Cardiopulmonary bypass
Reading File
Finding Sources
Searching PubMed
"cardiopulmonary bypass" complications management
Cardiopulmonary bypass anaesthetic implications
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cardiopulmonary bypass" anaesthesia complications
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of cardiopulmonary bypass (CPB) and its anaesthetic implications, drawn from Miller's Anesthesia (10e), Morgan & Mikhail's Clinical Anesthesiology (7e), and Barash's Clinical Anesthesia (9e).
Cardiopulmonary Bypass: Anaesthetic Implications
1. The CPB Circuit - What the Anaesthetist Needs to Know
CPB diverts venous blood from the right atrium (via one or two cannulae in the RA, SVC/IVC, or femoral vein), oxygenates and ventilates it through a membrane oxygenator, and returns it via an arterial cannula - usually in the ascending aorta. This produces a completely non-physiological state: non-pulsatile flow, reduced mean arterial pressure, haemodilution, hypothermia, and a systemic inflammatory response.
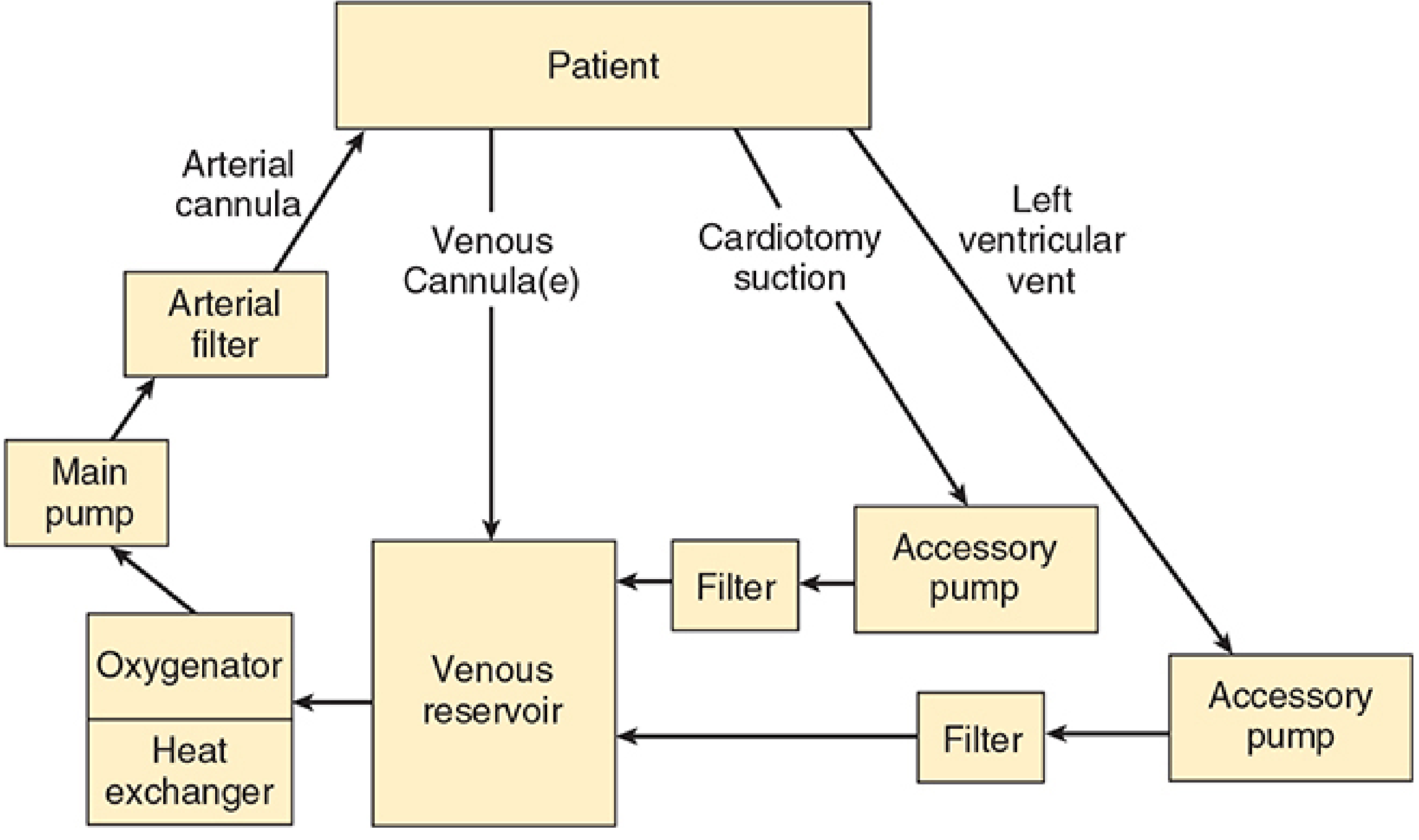
Basic design of the cardiopulmonary bypass circuit - Morgan & Mikhail's Clinical Anesthesiology, 7e
The five goals of CPB from the anaesthetist's perspective (Barash 9e):
- Provide a bloodless, motionless surgical field
- Oxygenate and ventilate
- Maintain organ perfusion and oxygen delivery
- Manage temperature (cooling for organ protection, rewarming prior to weaning)
- Provide inhalational or intravenous anaesthesia
2. Preoperative Considerations
Patient Assessment
- Focus on functional status, LV/RV function, valvular lesions, pulmonary pressures, renal function, and coagulation status
- Identify medications: antiplatelet agents (aspirin, clopidogrel), anticoagulants, beta-blockers, ACE inhibitors
- ACE inhibitors/ARBs are associated with vasoplegic syndrome post-CPB and some centres hold them preoperatively
Premedication
- Anxiolysis is important - cardiac patients are often highly anxious
- Benzodiazepines (e.g., midazolam 0.02-0.05 mg/kg IV/IM) are commonly used
- Cardiac medications should generally be continued up to the day of surgery
Haemodynamic Goals Pre-CPB
The pre-CPB period is when most ischaemic events occur. For coronary artery disease patients (Barash 9e):
- Control heart rate - tachycardia is the primary driver of increased MVO2
- Avoid hypotension (compromises coronary perfusion pressure)
- Avoid hypertension (increases wall stress and MVO2)
- Prevent LV distension
3. Monitoring
Monitoring requirements are extensive:
| Monitor | Notes |
|---|---|
| Arterial line | Always placed pre- or immediately post-induction. Radial artery preferred, but may give falsely low readings after sternal retraction (subclavian compression) or early after CPB (AV shunt opening during rewarming). Have a backup non-invasive cuff. |
| Central venous line | Right internal jugular preferred ("straight shot" to RA). CVP trends useful; isolated values less so. |
| Pulmonary artery catheter | Use is declining - reserve for reduced LV function, pulmonary hypertension, transplant. Must be withdrawn 2-3 cm during CPB as it migrates distally and can spontaneously wedge, causing fatal PA rupture on balloon inflation. |
| TOE (transoesophageal echocardiography) | Now standard. Invaluable for assessing ventricular filling, function, valve repair adequacy, detection of air, and weaning from bypass. |
| Temperature | Multiple sites: bladder/rectal (peripheral), oesophageal/nasopharyngeal (core), PA blood temperature. A gradient of >10°C between blood and brain during rewarming risks neurological injury (cerebral hyperthermia). |
| Urine output | Catheter inserted after induction. Reddish urine = haemolysis from CPB or transfusion reaction. |
| Cerebral oximetry (NIRS) | Increasingly used to detect cerebral desaturation during CPB. |
| ACT (Activated Clotting Time) | Point-of-care test to monitor heparin anticoagulation. ACT must be >400-480 seconds before initiating CPB. |
4. Anticoagulation
This is one of the most safety-critical aspects of CPB anaesthetic management.
- Heparin is given IV (typically 300-400 units/kg) before cannulation to prevent clotting in the extracorporeal circuit
- ACT target: >400-480 seconds before initiating CPB (some centres target >480 s)
- The APT is infinitely prolonged at these doses, so ACT (not aPTT) is used to monitor
- ACT is checked every 30-60 minutes on bypass and additional heparin given if needed
- Heparin resistance (ACT fails to reach target despite adequate dosing) - causes include antithrombin III deficiency, prior heparin infusion, or thrombocytosis. Treatment: antithrombin III concentrate or fresh frozen plasma
- At completion of CPB, protamine is given to reverse heparin (typically 1 mg per 100 units of heparin given). Risks of protamine: hypotension, pulmonary hypertension, anaphylaxis (especially in patients with prior protamine/NPH insulin exposure or fish allergy)
5. Pharmacokinetics on CPB - Drug Management
CPB causes profound changes in drug pharmacokinetics due to:
- Haemodilution from the pump prime (1200-1800 mL in adults) - lowers plasma protein concentrations and drug concentrations
- Hypothermia - reduces enzymatic metabolism and clearance
- Altered protein binding - pH changes and dilution of albumin/AAG affect free drug fractions
- Drug sequestration in the CPB circuit itself (tubing, oxygenator)
- Altered organ blood flow - reduced renal and hepatic perfusion
Key drug effects (Miller's 10e):
| Drug | CPB Effect |
|---|---|
| Fentanyl | Total concentration decreases at onset of CPB; unbound fraction rises. Concentration increases at rewarming. Population PK modelling shows the effect is clinically insignificant; a 3-compartment model predicts concentrations throughout. |
| Alfentanil | Prolonged elimination due to increased Vdss; central compartment volume significantly increased. Elimination t½β unchanged. |
| Remifentanil | Normothermic CPB - minimal effect on clearance. Hypothermic CPB reduces clearance ~20% (temperature effect on blood/tissue esterases). Volume of distribution increases 86% at initiation of CPB. Still short-acting even on CPB. |
| Propofol | Blood levels drop on initiation of CPB due to dilution. TIVA with propofol is commonly used. Adequate plasma levels must be maintained to prevent awareness. |
| Volatile agents | Delivered via a vaporiser attached to the oxygenator gas line. Concentration may be difficult to predict. Potent myocardial preconditioning effect (reduces infarct size and reperfusion injury). |
| Muscle relaxants | Non-depolarising agents may have prolonged action due to reduced hepatic/renal flow and hypothermia. |
Awareness on bypass is a genuine risk. The anaesthetist must ensure adequate anaesthetic delivery is maintained throughout CPB - either via volatile agent through the oxygenator or TIVA infusion. Depth of anaesthesia monitoring (BIS, entropy) is therefore valuable.
6. Physiological Changes on CPB
Haemodynamic
- MAP typically 50-80 mmHg (mean of ~60 mmHg) maintained with vasoconstrictors (phenylephrine, noradrenaline) or vasodilators (GTN, SNP) as needed
- Flow rate typically 2.2-2.4 L/min/m² (higher in children)
- Non-pulsatile flow - reduces shear stress-mediated NO production, may impair microcirculation
Temperature
- Mild hypothermia (32-34°C) - reduces metabolic rate, provides some organ protection
- Moderate hypothermia (25-32°C) - more protection, longer safe circulatory arrest times
- Deep hypothermic circulatory arrest (DHCA) - core temp 15-18°C, allows up to 60 min of complete arrest (used in aortic arch surgery, complex congenital cases)
- pH management: Alpha-stat (uncorrected for temperature, preferred in adults - maintains cerebral autoregulation) vs pH-stat (corrected for temperature, may be preferred in children undergoing DHCA for better cerebral cooling)
Haematological
- Haemodilution: hematocrit falls to ~22-27% at onset of CPB with crystalloid prime
- Acceptable haematocrit on CPB: generally 21-25% in adults (lower in hypothermia due to increased oxygen solubility and reduced demand)
- Blood is added to prime for neonates and infants (circuit volume is ~3x blood volume)
- Coagulopathy after CPB: dilution of clotting factors and platelets, platelet dysfunction, residual heparin effect, fibrinolysis. Treatment: protamine, FFP, platelets, cryoprecipitate, tranexamic acid/aminocaproic acid
Inflammatory Response
- CPB triggers a systemic inflammatory response (complement activation, cytokine release, neutrophil activation) due to contact of blood with the artificial circuit
- Magnitude correlates with bypass duration
- Contributes to post-CPB organ dysfunction (lung injury, cognitive impairment, renal impairment)
- Management: steroids (methylprednisolone) in selected cases (especially paediatric), leucocyte-depleting filters, miniaturised circuits, biocompatible circuit coatings
7. Weaning from CPB
This is the most demanding phase for the anaesthetist. Criteria before attempting to wean:
- Core temperature >36°C (nasopharyngeal/bladder)
- Sinus rhythm or paced rhythm at acceptable rate
- Adequate haematocrit (>21-25%)
- Electrolyte correction (especially K⁺, Ca²⁺, Mg²⁺)
- Adequate ventilation resumed (lungs re-expanded)
- Metabolic acidosis addressed
- TOE assessment of ventricular function and volume status
Weaning Process
Gradual reduction of CPB flow while venous drainage is progressively clamped, allowing the heart to fill. The anaesthetist must be ready to rapidly administer:
Inotropes/vasopressors (titrated based on TOE and haemodynamics):
- Dopamine/dobutamine (beta-1 support)
- Epinephrine (most potent inotrope + vasopressor)
- Milrinone or levosimendan (phosphodiesterase inhibitors - particularly for RV failure or when SVR is high; also reduce PVR)
- Noradrenaline or vasopressin for vasoplegic syndrome (common after prolonged CPB)
- Phenylephrine for isolated hypotension with preserved contractility
Vasoplegic syndrome: low SVR, low MAP despite preserved/high CO - occurs in up to 10-25% of cases. Treat with vasopressin, methylene blue (inhibits NO synthase/guanylate cyclase), or hydroxocobalamin (recent evidence: PMID 39438181).
RV failure is a feared complication - often triggered by: residual air embolism to RCA, protamine reaction (pulmonary vasoconstriction), reperfusion injury, pulmonary hypertension. Treat with inhaled NO, prostacyclin/iloprost, milrinone, reducing PEEP, and optimising RV preload.
8. Myocardial Protection
- The aorta is cross-clamped to allow a bloodless field
- Cardioplegia (cold blood or crystalloid solution with high K⁺ causing diastolic arrest) is delivered via the coronary arteries (antegrade via aortic root) or coronary sinus (retrograde)
- Topical hypothermia (ice-slush) may supplement
- Cross-clamp time must be minimised - prolonged ischaemia causes myocardial injury
- Volatile anaesthetic preconditioning: volatile agents (sevoflurane, isoflurane) given before and after ischaemia reduce infarct size and troponin release - a key reason to incorporate volatiles in cardiac anaesthesia even when TIVA is used for the non-bypass period
9. Post-CPB / Postoperative Period
Immediate Concerns
- Bleeding: from coagulopathy (as above), surgical bleeding. Decision to re-explore based on drain output, haemodynamic instability, and TOE (cardiac tamponade)
- Arrhythmias: AF is the most common (30-50% incidence post-CABG). May need DC cardioversion, amiodarone, magnesium
- Myocardial dysfunction: from reperfusion injury, inadequate protection, or pre-existing disease
- Respiratory: lung protective ventilation; avoid prolonged high FiO₂ (risk of atelectasis and oxygen toxicity)
Fast-Track Extubation
Contemporary cardiac anaesthesia aims for early extubation (within 6 hours post-op) in suitable patients using:
- Short-acting agents: remifentanil, propofol, desflurane/sevoflurane
- Reduced opioid strategies
- Dexmedetomidine infusion for sedation
- Regional/neuraxial adjuncts (intrathecal morphine, erector spinae plane block) reduce opioid requirements
10. Special Considerations
Paediatric CPB
- Circuit prime volume is 200-300% of the infant's blood volume; blood-prime essential for neonates
- High flow rates required (up to 200 mL/kg/min)
- DHCA commonly needed for complex repairs
- pH-stat management may improve neurological outcomes during DHCA
- Intense inflammatory response: corticosteroids + modified ultrafiltration post-bypass to remove cytokines and correct haemodilution
- Calcium supplementation important (calcium homeostasis frequently impaired)
- Close glucose monitoring (both hyper- and hypoglycaemia)
Off-Pump CABG (OPCAB)
- Avoids CPB entirely - reduces inflammatory response, haematological derangements, and potentially neurological complications
- But technically demanding, and evidence for improved outcomes is mixed
Summary Table: Key Anaesthetic Actions at Each Phase
| Phase | Key Anaesthetic Actions |
|---|---|
| Pre-induction | Arterial line insertion, preload assessment, anxiolysis, medication review |
| Induction | Haemodynamically stable induction, avoid tachycardia/hypotension, TOE probe insertion |
| Pre-CPB | Heparin administration, ACT confirmation >400-480 s, communicate with surgeon/perfusionist |
| On CPB | Maintain anaesthesia via oxygenator (volatile) or TIVA; cease ventilation; monitor ACT, temp, haematocrit, glucose, electrolytes; PA catheter withdrawal |
| Rewarming | Avoid hyperthermia (temp gradient <10°C); resume volatile; begin weaning drug preparation |
| Weaning | Restore ventilation; check rhythm, volume, electrolytes; TOE assessment; titrate inotropes/vasopressors |
| Post-protamine | Assess haemostasis; ACT check; coagulation support as needed |
| Post-CPB | Maintain haemodynamics; monitor for arrhythmia, RV failure, tamponade; plan for extubation |
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e (Chapters 21-22)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e (Chapter 39)
- Miller's Anesthesia, 2-Volume Set, 10e (Chapters on cardiac anaesthesia and pharmacokinetics)
Recent evidence note: A 2024 systematic review/meta-analysis (PMID 39438181) found hydroxocobalamin and methylene blue to be comparable treatments for vasoplegic shock following CPB, with hydroxocobalamin potentially having a favourable safety profile. A 2025 meta-analysis (PMID 40372573) supports prophylactic corticosteroids in neonatal cardiac surgery with CPB to reduce inflammation.
This is a shared conversation. Sign in to Orris to start your own chat.