Hyponatremia
Reading File
Finding Sources
Searching PubMed
"hyponatremia"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer. Let me compile it.
Hyponatremia
Serum [Na+] < 135 mEq/L - the most common electrolyte disorder in clinical practice.
Definition and Classification by Severity
| Level | Serum Na+ |
|---|---|
| Mild | 130-134 mEq/L |
| Moderate | 125-129 mEq/L |
| Severe | < 125 mEq/L |
| Critical (emergent) | ≤ 110-120 mEq/L |
Step 1: Check Plasma Osmolality First
The diagnostic approach begins with plasma osmolality to differentiate true hypotonic hyponatremia from mimics:
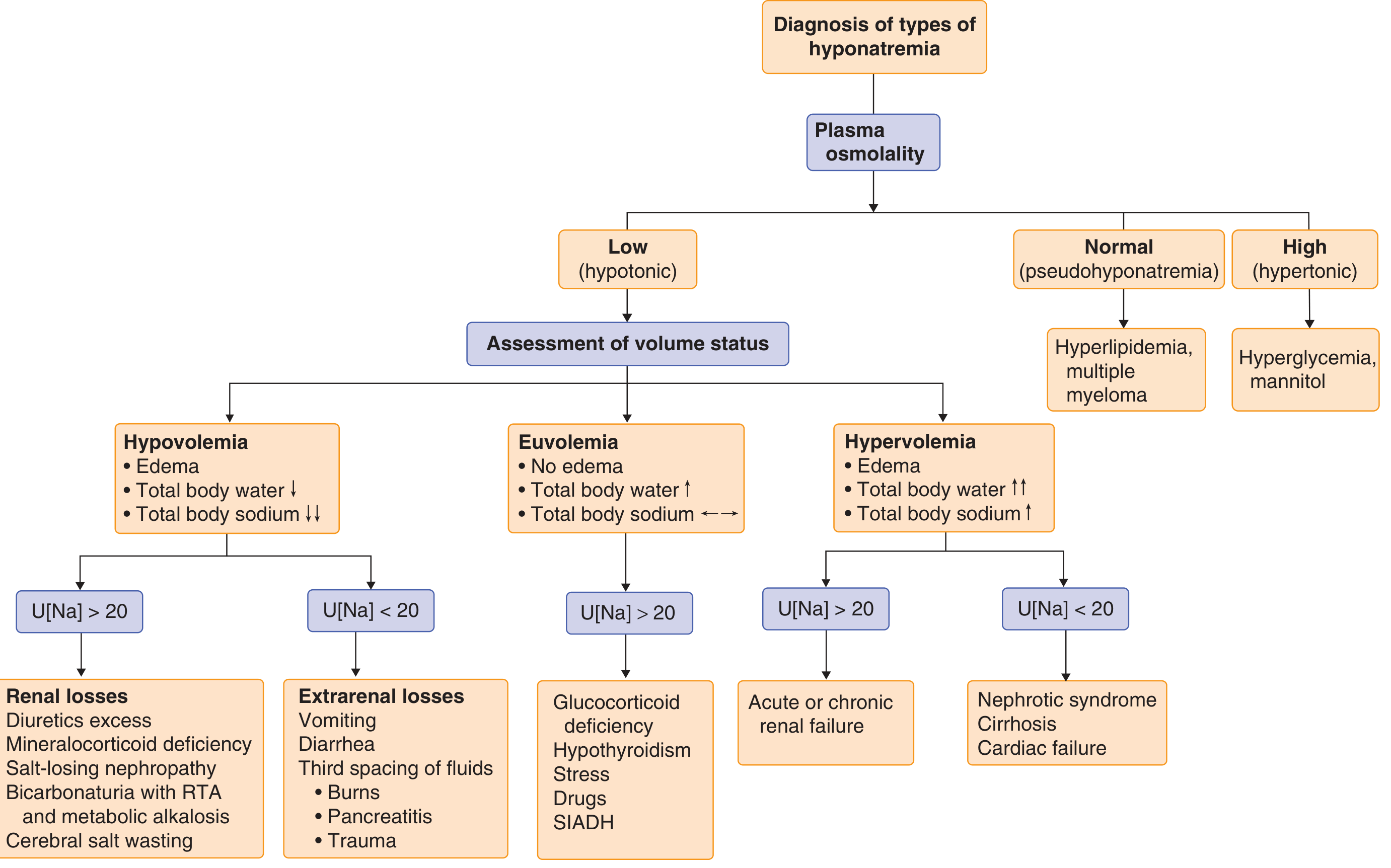
- Normal osmolality (Posm 280-295) → Pseudohyponatremia (hyperlipidemia, multiple myeloma, hyperproteinemia) - no water shift, lab artifact
- High osmolality (Posm >295) → Hypertonic hyponatremia - hyperglycemia, mannitol causing osmotic water shift into plasma
- Low osmolality (Posm <280) → True hypotonic hyponatremia - proceed to volume assessment
For hyperglycemia correction: add 1.6 mEq/L to the measured sodium for every 100 mg/dL glucose above 100 (some use 2.4 mEq/L for glucose >500).
Step 2: Classify by Volume Status
Once true hypotonic hyponatremia is confirmed, assess volume status clinically and with urine sodium (U[Na]) and urine osmolality.
Hypovolemic Hyponatremia
- Total body water ↓, Total body sodium ↓↓ (Na loss > water loss)
- U[Na] < 20 → Extrarenal losses: vomiting, diarrhea, sweating, GI suction, third-spacing (burns, pancreatitis, bowel obstruction)
- U[Na] > 20 → Renal losses: thiazide diuretics, mineralocorticoid deficiency, salt-losing nephropathy, RTA, cerebral salt wasting
Hypervolemic Hyponatremia
- Total body water ↑↑, Total body sodium ↑ (water excess > sodium excess), edema present
- U[Na] < 20 → Heart failure, cirrhosis, nephrotic syndrome (renal hypoperfusion triggers ADH and aldosterone)
- U[Na] > 20 → Acute or chronic renal failure
Euvolemic Hyponatremia
- Total body water ↑, Total body sodium normal (pure water retention), no edema
- U[Na] > 40, Uosm > 100 → SIADH (most common), hypothyroidism, adrenal (glucocorticoid) insufficiency, stress
- Very low Uosm → Psychogenic polydipsia, beer potomania, reset osmostat
SIADH - The Most Common Euvolemic Cause
Diagnostic criteria:
- Hypotonic hyponatremia (Posm < 275 mOsm/kg)
- Inappropriately concentrated urine (Uosm usually > 200, often > 100 mOsm/kg)
- Urine Na+ typically > 20-40 mEq/L (often > 100)
- Clinical euvolemia
- Normal adrenal, renal, cardiac, hepatic, and thyroid function
Common causes of SIADH:
| Category | Examples |
|---|---|
| CNS disorders | Meningitis, encephalitis, stroke, subdural hemorrhage, TBI, brain tumors, Guillain-Barre |
| Pulmonary | TB, lung abscess, empyema, acute respiratory failure |
| Malignancy (ectopic ADH) | Small cell lung cancer (10-15%), head/neck tumors, pancreas, lymphoma |
| Drugs | SSRIs/SNRIs, carbamazepine, cyclophosphamide, vincristine, opioids, haloperidol, amiodarone, desmopressin, MDMA |
| Other | Postoperative state, exercise-associated hyponatremia |
Symptoms
Symptoms depend on both the degree and rate of development of hyponatremia:
- Mild: Nausea, malaise, headache, lethargy
- Moderate: Confusion, disorientation, personality change
- Severe: Seizures, obtundation, coma, respiratory arrest, death
Acute hyponatremia (developing over <24-48 hours) is far more symptomatic at any given sodium level than chronic hyponatremia, because the brain has not had time to compensate via volume regulation (loss of intracellular osmoles).
Treatment
Key Principle: Rate of Correction Matters Critically
Two opposing dangers:
- Too slow correction → persistent cerebral edema, brain herniation, death
- Too fast correction → Osmotic Demyelination Syndrome (ODS), formerly "central pontine myelinolysis"
ODS is caused by rapid correction (>12 mEq/L/24h) causing water to shift OUT of neurons, leading to diffuse demyelination. It presents days later with: flaccid paralysis, pseudobulbar palsy, dysarthria, dysphagia, ataxia, fluctuating consciousness, and characteristic MRI signal changes in the brainstem. It is often irreversible and can be fatal.
Risk factors for ODS: Serum Na+ < 105 mmol/L, hypokalemia, alcohol use disorder, malnutrition, advanced liver disease.
Acute Symptomatic Hyponatremia (duration < 24-48 h, OR seizing/comatose)
Goal: Rapid correction by 4-6 mmol/L to relieve cerebral edema and prevent herniation.
- Severe symptoms (seizure, coma): 100 mL 3% NaCl IV over 10 minutes - repeat up to 2 more times as needed
- Mild-moderate symptoms: 3% NaCl at 0.5-2 mL/kg/hour
- Rate of correction is not restricted in true acute hyponatremia
- If duration uncertain, treat as chronic
Recent meta-analysis (JAMA Intern Med, 2025 - PMID 39556338) examined correction rates and outcomes in hospitalized adults with severe hyponatremia, and a 2025 systematic review (PMID 40053429) confirmed the safety profile of rapid intermittent bolus (100 mL × 3) vs continuous infusion for symptomatic severe hyponatremia.
Chronic Hyponatremia (duration > 24-48 h, or unknown duration)
Correction rate limits:
- Standard risk: Do not exceed 10-12 mmol/L in 24h or 18 mmol/L in 48h
- High risk of ODS (Na+ < 120 for >48h, alcoholism, malnutrition, liver disease): Do not exceed 8 mmol/L in 24h; aim for 4-6 mmol/L/day
If overcorrection occurs:
- Starting Na+ ≥ 120: observation usually sufficient
- Starting Na+ < 120: actively re-lower sodium with hypotonic fluids (free water or 0.45% NaCl) ± vasopressin analogue (desmopressin)
Treatment by Cause
| Volume Status | Treatment |
|---|---|
| Hypovolemic | Isotonic saline (0.9% NaCl) to restore volume - ADH will be suppressed as volume recovers, watch for rapid auto-correction |
| Hypervolemic (HF, cirrhosis, CKD) | Fluid restriction + treat underlying cause; loop diuretics; vaptans (tolvaptan) in selected cases |
| Euvolemic / SIADH | Fluid restriction (500 mL below urine output); salt tablets; demeclocycline; vaptans (tolvaptan, conivaptan); urea (oral) |
Vaptans (vasopressin V2 receptor antagonists) - tolvaptan, conivaptan - cause aquaresis (electrolyte-free water excretion) and are effective in SIADH and hypervolemic hyponatremia. Tolvaptan carries an FDA warning for liver toxicity in cirrhosis. A 2025 meta-analysis (PMID 39362395) confirmed oral urea as an effective and inexpensive alternative for SIADH-associated hyponatremia.
Special Populations
- Postoperative: Women of reproductive age are at disproportionate risk for fatal hyponatremic encephalopathy - rapid correction is warranted
- Exercise-associated: Induced by excessive hypotonic fluid intake; treat with hypertonic saline even without symptoms if Na+ is dropping rapidly
- Psychogenic polydipsia / beer potomania: Very dilute urine (Uosm very low); fluid restriction is first-line
- Cancer patients: Hyponatremia doubles hospital length of stay and increases 90-day mortality 3-5 fold; associated with SIADH from malignancy or chemotherapy (cyclophosphamide, cisplatin, vincristine, vinblastine)
Quick Reference: Urine Labs in Hyponatremia
| Cause | Urine Na | Urine Osm |
|---|---|---|
| SIADH | > 40 | > 200 (often > 300) |
| Hypovolemia (extrarenal) | < 20 | > 500 |
| Hypovolemia (renal, diuretics) | > 20 | Variable |
| HF / cirrhosis | < 20 | > 100 |
| Psychogenic polydipsia | < 20 | < 100 |
| Beer potomania | < 20 | < 100 |
Sources: Goldman-Cecil Medicine (9780323930345), Rosen's Emergency Medicine (9780323757898), Tintinalli's Emergency Medicine (9781260019933), Brenner and Rector's The Kidney (9780323532655). Recent meta-analyses: JAMA Intern Med 2025 (correction rates), Ann Afr Med 2025 (bolus vs infusion hypertonic saline), Am J Kidney Dis 2025 (urea for SIADH).
This is a shared conversation. Sign in to Orris to start your own chat.