Cardiovascular accident
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"stroke"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content from Harrison's and Frameworks for Internal Medicine. Let me compile the full answer.
Cerebrovascular Accident (CVA) - Stroke
Definition
A stroke, or cerebrovascular accident (CVA), is defined as an abrupt onset of a neurologic deficit attributable to a vascular cause - specifically, acute infarction of brain tissue, spinal cord, or retina resulting in neurologic deficits. The diagnosis is clinical, supported by brain imaging. If neurologic deficits resolve within 24 hours with no evidence of infarction on imaging, the event is called a transient ischemic attack (TIA) rather than a stroke.
- Harrison's Principles of Internal Medicine 22E, p. 3472
- Frameworks for Internal Medicine, p. 574
Epidemiology
- Stroke is the second leading cause of death worldwide - 7.1 million deaths in 2020
- A stroke occurs approximately every 40 seconds in the United States
- Prevalence is ~15% in adults over 80 years
- The 30-day mortality rate is ~10%; 1-year mortality ~20%; 5-year mortality ~40%
- Overall disease burden will continue to rise as the population ages
Classification

Strokes fall into two broad categories:
1. Ischemic Stroke (~80% of all strokes)
Caused by a reduction in blood flow lasting longer than several seconds. Neurons lack glycogen, so energy failure occurs rapidly. Types include:
- Thrombotic stroke - occlusion from atherosclerotic disease within the cerebral vessel itself
- Embolic stroke - embolus from a proximal arterial source (e.g., carotid artery) or from the heart (e.g., atrial fibrillation, cardiac thrombus)
- Small-vessel (lacunar) disease - occlusion of small penetrating arteries, typically from hypertension or diabetes
2. Hemorrhagic Stroke (~20% of all strokes)
Caused by bleeding directly into or around the brain. Subdivided into:
- Intracerebral hemorrhage (ICH) - bleeding into the brain parenchyma (~10-15% of all strokes); most common cause is hypertension
- Subarachnoid hemorrhage (SAH) - bleeding between the arachnoid and pia mater (~5% of all strokes); most common cause is aneurysm rupture
Hemorrhagic stroke is associated with significantly higher acute morbidity and mortality (30-day mortality approaching 50%, vs ~10% for ischemic stroke).
Pathophysiology
Ischemic injury: Cerebral ischemia causes neurologic symptoms within seconds. If flow cessation lasts minutes, brain infarction (irreversible cell death) occurs. Focal ischemia results from vessel thrombosis or embolism.
Hemorrhagic injury: Blood causes injury through mechanical compression of brain tissue and local toxicity from blood breakdown products, plus raised intracranial pressure.
A generalized reduction in cerebral blood flow (e.g., cardiac arrest, sepsis) can produce hypoxic-ischemic encephalopathy or border-zone infarctions - distinct from focal stroke.
Risk Factors
| Risk Factor | Notes |
|---|---|
| Hypertension | Strongest risk factor; present in most stroke patients (SBP ≥140 or DBP ≥90 mmHg) |
| Smoking | Doubles lifetime stroke risk; >1 pack/day = 6x greater risk; smokers + hypertension = 20x risk |
| Atrial fibrillation | Major source of cardioembolic stroke |
| Diabetes mellitus | Independent risk factor |
| Dyslipidemia | Contributes to atherosclerosis |
| Physical inactivity / poor nutrition | Modifiable lifestyle factors |
| Older age, family history | Non-modifiable |
| Chronic kidney disease | Associated with increased risk |
Good news on smoking: the risk of CVA declines rapidly after cessation and at 5 years equals that of a nonsmoker - emphasizing it is never too late to quit.
- Textbook of Family Medicine 9e; Frameworks for Internal Medicine, p. 574
Clinical Features - Warning Signs (FAST)
The FAST acronym is used to teach recognition to the lay public:
- F - Facial weakness (asymmetry, droop)
- A - Arm weakness (unilateral)
- S - Speech abnormality (dysarthria, aphasia)
- T - Time (treatments are highly time-sensitive - call emergency services immediately)
Other common symptoms:
- Loss of sensory/motor function on one side (hemiparesis in ~85% of ischemic strokes)
- Visual changes (hemianopia, monocular blindness)
- Gait disturbance, ataxia
- Sudden severe headache ("thunderclap" - classic for SAH)
Stroke Syndromes by Vascular Territory
| Territory | Key Features |
|---|---|
| Middle Cerebral Artery (MCA) | Contralateral face/arm > leg weakness & sensory loss; aphasia (dominant hemisphere); neglect, anosognosia (non-dominant); homonymous hemianopia |
| Anterior Cerebral Artery (ACA) | Contralateral leg > arm weakness; frontal lobe signs |
| Posterior circulation (vertebrobasilar) | Diplopia, vertigo, dysphagia, ipsilateral cranial nerve deficits + contralateral limb weakness; "crossed" deficits |
| Lacunar (small vessel) | Pure motor hemiplegia, pure sensory stroke, ataxic hemiparesis - no cortical signs |
Differential Diagnosis
Conditions that can mimic stroke or TIA:
- Seizure / Todd's paralysis (postictal paresis)
- Intracranial tumor or subdural hematoma
- Migraine (hemiplegic migraine)
- Hypoglycemia
- Metabolic encephalopathy
- Conversion disorder
Diagnosis
Brain imaging is mandatory to distinguish ischemic from hemorrhagic stroke - this cannot be done on clinical grounds alone, and the treatment differs fundamentally.
- Non-contrast CT - First-line; highly sensitive for acute hemorrhage, widely available, fast
- MRI (DWI) - More sensitive than CT for ischemic stroke, especially in the posterior fossa and within the first few hours
- Lumbar puncture - If CT is negative but SAH is suspected (xanthochromia or RBCs in CSF)
Management
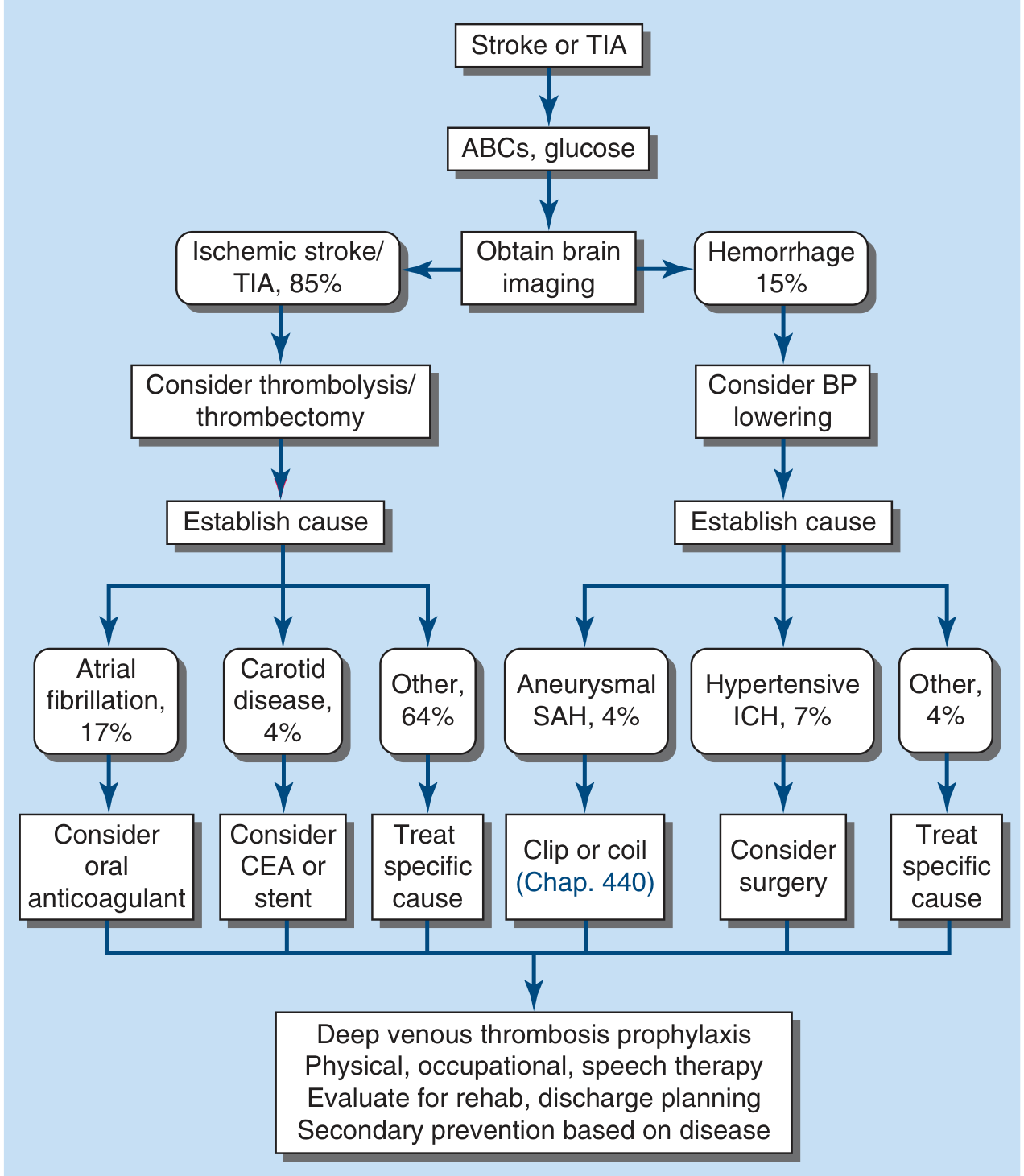
Figure: Medical management of stroke and TIA - from Harrison's Principles of Internal Medicine 22E
Acute Ischemic Stroke
- ABCs + stabilization - Airway, breathing, circulation; check glucose (hypoglycemia can mimic stroke)
- Thrombolysis - IV recombinant tPA (rtPA/alteplase) within the treatment window (generally 4.5 hours of onset) in eligible patients
- Mechanical thrombectomy - Endovascular clot removal for large vessel occlusion; highly effective up to 24 hours in selected patients
- Blood pressure management - BP is often elevated acutely; permissive hypertension in most ischemic strokes (do not lower aggressively unless giving tPA or BP is extreme)
- Antiplatelet therapy - Aspirin 325 mg within 24-48 hours (not if tPA given)
Acute Hemorrhagic Stroke
- Blood pressure lowering - Aggressive BP control is indicated
- Reverse anticoagulation if applicable (vitamin K, reversal agents)
- Surgical options - Consider surgery for hypertensive ICH in selected cases; aneurysmal SAH treated with surgical clipping or endovascular coiling
General In-Hospital Care (all stroke types)
- Deep venous thrombosis prophylaxis
- Dysphagia screening before oral intake
- Physical, occupational, and speech therapy
- Evaluation for inpatient rehabilitation
- Discharge planning and secondary prevention
Secondary Prevention
Targeted to the underlying stroke mechanism:
| Cause | Prevention Strategy |
|---|---|
| Atrial fibrillation (17% of ischemic strokes) | Oral anticoagulation (warfarin or DOAC) |
| Carotid atherosclerosis (4%) | Carotid endarterectomy (CEA) or stenting if significant stenosis |
| Other (large artery, small vessel, cryptogenic) (64%) | Antiplatelet therapy, statin, BP control, lifestyle modification |
| Aneurysmal SAH | Surgical clipping or endovascular coiling |
All patients benefit from: aggressive hypertension control, statin therapy, smoking cessation, diabetes management, and physical activity.
Prognosis
- 30-day mortality: ~10% overall (ischemic); approaching 50% for hemorrhagic
- 1-year mortality: ~20%; 5-year mortality: ~40%
- Worse prognosis with: older age, comorbid ischemic heart disease or diabetes, larger infarct size
- Long-term functional outcomes among survivors are similar between hemorrhagic and ischemic stroke
Harrison's Principles of Internal Medicine 22E, p. 3472-3474 | Frameworks for Internal Medicine, pp. 574-576 | Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.