
1000392430.jpg
Csf otorrhea and csf rhinorrea
Reading File
analyse_media
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I have enough information now to provide a comprehensive answer. Let me compile the full response.
CSF Otorrhea and CSF Rhinorrhea
CT Scan Analysis
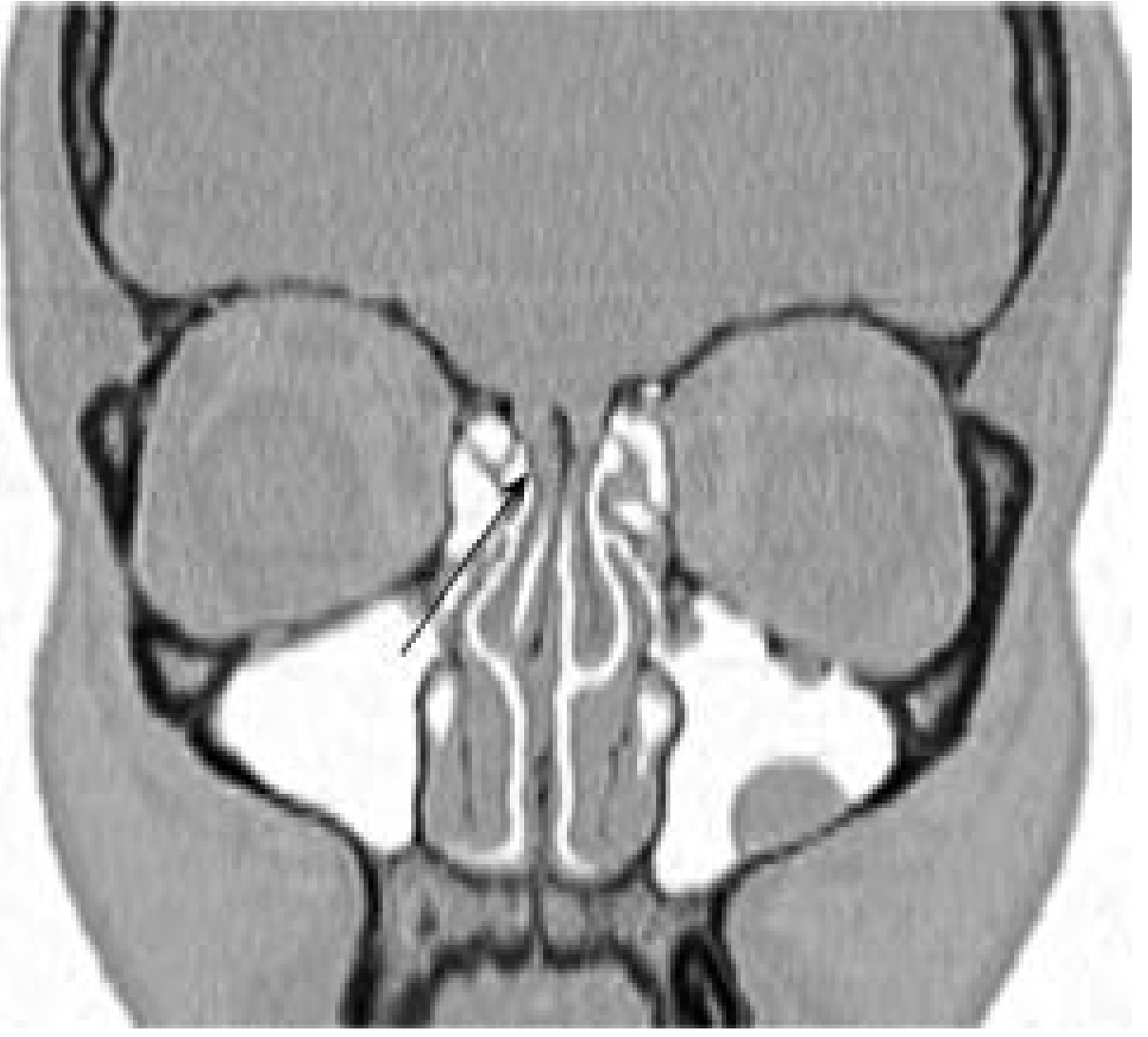
The non-contrast CT brain shown demonstrates marked ventriculomegaly (severe enlargement of lateral and third ventricles) with periventricular hypodensity, consistent with active hydrocephalus with transependymal CSF migration. There is chronic white matter ischemic disease (leukoaraiosis) bilaterally. No acute hemorrhage, midline shift, or pneumocephalus is identified on brain-window cuts. Dedicated high-resolution CT of the temporal bones/skull base with bone windows would be needed to assess for subtle fractures or tegmen defects causing CSF otorrhea/rhinorrhea. This finding of hydrocephalus is directly relevant - elevated intracranial pressure (ICP) is a known driver of nontraumatic CSF leaks.
Definitions
| Term | Definition |
|---|---|
| CSF Rhinorrhea | Communication between the CSF-containing subarachnoid space and the mucosalized space of the paranasal sinuses, resulting in CSF drainage from the nose |
| CSF Otorrhea | Leakage of CSF into the middle ear/external auditory canal, typically via a defect in the tegmen tympani or temporal bone |
Classification of CSF Rhinorrhea (Box 48.1, Cummings Otolaryngology)
I. TRAUMATIC
- A. Accidental
-
- Immediate (at time of injury)
-
- Delayed
-
- B. Surgical
- Complication of neurosurgical procedures: transsphenoidal hypophysectomy, frontal craniotomy, other skull base procedures
- Complication of rhinologic procedures: sinus surgery (FESS), septoplasty, other combined skull base procedures
II. NONTRAUMATIC
- A. Elevated ICP
- Intracranial neoplasm
- Hydrocephalus (noncommunicating or obstructive)
- Benign intracranial hypertension (BIH / pseudotumor cerebri)
- B. Normal ICP
- Congenital anomaly
- Skull base neoplasm (nasopharyngeal carcinoma, sinonasal tumors)
- Skull base erosive process (osteomyelitis, granulomatosis with polyangiitis, sinus mucosa erosion)
- Idiopathic
Epidemiology: ~80% of CSF rhinorrhea cases are traumatic. Only 4% are nontraumatic. Skull base fracture carries a 12-30% risk of CSF fistula. CSF rhinorrhea occurs in 2-3% of serious head trauma.
Pathophysiology
CSF dynamics: CSF is produced by the choroid plexus at 20 mL/hour in adults. Total volume is ~140 mL (20 mL ventricles, 50 mL intracranial subarachnoid space, 70 mL paraspinal). Normal ICP is up to 14 cm H2O in adults.
For a CSF leak to occur, two conditions must be met:
- A physical defect (disruption of bone + dura + mucosa) separating subarachnoid space from the sinus/ear
- A pressure gradient driving CSF outward
Key anatomic weak points:
- The lateral lamella of the cribriform plate (LLCP) is the weakest part of the skull base and most vulnerable to iatrogenic injury during FESS
- The tegmen tympani (roof of middle ear) - thin bone separating middle cranial fossa from middle ear
- Congenital dehiscence of the lateral sphenoid roof (Sternberg canal)
Nontraumatic mechanism: Elevated ICP (from BIH, hydrocephalus, or idiopathic) + constant dural pulsations erode weakened bone over time. Notably, 72-100% of patients with apparently spontaneous CSF rhinorrhea have underlying elevated ICP, and 100% of spontaneous leak patients in one series had empty sella syndrome (marker of elevated ICP). Mean ICP in these patients was 26.5-32.5 cm H2O (well above normal).
Clinical Presentation
CSF Rhinorrhea:
- Unilateral watery nasal discharge (clear, salty/metallic taste)
- Often posture-dependent or worsened by Valsalva maneuver
- History of head trauma, skull base surgery, or features of raised ICP
- In BIH-related cases: severe diffuse headache that paradoxically improves when rhinorrhea occurs and worsens when it stops (the leak acts as a pressure release valve)
CSF Otorrhea:
- Clear, copious, watery ear discharge
- May be pulsatile
- Occurs with Valsalva maneuver or positions that raise ICP
- History of head trauma, temporal bone surgery, or spontaneous
- Associated signs: hemotympanum, Battle's sign (mastoid ecchymosis), raccoon eyes - all suggest basilar skull fracture
Differential algorithm for otorrhea:
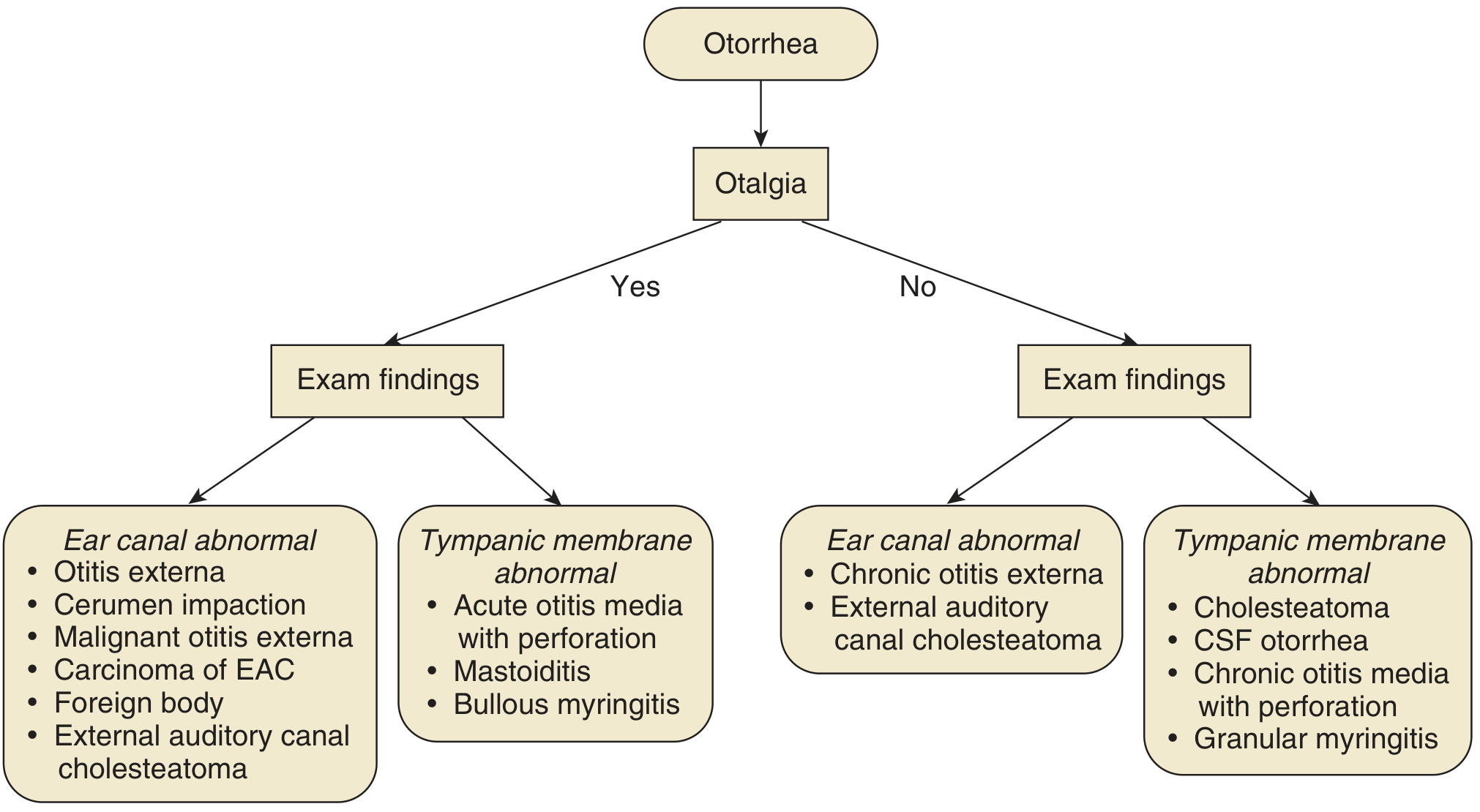
Rule out CSF otorrhea in:
- Copious watery otorrhea after ventilation tube placement
- Pulsatile clear copious otorrhea at time of tube placement
Diagnosis
| Test | Details |
|---|---|
| Beta-2 transferrin | Gold standard biochemical test - highly specific for CSF (not found in nasal secretions, saliva, tears, or serum). Confirms CSF leak. |
| Beta-trace protein | Alternative biochemical marker - simpler assay, comparable sensitivity |
| "Halo sign" | Blood-stained fluid on filter paper forms outer ring of CSF - unreliable, not diagnostic |
| Glucose testing | Unreliable - nasal secretions can contain glucose; poor specificity |
| CT Cisternography | Lumbar intrathecal contrast + CT; requires active leak; excellent spatial resolution for localization |
| MR Cisternography | No LP required; specific MRI protocols; good for active leaks; detects meningoceles |
| Radionuclide cisternography | Requires LP + intrathecal tracer; poor spatial resolution; now less preferred |
| Intrathecal fluorescein | Endoscopic use; confirms leak intraoperatively and localizes site; dilute dose mandatory (serious neurologic sequelae at higher doses) |
| HRCT temporal bone | For CSF otorrhea: evaluates tegmen tympani defects, temporal bone fractures |
| HRCT skull base (bone windows) | Evaluates cribriform plate, sphenoid, ethmoid bony defects |
Complications
- Meningitis - most feared; recurrent bacterial meningitis should always prompt evaluation for CSF leak (especially S. pneumoniae in children)
- Pneumocephalus - air enters through the skull base defect; can cause brain compression
- Ascending intracranial infection (encephalitis, abscess)
Management
Conservative (traumatic leaks):
- Bed rest + head elevation
- Avoid Valsalva, nose blowing, sneezing
- Most traumatic temporal bone fracture-related CSF leaks resolve within 5-7 days spontaneously
- If persists >7 days: lumbar drain
- If persists after 5-7 days of lumbar drainage: surgical repair
Surgical (endoscopic - now preferred standard):
- Endoscopic transnasal repair is the standard for CSF rhinorrhea with >90% success rates
- Steps: identify defect, close with autogenous graft (fascia, free bone, fat), allograft (acellular dermal), or xenogeneic collagen dural substitute; overlay free mucosal graft; secure with surgical sealant and packing
- High-flow leaks/large defects: consider vascularized mucosal flaps
- Replaced older intracranial approaches (bifrontal craniotomy - high failure rates up to 27%)
For CSF otorrhea (spontaneous tegmen defects):
- Transmastoid approach: effective for posterior tegmen defects
- Middle fossa approach: for large defects (>1.5 cm) or defects anterior to the epitympanum
- Repair uses fascia/perichondrium + cartilage or bone
Nontraumatic/idiopathic leaks:
- Unlikely to resolve spontaneously - operative repair warranted after excluding neoplasm
- Must address elevated ICP (weight loss, acetazolamide, or LP shunting) to prevent recurrence
- CSF diversion (lumbar drain) may be considered postoperatively in suspected elevated ICP
- Routine postoperative lumbar drains not confirmed beneficial in studies
Connecting the CT to CSF Leak Pathophysiology
The hydrocephalus seen on this patient's CT scan is a direct cause of elevated ICP, which is one of the primary nontraumatic mechanisms for CSF rhinorrhea and otorrhea. Elevated ICP leads to constant CSF pulsations against the skull base, eroding natural bony weak points (cribriform plate, tegmen tympani, lateral sphenoid recess) and eventually producing a dural defect and CSF fistula. If this patient presents with clear nasal or ear discharge, a CSF leak from raised ICP due to hydrocephalus should be strongly suspected. Treatment must address both the leak site (surgical repair) and the underlying hydrocephalus (VP shunt), or the leak will recur.
Sources: Cummings Otolaryngology Head and Neck Surgery (9780323612173); Shambaugh Surgery of the Ear (9781607950264)
Can evd done in this case
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I have enough information from the textbooks and clinical knowledge to give a complete, well-structured answer.
Can EVD Be Done in This Case?
Short answer: Yes - an EVD (External Ventricular Drain) is both feasible and potentially indicated in this case, with important caveats.
What the CT Shows (Recap)
The CT demonstrates marked ventriculomegaly (grossly enlarged lateral ventricles, dilated temporal horns, rounded frontal horns) with periventricular hypodensity (transependymal CSF migration) - indicating active, high-pressure hydrocephalus. This is the primary pathology driving the elevated ICP, which in turn drives the CSF leak (rhinorrhea/otorrhea).
What is an EVD?
An EVD (ventriculostomy) involves inserting a perforated plastic catheter into the frontal horn of the lateral ventricle via a burr hole, typically in the right frontal region. It:
- Monitors ICP continuously via a fluid column transducer
- Drains CSF to reduce ICP
- Allows CSF sampling for laboratory analysis
(Schwartz's Principles of Surgery, 11th Ed.)
Indications for EVD - Does This Case Qualify?
| Criterion | This Case |
|---|---|
| Hydrocephalus with raised ICP | YES - marked ventriculomegaly + transependymal flow |
| Active CSF leak (rhinorrhea/otorrhea) needing ICP reduction | YES - elevated ICP perpetuates the leak |
| Emergency CSF diversion needed | YES - if symptomatic with declining neurological status |
| Temporary measure before definitive surgery | YES - EVD as bridge to VP shunt or endoscopic repair |
Per Bailey & Love's Short Practice of Surgery (28th Ed.):
"Temporary CSF diversion can be achieved with an EVD. In the long term a shunt, usually connecting the lateral ventricles with the peritoneal cavity (ventriculoperitoneal shunt), is the mainstay of management."
Why EVD is Particularly Relevant Here
-
Breaks the cycle of CSF leak: Elevated ICP drives CSF through the skull base defect. By draining CSF externally, the EVD reduces the pressure gradient that is forcing CSF out - directly treating the rhinorrhea/otorrhea at its root cause.
-
Temporizing before definitive repair: The skull base defect causing the leak cannot be safely repaired endoscopically while ICP remains grossly elevated, as the repair would fail under continued pressure. EVD normalizes ICP first.
-
Acute/emergency access: EVD is faster to place than a VP shunt, especially in an acute setting or before full workup.
-
ICP monitoring: Allows measurement of real-time ICP - important because the opening pressure may be falsely normal during an active leak (the leak decompresses ICP transiently).
EVD vs. Lumbar Drain in CSF Leaks
| Feature | EVD | Lumbar Drain |
|---|---|---|
| Drains from | Ventricle (source) | Lumbar subarachnoid space |
| Preferred when | Obstructive hydrocephalus, gross ventriculomegaly, acute decompensation | Communicating hydrocephalus, moderate elevated ICP, post-op CSF leak management |
| ICP monitoring | Yes (continuous) | No |
| Risk | Ventriculitis, hemorrhage, catheter blockage | Headache, infection, over-drainage |
| This case | Preferred (gross ventriculomegaly suggests possible obstruction) | Risky if obstructive component exists |
Important: A lumbar drain is contraindicated or dangerous if there is an obstructive component to the hydrocephalus (non-communicating), as it can precipitate downward herniation. Given the marked ventriculomegaly seen here, EVD is the safer CSF diversion option until the nature of the hydrocephalus (communicating vs. obstructive) is confirmed.
Precautions / Contraindications to Consider
- Coagulopathy - must correct before insertion (INR <1.4, platelets >80,000)
- Overlying scalp infection - would require alternative access site
- Collapsed/slit ventricles - not relevant here (ventricles are large, easy targets)
- Active meningitis - an EVD can still be placed but antibiotic cover is mandatory; note that CSF otorrhea/rhinorrhea significantly raises meningitis risk
- Thrombocytopenia or anticoagulation - require correction first
Definitive Long-Term Management
EVD is a temporary measure. This patient will ultimately need:
- VP shunt (ventriculoperitoneal shunt) - long-term definitive treatment for hydrocephalus
- Endoscopic third ventriculostomy (ETV) - if obstruction is at the aqueduct level (avoids implanted hardware, no infection risk from tubing)
- Endoscopic skull base repair of the CSF fistula - once ICP is controlled
- Treatment of underlying cause of hydrocephalus (if identifiable - tumor, aqueduct stenosis, etc.)
Summary
Yes, EVD is indicated and appropriate in this case. The CT shows gross hydrocephalus with active transependymal flow - a neurosurgical urgency. EVD:
- Immediately reduces ICP
- Stops driving CSF through the skull base leak
- Allows ICP monitoring
- Serves as a bridge to definitive VP shunt and/or skull base repair
- Is safer than lumbar drain when obstructive hydrocephalus cannot be excluded
The correct sequence is: EVD (acute) → Investigate cause of hydrocephalus → VP shunt or ETV (definitive) → Endoscopic repair of CSF fistula once ICP controlled.
Sources: Schwartz's Principles of Surgery, 11th Ed.; Bailey & Love's Short Practice of Surgery, 28th Ed.; Cummings Otolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.