Explain clearly about Classify H1 Blockers (Anti – Histamines) & Mention MOA, Pharmacological Actions, Therapeutic Uses & Adverse Effects
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I have all the content needed to write a comprehensive answer. Let me now compose the full response.
H1 Blockers (Antihistamines) - Complete Review
Classification
H1 blockers are competitive antagonists at histamine H1 receptors. They are divided into two generations based on CNS penetration, selectivity, and sedative potential.
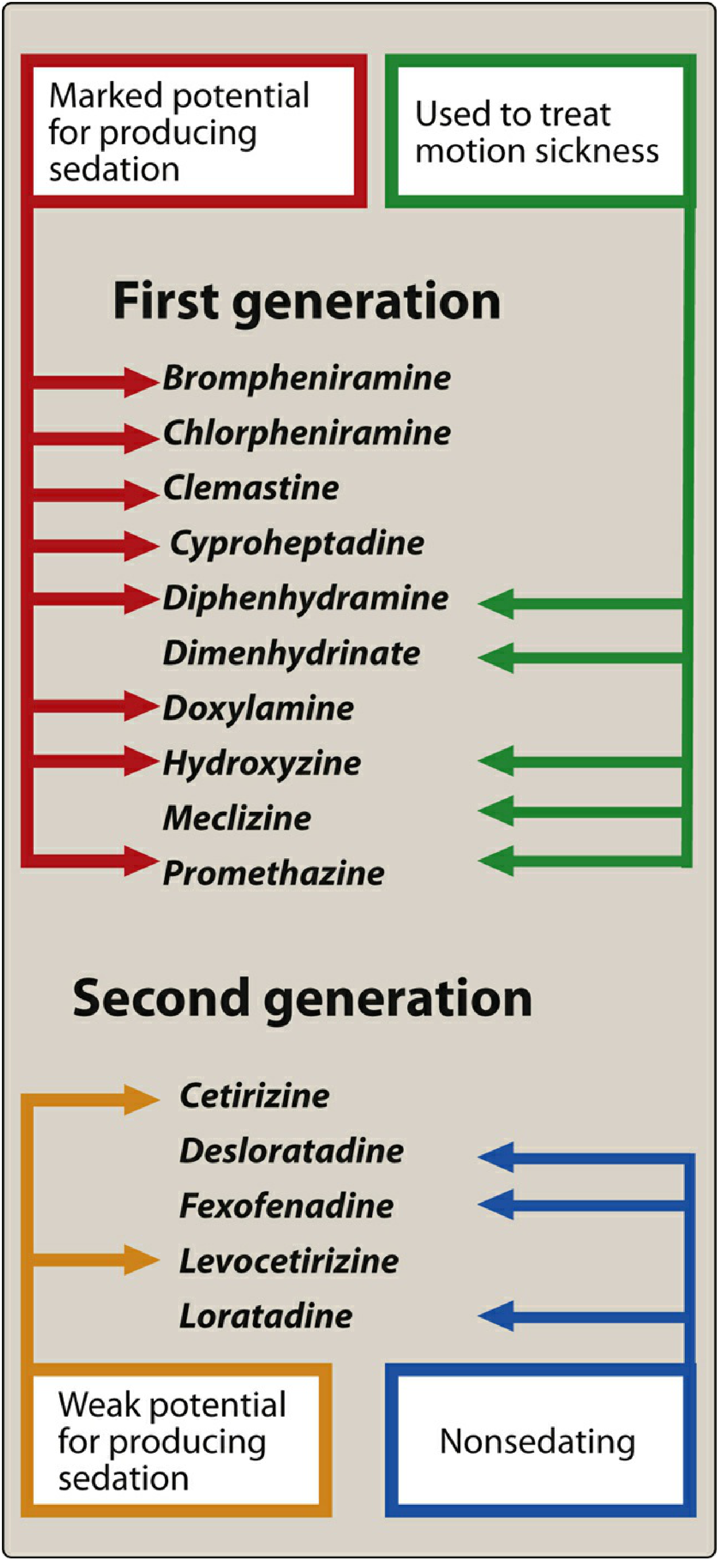
First Generation (Classical / Sedating)
These drugs cross the blood-brain barrier, cause sedation, and also block muscarinic, α-adrenergic, and serotonin receptors in addition to H1 receptors.
| Sub-class | Examples |
|---|---|
| Ethanolamines | Diphenhydramine, Dimenhydrinate, Doxylamine, Carbinoxamine |
| Ethylenediamines | Pyrilamine (Mepyramine), Tripelennamine |
| Alkylamines | Chlorpheniramine, Brompheniramine, Triprolidine |
| Piperazines | Hydroxyzine, Cyclizine, Meclizine (Meclozine), Buclizine |
| Phenothiazines | Promethazine |
| Piperidines | Cyproheptadine (also a 5-HT antagonist), Phenindamine |
| Others | Clemastine |
Key features:
- Strong CNS penetration → sedation
- Anticholinergic side effects (dry mouth, urinary retention, blurred vision)
- Short duration (4-6 hours) - require multiple daily dosing
- Useful for motion sickness, insomnia, nausea
Second Generation (Non-sedating / Peripherally Selective)
Made more polar (e.g., by adding carboxyl groups) so they do not penetrate the blood-brain barrier well. Highly selective for peripheral H1 receptors.
| Drug | Notes |
|---|---|
| Fexofenadine | Truly non-sedating; active metabolite of terfenadine |
| Loratadine | Non-sedating; hepatically metabolized |
| Desloratadine | Active metabolite of loratadine; non-sedating |
| Cetirizine | Carboxylated metabolite of hydroxyzine; mildly sedating |
| Levocetirizine | Active enantiomer of cetirizine; mildly sedating |
| Azelastine | Intranasal/ophthalmic; also has mast cell-stabilizing effect |
| Olopatadine | Ophthalmic/intranasal |
| Ketotifen | Ophthalmic; also mast cell stabilizer |
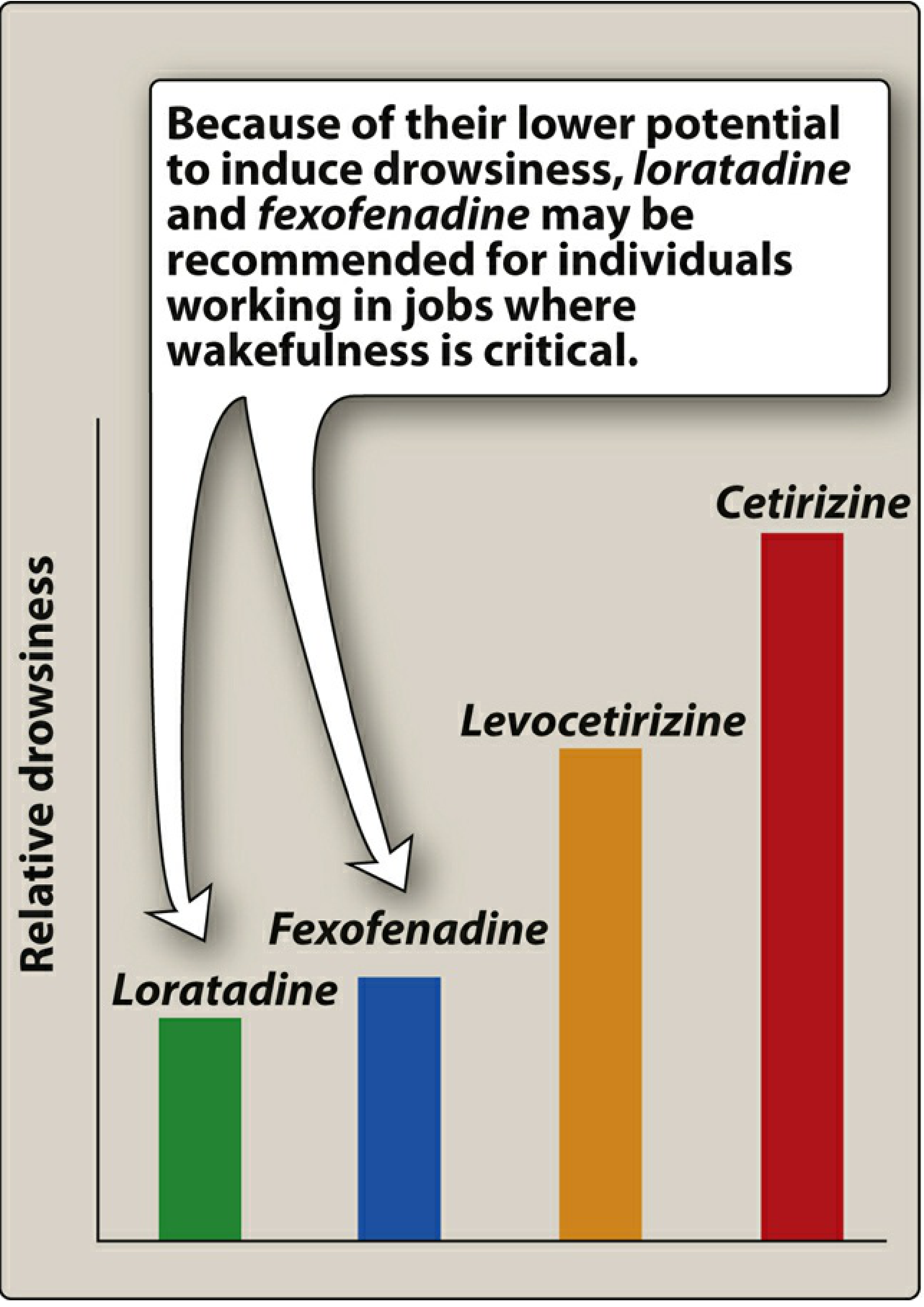
Relative drowsiness among second-generation agents (least to most): Loratadine < Fexofenadine < Levocetirizine < Cetirizine.
Mechanism of Action (MOA)
H1 blockers act as competitive, reversible antagonists at H1 receptors. They do NOT inhibit histamine synthesis or release. Instead, they:
- Block H1 receptor-mediated responses - compete with histamine at receptor sites on smooth muscle, glands, capillary endothelium, and nerve endings.
- Are more effective at prevention than reversal - they block responses before histamine binds, rather than displacing histamine already bound.
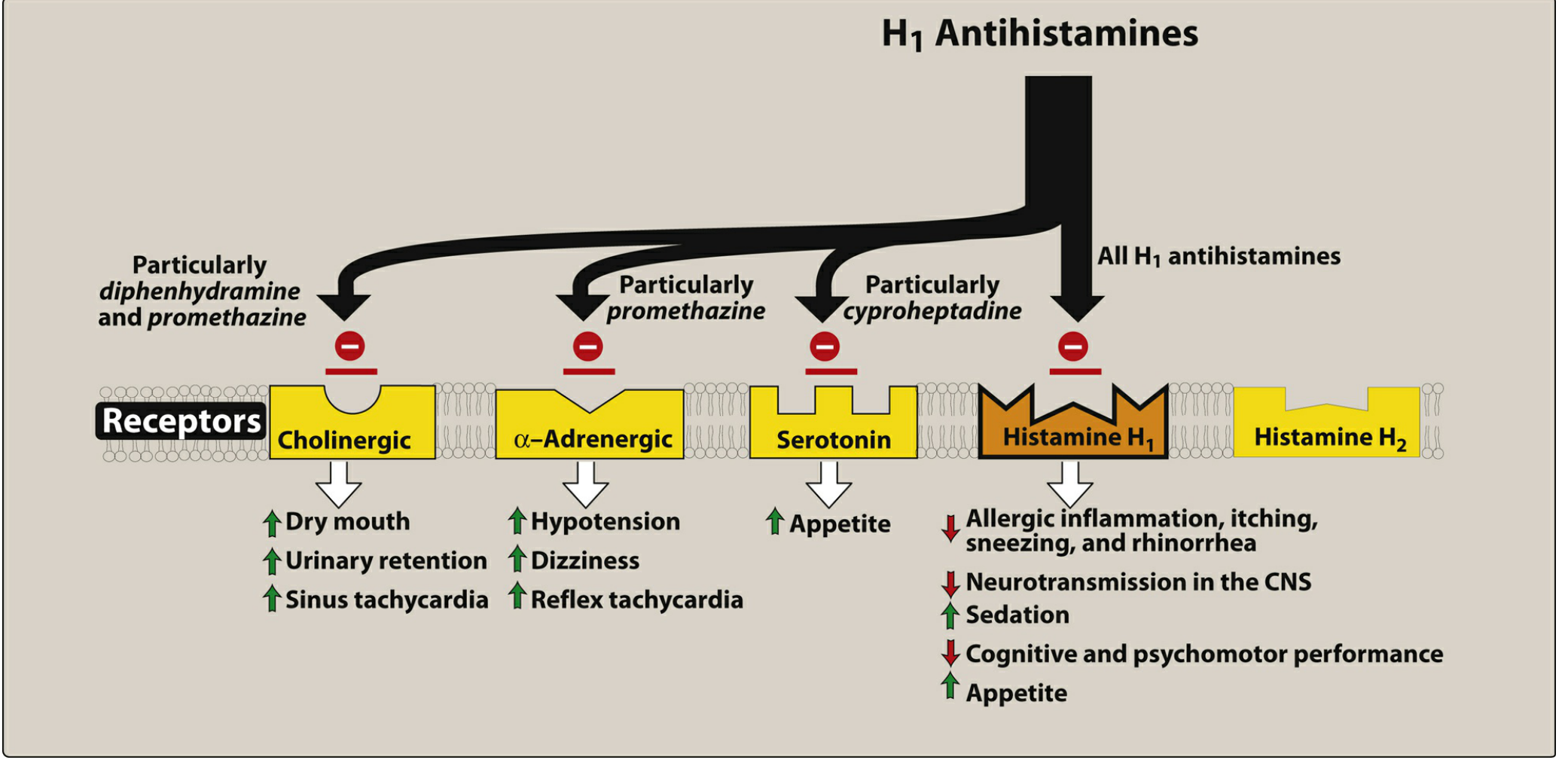
- First-generation agents additionally block:
- Muscarinic-cholinergic receptors (anticholinergic effects)
- α-adrenergic receptors (hypotension)
- Serotonin receptors (appetite stimulation - especially cyproheptadine)
- Some agents (azelastine, ketotifen) also stabilize mast cells, reducing histamine release in addition to blocking its receptor.
Pharmacological Actions
1. Antagonism of Histamine Effects
- Block histamine-induced bronchoconstriction (smooth muscle contraction) - but incomplete in asthma since leukotrienes and other mediators also contribute.
- Block histamine-induced vasodilation and increased capillary permeability (reduces wheal-and-flare).
- Block itch and pain from histamine stimulation of sensory nerve endings.
- Reduce histamine-induced gastric acid secretion only partially (H2 receptors handle most gastric secretion).
2. CNS Effects (predominantly first-generation)
- Sedation - the most common CNS effect; therapeutic in insomnia.
- Antiemetic and anti-motion-sickness effects via blockade of H1 and muscarinic receptors in the vestibular system and CTZ.
- At higher doses: paradoxical excitation, restlessness (especially in children with diphenhydramine).
- Local anesthetic action (sodium channel blockade) at very high doses.
3. Anticholinergic Effects (first-generation)
- Dry mouth, blurred vision, urinary retention, constipation, sinus tachycardia.
4. Anti-α-adrenergic Effects (especially promethazine)
- Orthostatic hypotension, reflex tachycardia, dizziness.
5. Anti-serotonin Effects (especially cyproheptadine)
- Appetite stimulation, used in management of serotonin syndrome.
6. Local Anesthetic Effect
- Diphenhydramine and promethazine have local anesthetic properties; used topically in some formulations.
Therapeutic Uses
1. Allergic and Inflammatory Conditions
- Allergic rhinitis - first-line symptomatic treatment (controls rhinorrhea, sneezing, and itching, but NOT nasal congestion). Second-generation agents preferred.
- Urticaria (hives) and angioedema - histamine is the principal mediator.
- Atopic dermatitis / contact dermatitis - relief of pruritus.
- Allergic conjunctivitis - ophthalmic formulations (azelastine, olopatadine, ketotifen).
- Anaphylaxis - adjunct only; epinephrine is the drug of choice (epinephrine opposes histamine by acting on β2 receptors to relax smooth muscle via cAMP).
- Drug and food hypersensitivity reactions.
Note: H1 blockers are NOT indicated for bronchial asthma because histamine is only one of several mediators responsible (leukotrienes, prostaglandins are also involved and not blocked by H1 antagonists).
2. Motion Sickness and Nausea/Vomiting
- Diphenhydramine, dimenhydrinate, meclizine, promethazine, hydroxyzine are effective.
- Must be given before symptoms develop (prophylactic); generally ineffective once symptoms are established.
- Second-generation agents have no value here.
3. Insomnia / Sleep Aid
- First-generation agents (diphenhydramine, doxylamine) used as OTC sleep aids.
- Doxylamine combined with pyridoxine (vitamin B6) is used for morning sickness in pregnancy (Diclegis).
4. Pruritus (Itching)
- First-generation agents (hydroxyzine, diphenhydramine) are effective for chronic pruritus, urticaria, insect bites.
5. Appetite Stimulation
- Cyproheptadine - serotonin and H1 antagonism together increase appetite; used in anorexia and cachexia.
6. Serotonin Syndrome
- Cyproheptadine can be used as adjunct management due to its anti-serotonin properties.
7. Ophthalmic/Nasal Use
- Azelastine, olopatadine, ketotifen (ophthalmic) for allergic conjunctivitis.
- Azelastine and olopatadine intranasal sprays for local effect with minimal systemic absorption.
8. Vertigo / Labyrinthine Disorders
- Meclizine, cyclizine, dimenhydrinate used for vertigo (Meniere's disease, labyrinthitis).
Adverse Effects
CNS Effects (primarily first-generation)
| Effect | Notes |
|---|---|
| Sedation/drowsiness | Most common; due to CNS H1 and muscarinic blockade |
| Fatigue, dizziness, impaired coordination | Especially in elderly |
| Cognitive impairment, psychomotor slowing | Impairs driving and operating machinery |
| Paradoxical CNS excitation | Children - restlessness, hyperactivity (esp. diphenhydramine) |
| Tremors, convulsions | At overdose |
Anticholinergic Effects (first-generation)
- Dry mouth, dry nasal passages
- Urinary retention (avoid in BPH)
- Blurred vision (cycloplegia)
- Constipation
- Sinus tachycardia
Cardiovascular Effects
- Hypotension - due to α-adrenergic blockade (especially promethazine)
- Reflex tachycardia and dizziness
- QT prolongation - a rare but serious effect seen with high-dose first-generation agents; historical terfenadine and astemizole (withdrawn second-generation agents) caused fatal arrhythmias via hERG channel blockade
GI Effects
- Nausea, vomiting, epigastric distress, anorexia (less common)
- Increased appetite and weight gain (cyproheptadine via anti-serotonin effect)
Second-Generation Specific
- Headache (most common)
- Mild sedation with cetirizine and levocetirizine
- Contact hypersensitivity with topical diphenhydramine
Teratogenicity & Pregnancy
- Doxylamine + pyridoxine - category A/safe for use in pregnancy for nausea.
- Most other antihistamines - generally avoided in first trimester when possible.
Drug Interactions
- CNS depressants (alcohol, benzodiazepines) - additive sedation with first-generation agents.
- MAO inhibitors - enhanced anticholinergic and CNS effects.
- Desloratadine and loratadine are metabolized by CYP3A4 and CYP2D6 - interactions with ketoconazole, erythromycin possible.
Quick Comparison Summary
| Feature | First Generation | Second Generation |
|---|---|---|
| CNS penetration | High | Low (polar compounds) |
| Sedation | Marked | Minimal to none |
| Receptor selectivity | Non-selective (also muscarinic, α, 5-HT) | Selective for peripheral H1 |
| Duration | 4-6 hours | 12-24 hours (once daily) |
| Motion sickness | Effective | No value |
| Sleep induction | Useful | No value |
| Anticholinergic effects | Yes | No |
| Preferred in allergic rhinitis | Less preferred | Preferred |
| Examples | Diphenhydramine, Chlorpheniramine, Promethazine | Cetirizine, Loratadine, Fexofenadine |
Sources: Lippincott Illustrated Reviews: Pharmacology, 7th Ed., Chapter 39; Katzung's Basic and Clinical Pharmacology, 16th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.