Bp measurement techniques
Reading File
Finding Sources
Searching the Web
blood pressure measurement techniques clinical guidelines 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Stethoscope on brachial artery guide me
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a complete step-by-step guide to auscultatory BP measurement using the stethoscope over the brachial artery.
Auscultatory Blood Pressure Measurement - Stethoscope on the Brachial Artery
This is the auscultatory method, first described by Scipione Riva-Rocci (1896) and refined by Nikolai Korotkoff (1905). It remains the gold standard for manual BP measurement.
Setup & Patient Preparation
- Patient seated with back supported, feet flat on the floor, arm relaxed and supported at heart level
- No caffeine, smoking, alcohol, or exercise for 30 minutes prior
- Rest quietly for 3-5 minutes before the first reading
- No talking during measurement
Cuff Placement
- Apply the cuff ~2.5 cm (1 inch) above the antecubital fossa (elbow crease)
- The center of the bladder should overlie the brachial artery (usually marked with an arrow on the cuff)
- Cuff sizing: bladder width = at least 40% of arm circumference; length = 80% of arm circumference. Too small a cuff overestimates BP; too large underestimates it.
Stethoscope Placement
- Place the bell of the stethoscope (not the diaphragm) directly over the brachial artery in the antecubital fossa, with as little pressure as possible
- Light pressure is key - heavy pressure can distort Korotkoff sounds or artificially extend Phase IV
Inflation
- First, palpate the radial pulse and inflate the cuff until the pulse disappears
- Inflate a further 30 mmHg above that point (this ensures you are above systolic pressure and avoids missing sounds due to the auscultatory gap)
- Then begin slow, controlled deflation at 2-3 mmHg per second
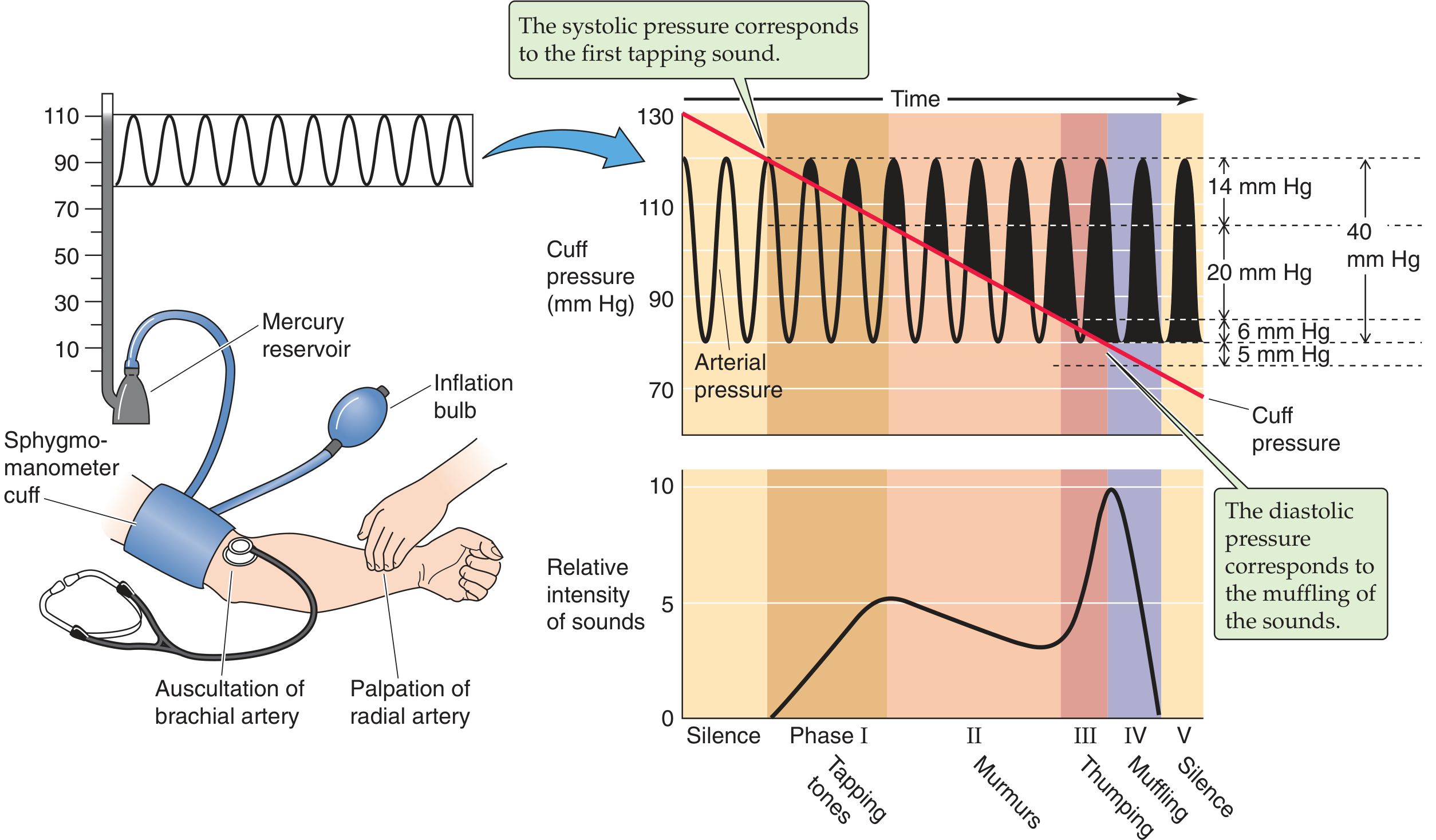
The Korotkoff Sounds - What You Hear
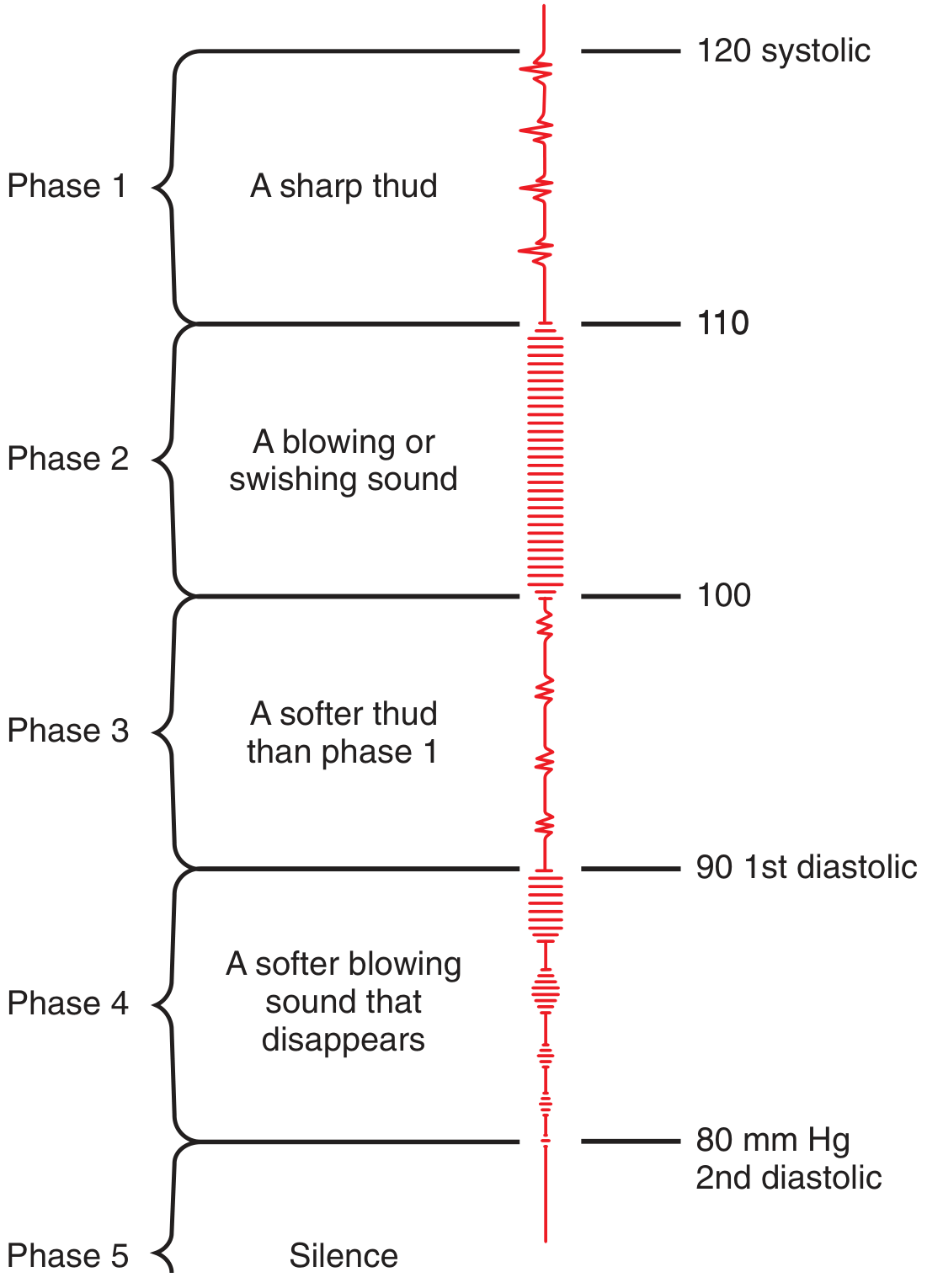
| Phase | Sound | Significance |
|---|---|---|
| Phase I | Sharp, clear tapping sounds, gradually increasing | = Systolic BP - record this pressure |
| Phase II | Blowing or swishing murmur | Turbulent flow as artery partially opens |
| Phase III | Louder thumping sounds | More blood passing under the cuff |
| Phase IV | Sounds become muffled and softer (1st diastolic) | Used as diastolic in children and pregnancy |
| Phase V | Sounds disappear completely (silence) | = Diastolic BP in adults - record this pressure |
- Systolic BP = cuff pressure at first appearance of Phase I tapping sounds
- Diastolic BP = cuff pressure at complete disappearance of sounds (Phase V)
- In children, use Phase IV (muffling) for diastolic, since sounds may never disappear
The Auscultatory Gap
In some patients (especially elderly or hypertensive), sounds may disappear briefly between Phase I and Phase III, then reappear. This is the auscultatory gap and can cause the examiner to underestimate systolic BP by 10-40 mmHg if the cuff was not inflated high enough. Always over-inflate by 30 mmHg above the palpated systolic.
After Measurement
- Fully deflate the cuff and wait 1-2 minutes before repeating
- Record the average of 2 readings
- Use the arm with the higher reading on the first visit
- Tell the patient their result
Common Errors to Avoid
| Error | Effect |
|---|---|
| Cuff too small | Falsely HIGH reading |
| Cuff too large | Falsely LOW reading |
| Arm below heart level | Overestimation |
| Deflating too fast (>2-3 mmHg/s) | Missing sounds, underestimates systolic |
| Heavy stethoscope pressure | Artificially extends Phase IV, underestimates diastolic |
| Not palpating first | May miss auscultatory gap |
| Patient talking | Raises BP 6-7 mmHg |
Why the Bell Over the Diaphragm?
Korotkoff sounds are low-frequency sounds. The bell of the stethoscope is designed to pick up low-frequency sounds better than the diaphragm. Research confirms the bell placed over the cubital fossa (or directly over the brachial artery) gives the best sound quality. However, modern stethoscopes with tunable diaphragms can also perform well.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 40-41
- Medical Physiology (Boron & Boulpaep), p. 615
- Tintinalli's Emergency Medicine, p. 253-254
This is a shared conversation. Sign in to Orris to start your own chat.