Ibs d
Reading File
Finding Sources
Searching PubMed
"irritable bowel syndrome" AND "diarrhea" AND treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of IBS-D (Irritable Bowel Syndrome with Predominant Diarrhea), based on Goldman-Cecil Medicine and Katzung's Pharmacology.
IBS-D: Overview
Definition
IBS is a functional bowel disorder characterized by chronic or recurrent abdominal pain associated with alterations in stool form and/or frequency, without structural disease to explain the symptoms. IBS-D is the subtype where loose/watery stools predominate. Using Rome IV criteria, IBS-D and IBS-mixed each account for 35-40% of all IBS cases, making them the most common subtypes.
Diagnosis - Rome IV Criteria
Recurrent abdominal pain at least 1 day/week in the last 3 months, associated with 2 or more of:
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in stool form/appearance
In IBS-D specifically: >25% of stools are loose/watery and <25% are hard/lumpy.
Red flag ("alarm") features that prompt investigation:
- Age >50 years with new-onset symptoms
- Rectal bleeding
- Unexplained weight loss
- Nocturnal symptoms that awaken the patient
- Family history of colorectal cancer or IBD
Recommended Diagnostic Tests
| Generally Recommended | Not Routinely Recommended |
|---|---|
| CBC, CRP | Colonoscopy if age <50 without alarm features |
| Fecal calprotectin/lactoferrin | Stool cultures without travel history |
| Celiac serologies (IgA anti-tTG + IgA level) | Food allergy/intolerance testing |
| Colonoscopy if new-onset symptoms at age ≥50 | Lactose or glucose hydrogen breath tests |
| Stool Giardia test (endemic areas) |
Pathophysiology
IBS-D is multifactorial - a dysregulation of gut-brain interactions producing:
- Altered motility: ~50% of IBS-D patients have accelerated colon transit; colonic motility is increased during fasting, postprandially, and with stress
- Visceral hypersensitivity: heightened perception of normal gut sensations; lower pain thresholds to balloon distension
- Mucosal barrier dysfunction: decreased tight-junction proteins in jejunum/colon, increased permeability correlating with pain severity
- Immune activation: increased colonic mast cells adjacent to sensory neurons; histamine release activates afferents
- Microbiome dysbiosis: excess Enterobacteriaceae/Lactobacillaceae/Bacteroides; reduced Faecalibacterium and Bifidobacterium
- Bile acid malabsorption: ~25% of IBS-D patients have bile acid diarrhea
- CNS changes: structural/functional brain network alterations; dysregulated HPA axis stress response
Treatment
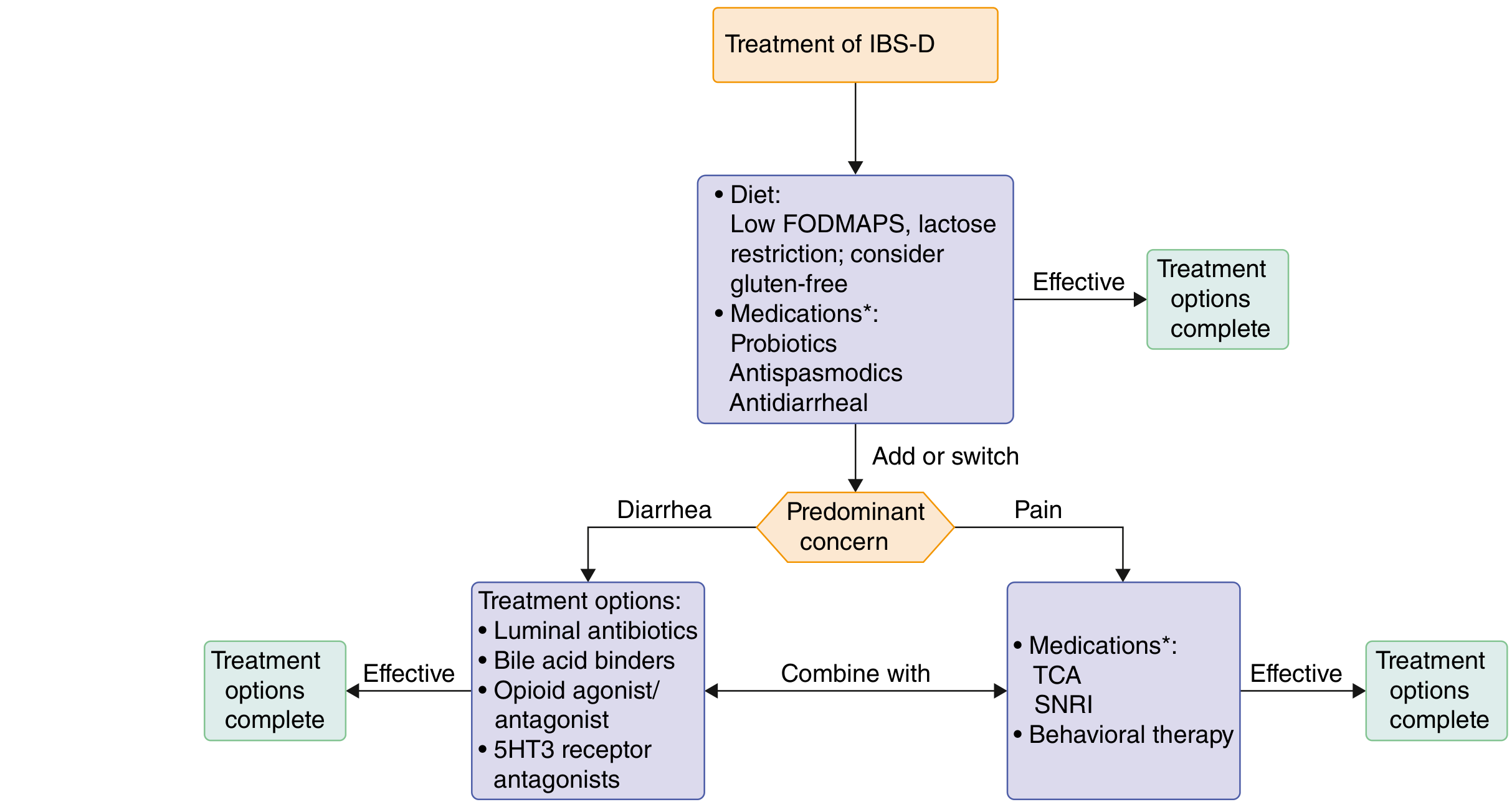
Step 1 - First-line (all IBS-D patients):
- Low-FODMAP diet - reduces fermentable carbohydrates (oligosaccharides, disaccharides, monosaccharides, polyols); effective in ~50-75% of patients
- Lactose restriction, consider gluten-free diet
- Probiotics - modest benefit for bloating/overall symptoms
- Antispasmodics (e.g., hyoscine, dicyclomine) - reduce abdominal cramping
- Loperamide - peripheral mu-opioid agonist; reduces stool frequency but does NOT improve global IBS symptoms or abdominal pain; best for patients with mild pain
Step 2 - Predominant Diarrhea:
| Drug | Mechanism | Dose | Notes |
|---|---|---|---|
| Rifaximin | Minimally absorbed broad-spectrum antibiotic; modulates microbiome | 550 mg TID x 14 days | Up to 3 retreatment courses; well tolerated |
| Eluxadoline | Mixed mu/kappa opioid agonist + delta antagonist | 100 mg BID (or 75 mg BID if intolerant) | Contraindicated without a gallbladder, hepatic impairment, biliary obstruction, pancreatic disease, alcohol use disorder |
| Bile acid sequestrants | Bind bile acids in colon | Cholestyramine, colesevelam | If bile acid diarrhea confirmed (or empiric trial) |
| Alosetron | 5-HT3 antagonist; slows GI transit, reduces visceral hypersensitivity | Restricted to women with severe IBS-D failing standard therapy (risk of ischemic colitis, serious constipation complications) |
Step 2 - Predominant Abdominal Pain:
| Drug | Mechanism | Notes |
|---|---|---|
| TCAs (e.g., amitriptyline) | Neuromodulation, slow GI transit | Low doses; good for pain + diarrhea |
| SNRIs (e.g., duloxetine) | Central pain modulation | Preferred if comorbid anxiety/depression |
Psychological/Behavioral Therapies (for persistent/severe symptoms):
- Cognitive-behavioral therapy (CBT)
- Gut-directed hypnotherapy
- Mindfulness meditation, relaxation training
- Associated with ~30% symptom reduction vs. usual care; recommended for patients with psychological distress, high avoidance behaviors, or poor pharmacotherapy response
Prognosis
- 30-45% of patients have persistent symptoms for up to 12 years
- Worse prognosis with: anxiety, negative appraisal of life events, female gender, younger age, prior anxiety/depression
Recent Evidence (2025-2026): A 2026 systematic review and meta-analysis on IBS pharmacotherapy safety (PMID 40471839) confirmed the overall safety profile of currently approved agents, without major new contraindications identified.
- Goldman-Cecil Medicine, 27th ed., pp. 1418-1421
- Katzung's Basic and Clinical Pharmacology, 16th ed.
Treatment how long we should give
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Here is a clear breakdown of treatment duration for IBS-D, organized by drug/intervention:
Treatment Duration in IBS-D
Key Principle
IBS is a chronic, relapsing-remitting condition - there is no fixed "cure" course. Treatment duration depends on:
- Severity of disease (mild 70%, moderate 25%, severe 5%)
- Type of agent used (on-demand vs. fixed course vs. long-term)
- Response to therapy - reassess at 4-8 weeks for most drugs
Drug-by-Drug Duration Guide
| Drug | Mode of Use | Duration |
|---|---|---|
| Loperamide | On-demand (as needed) | 2-4 mg per episode, max 12 mg/day; use when symptoms occur - no fixed course |
| Diphenoxylate/atropine (Lomotil) | On-demand or daily | 1-2 tabs as needed, up to 4x/day; no fixed end date |
| Rifaximin | Fixed course | 550 mg TID x 14 days (2 weeks); can repeat up to 3 retreatment courses if symptoms recur |
| Eluxadoline | Long-term/continuous | 100 mg BID - continued as long as effective and tolerated; no defined stop date |
| Alosetron | Long-term, restricted use | 0.5-1 mg BID - women with severe IBS-D only; ongoing under specialist supervision |
| Cholestyramine (bile acid binder) | Daily, long-term | 4 g with meals, start once daily, increase to TID; continued as long as needed |
| Antispasmodics (e.g., hyoscine) | On-demand or regular | Taken before meals or at symptom onset; no fixed course |
| TCAs (e.g., amitriptyline 25-75 mg) | Long-term | Start low, titrate up; minimum 3-6 months trial before judging efficacy; taper slowly when stopping |
| SNRIs (e.g., duloxetine) | Long-term | Similar to TCAs - minimum 3-6 month trial |
| Low-FODMAP diet | Phased | Phase 1 (strict restriction): 4-8 weeks → Phase 2 (reintroduction): gradual over weeks → Phase 3 (personalized long-term diet) |
| Psychological therapies (CBT, hypnotherapy) | Course-based | Typically 8-12 sessions over 2-3 months |
Practical Reassessment Timeline
Week 2: Check response to dietary changes and on-demand drugs
Week 4-8: Reassess rifaximin course; review antispasmodic/loperamide use
Week 8-12: Judge response to TCAs/SNRIs (neuromodulators need time)
Month 3-6: If persistent/severe - escalate to specialist, consider eluxadoline or alosetron
After Rifaximin - What Next?
Rifaximin is unique in IBS-D because its benefit can persist weeks after the course ends (due to microbiome rebalancing). If symptoms return, up to 3 repeat courses are approved and effective. There is no mandatory waiting period between retreatments.
Long-term Perspective
Since 30-45% of patients have symptoms for up to 12 years, many patients require:
- Intermittent on-demand drugs (loperamide, antispasmodics) indefinitely
- Periodic rifaximin retreatment courses
- Sustained dietary modifications
- Ongoing psychological support if there is significant comorbid anxiety/depression
The goal is symptom control and quality of life - not a defined "completion" date, with regular reassessment to step up or step down therapy.
- Goldman-Cecil Medicine, 27th ed., p. 1418-1421
- Harrison's Principles of Internal Medicine, 22nd ed. (2025), Table 338-4
This is a shared conversation. Sign in to Orris to start your own chat.