Long case viva questions on peripheral arterial diseases
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I have enough rich content to now compile a comprehensive set of long case viva questions on peripheral arterial disease. Let me write the detailed answer.
Long Case Viva Questions on Peripheral Arterial Disease (PAD)
Below is a structured set of viva questions organized the way a long case presentation unfolds - from history to examination to investigations to management. Expected answer points are included for each question.
SECTION 1: Introduction and Epidemiology
Q1. What is peripheral arterial disease? How prevalent is it and why is it clinically significant beyond the leg?
Expected answer:
- PAD is atherosclerotic occlusive disease of the peripheral (predominantly lower limb) arteries, causing a spectrum from asymptomatic stenosis to limb-threatening ischemia.
- It is age-dependent, underdiagnosed, and undertreated. The PARTNERS program found PAD in 29% of primary care patients aged >70 or aged 50-69 with smoking/diabetes history.
- More than 50% of patients with PAD are entirely asymptomatic.
- Clinically significant because it is a powerful independent predictor of mortality - PAD patients have a ~4-fold higher risk of MI and 2-3x higher risk of stroke vs. non-PAD patients. Approximately 40% of patients with atherosclerotic vascular disease have disease in more than one vascular bed.
- Patients with critical limb ischemia (CLI) have an annual mortality rate of ~25%.
(Textbook of Family Medicine 9e)
Q2. What are the risk factors for PAD?
Expected answer:
- Modifiable: Cigarette smoking (single most important), diabetes mellitus, hypertension, hyperlipidaemia, obesity, sedentary lifestyle.
- Non-modifiable: Age (>50 years), male sex, family history, ethnicity (higher in Black populations).
- Emerging: Hyperhomocysteinaemia, elevated lipoprotein(a), chronic kidney disease (CKD), inflammatory markers (CRP).
- Smoking is particularly important - it roughly doubles the risk of PAD and is directly associated with claudication severity and amputation risk.
SECTION 2: History Taking
Q3. How would you take a history from a patient presenting with possible PAD?
Expected answer:
- Claudication history:
- Onset, site, character of pain (cramping/aching in muscle groups)
- Claudication distance (how far before pain starts) - note this varies little day to day
- Relieved by standing still within 5 minutes (differentiates from nerve compression, which requires sitting)
- Pain not present on first step (unlike osteoarthritis)
- Worsening with uphill walking, increased speed, carrying weights
- Rest pain:
- Pain in foot/calf at rest, worse at night, worse with leg elevation
- Patient hangs foot out of bed or sleeps in chair for relief (gravity effect)
- Indicates more severe ischemia than claudication
- Skin changes: Non-healing ulcers, blackened tissue (gangrene)
- Cardiovascular review: Ask about chest pain, dyspnoea, palpitations, TIA/stroke, renal impairment (co-existing atherosclerosis)
- Risk factor assessment: Smoking history (pack-years), diabetes management, hypertension and medications, lipid profile, family history
- Functional impact: How has claudication affected occupation, social, and leisure activities?
- Erectile dysfunction - may indicate aortoiliac disease (Leriche syndrome)
(Bailey and Love's Short Practice of Surgery 28e; Textbook of Family Medicine 9e)
Q4. What is Leriche syndrome? What is its triad?
Expected answer:
- Leriche syndrome results from aortoiliac occlusion.
- Classic triad: (1) Buttock and thigh claudication; (2) absence of femoral pulses bilaterally; (3) erectile dysfunction (sexual impotence) in men due to internal iliac artery insufficiency.
- The level of claudication is one anatomical level below the arterial obstruction - aortoiliac disease causes thigh and buttock claudication.
(Bailey and Love's Short Practice of Surgery 28e)
Q5. How do you differentiate claudication from other causes of leg pain on history?
Expected answer:
| Feature | Arterial Claudication | Neurogenic Claudication (spinal stenosis) | Osteoarthritis |
|---|---|---|---|
| Onset | After fixed walking distance | Variable | On movement |
| Relief | Standing still (5 min) | Sitting/leaning forward | Rest (prolonged) |
| Position | Any resting position | Must sit | Any |
| First step | Pain-free | Often pain-free | Painful |
| Uphill | Worse | Better (spinal flexion) | Variable |
| Pulses | Absent/reduced | Normal | Normal |
SECTION 3: Clinical Examination
Q6. How would you examine a patient with suspected PAD?
Expected answer:
- General inspection: Pallor, cyanosis, tar-stained fingers (smoking), xanthelasma, corneal arcus
- Inspect the limbs: Skin colour (pallor, cyanosis, dependent rubor "sunset foot"), hair loss, muscle wasting, trophic skin changes, ulcers, gangrene
- Buerger's test:
- Elevate both legs to 45 degrees for 1-2 minutes - ischaemic limb goes pale (positive)
- Then hang legs down - ischaemic limb flushes deep red-purple (reactive hyperaemia/dependent rubor = "sunset foot" sign)
- Buerger's angle = the angle at which the limb becomes pale; <20 degrees = severe ischemia
- Capillary refill time: Press heel/toe pulp for 5 seconds; normal 2-3 seconds; prolonged >10 sec in severe ischemia
- Pulses: Systematically palpate femoral, popliteal, posterior tibial, dorsalis pedis
- Compare bilateral femoral pulses
- Note: pulse distal to an arterial occlusion is usually absent; collaterals may occasionally allow palpable distal pulses even with stenosis
- Exercise (walking to claudication) will cause a distal pulse to disappear as vasodilation occurs below the obstruction
- Auscultation: Bruit over aorta, iliac, femoral arteries (indicates turbulent flow, suggests stenosis). Note: tight stenoses/complete occlusions may be silent.
- Abdomen: Palpate for aortic aneurysm (may coexist with lower limb occlusive disease)
- Venous guttering: A chronically ischaemic leg elevated will show collapsing, guttered veins
(Bailey and Love's Short Practice of Surgery 28e)
Q7. What does the site of absent pulses tell you about the level of disease?
Expected answer: (Mirrors Table 61.1 from Bailey & Love)
| Site of obstruction | Clinical findings |
|---|---|
| Aortoiliac | Claudication in buttocks, thighs, calves. Both femoral and distal pulses absent. Aortoiliac bruit. Impotence (Leriche). |
| Iliac (unilateral) | Unilateral thigh/calf (sometimes buttock) claudication. Unilateral absent femoral and distal pulses. Iliac bruit. |
| Femoropopliteal (SFA - commonest, 70%) | Unilateral calf claudication. Femoral pulse present, popliteal and distal pulses absent. |
| Distal (tibial/peroneal) | Femoral and popliteal pulses present. Ankle pulses absent. Claudication in calf and foot. |
SECTION 4: Investigations
Q8. What is the ankle-brachial index (ABI)? How is it measured and how do you interpret it?
Expected answer:
- ABI = highest ankle systolic pressure (dorsalis pedis, posterior tibial, or peroneal) / highest ipsilateral brachial systolic pressure.
- Measured using a hand-held Doppler probe and sphygmomanometer.
- Interpretation:
- 0.9-1.4: Normal
- <0.9: Hemodynamically significant arterial lesion (PAD diagnosis)
- 0.5-0.9: Claudication range
- <0.4: Critical limb-threatening ischemia (CLTI)
-
1.4: Arterial calcification/incompressibility (falsely elevated - seen in diabetes, chronic renal failure)
- A drop of >20% from resting ABI after exercise is indicative of flow-limiting arterial disease (exercise ABI is useful when resting ABI is normal but symptoms suggest PAD).
- Pitfall: In diabetics with medial calcification, vessels are non-compressible. Use toe-brachial index (TBI) instead - toe (digital) arteries are rarely affected by calcification. TBI <0.6 suggests significant arterial disease.
(Bailey and Love's Short Practice of Surgery 28e; Textbook of Family Medicine 9e)
Q9. What investigations would you order for a patient with PAD? Justify each.
Expected answer:
Bedside/Basic:
- ABI with hand-held Doppler (confirms diagnosis, grades severity)
- Blood glucose, HbA1c (diabetes screening/monitoring)
- Full blood count (anaemia worsens ischemia by reducing O2 delivery)
- Lipid profile (identify and quantify dyslipidaemia)
- Renal function (coexisting renovascular disease; relevant for contrast use)
- ECG (coexisting coronary artery disease is present in ~50%)
Vascular Imaging (when intervention is planned):
- Duplex Doppler Ultrasonography (DUS): First-line non-invasive imaging. Localises stenosis, determines degree using peak systolic velocity ratio (PSVR). PSVR ≥2.4 = obstructive disease; PSVR ≥3.0 = functionally significant. Useful for graft/stent surveillance.
- CT Angiography (CTA): Best anatomical detail, 3D reconstruction, invaluable for pre-operative planning. Limitation: iodinated contrast (risk of nephropathy, especially in diabetics), ionising radiation. Metformin must be withheld periprocedurally.
- MR Angiography (MRA): No ionising radiation, no iodinated contrast. Uses gadolinium (caution in severe CKD - nephrogenic systemic fibrosis). Good for aortoiliac and femoropopliteal segments.
- Digital Subtraction Angiography (DSA): Gold standard for arterial anatomy. Access via Seldinger technique (usually common femoral artery). Provides dynamic flow information and can be combined with endovascular treatment. Complications: haematoma, false aneurysm, thrombosis, arterial dissection, distal embolisation, renal dysfunction, allergic reaction (~5%). Reserved for when intervention is planned.
(Bailey and Love's Short Practice of Surgery 28e; Textbook of Family Medicine 9e)
Q10. What is the Seldinger technique?
Expected answer:
- A technique for gaining percutaneous arterial access.
- Steps: (1) Needle puncture of the artery (usually CFA); (2) guidewire inserted through needle; (3) needle withdrawn over wire; (4) sheath/catheter threaded over wire; (5) wire removed.
- Allows introduction of catheters, sheaths, and interventional devices without surgical cut-down.
SECTION 5: Classification
Q11. Describe the Fontaine classification of PAD.
Expected answer:
| Stage | Clinical Features |
|---|---|
| I | Asymptomatic |
| IIa | Mild claudication (claudication distance >200 m) |
| IIb | Moderate-severe claudication (claudication distance <200 m) |
| III | Ischaemic rest pain |
| IV | Ulceration or gangrene |
Q12. What is the Rutherford classification of PAD?
Expected answer:
| Grade | Category | Description |
|---|---|---|
| 0 | 0 | Asymptomatic |
| I | 1 | Mild claudication |
| I | 2 | Moderate claudication |
| I | 3 | Severe claudication |
| II | 4 | Ischaemic rest pain |
| III | 5 | Minor tissue loss (non-healing ulcer) |
| III | 6 | Major tissue loss (frank gangrene) |
Categories 4, 5, 6 = critical limb-threatening ischemia (CLTI).
Q13. What is meant by chronic limb-threatening ischaemia (CLTI)?
Expected answer:
- CLTI (previously called critical limb ischemia/CLI) refers to patients with ischaemic rest pain and/or ischaemic ulceration/gangrene (tissue loss).
- Defines the highest-risk end of the PAD spectrum with an imminently threatened limb.
- Requires urgent vascular assessment and revascularisation to prevent major amputation.
- These patients have the lowest ABIs (<0.4) and the highest annual mortality (~25%).
- Bilateral co-morbidities (coronary, cerebral, renal) are almost universally present.
(Bailey and Love's Short Practice of Surgery 28e; Textbook of Family Medicine 9e)
SECTION 6: Management
Q14. Outline the management of a patient with intermittent claudication.
Expected answer:
Conservative/Medical (most claudicants improve or stabilise with this):
- Smoking cessation - single most effective intervention; dramatically slows progression
- Supervised exercise rehabilitation - structured walking programme (30-45 min, 3x/week); increases pain-free walking distance by improving collateral flow and muscle metabolism
- Antiplatelet therapy - aspirin 75-100 mg/day or clopidogrel 75 mg/day (reduces cardiovascular events, not claudication per se)
- Statins - reduce cardiovascular events; some improvement in walking distance
- Antihypertensives - ACE inhibitors preferred (also shown to reduce cardiovascular events in HOPE trial)
- Diabetes control - tight glycaemic control
- Cilostazol (PDE-3 inhibitor) - only drug with evidence of improving claudication: increases maximal walking distance by 54% vs placebo. Contraindicated in heart failure. Approved by FDA for claudication.
- Pentoxifylline - no randomised data showing benefit over placebo; not recommended.
- Foot care - especially in diabetics to prevent ulceration
Endovascular/Surgical (for disabling claudication or CLTI):
- Indications: lifestyle-limiting claudication not responding to 3-6 months of conservative treatment, rest pain, tissue loss
- Angioplasty ± stenting (PTA): First-line for short segment lesions (TASC A/B); shorter recovery, less morbidity. Risk of restenosis from neointimal hyperplasia.
- Surgical bypass: For long-segment occlusions (TASC C/D), failed endovascular procedures; e.g., aortobifemoral bypass (aortoiliac), femoro-popliteal bypass.
- Graft material: Autologous vein (long saphenous - best patency) vs. synthetic (PTFE or Dacron - acceptable above knee, poor below knee).
(Textbook of Family Medicine 9e; Bailey and Love's Short Practice of Surgery 28e)
Q15. What is cilostazol and how does it work? When is it contraindicated?
Expected answer:
- Cilostazol is a phosphodiesterase type III (PDE-3) inhibitor. It inhibits platelet aggregation and causes arterial vasodilation by preventing breakdown of cAMP.
- Approved by the FDA for treatment of intermittent claudication (1999).
- In randomised trials comparing cilostazol 100 mg twice daily vs. pentoxifylline vs. placebo, cilostazol improved maximum walking distance by 54% vs. 30% for pentoxifylline and 34% for placebo.
- Contraindication: Heart failure of any severity (increased mortality in trials with PDE inhibitors in heart failure).
- Dose: 100 mg twice daily.
(Textbook of Family Medicine 9e)
Q16. What are the indications for revascularisation in PAD?
Expected answer:
- Lifestyle-disabling intermittent claudication not improved after 3-6 months of maximal conservative therapy
- Ischaemic rest pain (Fontaine III / Rutherford 4)
- Tissue loss - non-healing ulceration (Fontaine IV / Rutherford 5)
- Gangrene with limb salvage potential (Rutherford 6)
- In CLTI, revascularisation should be performed urgently
Q17. What is the TASC classification? How does it guide treatment?
Expected answer:
- TASC (Trans-Atlantic Inter-Society Consensus) classifies lesions by morphology to guide revascularisation strategy:
- TASC A: Short single stenoses; recommended endovascular (PTA ± stenting)
- TASC B: Multiple short stenoses or single longer stenosis; endovascular preferred
- TASC C: Multiple long stenoses or single occlusion; surgery preferred
- TASC D: Complete occlusions, long segment or aortoiliac involvement; surgery recommended
- Endovascular has lower short-term morbidity; surgery has better long-term patency for complex lesions.
SECTION 7: Acute Limb Ischaemia (ALI) - Viva Extension
Q18. What are the 6 Ps of acute limb ischemia?
Expected answer:
- Pain - sudden severe onset
- Pallor - white/pale limb
- Pulselessness - absent distal pulses
- Paraesthesia - pins and needles (early nerve ischaemia)
- Paralysis - motor deficit (late/severe; urgent sign)
- Perishing cold (Poikilothermia)
Paraesthesia and paralysis indicate irreversible ischemia is approaching and demand emergency surgical intervention.
Q19. How do you differentiate thrombosis from embolism as causes of acute limb ischemia?
Expected answer:
| Feature | Embolism | Thrombosis in-situ |
|---|---|---|
| Onset | Sudden, abrupt | Gradual, preceding claudication |
| Contralateral limb | Normal pulses | Absent/reduced (background PAD) |
| AF/cardiac disease | Often present | Less common |
| Collaterals | Absent (no pre-existing PAD) | Present (compensated) |
| Severity | More severe (no collaterals) | Less severe (collaterals) |
| Treatment | Embolectomy | Thrombolysis ± bypass |
Q20. What is the management of acute limb ischemia?
Expected answer:
- Immediate: IV heparin to prevent propagation; analgesia; urgent vascular surgical referral
- Imaging: Emergency DSA or duplex to determine level and cause
- Surgical embolectomy (Fogarty balloon catheter) - for embolic occlusion, viable limb
- Catheter-directed thrombolysis - for thrombotic occlusion or if surgical risk is high; slower, requires ICU monitoring, risk of haemorrhage
- Surgical bypass - for thrombotic occlusion with anatomical disease
- Amputation - if limb is non-viable (irreversible ischemia with fixed mottling, rigor, paralysis)
- Post-procedure: Investigate and treat the source (echocardiogram if AF/cardiac embolism; anticoagulation)
SECTION 8: Complications and Prognosis
Q21. What are the long-term complications of PAD?
Expected answer:
- Progression to rest pain and CLTI
- Amputation (major or minor) - <5% of claudicants reach amputation; much higher in CLTI
- Myocardial infarction (fourfold risk vs. non-PAD)
- Stroke (2-3x risk)
- Cardiovascular death (leading cause of death in PAD patients)
- Reduced quality of life and functional decline
Q22. What is the natural history of intermittent claudication?
Expected answer:
- Apparent "improvement" in IC over time does NOT reflect disease improvement - it often reflects functional decline (patients walk slower/shorter distances to avoid pain).
- PAD is a progressive disorder causing significant decline in quality of life.
- ~25% of claudicants deteriorate, 25% improve (often due to functional decline), 50% stable.
- Fewer than 5% will ever require amputation.
- The dominant risk is cardiovascular mortality - not limb loss.
- The lower the ABI, the greater the cardiovascular event risk.
(Textbook of Family Medicine 9e)
SECTION 9: Special Situations
Q23. How does diabetes modify PAD presentation and management?
Expected answer:
- PAD in diabetics is more distal (tibial/peroneal vessels affected preferentially), more diffuse, and often bilateral.
- Neuropathy may mask ischemic pain - patient may present with painless ulceration or gangrene without preceding claudication.
- ABI is unreliable due to medial calcification; use TBI <0.6 as threshold.
- Foot ulcers in diabetics are often of mixed ischaemic and neuropathic origin.
- Worse prognosis with higher amputation rates.
- Tight glycaemic control, meticulous foot care, podiatry referral are essential.
- Metformin must be withheld before iodinated contrast studies (CTA/DSA) due to risk of lactic acidosis.
Q24. What is the ABCD (or secondary prevention) strategy in PAD?
Expected answer:
- A - Antiplatelet agents (aspirin or clopidogrel) + ACE inhibitors
- B - Blood pressure control (target <130/80)
- C - Cholesterol (statins - target LDL <1.8 mmol/L) + Cigarette cessation
- D - Diabetes control (HbA1c target ~7%) + Diet and exercise
These reduce cardiovascular events and mortality - the primary threat in PAD - rather than just improving claudication.
KEY IMAGES TO KNOW
The following visuals are commonly discussed in viva settings:
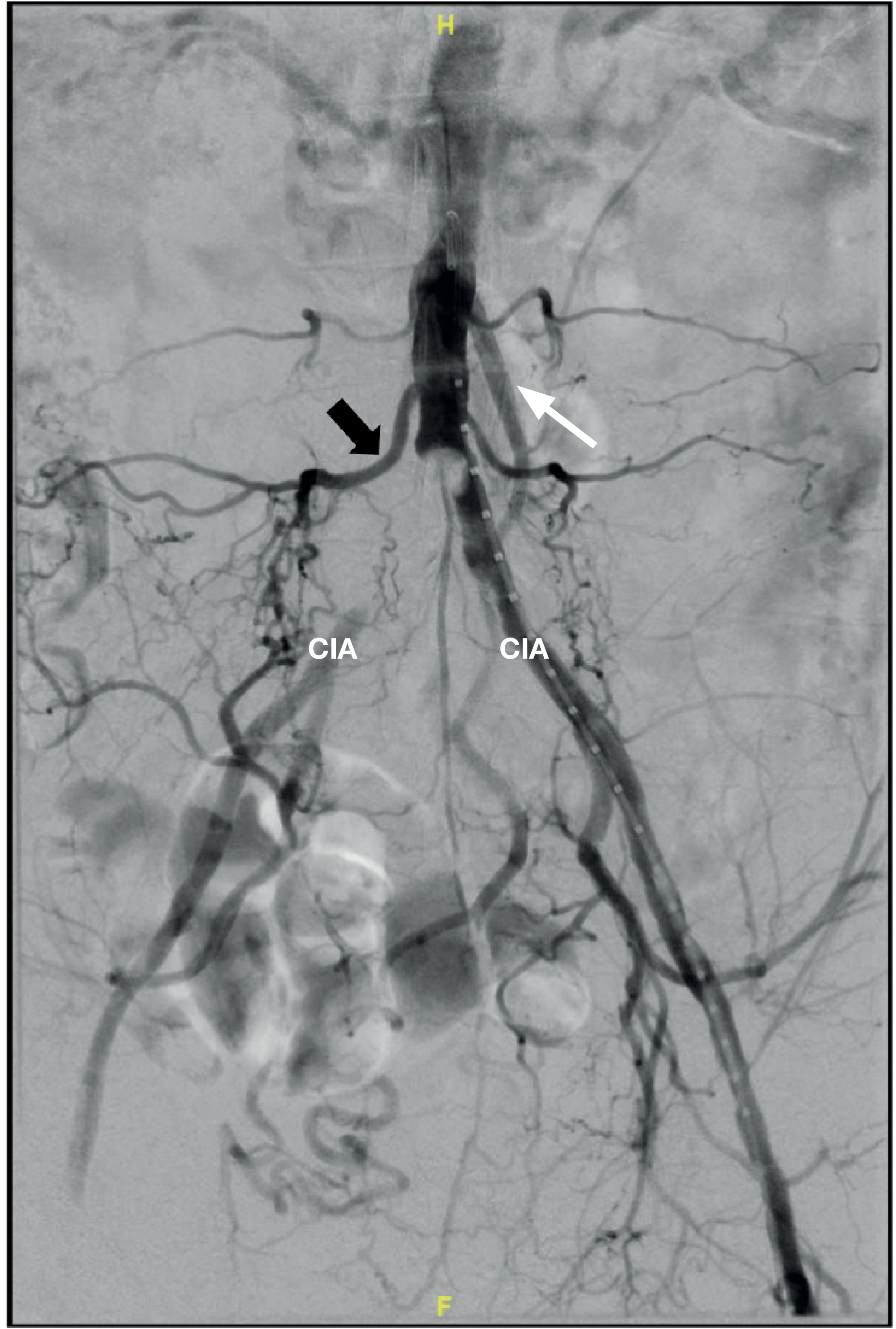
- Aortoiliac bifurcation disease angiogram with collateralisation via lumbar and inferior mesenteric arteries
- Dependent rubor / "sunset foot" - elevation pallor, dependency rubor

- Dry gangrene of the toes in CLTI

QUICK REFERENCE SUMMARY TABLE
| Topic | Key Point |
|---|---|
| Commonest artery affected | Superficial femoral artery (70% of claudication cases) |
| Claudication relief | Standing still ≤5 minutes |
| ABI normal range | 0.9-1.4 |
| ABI in claudication | 0.5-0.9 |
| ABI in CLTI | <0.4 |
| ABI falsely elevated | Diabetes/CKD (calcification) - use toe-brachial index |
| Drug for claudication | Cilostazol (PDE-3 inhibitor) - contraindicated in HF |
| Gold standard imaging | DSA |
| Most common cause of death in PAD | Cardiovascular (MI/stroke) |
| Leriche syndrome | Aortoiliac occlusion: buttock claudication + absent femoral pulses + impotence |
| CLTI annual mortality | ~25% |
Sources: Bailey and Love's Short Practice of Surgery 28th Edition; Textbook of Family Medicine 9e; Bailey and Love's Short Practice of Surgery Ch. 61.
Make a detailed Pg viva questions on pad
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Here is your comprehensive PG-level viva question bank on Peripheral Arterial Disease, structured across 7 major domains with 30 detailed questions and model answers. Here's a summary of what's covered:
Structure Overview
| Part | Topics | Questions |
|---|---|---|
| 1. Basic Science | Atherosclerosis pathophysiology, haemodynamics of claudication, collateral circulation, role of profunda femoris | Q1-4 |
| 2. Clinical Assessment | Fontaine & Rutherford classification, Buerger's test, Leriche syndrome, full clinical examination | Q5-8 |
| 3. Investigations | ABI (detailed technique + limitations), NVIS/segmental pressures, imaging modalities, blood workup | Q9-12 |
| 4. Medical Management | Evidence-based treatment, landmark trials (CAPRIE, EUCLID, CHARISMA, COMPASS, HOPE), cilostazol, beta-blockers | Q13-14 |
| 5. Surgical & Interventional | Indications, TASC II classification, conduit choice, open bypass options, endovascular options, restenosis mechanisms | Q15-19 |
| 6. Acute Limb Ischaemia | Rutherford ALI classification, embolism vs thrombosis, Fogarty procedure, catheter-directed thrombolysis, reperfusion injury and compartment syndrome | Q20-24 |
| 7. Special Topics | Buerger's disease, popliteal aneurysm, WIFI classification, post-revascularisation antithrombotics (COMPASS), bypass complications, graft surveillance | Q25-30 |
PG-Level High-Yield Points to Remember
- Fogarty catheter (1963) - Thomas Fogarty; first fem-pop bypass (1948) - Jean Kunlin; Seldinger technique (1953) - Sven-Ivar Seldinger
- Reperfusion injury >6 hrs = mandatory four-compartment fasciotomy consideration; compartment pressure >25 mmHg = fasciotomy
- COMPASS trial: Rivaroxaban 2.5 mg BD + aspirin reduces MALE + MACE in PAD
- CAPRIE trial: Clopidogrel > aspirin for secondary prevention in PAD
- Neointimal hyperplasia = predominant cause of intermediate graft/stent failure (1-24 months)
- Aortoenteric fistula = most dangerous late graft complication (herald bleed → exsanguination)
- WIFI score governs CLTI management (wound + ischaemia + foot infection must all be addressed)
- TBI <0.6 = significant arterial disease in diabetics when ABI is unreliable
This is a shared conversation. Sign in to Orris to start your own chat.