Explain me the topic ultrasound in pregnancy in detail for my medical final yr proff exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from Creasy & Resnik's Maternal-Fetal Medicine to compose a thorough final exam answer. Let me now compile the complete response.
Ultrasound in Pregnancy - Complete Guide for Final Year MBBS Exam
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice
1. Introduction and Principles
Obstetric ultrasound is the primary imaging modality in pregnancy. It uses high-frequency sound waves (2-10 MHz) that are reflected differently by tissues of varying acoustic impedance. The technique is safe (no ionizing radiation), real-time, and widely available.
The midtrimester fetal ultrasound examination ("anatomy scan") serves as an important checkpoint for evaluation of the pregnancy and its potential risks. It:
- Compares obstetric dating with fetal biometric measures
- Identifies structural abnormalities prior to fetal viability
- Detects maternal uterine findings (fibroids, placenta previa/accreta) requiring management changes
2. Types of Obstetric Ultrasound Examinations
| Examination Type | Timing | Purpose |
|---|---|---|
| First Trimester Standard (CPT 76801) | <14 weeks | Gestational age, fetal number, cardiac activity, NT |
| Basic Midtrimester (CPT 76805) | 18-22 weeks | Anatomy scan, biometry, placenta, AFV |
| Detailed Level II (CPT 76811) | When indicated | High-risk, known/suspected anomaly, detailed anatomy |
| Follow-up (CPT 76816) | As needed | Serial growth, reassessment |
| Limited (CPT 76815) | Specific indication | Fetal position, heartbeat, fluid check |
All examinations require a formal report containing:
- Patient identifying information
- Indication for the procedure
- Gestational age by established dates
- Fetal biometry with predicted gestational age
- Fetal number and chorionicity (if multifetal)
- Principal findings (normal, abnormal, and poorly visualized)
- Differential diagnosis for any abnormalities
- Recommendations for further management
3. First Trimester Ultrasound (6-13 Weeks)
Key Assessments
- Gestational sac: first structure visible (~4.5-5 weeks)
- Yolk sac: seen by ~5-6 weeks
- Fetal pole and cardiac activity: visible from ~6 weeks
- Crown-rump length (CRL): most accurate dating parameter in 1st trimester; error ±5-7 days
Dating Accuracy
- CRL is the gold standard for gestational age estimation in the first trimester
- Gestational sac size or CRL is a reliable measure of gestational age (within ±5 days up to 10 weeks; ±7 days up to 13 weeks)
First Trimester Structural Survey
- Assess intracranial anatomy (nasal bone, posterior fossa)
- Cardiac 4-chamber view feasible at 11-14 weeks
- Identify major malformations early (anencephaly, major cardiac defects, omphalocele, etc.)
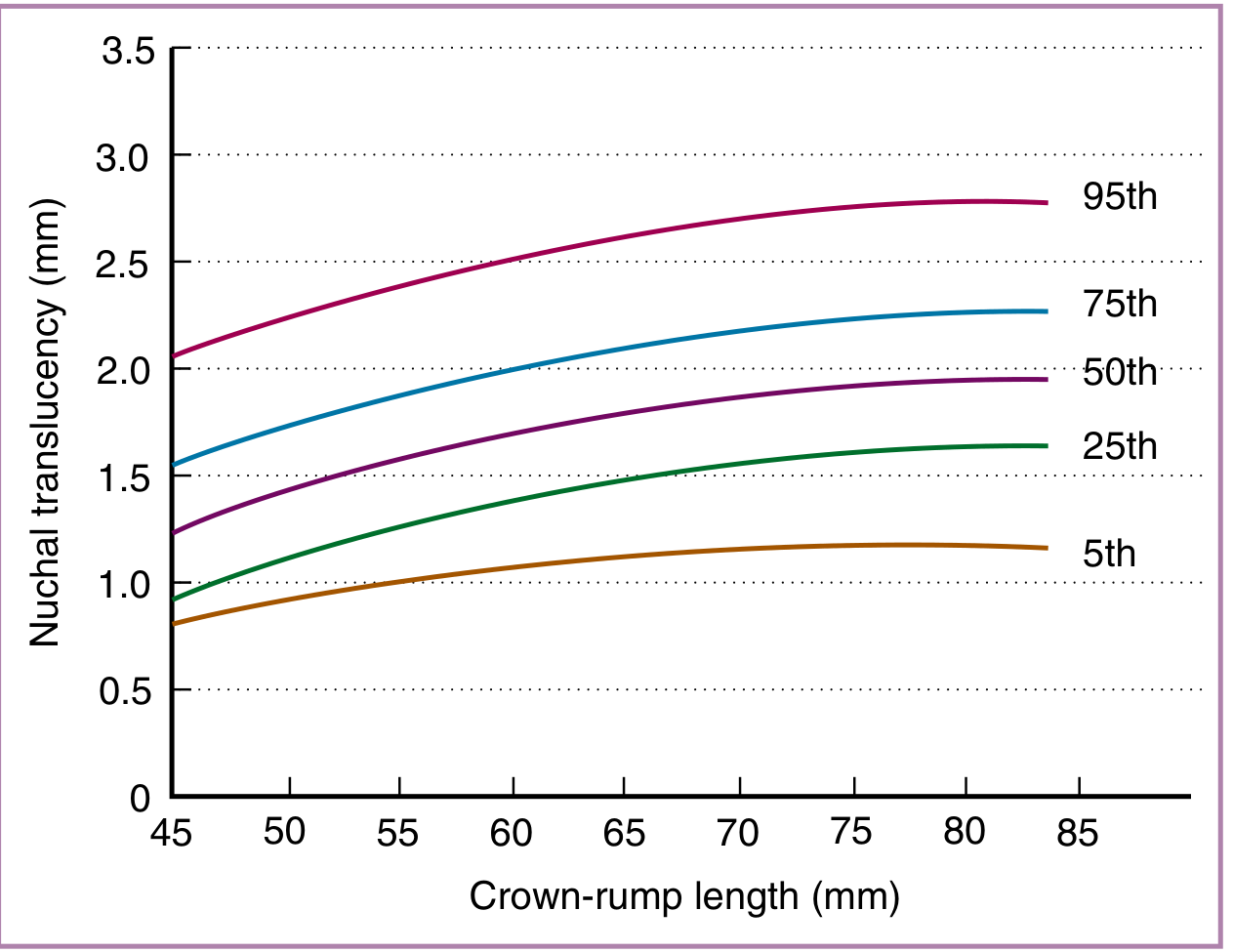
4. Nuchal Translucency (NT) - First Trimester Aneuploidy Screening
NT is defined as the collection of fluid under the skin behind the neck in fetuses between 11 and 14 weeks gestation.
NT Measurement Standards
- CRL must be 45-84 mm (success rate 98-100%)
- Either transabdominal (95% success) or transvaginal scanning
- True midline sagittal view of fetal spine in cervical and thoracic region; tip of nose visible; 3rd and 4th ventricle visible
- Magnification: fetal head, neck, and upper thorax must occupy >50% of the image
- Distinguish fetal skin from amniotic membrane carefully
- Calipers placed on the inner borders of the nuchal space; horizontal crossbar must NOT protrude into the space
- Maximum measurement is recorded
NT as Screening Tool
- NT measurement combined with maternal age and gestational age:
- Cutoff >1:300 = screen positive
- Detection rate for trisomy 21: 77-82% at 5-8.3% false-positive rate
- Combined with PAPP-A and free β-hCG: detection rate ~88%
- NT ≥3.0 mm is a clinically significant threshold
Combined First Trimester Screening (Combined Test)
Combines NT + nasal bone + serum markers:
- PAPP-A (pregnancy-associated plasma protein A)
- Free β-hCG
- Detection of Down syndrome: ~85-93% at 5% FPR
5. Nasal Bone Assessment (1st Trimester Marker)
- Based on the flat nasal bridge phenotype of Down syndrome
- Nasal bone is absent in 73% of trisomy 21 fetuses vs only 0.5% of euploid fetuses
- Sensitivity of absent nasal bone alone for trisomy 21: 65% with FPR of 0.8%
- Positive predictive value: 54% (one in two fetuses with absent NB had trisomy 21)
- Absent NB increases likelihood of trisomy 21 by 87-fold
- When combined with maternal age + NT: detection rate ~93% at 5% FPR
6. Second Trimester (Midtrimester) Anatomy Scan - 18-22 Weeks
This is the most important single ultrasound examination in pregnancy. It detects ~60% of major structural anomalies (Gagnon et al.).
Standard Midtrimester Anatomy Assessment Elements (CPT 76805)
Head and Face:
- Cranial bones (integrity, shape)
- Falx cerebri
- Cavum septi pellucidi (CSP) - absence suggests agenesis of corpus callosum or HPE
- Thalami
- Lateral ventricles - atrial width ≤10 mm is normal (ventriculomegaly if >10 mm)
- Cerebellum - banana sign in spina bifida
- Cisterna magna - obliterated in Chiari II
- Orbits
- Facial profile
- Upper lip (for cleft)
Thorax:
- Four-chamber view of heart (detects most major CHD)
- Cardiac axis (levocardia normal; dextrocardia suggests situs inversus or malformation)
- Left ventricular outflow tract (LVOT)
- Right ventricular outflow tract (RVOT)
- Lung parenchyma
Abdomen:
- Stomach (fluid-filled; gastric bubble absent in esophageal atresia)
- Intestines
- Abdominal umbilical cord insertion (omphalocele vs gastroschisis differentiation)
- Kidneys (bilateral; renal pelvis <10 mm AP diameter)
- Bladder and umbilical arteries (2 arteries + 1 vein; single umbilical artery = aneuploidy risk)
Spine and Extremities:
- Spine in longitudinal and transverse views (spina bifida, sacral agenesis)
- Upper and lower long bones of all 4 extremities (shortening in skeletal dysplasias)
- Hand and foot anatomy and posture (clubfoot, polydactyly)
- Genitalia appearance and gender

Placenta and Umbilical Cord:
- Location (previa if within 2 cm of os)
- Appearance (cysts, lucencies, accessory lobe)
- Umbilical cord vessels (normal = 2 arteries + 1 vein)
- Cord insertion into placenta (velamentous = risk)
Amniotic Fluid Volume:
- Maximum Vertical Pocket (MVP): normal 2-8 cm
- Amniotic Fluid Index (AFI): sum of MVP in 4 quadrants; normal 8-25 cm
- AFI <5 cm = oligohydramnios
- AFI >25 cm = polyhydramnios
- MVP <2 cm or AFI <5 cm = oligohydramnios
- MVP >8 cm or AFI >25 cm = polyhydramnios
7. Fetal Biometry and Growth Assessment
The four standard biometric measurements:
| Parameter | Plane | Age Range Most Useful |
|---|---|---|
| BPD (Biparietal Diameter) | Transventricular axial | 14-28 weeks |
| HC (Head Circumference) | Same plane as BPD | 14-40 weeks |
| AC (Abdominal Circumference) | At level of portal vein/stomach | All trimesters |
| FL (Femur Length) | Long axis of femur diaphysis | 14-40 weeks |
- EFW (Estimated Fetal Weight) = derived from HC, AC, FL (Hadlock formula most common)
- AC is the most sensitive parameter for detecting IUGR (reflects liver glycogen stores)
- Growth restriction = EFW <10th percentile for gestational age
- Serial growth scans every 3-4 weeks recommended for high-risk pregnancies
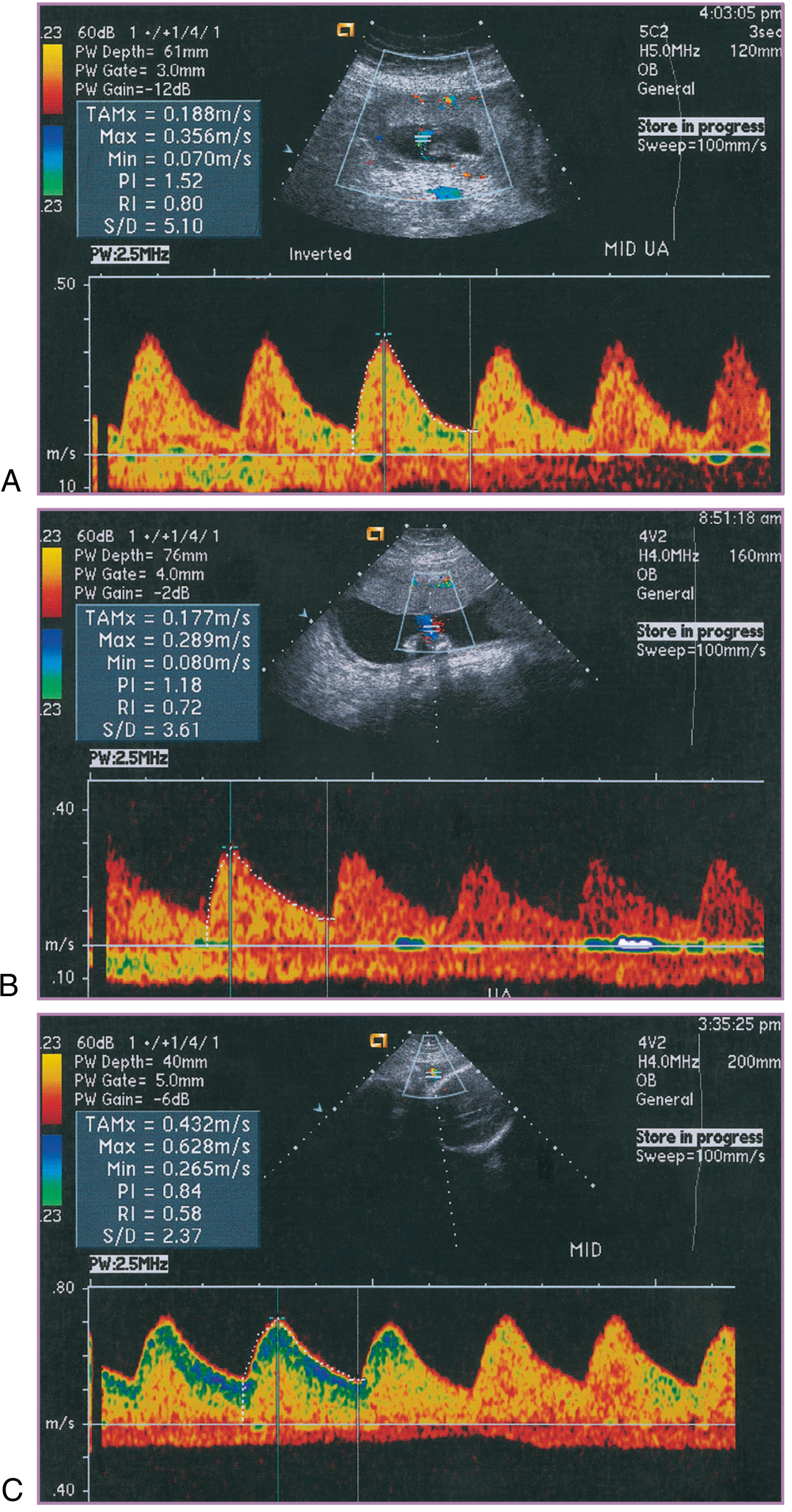
8. Doppler Ultrasound in Pregnancy
Doppler velocimetry assesses blood flow by measuring frequency shift of sound waves reflected from moving red cells.
Key Doppler Parameters
- S/D ratio = Peak systolic velocity / End-diastolic velocity
- Pulsatility Index (PI) = (S-D) / mean velocity
- Resistance Index (RI) = (S-D) / S
Umbilical Artery Doppler
- Reflects placental vascular resistance
- Normal: S/D ratio decreases through pregnancy (diastolic flow increases as placenta matures)
- Abnormal patterns (progressively worsening):
- Elevated S/D ratio - increased resistance, early IUGR
- Absent end-diastolic flow (AEDF) - severe placental insufficiency
- Reversed end-diastolic flow (REDF) - critical, immediate delivery often needed
- Umbilical artery Doppler findings strongly correlate with fetal growth restriction and critical fetal/neonatal outcomes
Middle Cerebral Artery (MCA) Doppler
- Low resistance normally (brain must receive high continuous flow)
- Brain-sparing: In IUGR, MCA PI falls (↓ cerebral resistance) as a compensatory mechanism
- MCA PSV (Peak Systolic Velocity): used to detect fetal anemia
- MCA PSV >1.5 MoM = significant fetal anemia (sensitivity ~88%)
- Replaced invasive amniocentesis for rhesus disease monitoring
Ductus Venosus Doppler
- Reflects fetal cardiac preload/right heart function
- Absent or reversed A-wave in ductus venosus = imminent fetal deterioration
- Combined with biophysical variables for preterm fetus surveillance
Uterine Artery Doppler
- Used for preeclampsia and IUGR prediction (usually at 20-24 weeks)
- Notching (persistence of early diastolic notch) = abnormal
- Elevated PI with bilateral notching = high risk for preeclampsia and placental insufficiency
9. Second Trimester Ultrasound Markers of Aneuploidy (Soft Markers)
| Marker | Association |
|---|---|
| Nuchal fold thickness ≥6 mm (16-20 weeks) | Trisomy 21 |
| Echogenic bowel | Trisomy 21, CF, CMV |
| Echogenic intracardiac focus (EIF) | Trisomy 21 (minor) |
| Short femur/humerus | Trisomy 21 |
| Choroid plexus cysts (CPCs) | Trisomy 18 |
| Renal pyelectasis | Trisomy 21 |
| Single umbilical artery | Trisomy 18 |
| Absent/hypoplastic nasal bone | Trisomy 21 |
Multiple soft markers in combination increase aneuploidy risk multiplicatively. Isolated minor markers in low-risk patients may not warrant invasive testing.
10. Cervical Ultrasound
- Transvaginal measurement of cervical length is the gold standard
- Normal cervical length: ≥25 mm at 16-24 weeks
- Short cervix (<25 mm) is the strongest predictor of spontaneous preterm birth
- Short cervix + fetal fibronectin (fFN) positive = highest risk
- Indications: previous preterm birth, cerclage assessment, incompetent cervix
11. Third Trimester Ultrasound
Key indications and assessments:
- Serial growth monitoring for suspected IUGR or macrosomia
- Biophysical Profile (BPP) scoring (fetal movement, tone, breathing, fluid, NST)
- Presentation (cephalic/breech/transverse) - important before 36 weeks for ECV counseling
- Placental localization - reassess placenta previa (often resolves by 36 weeks)
- Amniotic fluid assessment in post-dates, IUGR, PROM
Biophysical Profile (BPP)
Each of 5 parameters scored 0 or 2 (total max 10):
- Fetal movement (≥3 discrete body movements in 30 min)
- Fetal tone (≥1 episode of active extension/flexion)
- Fetal breathing movements (≥1 episode ≥30 sec in 30 min)
- Amniotic fluid volume (MVP ≥2 cm)
- Non-stress test (reactive = ≥2 accelerations)
| Score | Interpretation |
|---|---|
| 8-10/10 | Normal - reassuring |
| 6/10 | Equivocal - repeat in 24h |
| ≤4/10 | Abnormal - consider delivery |
12. Special Indications and Advanced Techniques
3D/4D Ultrasound
- Better for surface anatomy (cleft lip/palate, skeletal dysplasias)
- 4D = real-time 3D (fetal behavior, facial expressions)
- Limitation: image quality limited by fetal position and amniotic fluid
Color Doppler
- Detects vascular abnormalities (vasa previa, placenta accreta, cardiac defects)
- Vasa previa: fetal vessels overlying the cervical os - high risk of fetal exsanguination with membrane rupture
Transvaginal Ultrasound (TVS)
- Better resolution in early pregnancy
- Essential for cervical length
- First trimester bleeding workup (intrauterine vs ectopic)
13. Safety of Ultrasound in Pregnancy
- No ionizing radiation - no proven teratogenic effects
- Based on sound wave energy (mechanical and thermal effects at high intensities)
- ALARA principle (As Low As Reasonably Achievable): use minimum exposure to obtain diagnostic information
- Doppler has higher energy output than B-mode - use judiciously in first trimester
- No evidence of harm from routine clinical use at standard diagnostic settings
14. Indications for Ultrasound at Different Gestational Ages - Summary Table
| Trimester | Weeks | Main Purpose |
|---|---|---|
| 1st | 6-9 | Confirm intrauterine pregnancy, viability, number, gestational age (CRL) |
| 1st | 11-14 | NT measurement, aneuploidy screening, fetal survey, nasal bone |
| 2nd | 18-22 | Anatomy scan (standard/level II), biometry, placental location, AFV |
| 2nd | 22-24 | Uterine artery Doppler (preeclampsia risk), cervical length |
| 3rd | 28-32 | Fetal growth, presentation |
| 3rd | 36+ | Presentation, placenta, AFV, BPP, Doppler if indicated |
15. Exam High-Yield Points
- NT >3.5 mm = significant even if <95th percentile - needs karyotyping
- CRL is the most accurate method for dating (error ±5 days in 1st trimester)
- AC is most sensitive for IUGR detection
- Absent nasal bone increases trisomy 21 risk 87-fold
- AEDF/REDF in umbilical artery = critical IUGR - consider delivery
- MCA PSV >1.5 MoM = significant fetal anemia
- AFI <5 = oligohydramnios; AFI >25 = polyhydramnios
- Cervical length <25 mm at 16-24 weeks = preterm birth risk
- 4-chamber view + LVOT + RVOT = detects >80% of major CHD
- BPP ≤4/10 = abnormal, consider immediate delivery
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, 9th Ed.
Give information from marrow
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have now reviewed the complete catalog of all books in the medical library. Here's the honest answer:
"Marrow" is not available in this medical library.
The library contains standard international medical textbooks (Harrison's, Robbins, Guyton, Creasy & Resnik, Bailey & Love, etc.) but does not include Marrow - the Indian medical education platform/app used for MBBS exam preparation.
Marrow is a proprietary Indian med-ed platform with its own question banks, notes, and video lectures. Its content is not part of this textbook library.
What I can offer instead:
-
From the existing library - I already gave you a detailed answer from Creasy & Resnik's Maternal-Fetal Medicine (the gold-standard obstetrics reference) in the previous response. That content directly maps to what your final year proficiency exam will test.
-
If you have Marrow notes - you can paste or upload them here and I'll help you understand, expand, or explain any concept from those notes using the library textbooks.
-
I can reframe the previous answer in a more exam-point / high-yield format similar to how Marrow presents topics - short, structured, memory-friendly - if that's what you're looking for.
Would you like me to reformat the ultrasound in pregnancy content into a Marrow-style high-yield notes format (with mnemonics, tables, and exam points)?
Make flashcards of all the info above
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/usg-flashcards
Writing File
~/usg-flashcards/make_flashcards.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Ultrasound in Pregnancy – Flashcards";
pres.author = "Orris Medical";
// ─── COLOUR PALETTE ───────────────────────────────────────────────────────────
const BG_QUESTION = "1A237E"; // deep navy (question side)
const BG_ANSWER = "FFFFFF"; // white (answer side)
const BG_TITLE = "0D47A1"; // royal blue (section dividers)
const ACCENT = "E3F2FD"; // ice blue (answer header band)
const Q_TEXT = "FFFFFF"; // white text on navy
const A_LABEL = "1565C0"; // blue for "ANSWER" label
const A_TEXT = "1A1A2E"; // near-black body
const BORDER = "BBDEFB"; // light blue border
const TAG_BG = "E8F5E9"; // light green for exam-tip tags
const TAG_TEXT = "1B5E20";
// ─── HELPERS ──────────────────────────────────────────────────────────────────
function sectionDivider(title, subtitle) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: BG_TITLE } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 2.4, w: 10, h: 0.06, fill: { color: "64B5F6" } });
s.addText(title, {
x: 0.5, y: 1.4, w: 9, h: 1.0,
fontSize: 36, bold: true, color: "FFFFFF", align: "center", fontFace: "Calibri"
});
if (subtitle) {
s.addText(subtitle, {
x: 0.5, y: 2.6, w: 9, h: 0.9,
fontSize: 18, color: "90CAF9", align: "center", fontFace: "Calibri", italic: true
});
}
s.addText("Ultrasound in Pregnancy | Final Year MBBS", {
x: 0.5, y: 5.1, w: 9, h: 0.4,
fontSize: 10, color: "5C6BC0", align: "center", fontFace: "Calibri"
});
}
// cardNumber shown bottom-right
let cardNum = 0;
function flashcard(question, answerLines, examTip) {
cardNum++;
// ── QUESTION SLIDE ────────────────────────────────────────────────────────
const q = pres.addSlide();
q.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: BG_QUESTION } });
// top strip
q.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.55, fill: { color: "0D47A1" } });
q.addText("Q", {
x: 0.2, y: 0.07, w: 0.4, h: 0.38,
fontSize: 20, bold: true, color: "90CAF9", fontFace: "Calibri", align: "center"
});
q.addText(`CARD ${cardNum}`, {
x: 8.5, y: 0.12, w: 1.3, h: 0.3,
fontSize: 11, color: "90CAF9", fontFace: "Calibri", align: "right"
});
// question text
q.addText(question, {
x: 0.6, y: 0.9, w: 8.8, h: 4.2,
fontSize: 22, bold: true, color: Q_TEXT, fontFace: "Calibri",
align: "center", valign: "middle", wrap: true
});
// bottom hint
q.addText("▼ Flip for answer", {
x: 0.5, y: 5.18, w: 9, h: 0.35,
fontSize: 10, color: "5C6BC0", align: "center", fontFace: "Calibri", italic: true
});
// ── ANSWER SLIDE ─────────────────────────────────────────────────────────
const a = pres.addSlide();
a.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: BG_ANSWER } });
// header band
a.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: ACCENT } });
a.addText("A", {
x: 0.2, y: 0.1, w: 0.4, h: 0.5,
fontSize: 22, bold: true, color: A_LABEL, fontFace: "Calibri", align: "center"
});
a.addText(question.length > 80 ? question.substring(0, 80) + "…" : question, {
x: 0.75, y: 0.1, w: 8.5, h: 0.5,
fontSize: 12, color: "546E7A", fontFace: "Calibri", italic: true, valign: "middle"
});
// build rich-text answer array
const richLines = [];
answerLines.forEach((line, i) => {
if (typeof line === "string") {
richLines.push({ text: line, options: { bullet: { type: "bullet", indent: 15 }, color: A_TEXT, fontSize: 16, fontFace: "Calibri", breakLine: true } });
} else if (line.header) {
if (i > 0) richLines.push({ text: "", options: { breakLine: true, fontSize: 6 } });
richLines.push({ text: line.header, options: { bold: true, color: A_LABEL, fontSize: 15, fontFace: "Calibri", breakLine: true, underline: true } });
} else if (line.value) {
richLines.push({ text: `${line.key}: `, options: { bold: true, color: "0D47A1", fontSize: 15, fontFace: "Calibri" } });
richLines.push({ text: line.value, options: { color: A_TEXT, fontSize: 15, fontFace: "Calibri", breakLine: true } });
}
});
if (richLines.length) {
a.addText(richLines, { x: 0.4, y: 0.85, w: 9.2, h: examTip ? 3.9 : 4.5, wrap: true, valign: "top" });
}
// exam tip
if (examTip) {
a.addShape(pres.ShapeType.rect, { x: 0.3, y: 4.82, w: 9.4, h: 0.62, fill: { color: TAG_BG }, line: { color: "A5D6A7", width: 1 } });
a.addText([
{ text: "★ EXAM TIP: ", options: { bold: true, color: TAG_TEXT, fontSize: 13, fontFace: "Calibri" } },
{ text: examTip, options: { color: TAG_TEXT, fontSize: 13, fontFace: "Calibri" } }
], { x: 0.5, y: 4.85, w: 9.0, h: 0.56, wrap: true, valign: "middle" });
}
a.addText(`Card ${cardNum}`, {
x: 8.8, y: 5.33, w: 1.0, h: 0.25,
fontSize: 9, color: "B0BEC5", align: "right", fontFace: "Calibri"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// COVER
// ══════════════════════════════════════════════════════════════════════════════
const cover = pres.addSlide();
cover.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: "0A1045" } });
cover.addShape(pres.ShapeType.rect, { x: 0, y: 4.8, w: 10, h: 0.825, fill: { color: "0D47A1" } });
cover.addShape(pres.ShapeType.rect, { x: 0, y: 1.95, w: 10, h: 0.06, fill: { color: "1565C0" } });
cover.addText("ULTRASOUND IN PREGNANCY", {
x: 0.5, y: 0.5, w: 9, h: 1.3,
fontSize: 38, bold: true, color: "FFFFFF", align: "center", fontFace: "Calibri", charSpacing: 2
});
cover.addText("FLASHCARD DECK", {
x: 0.5, y: 1.7, w: 9, h: 0.6,
fontSize: 22, color: "64B5F6", align: "center", fontFace: "Calibri", charSpacing: 4
});
cover.addText("Final Year MBBS · Obstetrics & Gynaecology", {
x: 0.5, y: 2.2, w: 9, h: 0.6,
fontSize: 16, color: "90CAF9", align: "center", fontFace: "Calibri", italic: true
});
cover.addText("Topics Covered:", {
x: 1.0, y: 2.95, w: 8, h: 0.45,
fontSize: 14, bold: true, color: "E3F2FD", fontFace: "Calibri"
});
cover.addText([
{ text: "Principles · Types of Scans · First Trimester · NT Screening · Nasal Bone · Anatomy Scan\n", options: { color: "90CAF9", fontSize: 13, fontFace: "Calibri" } },
{ text: "Fetal Biometry · Doppler · Soft Markers · Cervical Length · Third Trimester · BPP", options: { color: "90CAF9", fontSize: 13, fontFace: "Calibri" } }
], { x: 1.0, y: 3.4, w: 8, h: 1.2, wrap: true });
cover.addText("Source: Creasy & Resnik's Maternal-Fetal Medicine | Orris AI", {
x: 0.5, y: 4.88, w: 9, h: 0.3,
fontSize: 10, color: "90CAF9", align: "center", fontFace: "Calibri"
});
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 1 – PRINCIPLES
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 1", "Principles & Physics of Obstetric Ultrasound");
flashcard(
"What is the physical principle behind obstetric ultrasound?",
[
"Uses high-frequency sound waves (2–10 MHz)",
"Waves reflect differently from tissues with varying acoustic impedance",
"No ionising radiation – safe throughout pregnancy",
"Real-time B-mode imaging is standard",
"Doppler mode measures frequency shift from moving red cells"
],
"USG is the ONLY imaging modality that is safe at ALL gestational ages"
);
flashcard(
"What is the ALARA principle in obstetric ultrasound?",
[
{ key: "ALARA", value: "As Low As Reasonably Achievable" },
"Use minimum exposure to obtain diagnostic information",
"Doppler has HIGHER energy output than B-mode",
"Use Doppler judiciously in the first trimester",
"No proven teratogenic effects at standard diagnostic settings"
],
"Doppler in 1st trimester: use only when clinically indicated (higher thermal index)"
);
flashcard(
"What are the three main values delivered by the midtrimester anatomy scan?",
[
"1. Confirms/corrects gestational age by biometry",
"2. Detects structural fetal abnormalities before viability",
"3. Identifies maternal findings – fibroids, placenta previa/accreta"
],
"Anatomy scan detects ~60% of major structural anomalies (Gagnon et al.)"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 2 – TYPES OF EXAMINATIONS
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 2", "Types of Obstetric Ultrasound Examinations");
flashcard(
"Name the main types of obstetric ultrasound and their CPT codes.",
[
{ key: "76801", value: "Standard 1st trimester (<14 wks) – single gestation" },
{ key: "76802", value: "Standard 1st trimester – each additional gestation" },
{ key: "76805", value: "Basic midtrimester anatomy scan (18–22 wks)" },
{ key: "76811", value: "Detailed Level II – known/suspected anomaly" },
{ key: "76816", value: "Follow-up / serial growth scans" },
{ key: "76815", value: "Limited – fetal position, heartbeat, fluid check" }
],
"76811 (Level II) is NOT for routine scans – needs a specific indication (anomaly risk, diabetes, teratogen)"
);
flashcard(
"What must every obstetric ultrasound report contain?",
[
"Patient identifying information & date",
"Indication for the procedure",
"Type of examination",
"Gestational age by established dates",
"Fetal number & chorionicity (if multifetal)",
"Fetal biometry with predicted gestational age",
"Principal findings – normal, abnormal, poorly visualised",
"Differential diagnosis for any abnormality",
"Recommendations for management or further scans"
],
null
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 3 – FIRST TRIMESTER
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 3", "First Trimester Ultrasound (6–13 Weeks)");
flashcard(
"What are the sequential sonographic milestones in the first trimester?",
[
{ key: "~4.5–5 wks", value: "Gestational sac (first structure visible)" },
{ key: "~5–6 wks", value: "Yolk sac" },
{ key: "~6 wks", value: "Fetal pole + cardiac activity" },
{ key: "6–13 wks", value: "Crown-rump length (CRL) – gold standard dating" }
],
"Cardiac activity visible from ~6 weeks (FHR 90–110 bpm at 6 wks → 150–180 at 8–10 wks)"
);
flashcard(
"What is the most accurate parameter for gestational age in the first trimester, and what is its error margin?",
[
{ key: "Parameter", value: "Crown-Rump Length (CRL)" },
{ key: "Error ≤10 wks", value: "± 5 days" },
{ key: "Error 10–13 wks", value: "± 7 days" },
"CRL is SUPERIOR to LMP in irregular cycles",
"Measured in strict mid-sagittal plane, maximum length of embryo",
"After 13 wks, CRL loses accuracy – use biometry (BPD, HC, AC, FL)"
],
"If CRL and LMP differ by >7 days before 10 wks, change EDD to CRL-based date"
);
flashcard(
"What structural assessments are possible at 11–14 weeks?",
[
"Nuchal translucency (NT) measurement",
"Nasal bone assessment",
"Cardiac 4-chamber view (feasible early)",
"Intracranial anatomy – posterior fossa, falx",
"Major malformation screen: anencephaly, omphalocele, megacystis",
"Chorionicity determination in multiple pregnancy (most accurate before 14 wks)"
],
"Chorionicity: T-sign = monochorionic; Lambda (twin-peak) sign = dichorionic"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 4 – NUCHAL TRANSLUCENCY
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 4", "Nuchal Translucency (NT) Screening");
flashcard(
"Define Nuchal Translucency (NT). When is it measured?",
[
"Collection of fluid under the skin behind the fetal neck",
{ key: "Gestational window", value: "11–14 weeks" },
{ key: "CRL range", value: "45–84 mm" },
"Transabdominal approach successful in ~95% of cases",
"Median NT increases with CRL – must convert to MoM or delta NT before risk calculation",
"Reflects lymphatic fluid accumulation related to chromosomal/cardiac anomalies"
],
"NT ≥3.5 mm is significant even if below 95th centile – warrants karyotyping"
);
flashcard(
"List the 7 technical standards for NT measurement.",
[
"1. CRL must be 45–84 mm (success 98–100%)",
"2. Transabdominal OR transvaginal (TA preferred)",
"3. True mid-sagittal view – tip of nose visible, 3rd & 4th ventricle seen",
"4. Fetal head, neck & upper thorax occupy >50% of image",
"5. Clearly distinguish fetal skin from amniotic membrane",
"6. Calipers on INNER borders of nuchal space; crossbar must NOT protrude into space",
"7. Maximum measurement is recorded and used for risk calculation"
],
"Calipers on INNER borders – most common exam question about NT technique"
);
flashcard(
"What is the Down syndrome detection rate of NT alone vs combined first-trimester screening?",
[
{ key: "NT alone", value: "77–82% detection at 5–8.3% FPR" },
{ key: "NT + age", value: "77% at 5% FPR (cutoff >1:300)" },
{ key: "Combined test (NT + PAPP-A + free β-hCG)", value: "~88% detection at 5% FPR" },
{ key: "With nasal bone added", value: "~93% detection at 5% FPR" },
"Sample: >100,000 pregnancies; 326 trisomy 21 fetuses"
],
"Combined 1st trimester test = NT + PAPP-A + free β-hCG → 88% detection"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 5 – NASAL BONE
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 5", "Nasal Bone – First Trimester Marker");
flashcard(
"What is the clinical significance of absent nasal bone in the first trimester?",
[
"Based on flat nasal bridge – classic feature of Down syndrome",
{ key: "Absent NB in trisomy 21", value: "73% of cases" },
{ key: "Absent NB in euploid fetuses", value: "only 0.5%" },
{ key: "Sensitivity (absent NB alone)", value: "65% for trisomy 21" },
{ key: "FPR", value: "0.8%" },
{ key: "PPV", value: "54% – 1 in 2 fetuses with absent NB had trisomy 21" },
{ key: "Likelihood ratio increase", value: "87-fold for trisomy 21" }
],
"Absent NB → 87× increase in trisomy 21 risk. Combined with NT + age → 93% detection"
);
flashcard(
"What factors affect nasal bone visibility / absence in euploid fetuses?",
[
"Increasing NT measurement (more absent NB with higher NT)",
"Ethnicity – African origin has higher rate of absent NB in euploids",
"Gestational age / CRL – affects ossification timing",
"Must be imaged in strict mid-sagittal plane at correct angle",
"Absent NB in 2nd trimester (14–25 wks) found in 1/3 of Down syndrome (radiographic studies)"
],
null
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 6 – ANATOMY SCAN
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 6", "Second Trimester Anatomy Scan (18–22 Weeks)");
flashcard(
"What are the HEAD & FACE elements assessed in the standard midtrimester anatomy scan?",
[
"Cranial bones (integrity, shape – lemon sign in spina bifida)",
"Falx cerebri",
"Cavum septi pellucidi (CSP) – absent → agenesis of CC or HPE",
"Thalami",
"Lateral ventricles (atrial width ≤10 mm is normal)",
"Cerebellum (banana sign in spina bifida; Chiari II)",
"Cisterna magna (obliterated in Chiari II)",
"Orbits",
"Facial profile & nasal bone",
"Upper lip (cleft lip screening)"
],
"Absent CSP → think agenesis of corpus callosum or holoprosencephaly"
);
flashcard(
"What are the THORAX elements in the midtrimester anatomy scan?",
[
"Four-chamber view of heart (detects most major CHD)",
"Cardiac axis (normal = 45° ± 20° to left) – dextrocardia if deviated right",
"Left ventricular outflow tract (LVOT) – aortic root",
"Right ventricular outflow tract (RVOT) – pulmonary artery",
"Lung parenchyma (echogenicity for CDH, CCAM)"
],
"4-chamber + LVOT + RVOT views together detect >80% of significant CHD"
);
flashcard(
"What are the ABDOMINAL elements in the midtrimester anatomy scan?",
[
"Stomach (fluid-filled gastric bubble; absent → esophageal atresia)",
"Intestines (echogenic bowel = soft marker for aneuploidy, CF, CMV)",
"Abdominal cord insertion (omphalocele: covered, cord at apex; gastroschisis: uncovered, to right of cord)",
"Kidneys bilaterally (renal pelvis AP <10 mm)",
"Bladder (distended = obstruction; absent = bilateral renal agenesis)",
"Umbilical arteries around bladder (normal = 2 arteries; single UA = trisomy 18 risk)"
],
"Omphalocele: liver-covered mass at cord base → high aneuploidy risk. Gastroschisis: bowel floating freely, to right of cord"
);
flashcard(
"What are the SPINE & EXTREMITY elements in the midtrimester scan?",
[
"Spine in BOTH longitudinal and transverse planes (spina bifida, sacral agenesis)",
"Upper long bones: humerus, radius/ulna – both sides",
"Lower long bones: femur, tibia/fibula – both sides",
"Hand and foot anatomy (clubfoot, polydactyly, rocker-bottom foot = trisomy 18)",
"Posture of hands and feet",
"Genitalia (gender determination)"
],
"Clubfoot (talipes) is a soft marker for trisomy 18 (especially with other anomalies)"
);
flashcard(
"What placenta, cord & amniotic fluid parameters are documented in the anatomy scan?",
[
{ header: "PLACENTA" },
"Location (previa if <2 cm from internal os on TVS)",
"Appearance: cysts, lucencies, accessory lobe",
"Cord insertion site into placenta (velamentous = risk of vasa previa)",
{ header: "AMNIOTIC FLUID VOLUME" },
{ key: "AFI (4-quadrant sum)", value: "Normal 8–25 cm" },
{ key: "MVP (max vertical pocket)", value: "Normal 2–8 cm" },
{ key: "Oligohydramnios", value: "AFI <5 cm OR MVP <2 cm" },
{ key: "Polyhydramnios", value: "AFI >25 cm OR MVP >8 cm" }
],
"Placenta previa diagnosed if placental edge <2 cm from internal os on TVS at 32+ weeks"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 7 – FETAL BIOMETRY
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 7", "Fetal Biometry & Growth Assessment");
flashcard(
"Name the four standard fetal biometric parameters and their measurement planes.",
[
{ key: "BPD (Biparietal Diameter)", value: "Transventricular axial plane; outer-to-inner" },
{ key: "HC (Head Circumference)", value: "Same plane as BPD; ellipse method" },
{ key: "AC (Abdominal Circumference)", value: "Transverse plane at level of portal vein sinus & stomach" },
{ key: "FL (Femur Length)", value: "Long axis of femur diaphysis; ossified shaft only" },
"EFW = derived from HC + AC + FL (Hadlock formula)",
"AC is most sensitive for IUGR (reflects fetal liver glycogen stores)"
],
"Most sensitive parameter for IUGR = AC (abdominal circumference)"
);
flashcard(
"What defines fetal growth restriction (FGR) on ultrasound?",
[
{ key: "Definition", value: "EFW or AC <10th percentile for gestational age" },
{ key: "Severe FGR", value: "EFW <3rd percentile" },
"Serial growth scans every 3–4 weeks in high-risk pregnancy",
"Most sensitive single marker: AC (reflects liver size / glycogen stores)",
"Asymmetric FGR (head sparing): head growth maintained; AC falls first",
"Symmetric FGR: all parameters equally reduced (early onset / chromosomal)"
],
"Asymmetric FGR = uteroplacental insufficiency (AC↓ first). Symmetric FGR = chromosomal or early-onset"
);
flashcard(
"Gestational age dating accuracy by trimester – what are the error margins?",
[
{ key: "1st trimester (CRL)", value: "±5–7 days (most accurate)" },
{ key: "2nd trimester (18–22 wks)", value: "±10–14 days" },
{ key: "3rd trimester (>28 wks)", value: "±21–28 days (least accurate)" },
"Never change EDD established by early ultrasound using later scans",
"EDD based on 1st trimester CRL supersedes LMP if they differ by >7 days (before 10 wks)"
],
"1st trimester CRL = most accurate dating (±5 days). 3rd trimester USG = ±3 weeks"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 8 – DOPPLER
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 8", "Doppler Ultrasound in Pregnancy");
flashcard(
"What are the three key Doppler indices and their formulas?",
[
{ key: "S/D ratio", value: "Peak systolic velocity ÷ End-diastolic velocity" },
{ key: "Resistance Index (RI)", value: "(S − D) ÷ S" },
{ key: "Pulsatility Index (PI)", value: "(S − D) ÷ mean velocity (most comprehensive)" },
"All three decrease through normal pregnancy as placental resistance falls",
"PI is preferred in research; S/D ratio widely used clinically"
],
"PI is NOT affected by absent/reversed diastolic flow (unlike S/D ratio which → infinity)"
);
flashcard(
"Describe the progressive Doppler abnormalities in umbilical artery and their clinical significance.",
[
{ header: "Umbilical Artery Doppler – Progressive Worsening" },
{ key: "1. Elevated S/D ratio", value: "Increased placental resistance → early IUGR" },
{ key: "2. Absent End-Diastolic Flow (AEDF)", value: "Severe placental insufficiency; ~70% of chorionic villi obliterated" },
{ key: "3. Reversed End-Diastolic Flow (REDF)", value: "Critical – fetal pH likely acidotic; expedite delivery" },
"Normal: S/D falls progressively through pregnancy (diastolic flow increases)",
"Correlates strongly with IUGR and adverse neonatal outcomes"
],
"REDF = imminent fetal danger → consider immediate delivery regardless of gestational age"
);
flashcard(
"What is the clinical significance of Middle Cerebral Artery (MCA) Doppler?",
[
{ key: "Normal MCA", value: "LOW resistance (brain needs continuous high flow)" },
{ key: "Brain-sparing (IUGR)", value: "MCA PI falls (cerebrovascular vasodilation) as compensation" },
{ key: "MCA PSV >1.5 MoM", value: "Significant fetal anaemia (sensitivity ~88%)" },
"MCA PSV >1.5 MoM has replaced amniocentesis for monitoring rhesus disease",
"Cerebroplacental ratio (CPR) = MCA PI ÷ UA PI; CPR <1.0 = brain-sparing"
],
"MCA PSV >1.5 MoM → fetal anaemia. Seen in Rh isoimmunisation, parvovirus B19 infection"
);
flashcard(
"What is the significance of ductus venosus and uterine artery Doppler?",
[
{ header: "DUCTUS VENOSUS" },
"Reflects fetal cardiac preload / right heart function",
{ key: "Absent or reversed A-wave", value: "Imminent fetal cardiac decompensation" },
"Used in combination with BPP for preterm IUGR surveillance",
{ header: "UTERINE ARTERY" },
"Assessed at 20–24 weeks for preeclampsia / IUGR prediction",
{ key: "Persistent bilateral notching + elevated PI", value: "High risk for preeclampsia & placental insufficiency" }
],
"Reversed DV A-wave = worst Doppler sign → imminent fetal death, delivery indicated"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 9 – SOFT MARKERS
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 9", "Second Trimester Soft Markers of Aneuploidy");
flashcard(
"List the second trimester ultrasound soft markers and their aneuploidy associations.",
[
{ key: "Nuchal fold ≥6 mm (16–20 wks)", value: "Trisomy 21 (strongest marker)" },
{ key: "Echogenic bowel", value: "Trisomy 21, cystic fibrosis, CMV, IUGR" },
{ key: "Echogenic intracardiac focus (EIF)", value: "Trisomy 21 (minor – isolated EIF in low-risk: reassure)" },
{ key: "Short femur / short humerus", value: "Trisomy 21" },
{ key: "Choroid plexus cysts (CPCs)", value: "Trisomy 18 (especially with other markers)" },
{ key: "Renal pyelectasis (>4 mm)", value: "Trisomy 21" },
{ key: "Single umbilical artery", value: "Trisomy 18, structural anomalies" },
{ key: "Absent / hypoplastic nasal bone", value: "Trisomy 21" }
],
"Nuchal fold ≥6 mm at 16–20 wks = STRONGEST 2nd trimester soft marker for T21"
);
flashcard(
"How do isolated soft markers change aneuploidy risk management?",
[
"Multiple soft markers: risk is multiplicative – offer invasive testing",
"Single isolated minor marker (EIF, mild pyelectasis) in low-risk patient: does NOT require amniocentesis",
"Nuchal fold ≥6 mm: significant even in isolation – offer genetic counselling",
"CPCs with trisomy 18 features: hands (clenched/overlapping fingers), rocker-bottom foot, cardiac defect",
"Integrated sequential screening uses soft markers + serum markers + NT for final risk"
],
"Isolated EIF in low-risk patient – reassure. Multiple markers – offer amniocentesis"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 10 – CERVICAL LENGTH
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 10", "Cervical Ultrasound");
flashcard(
"What is the role of cervical length ultrasound in predicting preterm birth?",
[
{ key: "Method", value: "Transvaginal ultrasound (TVS) – gold standard" },
{ key: "Normal CL", value: "≥25 mm at 16–24 weeks" },
{ key: "Short cervix", value: "<25 mm – strongest predictor of spontaneous PTB" },
{ key: "Very short cervix", value: "<15 mm – very high risk" },
"Short CL + fFN (fetal fibronectin) positive = highest risk combination",
"Progesterone therapy indicated for short cervix in singleton pregnancy",
"Cerclage indicated in history of preterm birth + short cervix"
],
"CL <25 mm at 16–24 wks → offer vaginal progesterone (17-OHPC or micronised)"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 11 – THIRD TRIMESTER & BPP
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 11", "Third Trimester Ultrasound & BPP");
flashcard(
"What are the main indications for third trimester ultrasound?",
[
"Serial fetal growth monitoring (IUGR, macrosomia)",
"Fetal presentation (cephalic / breech / transverse) – ECV counselling before 36 wks",
"Placental localisation (re-assess previa at 32–36 wks)",
"Amniotic fluid assessment (post-dates, IUGR, PROM)",
"Biophysical profile (BPP) for fetal wellbeing",
"Doppler assessment in high-risk (IUGR, PET, Rh disease)",
"Evaluate for placenta accreta spectrum if previa present"
],
"Placenta previa found at 20 wks: 90% will migrate away from os by 36 wks (especially if posterior)"
);
flashcard(
"Describe the 5 components of the Biophysical Profile (BPP) and scoring.",
[
{ header: "Each parameter: 2 = present, 0 = absent (max 10/10)" },
{ key: "1. Fetal movement", value: "≥3 discrete body/limb movements in 30 min" },
{ key: "2. Fetal tone", value: "≥1 episode of extension + return to flexion (hand open/close counts)" },
{ key: "3. Fetal breathing", value: "≥1 episode of breathing ≥30 sec in 30 min" },
{ key: "4. Amniotic fluid", value: "MVP ≥2 cm in ≥1 pocket" },
{ key: "5. Non-stress test (NST)", value: "Reactive = ≥2 accelerations in 20 min" }
],
"BPP 8–10 = normal; 6 = equivocal (repeat in 24h); ≤4 = abnormal → consider delivery"
);
flashcard(
"Interpret BPP scores and their management.",
[
{ key: "10/10 or 8/10 (normal AFV)", value: "Reassuring – routine management" },
{ key: "8/10 (abnormal AFV)", value: "Deliver if ≥36 wks; consider early delivery" },
{ key: "6/10", value: "Equivocal – repeat in 24 hours; deliver if ≥36 wks or mature lungs" },
{ key: "4/10", value: "Strongly consider immediate delivery" },
{ key: "2/10 or 0/10", value: "Deliver immediately (acute fetal distress)" },
"Modified BPP = NST + AFI (widely used in US practice)",
"Acute markers: movement, tone, breathing (reflect CNS function at time of scan)",
"Chronic marker: AFI (reflects placental function over days)"
],
"BPP ≤4/10 = deliver immediately regardless of gestational age (if viable)"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 12 – ADVANCED TECHNIQUES
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 12", "Advanced Techniques");
flashcard(
"What are the uses and limitations of 3D/4D ultrasound in pregnancy?",
[
{ header: "3D ULTRASOUND" },
"Better surface anatomy: cleft lip/palate, skeletal dysplasias",
"More accurate volume measurements (e.g., nuchal volume)",
"Limitations: image quality limited by fetal position and AFV",
{ header: "4D ULTRASOUND (real-time 3D)" },
"Fetal behaviour and facial expressions",
"Cardiac morphology (spatiotemporal image correlation – STIC)",
"NOT superior to 2D for routine anomaly screening"
],
null
);
flashcard(
"What is vasa previa and how is it detected on ultrasound?",
[
{ key: "Definition", value: "Fetal vessels (umbilical or velamentous) overlying the internal cervical os" },
"Detected with: colour Doppler + transvaginal ultrasound",
{ key: "Risk", value: "Vessel rupture with membrane rupture → fetal exsanguination (mortality ~60% if undiagnosed)" },
"Associations: low-lying placenta, velamentous cord insertion, bilobed/succenturiate placenta",
"Management: elective CS at 35–37 weeks, hospitalisation from 32 wks"
],
"Vasa previa = fetal vessels over os → painless PV bleeding at ROM = fetal emergency"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 13 – SCANNING SCHEDULE
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 13", "Recommended Ultrasound Schedule in Pregnancy");
flashcard(
"What is the recommended ultrasound schedule throughout pregnancy?",
[
{ key: "6–9 wks", value: "Confirm IUP, viability, number, CRL dating, ectopic exclusion" },
{ key: "11–14 wks", value: "NT + nasal bone + aneuploidy screening + fetal survey" },
{ key: "18–22 wks", value: "Anatomy scan (CPT 76805) – biometry, anomalies, placenta, AFV" },
{ key: "22–24 wks", value: "Uterine artery Doppler (PET risk), cervical length (PTB risk)" },
{ key: "28–32 wks", value: "Fetal growth, presentation" },
{ key: "34–36 wks", value: "Presentation, placenta migration, AFV, BPP/Doppler if indicated" }
],
"In LOW RISK pregnancy: minimum 2 scans (dating at 11–14 wks + anatomy at 18–22 wks)"
);
// ══════════════════════════════════════════════════════════════════════════════
// SECTION 14 – HIGH-YIELD EXAM POINTS
// ══════════════════════════════════════════════════════════════════════════════
sectionDivider("SECTION 14", "High-Yield Exam Points");
flashcard(
"What are the HIGH-YIELD number-based facts for the final exam?",
[
{ key: "NT measurement window", value: "CRL 45–84 mm (11–14 weeks)" },
{ key: "NT clinical significance threshold", value: "≥3.5 mm warrants karyotyping" },
{ key: "Lateral ventricle width (normal)", value: "≤10 mm" },
{ key: "Cisterna magna (normal)", value: "2–10 mm" },
{ key: "Placenta previa threshold (TVS)", value: "Placental edge <2 cm from internal os" },
{ key: "Normal AFI", value: "8–25 cm; oligohydramnios <5 cm; polyhydramnios >25 cm" },
{ key: "Normal MVP", value: "2–8 cm" },
{ key: "Cervical length (short)", value: "<25 mm at 16–24 weeks" },
{ key: "MCA PSV threshold (anaemia)", value: ">1.5 MoM" },
{ key: "Nuchal fold ≥6 mm", value: "At 16–20 weeks (T21 soft marker)" }
],
null
);
flashcard(
"What are the key MNEMONICS and diagnostic clues to remember?",
[
{ key: "Lemon sign + Banana sign", value: "Spina bifida (neural tube defect)" },
{ key: "Double bubble", value: "Duodenal atresia (T21 association)" },
{ key: "Snowstorm appearance", value: "Hydatidiform mole" },
{ key: "T-sign (1st tri)", value: "Monochorionic twins" },
{ key: "Lambda/Twin-peak sign", value: "Dichorionic twins" },
{ key: "Brain-sparing", value: "MCA PI↓ + UA PI↑ = IUGR compensation" },
{ key: "AEDF/REDF", value: "Absent/Reversed end-diastolic flow → imminent fetal compromise" },
{ key: "Absent nasal bone", value: "87× risk for Down syndrome" }
],
"Lemon + Banana signs = Open spina bifida (Arnold-Chiari II malformation)"
);
flashcard(
"What Doppler findings indicate the most serious fetal compromise and what is the management?",
[
{ header: "MOST CRITICAL SIGNS (in order of severity)" },
{ key: "1. Elevated UA S/D ratio", value: "Watch + serial Doppler every 1–2 wks" },
{ key: "2. Absent end-diastolic flow (AEDF)", value: "Admit + steroids + daily Doppler; deliver at 34 wks" },
{ key: "3. Reversed end-diastolic flow (REDF)", value: "Deliver immediately if viable (>24 wks)" },
{ key: "4. Absent/reversed DV A-wave", value: "Imminent cardiac failure → deliver IMMEDIATELY" },
"MCA PSV >1.5 MoM → intrauterine transfusion (IUT) if <34 wks"
],
"REDF + reversed DV A-wave = DO NOT DELAY delivery (perinatal mortality very high)"
);
// ══════════════════════════════════════════════════════════════════════════════
// BACK COVER
// ══════════════════════════════════════════════════════════════════════════════
const back = pres.addSlide();
back.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: "0A1045" } });
back.addText("🎯 ALL DONE!", {
x: 0.5, y: 1.0, w: 9, h: 1.0,
fontSize: 40, bold: true, color: "FFFFFF", align: "center", fontFace: "Calibri"
});
back.addText(`Total Cards: ${cardNum} · 14 Sections`, {
x: 0.5, y: 2.1, w: 9, h: 0.6,
fontSize: 20, color: "90CAF9", align: "center", fontFace: "Calibri"
});
back.addText("Review daily. Cover the answer side first. Good luck in your finals!", {
x: 1.0, y: 2.9, w: 8, h: 0.8,
fontSize: 15, color: "B3E5FC", align: "center", fontFace: "Calibri", italic: true
});
back.addText("Source: Creasy & Resnik's Maternal-Fetal Medicine | Orris AI", {
x: 0.5, y: 5.1, w: 9, h: 0.35,
fontSize: 10, color: "5C6BC0", align: "center", fontFace: "Calibri"
});
// ══════════════════════════════════════════════════════════════════════════════
// SAVE
// ══════════════════════════════════════════════════════════════════════════════
pres.writeFile({ fileName: "/home/daytona/workspace/usg-flashcards/USG_Pregnancy_Flashcards.pptx" })
.then(() => console.log("✅ Done! Cards:", cardNum))
.catch(e => { console.error(e); process.exit(1); });
Running Command
cd /home/daytona/workspace/usg-flashcards && node make_flashcards.js
Your flashcard deck is ready!
USG Pregnancy Flashcards
Presentation · PPTX
What's inside - 37 flashcards across 14 sections:
Each card has a Question slide (deep navy) followed by an Answer slide (white) with a green exam tip at the bottom where relevant.
| Section | Topic | Cards |
|---|---|---|
| 1 | Principles & Physics | 3 |
| 2 | Types of Examinations | 2 |
| 3 | First Trimester | 3 |
| 4 | Nuchal Translucency | 3 |
| 5 | Nasal Bone | 2 |
| 6 | Anatomy Scan (Head, Thorax, Abdomen, Spine, Placenta) | 5 |
| 7 | Fetal Biometry & Growth | 3 |
| 8 | Doppler Ultrasound | 4 |
| 9 | Soft Markers of Aneuploidy | 2 |
| 10 | Cervical Length | 1 |
| 11 | Third Trimester & BPP | 3 |
| 12 | Advanced Techniques (3D/4D, Vasa Previa) | 2 |
| 13 | Scanning Schedule | 1 |
| 14 | High-Yield Exam Points & Mnemonics | 3 |
How to use: Open in PowerPoint or Google Slides. Read the question slide, think of your answer, then advance to the answer slide to check. All critical exam numbers (NT 45-84 mm, AFI <5 = oligo, MCA >1.5 MoM, etc.) are highlighted in blue. Green boxes = examiner favourite points.
This is a shared conversation. Sign in to Orris to start your own chat.