essential even if initial K+ is normal or high, as insulin therapy will drop it
Preventing Recurrence
- K+-sparing diuretics: spironolactone, eplerenone (block aldosterone), amiloride/triamterene (block ENaC)
- ACEi/ARBs reduce RAAS-driven kaliuresis
- Increase dietary K+ intake (fruits, vegetables, nuts)
PART 2: HYPONATREMIA
Definition & Epidemiology
Sodium (Na+) normal range: 136 - 145 mEq/L
| Grade | Serum Na+ | Clinical Features |
|---|---|---|
| Mild | 130-135 mEq/L | Often asymptomatic |
| Moderate | 125-130 mEq/L | Nausea, malaise, weakness |
| Severe | < 125 mEq/L | Confusion, seizures, coma |
| Critical | < 105 mEq/L | Herniation, death |
Hyponatremia is the most common electrolyte disorder - occurs in 15-30% of hospitalized patients. (Tietz Textbook of Laboratory Medicine 7e)
Pathophysiology
Na+ concentration reflects the ratio of exchangeable Na+ + K+ to total body water (TBW):
Plasma [Na+] = (Exchangeable Na+ + Exchangeable K+) / TBW
This has a key implication: replacing K+ will raise plasma Na+ - and aggressive K+ repletion can overcorrect hyponatremia even without hypertonic saline.
Hyponatremia almost always results from:
- Excess circulating AVP (arginine vasopressin/ADH) - retains free water
- Increased renal sensitivity to AVP
- Combined with free water intake
- Exception: low solute intake (beer potomania)
AVP is stimulated by:
- Osmotic: plasma hyperosmolality (normal)
- Nonosmotic: hypovolemia, pain, nausea, drugs, CNS disease (pathological)
Classification and Causes
The clinical approach begins by measuring plasma osmolality, then volume status.
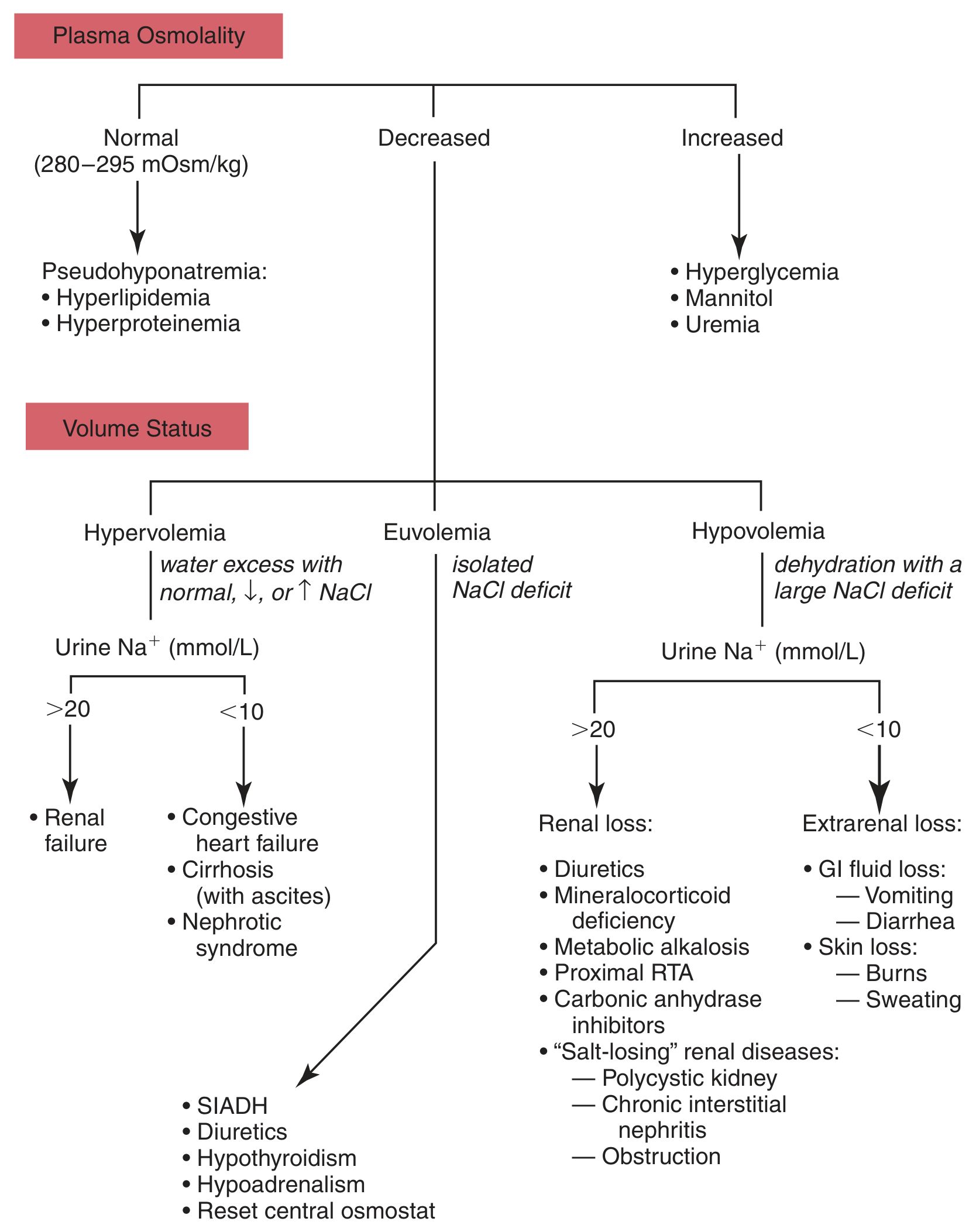
Step 1 - By Plasma Osmolality
| Osmolality | Type | Causes |
|---|---|---|
| Normal (280-295 mOsm/kg) | Pseudohyponatremia | Hyperlipidemia, hyperproteinemia (lab artifact with flame photometry) |
| High (> 295 mOsm/kg) | Hyperosmolar hyponatremia | Hyperglycemia (most common), mannitol, uremia |
| Low (< 280 mOsm/kg) | True / Hypoosmolar hyponatremia | Most clinically important - subdivide by volume status |
Correction for hyperglycemia: For every 100 mg/dL rise in glucose above normal, Na+ falls by ~1.6-2.4 mEq/L (dilutional effect of osmotic water shift).
Step 2 - Hypoosmolar Hyponatremia by Volume Status
A. HYPOVOLEMIC HYPONATREMIA (Total body Na+ decreased)
Mechanism: Volume depletion → nonosmotic AVP release → water retention
| Urine Na+ < 20 mEq/L (Extrarenal loss) | Urine Na+ > 20 mEq/L (Renal loss) |
|---|---|
| Vomiting, diarrhea | Diuretics (thiazides > loop) |
| Burns, sweating | Mineralocorticoid deficiency (Addison's) |
| Third spacing | Salt-losing nephropathy |
| Cerebral salt wasting | |
| Proximal RTA, carbonic anhydrase inhibitors |
Thiazide-specific mechanism: Unlike loop diuretics, thiazides inhibit urinary dilution but not concentration. This makes them 12 times more likely to cause hyponatremia. 80% of cases occur in older females with low body mass. Develops within the first 2 weeks. Mechanism involves a prostaglandin transporter variant (SLCO2A1) that causes AVP-independent free water reabsorption. - Brenner and Rector's The Kidney
B. EUVOLEMIC HYPONATREMIA (Total body Na+ normal, excess water)
Most common form in clinical practice. Urine Na+ is usually > 20 mEq/L.
| Cause | Key Feature |
|---|---|
| SIADH (most common) | Urine osmolality inappropriately high (> 100 mOsm/kg), Urine Na+ > 40 mEq/L |
| Hypothyroidism | Decreased cardiac output → nonosmotic AVP |
| Secondary adrenal insufficiency | Loss of cortisol's normal inhibition of AVP |
| Psychogenic polydipsia | Urine is maximally dilute (Uosm < 100); large volume intake overwhelms excretion |
| Beer potomania | Very low solute intake limits free water excretion; very high risk of ODS |
| Exercise-associated | Nonosmotic AVP + excessive hypotonic fluid intake |
| MDMA ("Ecstasy") | Potent stimulation of both thirst AND AVP |
C. HYPERVOLEMIC HYPONATREMIA (Total body Na+ increased, but water even more increased)
| Urine Na+ < 20 mEq/L | Urine Na+ > 20 mEq/L |
|---|---|
| Congestive heart failure | Acute/chronic kidney disease |
| Liver cirrhosis (with ascites) | |
| Nephrotic syndrome |
Mechanism: Effective arterial blood volume is reduced despite total body Na+ excess → nonosmotic AVP activation → water retention
Causes of SIADH
SIADH is the single most important cause of euvolemic hyponatremia. Diagnosed by exclusion.
Diagnostic criteria for SIADH:
- Hypo-osmolality (plasma Osm < 280 mOsm/kg)
- Inappropriately concentrated urine (Uosm > 100 mOsm/kg)
- Urine Na+ > 40 mEq/L (with normal salt and water intake)
- Clinical euvolemia
- Normal renal, thyroid, and adrenal function
- No recent diuretic use
Causes:
| Category | Examples |
|---|---|
| CNS | Meningitis, encephalitis, stroke, subarachnoid hemorrhage, head injury |
| Pulmonary | Pneumonia, TB, lung abscess, mechanical ventilation |
| Malignancy | Small cell lung cancer (ectopic ADH), pancreatic cancer, lymphoma |
| Drugs | SSRIs, SNRIs, carbamazepine, cyclophosphamide, NSAIDs, chlorpropamide, opioids |
| Surgery | Postoperative (pain, nausea → nonosmotic AVP) |
| Hypothyroidism | |
| HIV/AIDS |
Clinical Features of Hyponatremia
Symptoms are caused by cerebral edema - osmotic water movement into brain cells as plasma osmolality falls.
The rate of fall is more important than the absolute value for symptom severity.
Acute Hyponatremia (< 48 hours)
- Headache, nausea, vomiting
- Confusion, lethargy
- Seizures, obtundation
- Cerebral herniation (life-threatening)
- Women (especially premenopausal) and children are more vulnerable - estrogen impairs brain cell adaptation
Chronic Hyponatremia (> 48 hours)
Brain adapts by extruding organic osmolytes (creatine, betaine, glutamate, myoinositol, taurine) - reduces intracellular osmolality, limiting cerebral edema
- "Asymptomatic" but subtle: gait instability, cognitive deficits, attention problems
- Increased risk of falls and fractures
- Decreased bone density
- Nausea, confusion at Na+ < 125 mEq/L
- Seizures at Na+ < 105-110 mEq/L
Investigation of Hyponatremia
Step-wise approach:
- Plasma Na+ - confirm hyponatremia (< 135 mEq/L)
- Plasma osmolality - rule out pseudohyponatremia and hyperosmolar causes
- Volume status - clinical exam (BP, skin turgor, JVP, edema)
- Urine osmolality:
- Uosm < 100 mOsm/kg = maximally dilute = appropriate response (psychogenic polydipsia, beer potomania)
- Uosm > 100 mOsm/kg = inappropriately concentrated = AVP excess
- Urine Na+:
- < 20 mEq/L = extrarenal loss or hypervolemic state (Na+ avid kidneys)
-
40 mEq/L = SIADH, diuretics, renal failure, adrenal insufficiency
- Serum K+, glucose, creatinine, TSH, cortisol
- Urine-to-plasma electrolyte ratio: (UNa + UK) / PNa
- Ratio > 1 = every liter of urine excreted retains free water → need aggressive fluid restriction
Treatment of Hyponatremia
(Harrison's Principles of Internal Medicine 22E)
The three guiding principles:
1. Treat the underlying cause first
- SIADH from drugs → stop the drug
- Hypothyroidism → thyroxine replacement
- Adrenal insufficiency → hydrocortisone
- Volume depletion → isotonic saline (as AVP falls, water diuresis ensues)
- Hypervolemic (CHF) → optimize cardiac output (ACEi, diuretics cautiously)
2. Correction rate (CRITICAL to prevent ODS)
Maximum safe correction rate: 8-10 mEq/L in 24 hours, 18 mEq/L in 48 hours
Why? After chronic hyponatremia, brain cells lose organic osmolytes. When Na+ is corrected rapidly, brain cells cannot reaccumulate these osmolytes fast enough. The resulting osmotic stress in astrocytes activates the unfolded protein response → apoptosis → Osmotic Demyelination Syndrome (ODS) = central pontine myelinolysis.
High-risk patients for ODS: Alcoholics, malnutrition, liver disease, hypokalemia, burns.
ODS features: Dysarthria, dysphagia, flaccid quadriplegia, "locked-in" syndrome - appearing 2-6 days after correction.
If overcorrection occurs: Give DDAVP (desmopressin) + 5% dextrose water to re-lower Na+.
3. Specific Therapies
| Scenario | Treatment |
|---|---|
| Severe symptomatic (acute): seizures, herniation | 3% hypertonic saline - bolus 100-150 mL over 20 min, repeat as needed; target 5 mEq/L rise over 1 hour to control seizures |
| Chronic, symptomatic | Slow correction with 3% saline; fluid restriction |
| SIADH, chronic, mild | Fluid restriction (< 1-1.5 L/day); urea tablets; tolvaptan/conivaptan (V2 receptor antagonists) |
| Hypovolemic | Isotonic (0.9%) saline - repletes volume, suppresses AVP |
| Beer potomania/low solute | Isotonic saline + resume normal diet |
| K+ depletion + hyponatremia | Replace K+ carefully - K+ replacement itself raises plasma Na+ |
Fluid Restriction (for SIADH/euvolemic)
- Urine-to-plasma ratio > 1 → restrict to < 500 mL/day
- Urine-to-plasma ratio ~1 → restrict to 500-700 mL/day
- Urine-to-plasma ratio < 1 → restrict to < 1 L/day
Vaptans (AVP Receptor Antagonists)
- Tolvaptan (oral, V2-selective) - produces electrolyte-free water excretion ("aquaresis")
- Conivaptan (IV, V1A + V2) - for hospitalized patients
- Use when fluid restriction fails in SIADH; avoid in hypovolemic hyponatremia
- Risk of rapid overcorrection - start low, monitor closely; avoid in liver disease (tolvaptan)
Quick Comparison Table
| Feature | Hypokalemia | Hyponatremia |
|---|---|---|
| Normal range | 3.5-5.0 mEq/L | 136-145 mEq/L |
| Most common cause | Diuretics (thiazide/loop), diarrhea | SIADH, diuretics, heart failure |
| Hallmark ECG change | Prominent U wave, flattened T wave | No specific ECG change (QT shortening reported) |
| Life-threatening complication | VF, paralysis | Cerebral herniation (acute) / ODS (overcorrection) |
| Key investigation | Urine K+ / TTKG | Urine Na+, Urine osmolality, volume status |
| First-line treatment | Oral KCl (correct Mg2+ first) | Treat cause; rate limit correction to 8-10 mEq/L/24h |
| Special warning | Refractory to K+ without Mg2+ repletion | Never correct faster than 10 mEq/L/24h (ODS risk) |
| Important association | Co-exists: correcting K+ raises Na+ | Hypokalemia worsens hyponatremia |
Key High-Yield Mnemonics for MBBS Exams
Causes of SIADH - "MNISSTC"
- Malignancy (SCLC)
- Neurological (meningitis, SAH)
- Infections (pneumonia, TB)
- SSRIs/Drugs
- Surgery/Stress
- Thyroid deficit (hypothyroidism)
- Cortisol deficit (adrenal insufficiency)
Hypokalemia ECG - "No Pot No T" - T wave flattens, U wave appears
ODS Risk in hyponatremia - "ABC of ODS"
- Alcoholism
- Burn patients
- Chronic malnutrition / hypoKalemia / liver disease
Sources: Harrison's Principles of Internal Medicine 22E (2025), Brenner and Rector's The Kidney 10e, Tietz Textbook of Laboratory Medicine 7e, Barash Clinical Anesthesia 9e, Washington Manual of Medical Therapeutics, Morgan & Mikhail's Clinical Anesthesiology 7e
This is a shared conversation. Sign in to Orris to start your own chat.