Empyema thoracis 6 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the material needed for a thorough 6-mark answer. Here is the complete response:
Empyema Thoracis
Definition
Empyema thoracis is the collection of purulent fluid (pus) within the pleural space, resulting from invasion by pyogenic bacteria, fungi, parasites, or mycobacteria. Pathologically, it requires the presence of thick pus with a thick cortex of fibrin and coagulum overlying the lung.
- Bailey & Love's Short Practice of Surgery, 28th Ed., p. 5534
- Sabiston Textbook of Surgery, p. 2287
Etiology / Predisposing Conditions
| Category | Examples |
|---|---|
| Pulmonary infection | Pneumonia (most common), lung abscess, bronchiectasis, TB |
| Aspiration of pleural effusion | Any aetiology |
| Trauma | Penetrating injury, haemothorax infection |
| Surgery | Post-thoracic surgery, bronchopleural fistula |
| Extrapulmonary | Subphrenic abscess, oesophageal perforation/rupture |
| Bone infection | Osteomyelitis of ribs or vertebrae |
- Bailey & Love's, Table 60.3
Microbiology
-
Community-acquired: Streptococcus milleri, Haemophilus influenzae (especially children), Streptococcus pneumoniae (now only 5-10% of cases), anaerobes (25-40%)
-
Hospital-acquired / post-surgical: S. aureus, Gram-negative organisms (Pseudomonas, Klebsiella, E. coli), MRSA
-
Anaerobes (Fusobacterium nucleatum, Prevotella spp., Peptostreptococcus, Bacteroides fragilis) account for up to 76% in some series - often related to aspiration
-
Immunocompromised: Gram-negative bacteria, Aspergillus, other fungi
-
Fishman's Pulmonary Diseases, pp. 2246-2248
Pathological Stages (Three Phases)
Phase 1 - Exudative (Acute)
- Protein-rich (>30 g/L), free-flowing serous or serosanguineous fluid
- Low cell count, pH >7.3, normal glucose
- Sterile; may resolve with antibiotics alone ± aspiration
Phase 2 - Fibrinopurulent (Transitional)
- Fluid thickens; fibrin strands form loculations
- Bacteria invade; neutrophils accumulate (>25,000 WBC/mL)
- pH 7.0-7.3, falling glucose
- Drainage essential; antibiotics alone insufficient
Phase 3 - Organizing (Chronic)
-
Lung "trapped" by thick fibrinous peel (cortex)
-
pH <7.0, very low glucose, high LDH
-
Surgical management (decortication) usually required
-
Bailey & Love's, p. 5545-5551; Fishman's, p. 2250
Clinical Features
Symptoms:
- Fever, rigors, malaise, weight loss, loss of appetite
- Pleuritic chest pain (sharp, worsens on breathing)
- Dyspnoea (from compressive effusion)
- Cough (often productive if co-existing pneumonia)
Signs:
- Reduced chest expansion on affected side
- Stony dull percussion note
- Diminished or absent breath sounds
- Tracheal and mediastinal shift away from the effusion (if large)
- Clubbing in chronic cases
Investigations
Bloods: Raised WBC, elevated CRP/ESR, blood cultures
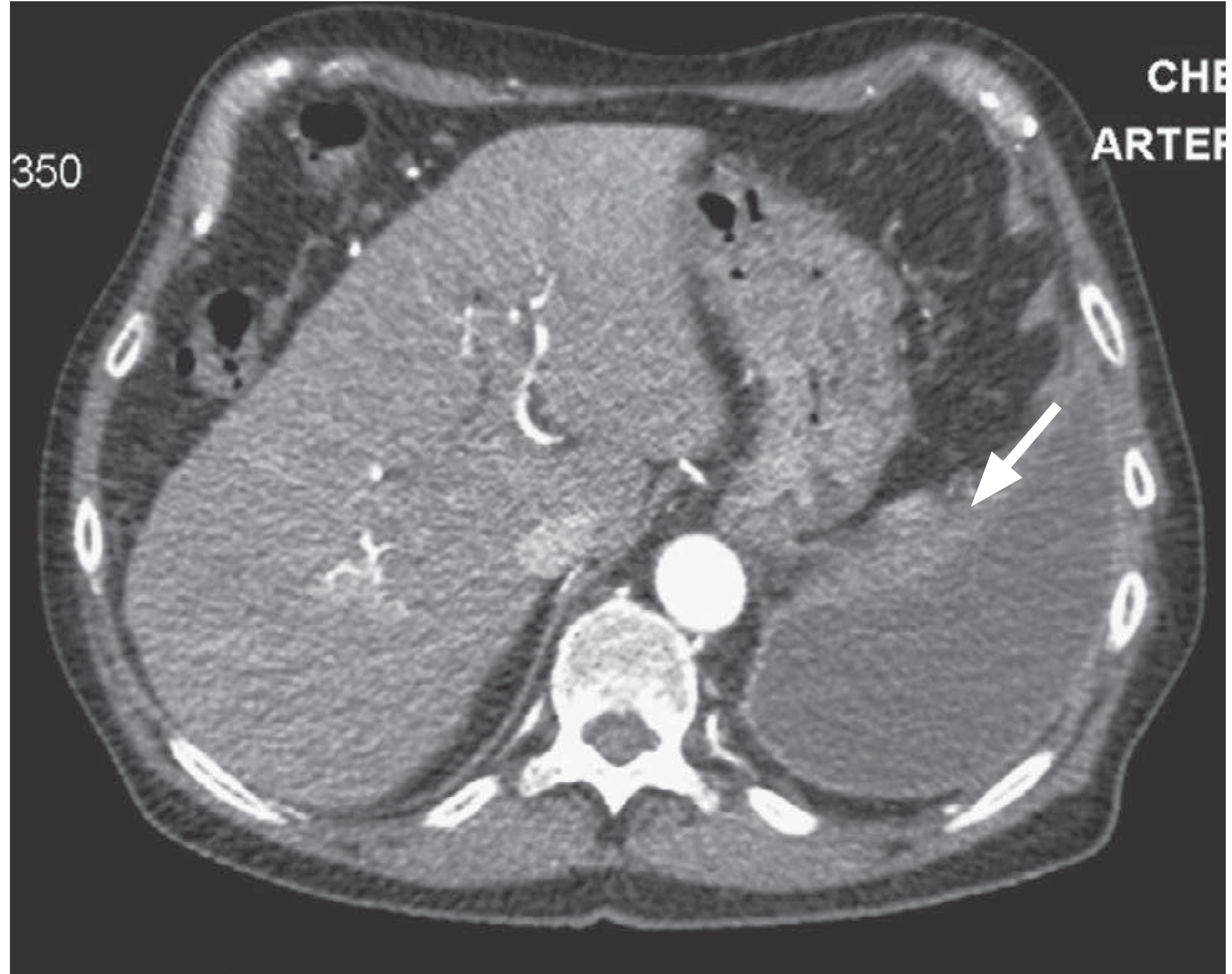
Imaging:
- CXR: Opacification of hemithorax, often with meniscus sign; mediastinal shift
- CT chest: Gold standard - confirms loculation, measures peel thickness, identifies underlying cause (see image below)
- Ultrasound: Guides safe drainage, identifies echogenic/loculated fluid
Pleural fluid analysis (diagnostic thoracentesis):
| Parameter | Empyema |
|---|---|
| Appearance | Purulent/turbid |
| WBC | >25,000/mL (neutrophil predominance); frank pus >100,000/mL |
| pH | <7.2 (frank empyema) |
| Glucose | Low (<50% serum) |
| LDH | Very high |
| Gram stain/culture | Positive in ~60% |
- Fishman's, pp. 2249-2250; Quick Compendium of Clinical Pathology
Treatment
Treatment requires drainage + antibiotics, tailored to disease stage.
1. Antibiotics
- Started empirically; guided by culture/sensitivities
- Cover anaerobes (metronidazole), Gram-positives, and Gram-negatives based on clinical context
- Intrapleural antibiotics are NOT recommended (irritating, ineffective)
2. Drainage
Phase 1 (exudative):
- Serial needle aspiration (thoracentesis) if pH >7.3
- Small-bore pigtail catheter or chest tube sufficient
Phase 2 (fibrinopurulent):
- Chest tube drainage (intercostal drain) is the mainstay
- Intrapleural fibrinolytics: Combined tPA + DNase (two-agent) instilled through the chest tube breaks down loculations and reduces the need for surgery
- Chest tube removal when drainage <100-200 mL/day and imaging confirms resolution
Phase 3 (organizing):
-
VATS (Video-Assisted Thoracoscopic Surgery): Surgical debridement, disruption of loculations, creation of a single cavity, dependent drainage - preferred for early fibrinopurulent/organizing stage
-
Decortication (thoracotomy): Removes the fibrous cortex/peel entrapping the lung; allows full re-expansion; usually posterolateral thoracotomy - reserved for chronic trapped lung
-
Open drainage (Eloesser flap): Rib resection + pleurocutaneous fistula in high-risk surgical patients
-
Bailey & Love's, pp. 5590-5616; Fishman's, pp. 2250-2251; Sabiston, p. 2300
Complications
- Bronchopleural fistula - communication between bronchial tree and pleural space
- Trapped/restricted lung - fibrous encasement preventing expansion
- Empyema necessitans - spontaneous external rupture through chest wall (rare; classically TB)
- Pyopneumothorax - pus + air in pleural space
- Septicaemia / metastatic infection
- Respiratory failure
- Chronic pleural fibrosis with restrictive physiology
Summary
Empyema thoracis progresses through three distinct stages: exudative → fibrinopurulent → organizing. Early recognition and drainage (guided by pleural fluid analysis - especially pH) is key to preventing chronic trapped lung. Management is stage-dependent: antibiotics ± aspiration in phase 1; chest tube + tPA/DNase in phase 2; VATS debridement or decortication in phase 3.
- Bailey & Love's Short Practice of Surgery, 28th Ed.
- Fishman's Pulmonary Diseases and Disorders
- Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.