Acute onset painless vision loss detailed information
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Searching PubMed
acute painless vision loss retinal artery occlusion management
I now have comprehensive information from multiple authoritative sources. Let me compile a thorough, well-organized response.
Acute Onset Painless Vision Loss
Acute painless vision loss is a true ophthalmic and neurological emergency. The absence of pain is the key clinical discriminator - it immediately shifts the differential toward vascular, retinal, or posterior pathway causes rather than inflammatory or pressure-related ones.
Classification: Monocular vs. Binocular
| Type | Location of Pathology | Examples |
|---|---|---|
| Monocular | Eye, optic nerve (anterior to chiasm) | CRAO, CRVO, AION, vitreous hemorrhage, retinal detachment |
| Binocular | Chiasm or posterior to it | Occipital stroke, basilar artery territory infarction, homonymous hemianopia |
A sudden complete bilateral blindness most often indicates basilar artery territory infarction of both occipital lobes. A sudden homonymous hemianopia results from infarction of the temporal, parietal, or occipital lobes. - Rosen's Emergency Medicine, 10e
Causes and Differential Diagnosis
1. Central Retinal Artery Occlusion (CRAO)
Definition: Embolic, thrombotic, vasculitic, or vasospastic occlusion of the central retinal artery, causing acute retinal ischemia.
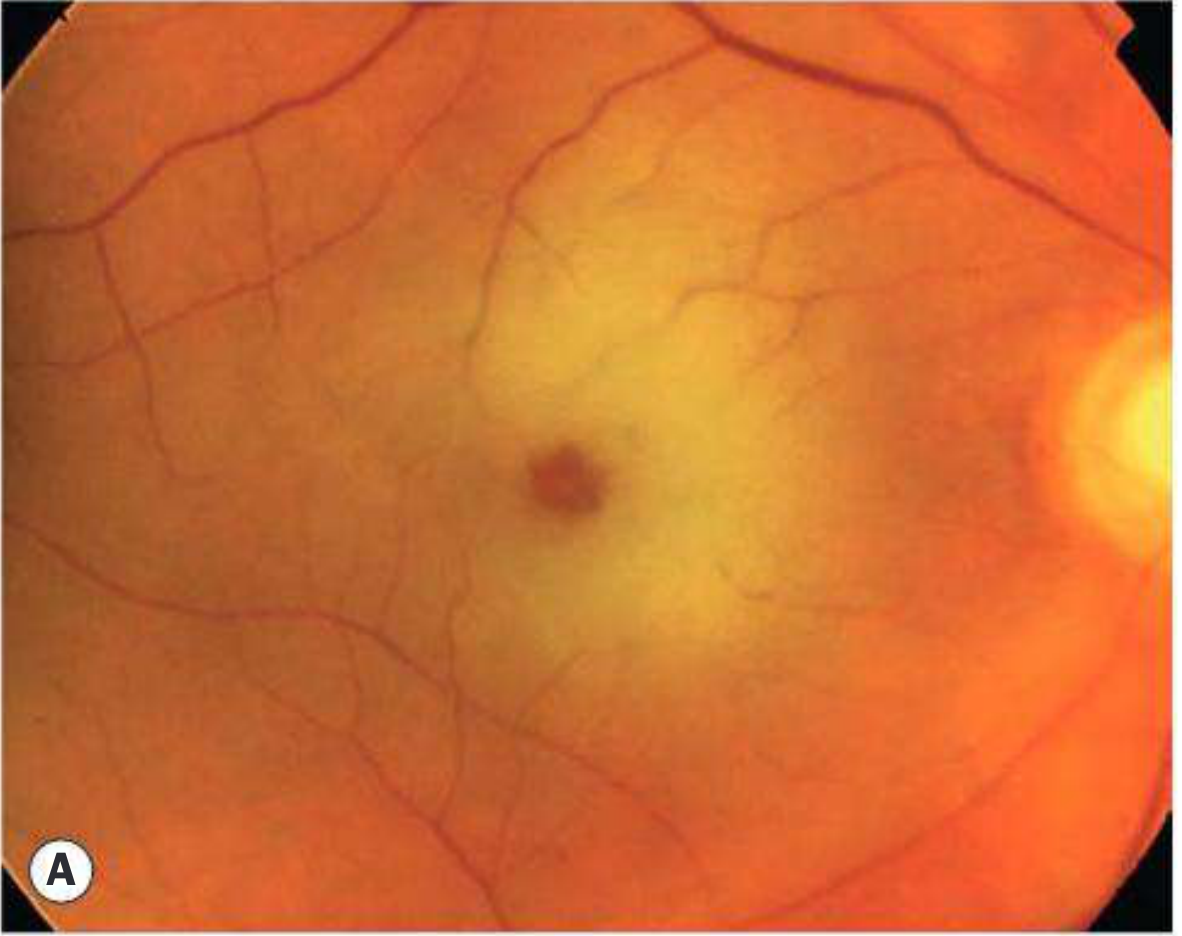
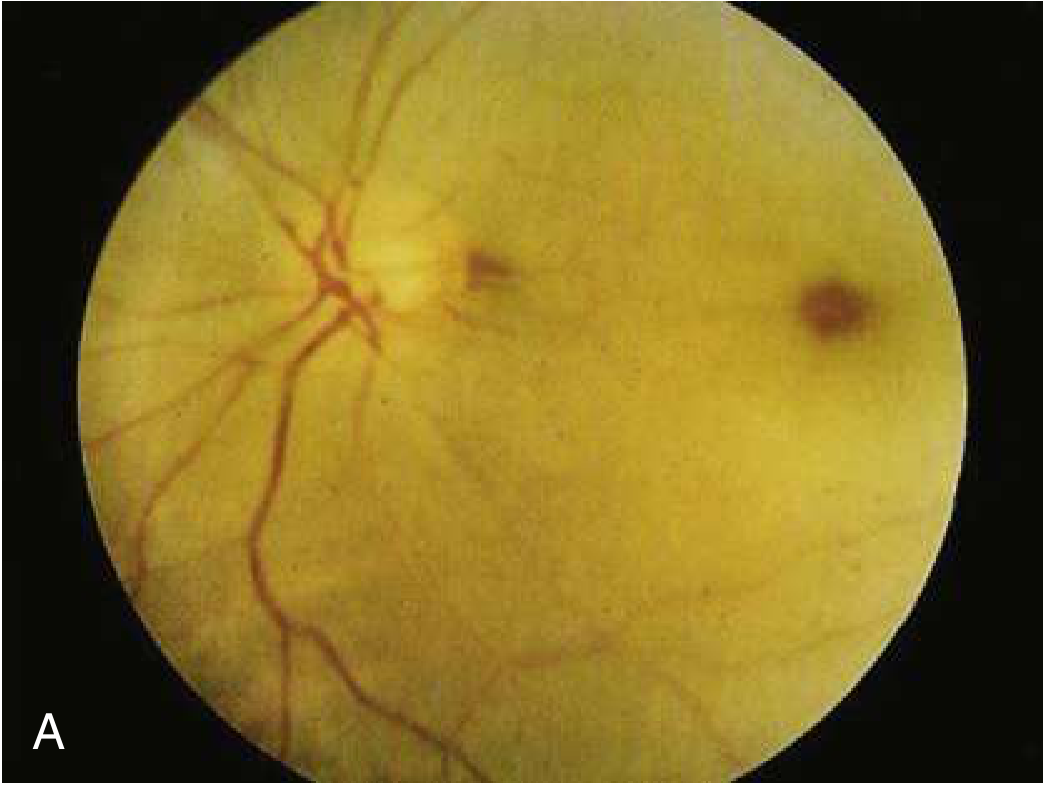
Pathophysiology: The retina tolerates ischemia for approximately 90 minutes with full recovery possible. Beyond 4 hours, damage becomes irreversible. The fovea is supplied by choroidal circulation - this is why the classic "cherry-red spot" appears (the intact choroidal reflex through the thin fovea contrasts against the surrounding pale, edematous ischemic retina).
Subtypes:
- Non-arteritic permanent (>2/3 of cases) - equivalent to ischemic stroke of the retina
- Non-arteritic transient - related to vasospasm; may present as TIA of the retina
- Arteritic - due to giant cell arteritis (GCA/temporal arteritis)
Risk factors: Age 50-70 years, hypertension, hyperlipidemia, diabetes mellitus, atrial fibrillation, cardiac valvular abnormality, sickle cell disease, collagen vascular disease, vasculitis, increased orbital pressure (acute glaucoma, retrobulbar hemorrhage, endocrine exophthalmos).
Clinical features:
- Sudden, profound, painless monocular vision loss (pain suggests GCA)
- VA severely reduced; absence of light perception suggests GCA or ophthalmic artery occlusion
- Relative afferent pupillary defect (RAPD) - profound, sometimes total (amaurotic pupil)
- Fundoscopy: pale/gray-white edematous retina with cherry-red spot at the fovea, attenuated arteries, "cattle-trucking" or "box-car" segmentation of blood column
Prognosis: Poor - spontaneous recovery in only 1-8% of cases. In 2/3 of patients, final VA is worse than 6/120; only 1/5 are left with VA of 6/12 or better.
Special note: If a cilioretinal artery is present (a variant supplying the macular area directly from the choroidal circulation), central vision may be preserved despite CRAO.
2. Branch Retinal Artery Occlusion (BRAO)
- Sudden, profound, painless altitudinal or sectoral visual field loss
- BRAO may go unnoticed if central vision is spared
- RAPD often present
- Fundus: cloudy white "ground glass" retinal edema in affected sector; occluding emboli visible at bifurcation points; "cattle-trucking" of blood column
- FA shows delayed arterial filling and hypofluorescence
- Carries a somewhat better prognosis than CRAO
- Superotemporal quadrant most commonly affected
3. Central Retinal Vein Occlusion (CRVO)
Pathophysiology: Venous congestion leads to increased hydrostatic pressure, fluid extravasation, and secondary retinal ischemia.
Subtypes:
- Non-ischemic CRVO: dilated retinal vessels and edema only; VA >20/200 in over 80% of patients
- Ischemic CRVO: sudden onset of painless monocular vision loss; VA <20/200 in over 90%; major complications are neovascular glaucoma and macular edema
Risk factors: Hypertension (most important), hyperlipidemia, diabetes mellitus, vasculitides, hyperviscosity states, smoking.
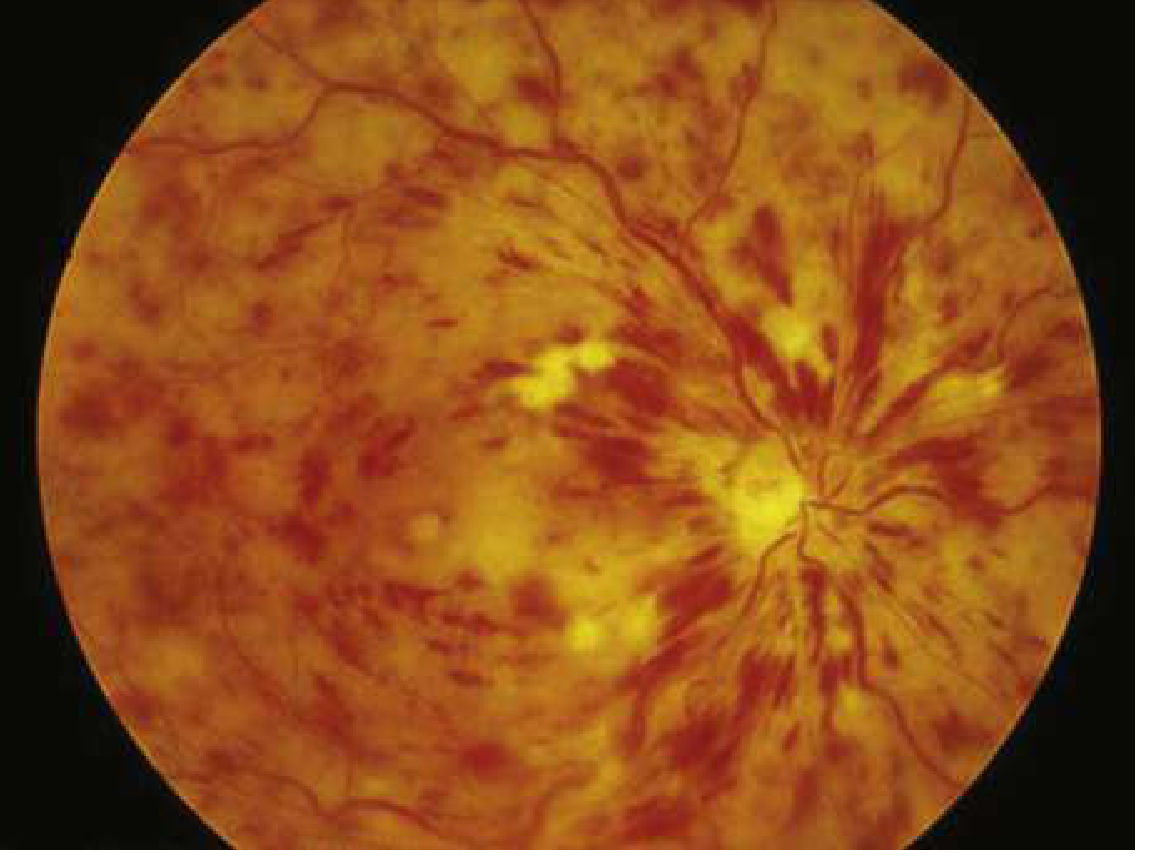
Fundoscopy - classic "blood and thunder" appearance:
- Dilated and tortuous retinal veins in ALL quadrants
- Flame-shaped hemorrhages throughout all 4 quadrants
- Disc edema and cotton-wool spots
4. Branch Retinal Vein Occlusion (BRVO)
- Blurred vision and metamorphopsia if macula involved; asymptomatic if peripheral
- Flame-shaped and dot/blot hemorrhages confined to the sector drained by the thrombosed vein
- Superotemporal quadrant most commonly affected (at an arteriovenous crossing point)
- Chronic macular edema is the most common cause of persistent poor VA
- Retinal neovascularization occurs in ~8% by 3 years; risk higher with >5 disc areas of non-perfusion on FA
5. Ischemic Optic Neuropathy (ION)
Two primary types:
Anterior Ischemic Optic Neuropathy (AION)
Involves the optic nerve head. Subdivided as:
A. Non-arteritic AION (NA-AION) - most common
- Patients >50 years with systemic vascular disease, diabetes, hypertension
- Precipitated by: anemia, hypovolemia, dehydration, systemic hypotension, nocturnal BP fluctuations, dialysis
- Visual field defect often respects the horizontal midline (altitudinal defect)
- Pale, swollen optic disc; large RAPD
B. Arteritic AION (A-AION) - due to Giant Cell Arteritis (GCA/Temporal Arteritis)
- Extremely rare under 50 years; incidence rises with each decade
- Systemic symptoms: weight loss, malaise, jaw claudication, headache, scalp tenderness, polymyalgia rheumatica, low-grade fever
- In up to 25%, acute vision loss is the ONLY symptom
- Vision loss: unilateral 46%, sequential 37%, simultaneously bilateral 17%
- May be preceded by amaurosis fugax
- Untreated: may progress to involve the other eye
- ESR and CRP are elevated; temporal artery biopsy confirms diagnosis
Posterior Ischemic Optic Neuropathy (PION)
Involves the retrobulbar portion of the optic nerve; no disc swelling initially.
6. Amaurosis Fugax (Transient Monocular Vision Loss)
- Transient, painless monocular vision loss, classically described as "a curtain coming down over the eye"
- Typically lasts minutes, recovery in reverse order of loss
- Usually of embolic origin (from ipsilateral carotid stenosis or cardiac source)
- A TIA equivalent of the retina - warns of impending stroke
- Reported in: 2% of CRAO, 14% of BRAO, 5% of CRVO, 3% of NA-AION, and 32% of GCA with ocular involvement
- Attacks can range from several times daily to once every few months
- Management: same as stroke workup - urgent
7. Vitreous Hemorrhage
- Sudden painless vision loss, often described as "floaters," "haze," or complete visual obscuration
- Causes: proliferative diabetic retinopathy, posterior vitreous detachment with retinal tear, subarachnoid hemorrhage (Terson syndrome), sickle cell disease, trauma
- Fundoscopy: red reflex absent or poor; dark blood in vitreous
8. Retinal Detachment
- Painless visual field loss, often preceded by photopsia (flashing lights) and floaters
- "Curtain" or "shadow" spreading across visual field
- Risk factors: myopia, trauma, prior ocular surgery, family history
- Fundoscopy: detached retina appears elevated and billowing
9. Occipital Cortex Infarction (Cortical/Posterior Visual Pathway)
- Binocular visual field loss (homonymous hemianopia) - affects the same field in both eyes
- Caused by posterior cerebral artery infarction
- Associated neurological symptoms common (except in pure occipital strokes)
- Important: basilar artery territory infarction causes sudden complete bilateral blindness
Key Differentiating Features
| Condition | Eye | Pain | VA | RAPD | Fundus |
|---|---|---|---|---|---|
| CRAO | Monocular | No | Profound loss | Large | Pale retina, cherry-red spot, attenuated arteries |
| BRAO | Monocular | No | Variable/sectoral | Often present | Ground-glass edema in sector, visible embolus |
| CRVO | Monocular | No | Variable | Variable | "Blood and thunder" - 4-quadrant hemorrhages, tortuous veins, disc edema |
| BRVO | Monocular | No | Variable (macular) | Variable | Sectoral hemorrhages, AV crossing point |
| A-AION (GCA) | Monocular (may progress to bilateral) | No (systemic Sx) | Severe | Large | Pale, swollen disc |
| NA-AION | Monocular | No | Moderate-severe | Large | Pale, swollen disc, altitudinal VF defect |
| Amaurosis fugax | Monocular | No | Transient - recovers | None (transient) | Normal (between attacks) |
| Vitreous hemorrhage | Monocular | No | Variable | Usually absent | Absent red reflex, vitreous blood |
| Retinal detachment | Monocular | No | Field loss | Present if extensive | Elevated, billowing retina |
| Occipital stroke | Binocular (hemianopia) | No | Hemianopic loss | Absent | Normal fundus |
Diagnostic Approach
History:
- Onset speed (seconds = vascular; minutes = TIA; gradual = other)
- Monocular vs. binocular (critical - have patient cover each eye)
- Duration (transient = amaurosis fugax; persistent = infarction)
- Associated systemic symptoms (jaw pain, scalp tenderness = GCA; neurological Sx = stroke)
- Risk factors: cardiovascular disease, DM, HTN, atrial fibrillation
Examination:
- Visual acuity (each eye separately)
- Visual fields (confrontation testing)
- RAPD testing (swinging flashlight test)
- Fundoscopy (critical - most diagnoses can be made here)
- Check for carotid bruits
Investigations:
- ESR, CRP - mandatory if GCA suspected (elevated in >90%)
- Temporal artery biopsy - gold standard for GCA
- CT/MRI brain - cortical causes, posterior pathway pathology
- Carotid Doppler ultrasound - stenosis evaluation
- Echocardiography - cardiac embolic source
- FFA (fluorescein angiography) - delineate extent of ischemia
- Hypercoagulable workup - mandatory in patients under 50 years
Management
CRAO - A True Emergency (Stroke of the Retina)
Window for intervention: < 4-6 hours from onset
Acute interventions (evidence limited, but widely attempted):
- Ocular massage - 10-15 seconds of pressure through closed eyelids then sudden release, for 3-5 minutes; aims to dislodge embolus and promote forward flow
- Anterior chamber paracentesis - 27-gauge needle to withdraw aqueous humor, acutely lowering IOP to increase perfusion gradient
- IOP-lowering agents - topical timolol, acetazolamide IV, mannitol
- Carbogen inhalation (95% O2 + 5% CO2) - causes vasodilation of retinal arteries, increases intra-arterial pCO2
- IV thrombolysis (tPA) - alteplase 0.9 mg/kg (10% as bolus, remainder over 59 min) if < 4.5 hours from onset for non-arteritic CRAO; intra-arterial thrombolysis if < 6 hours
- Hyperbaric oxygen (HBO) - theoretical direct oxygenation of retina; current evidence limited to retrospective data
None of the above therapies have been conclusively proven to improve visual outcomes in randomized trials. Treatment should be individualized in consultation with an ophthalmologist.
Systemic workup and secondary prevention (critical):
- 30% of CRAO patients have severe carotid disease, coincidental stroke, or extreme hypertension
- 20% have simultaneous MI or critical heart disease
- ~95% need a change in systemic medication; 25% require urgent surgical intervention
- Antiplatelet therapy (aspirin 600 mg loading dose) unless contraindicated
- Oral anticoagulation for atrial fibrillation
- Carotid endarterectomy for symptomatic stenosis >70%
- Urgent referral to stroke clinic - high risk of cerebrovascular event in the days following
CRVO
- Treat underlying systemic causes (hypertension, diabetes, hyperlipidemia)
- Intravitreal anti-VEGF injections - mainstay for macular edema (bevacizumab, ranibizumab, aflibercept)
- Intravitreal corticosteroid implants (dexamethasone)
- Laser photocoagulation for neovascularization
- Monitor for neovascular glaucoma
Arteritic AION (GCA)
- Ophthalmologic emergency - urgent high-dose IV methylprednisolone (500 mg - 1 g/day for 3 days) to prevent fellow eye involvement
- Then oral prednisolone 1 mg/kg/day
- Temporal artery biopsy (should not delay steroid treatment)
- Long-term steroid taper with monitoring of ESR/CRP
NA-AION
- No proven treatment for the acute episode
- Address underlying vascular risk factors
- Aspirin may reduce risk of fellow eye involvement
- Avoid nocturnal hypotension (especially in dialysis patients)
Amaurosis Fugax
- Urgent workup as for TIA/stroke
- Carotid Doppler, echocardiography, cardiac monitoring (Holter)
- Antiplatelet or anticoagulant therapy based on etiology
- Carotid endarterectomy for high-grade ipsilateral stenosis
Ocular Ischemic Syndrome (OIS)
A related condition caused by chronic ocular hypoperfusion due to severe (>90%) ipsilateral atherosclerotic carotid stenosis. Typically affects older patients; may be associated with diabetes and cardiovascular disease. Presents with dull aching eye pain, dilated but non-tortuous retinal veins, and microaneurysms - Kanski's Clinical Ophthalmology, 10e.
Key Clinical Pearls
- Acute angle-closure glaucoma - can cause sudden monocular vision loss but pain is universal; a cloudy/steamy lens is visible. Always rule this out if any doubt exists.
- CRAO is a stroke equivalent - treat with the same urgency as acute ischemic stroke. The risk of subsequent cerebrovascular events is substantial.
- GCA is bilateral threat - untreated arteritic AION progresses to bilateral blindness. Steroids must be started immediately, before biopsy results.
- Always ask about monocular vs. binocular - patients commonly cannot distinguish between unilateral visual loss and a contralateral hemianopia. Have them cover each eye.
- The pain-vision loss combination - pain with sudden vision loss points to acute angle closure glaucoma, optic neuritis (pain on eye movement), or GCA (jaw pain, headache).
- Hypercoagulable workup - mandatory in all patients under 50 years with any retinal vascular occlusion.
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10e - Chapters on Retinal Vascular Disease, RAO, RVO, AION
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 10e - Chapter 57: Sudden Monocular Vision Loss
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.