Hi Orris
Hey! How can I help you today?
Today i wanna learn about jaundice, teach me everything from zero to hero with simple examples make it interesting
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have comprehensive content from Harrison's, Schwartz's, Sleisenger, Robbins, Goldman-Cecil, Harper's Biochemistry, and other top textbooks. Let me compile the full "zero to hero" guide on jaundice.
🟡 Jaundice: Zero to Hero Guide
Sources: Harrison's Internal Medicine 22E, Schwartz's Principles of Surgery 11E, Sleisenger & Fordtran's GI & Liver Disease, Robbins Basic Pathology, Goldman-Cecil Medicine, Harper's Biochemistry 32E
1. What IS Jaundice? (The Simple Version)
Imagine your body as a city with a waste management system. Red blood cells (RBCs) are like buses that run their route for ~120 days and then retire. When they retire, they get broken down. That breakdown produces a yellow pigment called bilirubin - essentially "used bus parts."
The liver is the recycling plant. It processes bilirubin and flushes it out through bile into your gut, eventually leaving as the brown color of your stool.
Jaundice happens when bilirubin builds up in the blood and leaks into tissues - turning your skin, eyes (sclera), and mucous membranes yellow.
"Jaundice refers to the yellowish staining of the skin, sclera, and mucous membranes with the pigment bilirubin. Hyperbilirubinemia is usually detectable as jaundice when blood levels rise above 2.5 to 3 mg/dL."
- Schwartz's Principles of Surgery, p. 1381
The medical term for bilirubin building up in the blood is hyperbilirubinemia (hyper = too much, bilirubin = the pigment, emia = in blood).
2. Bilirubin Metabolism: The Factory Tour 🏭
Understanding jaundice = understanding bilirubin's journey through your body. Think of it as a 4-step assembly line:
Step 1 - Production (The Breakdown Plant)
- ~70-80% of bilirubin comes from old red blood cells being destroyed in the spleen
- The remaining 20-30% comes from other heme-containing proteins (cytochromes, catalase) in the liver
- A healthy adult produces about 4 mg/kg of bilirubin per day - that's almost 300 mg/day for a 70 kg person!
- At this stage, bilirubin is fat-soluble (hydrophobic) - it can't dissolve in water, so it binds to albumin (a blood protein) for transport. This form is called unconjugated (indirect) bilirubin.
Step 2 - Liver Uptake (Security Check)
- The albumin-bilirubin complex arrives at the liver
- Bilirubin separates from albumin and enters the liver cell (hepatocyte)
- Inside the hepatocyte, it binds to proteins called glutathione-S-transferases (formerly called ligandins) to prevent it from leaking back out
Step 3 - Conjugation (The Conversion Machine) ⚙️
- This is the KEY step! The enzyme UDP-glucuronosyltransferase (UGT) in the endoplasmic reticulum attaches glucuronic acid to bilirubin
- This makes bilirubin water-soluble (hydrophilic) - now called conjugated (direct) bilirubin
- Think of it like converting an oily substance into something that can dissolve in water
Step 4 - Excretion (Taking Out the Trash)
- Conjugated bilirubin is pumped from the hepatocyte into the bile via a transporter called MRP-2 (multidrug resistance protein 2)
- It travels through bile ducts → gallbladder → small intestine
- In the gut, bacteria convert it to urobilinogen, which is then further converted to stercobilin - this is what gives your stool its brown color!
- A small amount of urobilinogen gets reabsorbed, goes back to the liver, and some spills into urine as urobilin - giving urine its yellow color
3. The 3 Types of Jaundice: PRE, INTRA, POST 🚦
Now here's the beautiful clinical framework. Since jaundice results from a problem somewhere along the bilirubin assembly line, we classify it by WHERE things go wrong:
🔴 PRE-hepatic → 🟡 INTRA-hepatic → 🟢 POST-hepatic
(Before the liver) (Inside the liver) (After the liver)
🔴 Pre-hepatic (Hemolytic) Jaundice
The problem: Too much bilirubin being made, overwhelming the liver
Analogy: The recycling plant is working fine, but the city is sending 10x too much trash. The trucks can't keep up.
Causes:
- Inherited hemolytic anemias: sickle cell disease, thalassemia, hereditary spherocytosis, G6PD deficiency
- Acquired hemolytic anemias: autoimmune (positive Coombs test), mechanical hemolysis (prosthetic heart valves), malaria, transfusion reactions
- Ineffective erythropoiesis
Key lab finding: High unconjugated (indirect) bilirubin
- Stool: normal or dark (more bilirubin going through)
- Urine: NO bilirubin (unconjugated can't pass into urine - it's fat-soluble), but urobilinogen may be increased
🟡 Intra-hepatic Jaundice
The problem: The liver itself is damaged or its enzyme machinery is broken
Analogy: The recycling plant has broken equipment or is flooded.
This is the most complex category, with two subtypes:
A) Defects in Conjugation (Unconjugated hyperbilirubinemia)
| Condition | What's Wrong | Key Facts |
|---|---|---|
| Gilbert's Syndrome | Mildly reduced UGT activity (~30%) | Benign! Affects 4-7% of population. Jaundice during fasting/stress/illness only |
| Crigler-Najjar Type I | Complete absence of UGT | Severe! Neonatal. Causes kernicterus (brain damage) - often fatal without liver transplant |
| Crigler-Najjar Type II | Severely reduced UGT | Less severe than Type I. Responds to phenobarbital |
| Neonatal Jaundice | Immature UGT enzyme in newborns | Physiologic, resolves on its own; treat with phototherapy if severe |
B) Defects in Excretion (Conjugated hyperbilirubinemia)
| Condition | What's Wrong |
|---|---|
| Dubin-Johnson Syndrome | Can't excrete conjugated bilirubin (MRP2 mutation). Black liver on autopsy! |
| Rotor Syndrome | Impaired storage/re-uptake of conjugated bilirubin |
C) Hepatocellular Disease (Both fractions elevated)
- Viral hepatitis (Hep A, B, C, D, E) - most common worldwide
- Alcoholic hepatitis - chronic alcohol use
- Drug-induced: Acetaminophen overdose is the most common cause of acute liver failure from toxins
- Ischemic hepatitis - shock, heart failure, Budd-Chiari syndrome
- Cirrhosis - end-stage scarring from any chronic liver disease
- Wilson's disease - copper accumulation (think young patients + Kayser-Fleischer rings)
🟢 Post-hepatic (Obstructive/Cholestatic) Jaundice
The problem: The bile duct is blocked - bilirubin gets made and conjugated correctly, but can't get out!
Analogy: The recycling plant works perfectly but the exit door is blocked. Everything backs up.
Causes:
- Gallstones (most common) - blocking the common bile duct
- Pancreatic cancer - classic "painless jaundice" in an older patient
- Cholangiocarcinoma - bile duct cancer
- Primary sclerosing cholangitis (PSC)
- Primary biliary cholangitis (PBC)
- Strictures after surgery or inflammation
Key lab finding: High conjugated (direct) bilirubin
- Stool: pale/clay-colored (no bilirubin reaching the gut = no brown stercobilin)
- Urine: dark/tea-colored (conjugated bilirubin is water-soluble, spills into urine)
- Itching (pruritus): bile salts deposit in skin
- Elevated Alkaline Phosphatase (ALP) - the hallmark enzyme of obstruction
4. Clinical Features: How Does It Look? 👁️
The classic triad of obstructive jaundice:
- Yellow skin/eyes (icterus)
- Dark urine ("Coca-Cola colored")
- Pale/clay-colored stools
Other associated symptoms:
- Pruritus (itching) - from bile salt deposition
- Fatigue, anorexia, nausea
- Right upper quadrant pain (if gallstones)
- Fever + jaundice + RUQ pain = Charcot's Triad → cholangitis (emergency!)
- Painless jaundice in elderly + weight loss → think pancreatic cancer until proven otherwise
5. Diagnosis: Cracking the Case 🔍
Here is the actual diagnostic flowchart from Harrison's Internal Medicine 22E:
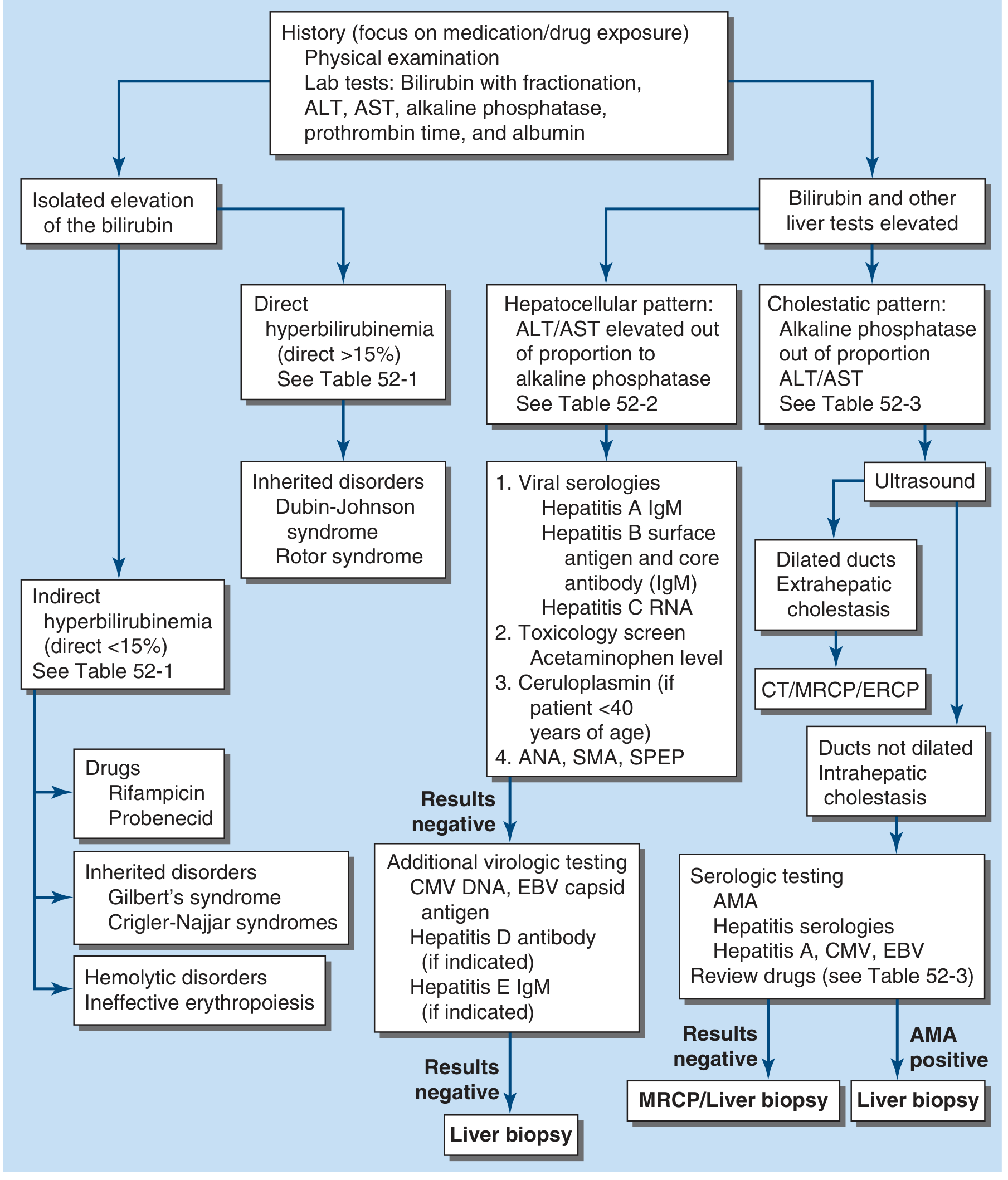
Key Lab Tests:
| Test | What it Tells You |
|---|---|
| Total bilirubin | Severity of jaundice (normal < 1 mg/dL) |
| Direct (conjugated) bilirubin | If >15% of total → direct hyperbilirubinemia |
| Indirect (unconjugated) bilirubin | Elevated in hemolysis or conjugation defects |
| ALT / AST | Hepatocellular damage markers - very high in hepatitis |
| Alkaline Phosphatase (ALP) | Cholestasis/obstruction marker |
| GGT | Also elevated in cholestasis; confirms ALP is hepatic |
| PT / INR | Liver synthetic function |
| Albumin | Chronic liver function |
The key diagnostic question: Is bilirubin predominantly conjugated or unconjugated?
- Unconjugated dominant → pre-hepatic or conjugation defect
- Conjugated dominant → excretion problem or obstruction
Imaging:
- Ultrasound (first line) - looks for dilated bile ducts, gallstones
- CT scan - better for masses (pancreatic cancer)
- MRCP - non-invasive bile duct imaging (gold standard for mapping ducts)
- ERCP - invasive but therapeutic - can remove stones, place stents
6. Special Case: Neonatal Jaundice 👶
This deserves its own section because it's so common and important.
Why do newborns get jaundice?
Three reasons hit at once:
- Newborns have fetal hemoglobin being rapidly replaced → massive bilirubin production
- The liver's UGT enzyme is immature at birth
- Gut bacteria aren't established yet → less bilirubin conversion
"The unconjugated hyperbilirubinemia of neonatal 'physiologic jaundice' results from accelerated hemolysis and an immature hepatic system for the uptake, conjugation, and secretion of bilirubin."
- Harper's Illustrated Biochemistry 32E
Physiologic jaundice appears at day 2-3 of life and resolves by day 5-7. Benign.
Pathologic jaundice appears within 24 hours - think hemolytic disease of the newborn (Rh incompatibility, ABO incompatibility).
The danger: Kernicterus 🧠
- Unconjugated bilirubin is fat-soluble and can cross the blood-brain barrier
- In newborns (immature blood-brain barrier), it deposits in the basal ganglia and brainstem
- Results in permanent brain damage: cerebral palsy, deafness, intellectual disability
Treatment:
- Phototherapy (blue light, ~460 nm wavelength): Light converts unconjugated bilirubin into water-soluble isomers that can be excreted in urine and bile WITHOUT conjugation
- Exchange transfusion in severe cases
7. Treatment: The Big Picture 💊
Treatment targets the underlying cause, not just the yellow color:
| Type | Treatment |
|---|---|
| Hemolytic jaundice | Treat the underlying hemolysis (e.g., steroids for autoimmune, avoid triggers for G6PD) |
| Gilbert's syndrome | No treatment needed - it's benign |
| Crigler-Najjar Type I | Phototherapy for ~12 hrs/day + liver transplant |
| Viral hepatitis | Supportive care (Hep A/E self-limited); antivirals for Hep B/C |
| Acetaminophen toxicity | N-acetylcysteine (NAC) - the antidote |
| Alcoholic hepatitis | Steroids (prednisolone) in severe cases, abstinence |
| Gallstone obstruction | ERCP to remove stone; cholecystectomy |
| Pancreatic cancer | Surgery (Whipple procedure) if resectable; stenting for palliation |
| Primary biliary cholangitis | Ursodeoxycholic acid (UDCA) |
| Neonatal jaundice | Phototherapy; exchange transfusion if severe |
8. Memory Trick: The Classic Comparison Table 🧠
| Feature | Pre-hepatic | Intra-hepatic | Post-hepatic |
|---|---|---|---|
| Bilirubin type | Unconjugated ↑ | Mixed ↑ | Conjugated ↑ |
| Urine color | Normal | Dark | Dark (tea) |
| Stool color | Normal/dark | Pale | Pale/clay |
| Urine bilirubin | Absent | Present | Present |
| Urobilinogen | Increased | Variable | Decreased/absent |
| ALP | Normal | Variable | Very high ↑↑ |
| ALT/AST | Normal | Very high ↑↑ | Mildly elevated |
| Pruritus | No | Sometimes | Yes (severe) |
9. Quick Summary: The One-Paragraph Version
Jaundice is yellow discoloration from bilirubin buildup, visible when serum bilirubin exceeds ~2.5 mg/dL. Bilirubin is produced from heme breakdown, transported as unconjugated (fat-soluble) bilirubin bound to albumin, conjugated in the liver to become water-soluble, and excreted in bile. Problems at any stage cause jaundice: pre-hepatic (too much bilirubin made - hemolysis) gives unconjugated hyperbilirubinemia; intra-hepatic (liver cell damage or enzyme defects) gives mixed picture; post-hepatic (bile duct obstruction - gallstones, cancer) gives conjugated hyperbilirubinemia with dark urine and pale stools. The first diagnostic step is always: conjugated or unconjugated?
That's jaundice from zero to hero! Got any specific part you want to dig deeper into - whether it's a specific genetic syndrome, the biochemistry of phototherapy, or the clinical approach to a specific scenario?
Here i didn't understand the values and terminologies like total bilirubin means, direct bilirubin value, indirect bilirubin values
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Perfect. Now I have everything needed for a crystal-clear explanation. Here it is:
🧪 Bilirubin Values Explained: Simply & Clearly
First - Where Do These Names Come From? (The Origin Story)
Back in 1916, two scientists named van den Bergh and Muller were doing a lab experiment. They mixed bilirubin in blood with a chemical called diazo reagent and watched what happened:
- Some bilirubin reacted immediately (within 30-60 seconds) → they called it "Direct" bilirubin
- Some bilirubin was slow and needed a helper chemical (alcohol) to react → they called it "Indirect" bilirubin
Later, scientists figured out WHY:
- Direct = Conjugated bilirubin (water-soluble, already processed by the liver - reacts directly with the diazo chemical)
- Indirect = Unconjugated bilirubin (fat-soluble, not yet processed - needs a helper to react)
So the names "direct" and "indirect" are literally just old lab terms that stuck around. They describe HOW the bilirubin reacted in a test tube 100+ years ago!
"The terms direct and indirect bilirubin, which correspond roughly to conjugated and unconjugated bilirubin, respectively, derive from the original van den Bergh reaction."
- Sleisenger & Fordtran's GI and Liver Disease
The Three Numbers on a Blood Report 📋
When a doctor orders a Liver Function Test (LFT), you will see three bilirubin numbers:
Total Bilirubin = Direct Bilirubin + Indirect Bilirubin
(Total) (Conjugated) (Unconjugated)
Think of it like a fruit bowl:
- Total bilirubin = all the fruit in the bowl
- Direct bilirubin = the apples
- Indirect bilirubin = the oranges
- Total = Apples + Oranges ✅
Normal Values (From the Textbook) 📊
| Bilirubin Type | Normal Range | What It Means |
|---|---|---|
| Total Bilirubin | 0.2 - 1.0 mg/dL (95% of healthy people) | All bilirubin combined |
| Indirect (Unconjugated) | Up to 0.8 - 1.2 mg/dL | Fat-soluble, not yet processed |
| Direct (Conjugated) | Up to 0.3 mg/dL | Water-soluble, processed by liver |
"Normal values of total bilirubin are between 1.0 and 1.5 mg/dL, with 95% of a normal population falling between 0.2 and 0.9 mg/dL. The most frequently reported upper limit of normal for conjugated bilirubin is 0.3 mg/dL."
- Sleisenger & Fordtran's GI and Liver Disease
Jaundice becomes VISIBLE when total bilirubin rises above ~2.5-3.0 mg/dL - that's roughly 3x the normal level. Below that, even if bilirubin is slightly elevated, your skin still looks normal.
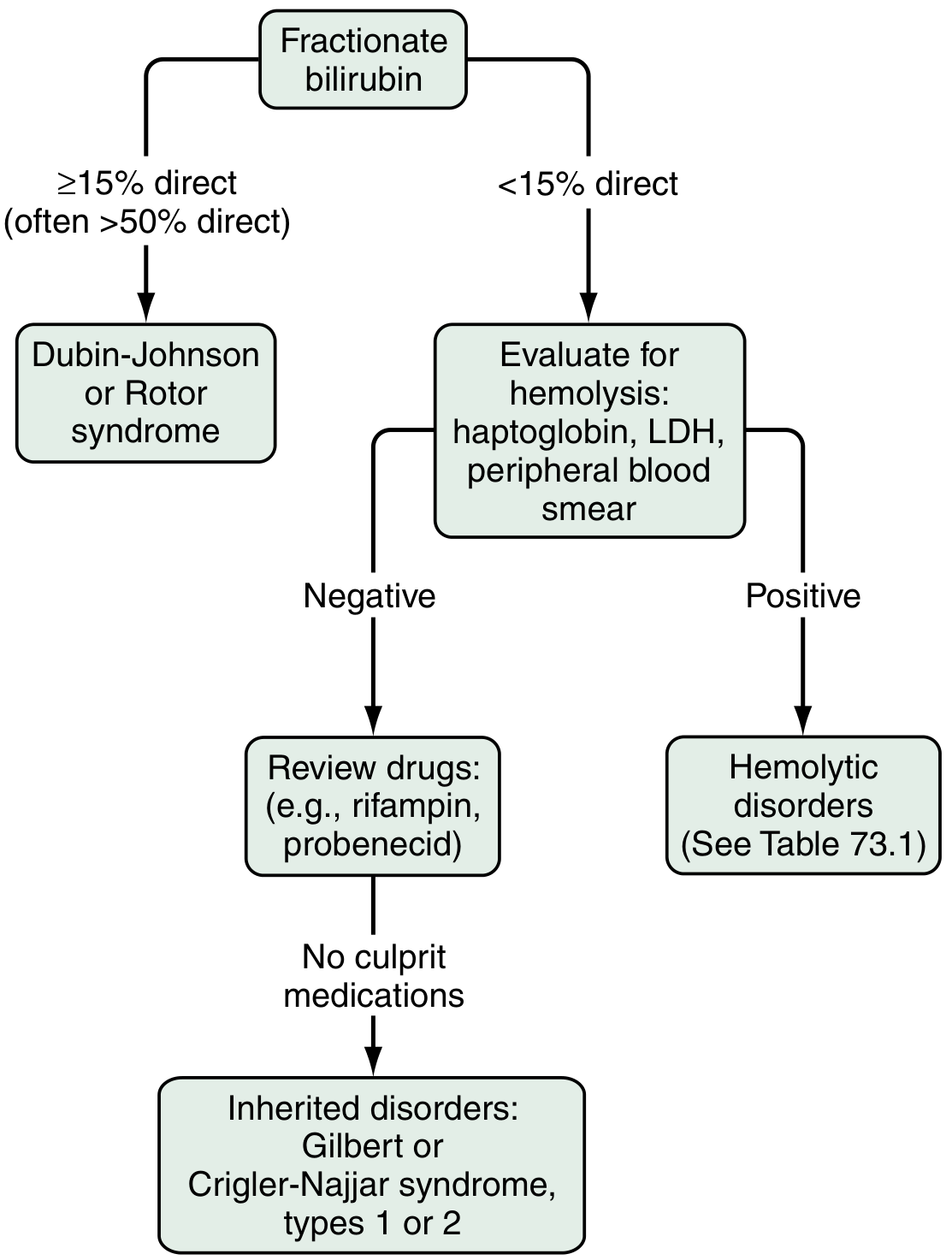
The Magic 15% Rule 🎯
Doctors use a simple trick: what percentage of total bilirubin is direct?
Direct Bilirubin
───────────────── × 100 = % Direct
Total Bilirubin
| Result | Meaning |
|---|---|
| Direct < 15% of total | Almost ALL bilirubin is indirect (unconjugated) → think PRE-hepatic (hemolysis) or liver conjugation problem |
| Direct ≥ 15% of total | Significant conjugated bilirubin → think liver disease or OBSTRUCTION |
Real example:
- Total bilirubin = 6 mg/dL, Direct = 0.6 mg/dL
- 0.6 ÷ 6 × 100 = 10% → Less than 15% → mostly indirect → likely hemolysis or Gilbert's syndrome
Another example:
- Total bilirubin = 8 mg/dL, Direct = 6 mg/dL
- 6 ÷ 8 × 100 = 75% → Way above 15% → mostly direct → likely bile duct obstruction or hepatitis
Here is the clinical flowchart from Sleisenger & Fordtran showing exactly how doctors use this:
Why Can't You See Bilirubin in Urine Normally?
This is a classic question with a beautiful answer:
-
Indirect (unconjugated) bilirubin is fat-soluble AND tightly bound to albumin (a large protein)
-
Albumin is too big to pass through the kidney filter (glomerulus)
-
So indirect bilirubin NEVER appears in urine - no matter how high it goes!
-
Direct (conjugated) bilirubin is water-soluble and NOT tightly bound
-
It CAN pass through the kidney filter
-
So dark urine = direct (conjugated) bilirubin = a sign of liver disease or obstruction
"Unconjugated bilirubin is never found in urine because in the serum it is bound to albumin and not filtered by the glomerulus. The presence of bilirubin in urine indicates conjugated hyperbilirubinemia and hepatobiliary disease."
- Sleisenger & Fordtran's GI and Liver Disease
A Bonus Term: Delta (δ) Bilirubin
There is actually a 4th type you may see mentioned:
- Delta bilirubin = conjugated bilirubin that has stuck very tightly (covalently) to albumin
- It forms when someone has been jaundiced for a long time
- Its half-life is 14-21 days (same as albumin) vs normal bilirubin's half-life of just 4 hours
- This is why some patients' jaundice seems to persist even after their liver recovers - the delta bilirubin slowly fades over weeks
The Complete Picture in One Table
| Indirect Bilirubin | Direct Bilirubin | |
|---|---|---|
| Other name | Unconjugated | Conjugated |
| Where it is | Before/in the liver (not yet processed) | After liver processing |
| Solubility | Fat-soluble (hydrophobic) | Water-soluble (hydrophilic) |
| Bound to | Albumin (tightly) | Free in plasma |
| Appears in urine? | ❌ NO | ✅ YES (dark urine) |
| Normal value | Up to 1.2 mg/dL | Up to 0.3 mg/dL |
| When elevated | Hemolysis, Gilbert's, Crigler-Najjar | Liver disease, obstruction, Dubin-Johnson |
| Why the name? | Reacted slowly/indirectly in 1916 lab test | Reacted directly/immediately |
In short: Total = Direct + Indirect, and the key question a doctor asks is "which fraction is elevated?" - that one question points you straight to the diagnosis. Does this clear it up? Want me to walk through a real lab report example?
You told a human body produce... 4 mg per deciliter of bilirubin. 1 kg.
Great catch - let me clarify that! There's a units confusion here.
The textbook said "4 mg/kg/day" - that is NOT mg per deciliter (mg/dL). Those are completely different units. Let me break it down:
What the Textbook Actually Said
"A healthy adult produces an average of 4 mg/kg of bilirubin each day"
- Sleisenger & Fordtran's GI and Liver Disease
The Two Very Different Units
| Unit | What it measures | Used for |
|---|---|---|
| mg/kg/day | How much bilirubin the BODY produces per kilogram of body weight per day | Production rate |
| mg/dL | How much bilirubin is floating in 100 mL of blood at any moment | Blood concentration |
Think of it like this:
- A factory produces 4 tonnes of waste per day → that's the production rate (mg/kg/day)
- The river nearby has 0.5 mg of pollution per litre → that's the concentration (mg/dL)
These are completely different measurements!
So How Much Does a 70 kg Person Produce Per Day?
Simple math:
4 mg/kg/day × 70 kg = 280 mg of bilirubin per day
That is roughly 280 mg produced daily - about the weight of 5-6 grains of rice.
Yet the blood concentration stays at only 0.2 - 1.0 mg/dL - because the liver is continuously processing and clearing it out as fast as it is made.
Why Does the Concentration Stay So Low?
Because the liver is an incredibly efficient recycling machine:
- Bilirubin is produced → enters blood → liver grabs it → conjugates it → excretes it into bile
- The whole process is so fast that bilirubin's half-life in blood is only about 4 hours
- So even though 280 mg is made daily, very little accumulates at any one time
Jaundice only happens when this clearing system gets overwhelmed or broken - either too much bilirubin coming in, or the liver/bile ducts can't get rid of it fast enough.
So to summarise: I said 4 mg/kg (per kg of body weight, per day) - that is the daily production rate, not a blood concentration. Blood concentration (mg/dL) is a separate measurement and is normally kept very low (under 1 mg/dL) by the liver working continuously. Good question for catching that!
Normal value of direct bilirubin percentage, and Elevated Alkaline Phosphatase (ALP) - the hallmark enzyme of obstruction....why
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Got everything I need from Sabiston's Surgery and Harrison's. Here is the full clear answer to both questions:
Two Great Questions - Answered Properly
Question 1: Normal Value of Direct Bilirubin as a Percentage
This was already covered but let me make it crystal clear with the numbers:
The Absolute Number
- Normal direct (conjugated) bilirubin = up to 0.3 mg/dL
- Normal total bilirubin = 0.2 to 1.0 mg/dL
The Percentage Rule
The percentage rule exists because the absolute value of direct bilirubin can be misleading when total bilirubin is very high. So doctors look at the proportion:
Direct Bilirubin ÷ Total Bilirubin × 100 = % Direct
| % Direct | Interpretation |
|---|---|
| < 15% | Normal proportion - almost ALL bilirubin is indirect. Pre-hepatic or conjugation problem. |
| ≥ 15% | Too much direct - liver disease or obstruction. (Often >50% in obstruction) |
Real example to feel this:
- Patient A: Total = 3 mg/dL, Direct = 0.3 mg/dL → 10% → indirect dominant → likely hemolysis
- Patient B: Total = 3 mg/dL, Direct = 2.4 mg/dL → 80% → direct dominant → likely obstruction or hepatitis
"If less than 15% of the total is conjugated, one can be assured that virtually all the serum bilirubin is unconjugated."
- Sleisenger & Fordtran's GI and Liver Disease
Question 2: Why is ALP the Hallmark of Obstruction? 🤔
This is a fantastic "WHY" question. Here is the full story:
First - What is ALP?
Alkaline Phosphatase (ALP) is an enzyme that exists in many organs:
Liver (bile duct lining cells)
Bone
Intestine
Placenta
Kidney
Leukocytes
"ALP is expressed in liver, bile ducts, bone, intestine, placenta, kidney, and leukocytes."
- Sabiston Textbook of Surgery
So ALP is NOT liver-specific. It can be raised in bone disease, pregnancy, and growing children too. But in the context of jaundice, it is the key marker of obstruction. Here is why:
The Mechanism: WHY Does Obstruction Raise ALP? 🏗️
Here is the step-by-step story - this is the part most textbooks don't explain simply:
Step 1 - Normal situation:
ALP sits quietly on the surface of bile duct cells (cholangiocytes) and liver cell membranes facing the bile. Its job is to help transport things across the membrane into bile.
Step 2 - Obstruction happens (e.g., a gallstone blocks the bile duct):
Bile can no longer flow forward. It backs up like a blocked drain. Pressure builds in the bile ducts.
Step 3 - The bile "washes back" into the liver cells:
Bile acids (the detergent-like chemicals in bile) accumulate under pressure. These bile acids are like a solvent - they strip ALP off the membrane of the bile duct cells.
Step 4 - ALP floods into the bloodstream:
The freed ALP enters the blood directly. The bile acids also stimulate liver cells to PRODUCE MORE ALP - this is the key part.
"Elevations of ALP levels in hepatobiliary diseases are generally secondary to cholestasis or biliary obstruction. Such elevations are caused by increased PRODUCTION of this enzyme."
- Sabiston Textbook of Surgery
So it is not just leakage - the body actually manufactures extra ALP in response to bile duct pressure/obstruction. That is why it shoots up so high.
How High Does ALP Go?
| Situation | ALP Level |
|---|---|
| Normal | 40 - 130 U/L (varies by lab) |
| Any liver disease (mild) | Up to 3x normal - not specific |
| Obstruction / Cholestasis | >4x normal - highly suggestive |
| Cancer infiltrating liver | Can be very high |
"Alkaline phosphatase elevations greater than four times normal occur primarily in patients with cholestatic liver disorders, infiltrative liver diseases such as cancer and amyloidosis."
- Harrison's Internal Medicine 22E
But How Do We Know the ALP is from LIVER, Not Bone?
This is a smart follow-up question. Since ALP comes from many organs, a raised ALP doesn't automatically mean liver obstruction. Doctors confirm it is hepatic by checking two other tests:
| Confirmatory Test | What it tells you |
|---|---|
| GGT (Gamma-glutamyl transferase) | GGT is raised in liver disease but NORMAL in bone disease. If ALP↑ + GGT↑ = liver source confirmed |
| 5'-Nucleotidase | Also specific to liver - elevated only in hepatic disease, not bone |
"The source of the alkaline phosphatase elevation often can be determined by measuring the gamma-glutamyl transferase (GGT), which is elevated in liver disease but normal in bone disease."
- Rheumatology, 2-Volume Set (Elsevier)
Quick example:
- Elderly woman, ALP = 400 U/L, GGT = normal → Bone source (osteoporosis, Paget's disease)
- Middle-aged man, ALP = 400 U/L, GGT = very high → Liver/bile duct source (obstruction)
Summary: ALP and Obstruction in One Picture
BILE DUCT BLOCKED
↓
Bile backs up, pressure builds
↓
Bile acids strip ALP off duct cell membranes
+
Liver cells are INDUCED to make MORE ALP
↓
ALP floods into bloodstream
↓
ALP > 4x normal on blood test
That is why ALP is the hallmark enzyme of obstruction - not because the liver cells are dying (that would raise ALT/AST), but because the PLUMBING is blocked and the duct cells respond by overproducing and releasing ALP.
This is a shared conversation. Sign in to Orris to start your own chat.