Ultrasound guided interventions for cervical pain and pros and cons of Ultrasound versus flouroscopic epidurlas
Reading File
Finding Sources
Finding Sources
Searching PubMed
ultrasound guided cervical spine injection
Searching PubMed
ultrasound versus fluoroscopy cervical epidural steroid injection
Reading File
Finding Sources
Finding Sources
Reading Article
PMID: 36650602
Reading Article
PMID: 39063975
Reading File
Finding Sources
Finding Sources
Searching PubMed
ultrasound guided cervical facet medial branch block
Reading File
Reading Article
PMID: 34934598
Reading Article
PMID: 39274505
Reading Article
PMID: 40172750
Loading Image
Finding Sources
I now have comprehensive information to write a thorough, well-cited response. Here is the full answer:
Ultrasound-Guided Interventions for Cervical Pain
Overview of Cervical Pain Sources Amenable to Injection
Cervical pain arises from several structures, each with specific injection targets:
| Pain Source | Target Structure | Intervention |
|---|---|---|
| Disc herniation / radiculopathy | Epidural space or nerve root | Cervical epidural steroid injection (ESI) or transforaminal ESI |
| Facet (zygapophyseal) joint | Joint capsule or medial branch nerves | Intra-articular injection or medial branch block (MBB) |
| Myofascial / soft tissue | Trigger points, muscles | Trigger point injections |
| Occipital neuralgia | Greater/lesser occipital nerves | Occipital nerve block |
| Cervical radiculopathy | Specific nerve root | Selective nerve root block (SNRB) |
Ultrasound-Guided Cervical Interventions
1. Cervical Facet Joint Injections and Medial Branch Blocks
Fluoroscopically guided facet joint injections have long been considered the "gold standard" for isolating or excluding the facet joint as a source of spine/extremity pain. The exact pain mechanism involves meniscoid entrapment, synovial impingement, chondromalacia, capsular inflammation, and osteoarthritis. Radiographic changes correlate poorly with pain severity. (Campbell's Operative Orthopaedics 15th Ed 2026)
Under ultrasound guidance, both intra-articular injections and medial branch blocks are now performed with increasing frequency. The sonoanatomic approach to cervical MBBs targets the articular pillar "waist" at each level (C3-C7). Each cervical facet joint (C3-4 through C7-T1) receives dual innervation from the medial branches above and below the joint, both curving consistently around the articular pillar of the same-numbered vertebra.
A 2024 systematic review of 9 studies (n=958 patients) found that US-guided cervical facet injections using the lateral approach achieve accuracy of 92-98%, with decreased procedure time and fewer needle passes compared to X-ray-guided technique. The authors concluded US-guided injections are "a safe and effective method to treat cervical facet joint syndrome, granting high functional recovery and long-lasting pain relief." However, they are strictly operator-dependent and require significant training. (PMID: 39274505)
2. Cervical Selective Nerve Root Block (SNRB)
Under ultrasound guidance, the target nerve root is visualized as it exits the neural foramen. Color Doppler is applied to identify the adjacent vertebral artery before needle placement. Precise understanding of cervical sonoanatomy - including bony landmarks (transverse processes, articular pillars), the anterior/posterior tubercle relationship, and neurovascular structures - is mandatory before attempting these procedures.
A 2024 randomized controlled trial (n=60) compared US-guided cervical SNRB vs. fluoroscopy-guided interlaminar cervical ESI for single-level disc herniation radiculopathy. At 6-month follow-up, both groups showed significant improvement in pain (NRS), disability (NDI), and quality of life (SF-36). Treatment success was 50% (US-SNRB) vs. 56.6% (FL-interlaminar ESI) - not significantly different (p=0.617). The US-guided approach had no radiation exposure and required less procedure time. (PMID: 39063975)
3. Occipital Nerve Blocks
US-guided blocks of the greater and lesser occipital nerves are among the most established ultrasound-guided cervical interventions. The occipital arteries serve as key sonographic landmarks. These are used for occipital neuralgia, cervicogenic headache, and post-traumatic neck pain.
4. Cervical Transforaminal Steroid Injection (TFSI)
A 2023 RCT (n=430) directly compared US-guided vs. CT-fluoroscopy-assisted cervical TFSI for radicular pain from disc herniation or spondylosis. Key results:
- Satisfactory contrast distribution: 92.1% (US) vs. 95.8% (CT) - non-inferior
- No significant difference in NRS or NDI improvement at 1 month or 3 months
- No permanent or severe complications in either group
- US allowed real-time visualization of critical vessels, avoiding radiation
The authors concluded US is non-inferior to CT-guided TFSI and advantageous due to vascular visualization and zero radiation. (PMID: 36650602)
5. Interlaminar Cervical Epidural Steroid Injection (IL-CESI)
The standard technique for IL-CESI uses fluoroscopy at the C7-T1 interspace (paramedian approach), with loss-of-resistance to identify the epidural space, contrast epidurogram to confirm placement, and a test dose of lidocaine before steroid injection. (Campbell's Operative Orthopaedics 15th Ed 2026)
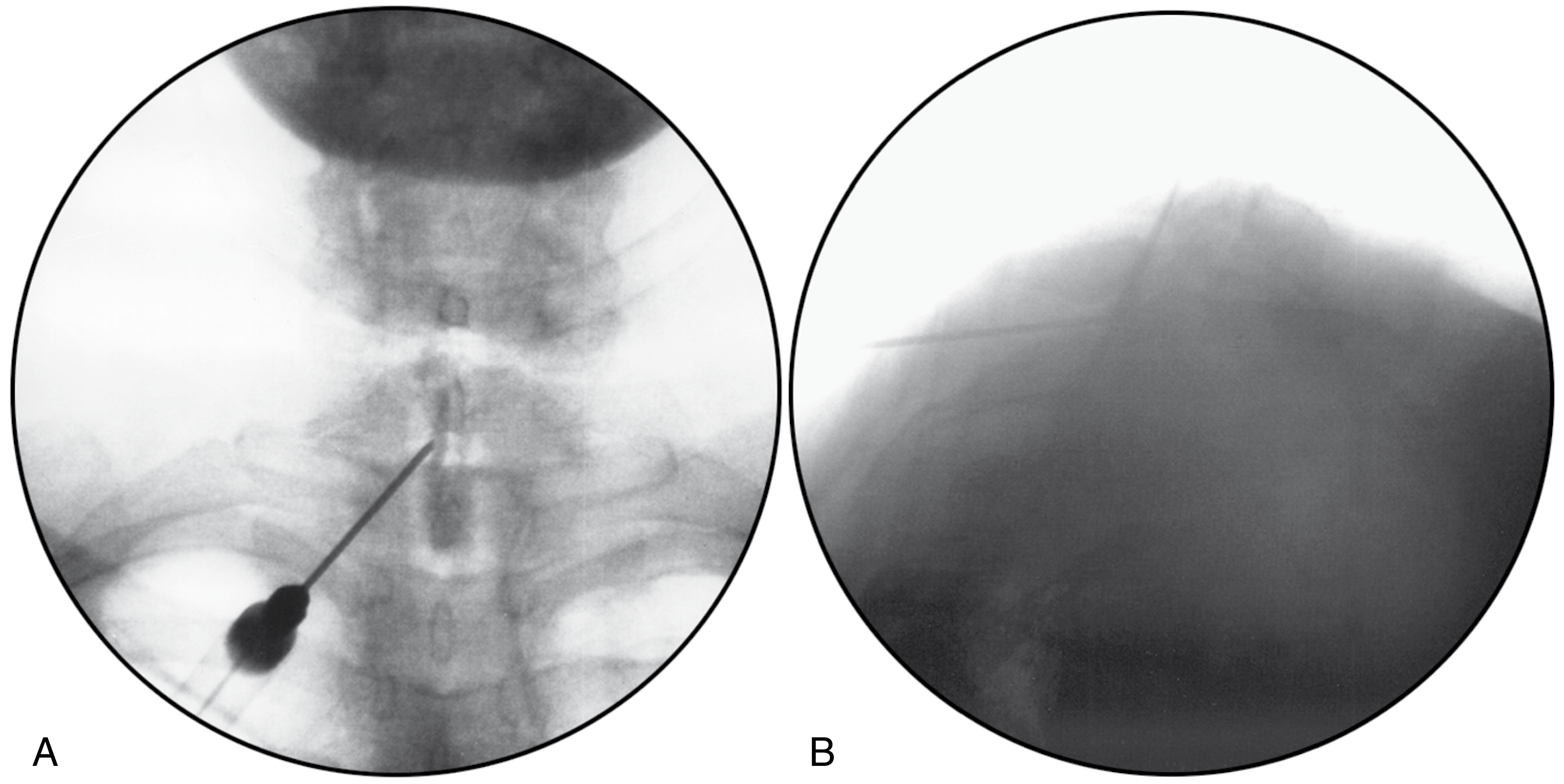
Fluoroscopic cervical interlaminar epidurogram - AP view (A) and lateral view (B) confirming C7-T1 epidural contrast spread. From Campbell's Operative Orthopaedics 15th Ed 2026.
Indications include cervical spondylosis with acute disc disruption, radiculopathies, cervical strain with myofascial pain, post-laminectomy pain, RSD, postherpetic neuralgia, and muscle contraction headaches. Reported significant pain relief in 63% of patients, with better outcomes in patients >50 years and those treated early (<100 days from diagnosis). Preoperative opioid use correlates with worse outcomes.
Ultrasound vs. Fluoroscopy for Cervical Epidural / Spinal Injections: Pros and Cons
Ultrasound Guidance
| PROS | CONS |
|---|---|
| No ionizing radiation - neither patient nor operator is exposed | Cannot visualize epidural space directly - loss-of-resistance still required for IL-ESI |
| Real-time soft tissue visualization - nerves, muscles, vessels seen in real time | Bone shadowing limits deep structure visualization; the ligamentum flavum, epidural space, and posterior disc are not well seen |
| Doppler for vascular mapping - critical for cervical procedures near vertebral artery | Operator-dependent - steep learning curve; sonoanatomy expertise mandatory |
| No contrast required for most procedures | Cannot confirm injectate spread pattern in same way fluoroscopy can with contrast epidurogram |
| Faster procedure time (shown in multiple RCTs) | Accuracy varies with level and patient body habitus |
| Portability - usable at bedside, clinic, or remote settings | Limited access to deep structures at mid-cervical levels due to bony architecture |
| Fewer needle passes in facet/MBB procedures | Not well-validated for all cervical procedures (evidence base still growing) |
| No allergic risk from contrast agents | Cannot reliably confirm epidural spread without adjunct fluoroscopy |
| Multiplanar real-time imaging of soft tissue | Equipment/probe selection critical - linear high-frequency probe needed |
| Excellent for superficial targets (occipital nerves, facet joints, MBBs) | Image quality degraded in obese or muscular patients |
Fluoroscopy Guidance
| PROS | CONS |
|---|---|
| Gold standard for epidural injections and spinal procedures | Ionizing radiation - cumulative exposure risk to patient and staff |
| Epidurogram confirms spread of injectate in real time | No soft tissue visualization - nerves, vessels, and muscles not directly seen |
| Bony landmark identification is excellent and reliable | Contrast agent required - risk of allergy, nephrotoxicity |
| Widely validated evidence base for all levels | Cannot detect intravascular injection unless real-time contrast monitoring used |
| Accurate needle tip localization at any spinal level | Requires dedicated fluoroscopy suite - not portable |
| Confirmed contrast distribution reduces missed epidural placements | Misplacement rate without imaging: up to 53% for cervical interlaminar ESI; up to 20% for cervical TFSI at cervical levels (PMID: 40172750) |
| C-arm allows multiplanar (AP, lateral, oblique) views | No vascular visualization - vertebral artery and radicular arteries invisible |
| Required for transforaminal injections where intra-arterial injection risk is highest | Requires patient transfer to fluoroscopy suite |
The Critical Safety Issue: Cervical Transforaminal Injections
Extreme caution is required for cervical transforaminal injections due to the increasing number of catastrophic neurologic complications involving spinal cord and brainstem injury. These arise from:
- Intra-arterial injection into a reinforcing radicular artery or the vertebral artery
- Intra-arterial corticosteroid injection with distal embolization
Injection into a radicular artery can be recognized by real-time monitoring of a contrast test dose - if intraarterial injection is confirmed, the procedure must be aborted immediately. (Campbell's Operative Orthopaedics 15th Ed 2026)
This risk is one of the primary reasons ultrasound - with its ability to visualize the vertebral artery in real time using Doppler - is increasingly favored for TFSI, since fluoroscopy cannot see vascular anatomy.
A comprehensive 2025 narrative review (PMID: 40172750) concluded: "Image guidance is a mandatory requirement when performing spinal procedures for pain management. Fluoroscopy enhances safety and accuracy, with stored images benefiting patient records. Ultrasound also has an increasingly important role either alone or with fluoroscopy."
Summary: Which Modality for Which Procedure?
| Procedure | Preferred Guidance | Notes |
|---|---|---|
| Cervical IL-ESI | Fluoroscopy (± US) | Epidurogram required to confirm placement |
| Cervical TFSI | Fluoroscopy or CT-fluoroscopy; US emerging | US non-inferior in RCT; vascular visualization is US advantage |
| Cervical facet intra-articular | Fluoroscopy or US | US accuracy 92-98%; fewer needle passes |
| Cervical medial branch block | Fluoroscopy or US | US increasingly used; comparable efficacy |
| Cervical SNRB | Fluoroscopy or US | US as effective as FL-guided IL-CESI in RCT; no radiation |
| Occipital nerve block | US preferred | Excellent soft tissue visualization; arteries as landmarks |
| Trigger point injections | US preferred | Real-time muscle/fascia visualization |
Key References
- Campbell's Operative Orthopaedics 15th Ed 2026 - Cervical Epidural Injection section, pp. 2286-2290
- Moreno & Barbosa (2021) - "Ultrasound-Guided Procedures in the Cervical Spine" - Cureus [PMID: 34934598]
- Yue et al. (2023) - US vs. CT-fluoroscopy TFSI RCT, n=430 - Clin J Pain [PMID: 36650602]
- Kose et al. (2024) - US-SNRB vs. FL-IL-CESI RCT, n=60 - J Pers Med [PMID: 39063975]
- Viva et al. (2024) - Systematic review of US facet injections, n=958 - J Clin Med [PMID: 39274505]
- Rekatsina & Peng (2025) - Image guidance in spine interventions - Pain Ther [PMID: 40172750]
This is a shared conversation. Sign in to Orris to start your own chat.