Psoriasis
Reading File
Finding Sources
Searching PubMed
psoriasis treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
I now have comprehensive information to write a thorough response. Let me compile everything.
Psoriasis
Overview
Psoriasis is a common, chronic, recalcitrant inflammatory skin disease affecting approximately 3% of the general population worldwide, with equal frequency in males and females. About one-third of patients have a positive family history. It has a bimodal age of onset - peaking at approximately 22.5 years and again at 55 years. It is now recognized as a systemic inflammatory disease, not merely a skin condition.
- Goldman-Cecil Medicine, p. 4278
- Fitzpatrick's Dermatology, p. 227
Etiopathogenesis
Genetics
Psoriasis has complex polygenic inheritance. It is strongly associated with HLA-Cw6. Genome-wide studies have identified more than 85 non-MHC loci that increase risk.
Immune Mechanisms
The pathogenesis involves both the innate and adaptive immune systems with abnormal keratinocyte proliferation at its core.
Key immune mediators:
| Mediator | Role |
|---|---|
| IL-23 (p19/p40 heterodimer) | Drives Th17 cell development and maintenance of chronic inflammation |
| IL-17A | Promotes neutrophil-predominant inflammation; stimulates keratinocyte proliferation via autocrine loops |
| TNF-α | Primary proinflammatory cytokine produced by dermal dendritic cells; coproduced with IL-23 |
| IL-12 | Promotes Th1 differentiation |
| IFN-γ | Effector cytokine of Th1 cells |
| IL-22, IL-6 | Activate STAT3 in keratinocytes |
The inflammatory infiltrate of psoriatic skin is predominantly composed of Th1- and Th17-polarized memory T cells, along with neutrophils, macrophages, and increased dendritic cells.
Vascular changes are also characteristic: capillary loops within the papillary dermis elongate, dilate, and at the turnaround point touch the epidermis ("kissing"). The remodeled endothelium expresses venular adhesion molecules, allowing lymphocytes and neutrophils to exit at the papillary tips - a histologic feature called "squirting papillae."
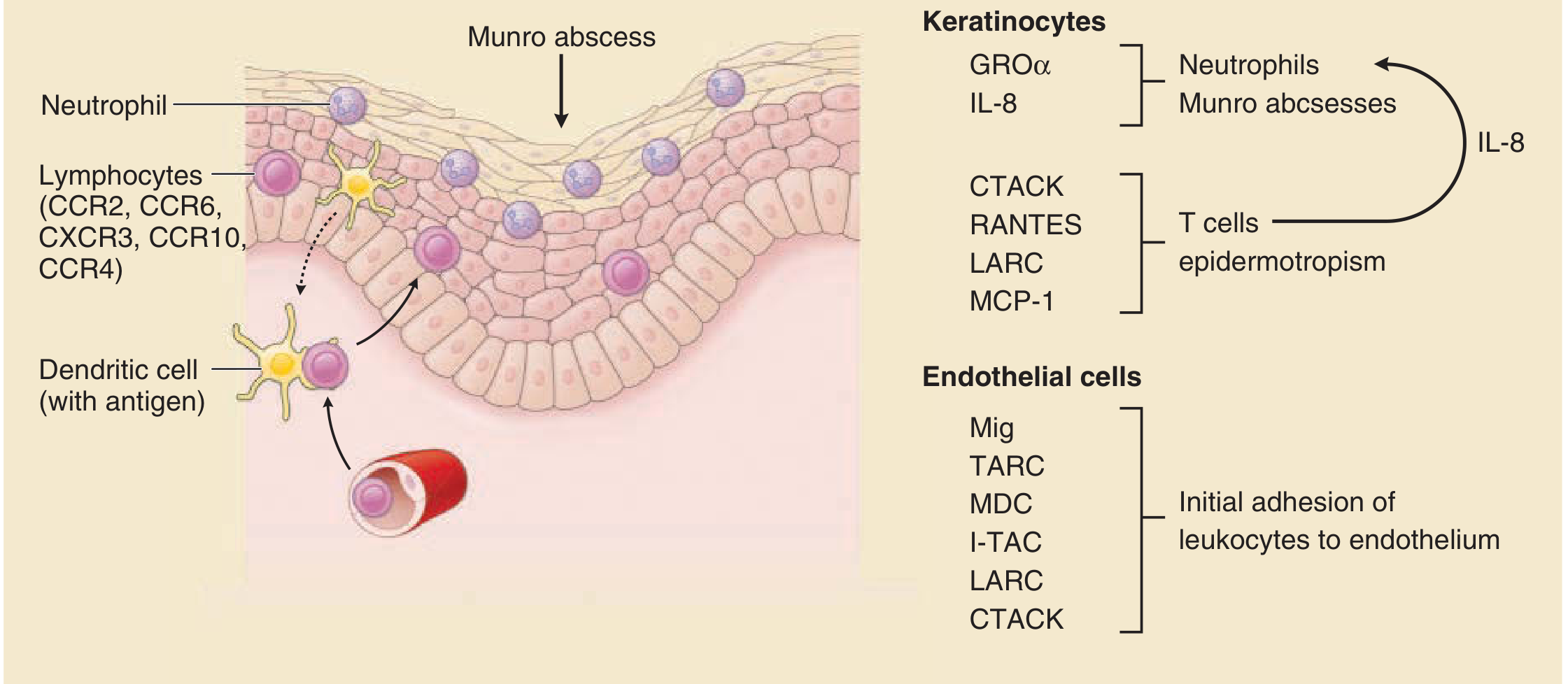
Chemokine network in psoriasis - Fitzpatrick's Dermatology, Fig. 12-11
Triggers
- Trauma (Koebner phenomenon)
- Streptococcal infection (especially guttate type)
- Stress
- Medications (lithium, beta-blockers, antimalarials, NSAIDs, systemic steroid withdrawal)
- Smoking (especially palmoplantar pustular type)
- HIV infection
Clinical Forms

Psoriasis vulgaris - Goldman-Cecil Medicine, Fig. 405-13
| Type | Features |
|---|---|
| Psoriasis vulgaris (plaque) | Most common. Persistent erythematous plaques with silvery/micaceous scales on elbows, knees, scalp, lumbosacral area |
| Guttate psoriasis | Small "raindrop" erythematous scaly papules over large body area; triggered by streptococcal infection |
| Inverse psoriasis | Affects skin folds (groin, axilla, inframammary); erythematous, shiny, scale-absent (friction removes it) |
| Pustular psoriasis | Sterile pustules; can be localized (palmoplantar) or generalized (von Zumbusch - medical emergency with systemic involvement) |
| Erythrodermic psoriasis | Widespread erythroderma with fine silvery scales; life-threatening |
| Palmoplantar psoriasis | Keratotic scaly plaques/patches on palms and soles, often with fissures |
| Nail psoriasis | Pitting, "oil drop" sign (yellowish macule under nail plate), onychodystrophy |
| Psoriatic arthritis | Inflammatory arthritis in ~30% of patients; may occur without skin disease |
Key Clinical Signs
- Auspitz sign: Pinpoint bleeding when scale is removed (exposes dilated papillary capillary loops)
- Koebner (isomorphic) phenomenon: New lesions appear at sites of skin trauma
- Silvery/micaceous scale: Distinguishes psoriasis from other erythematous conditions
Histopathology
- Acanthosis (epidermal thickening/hyperplasia) with reduced keratinocyte transit time
- Parakeratosis (retention of nuclei in stratum corneum)
- Munro microabscesses: collections of neutrophils in the stratum corneum
- Spongiform pustules of Kogoj: neutrophilic aggregates in the spinous/granular layer (especially pustular psoriasis)
- Thinned/absent granular layer
- Elongated, clubbed rete ridges
- Dilated, tortuous capillaries in papillary dermis ("squirting papillae")
Diagnosis
Diagnosis is primarily clinical, based on the characteristic morphology and distribution.
Differential diagnosis includes: seborrheic dermatitis, eczema/atopic dermatitis, pityriasis rubra pilaris, lichen planus, secondary syphilis, tinea corporis, mycosis fungoides.
Biopsy is rarely needed but confirms histopathologic features above when diagnosis is uncertain.
Treatment
Treatment is guided by disease severity (extent of body surface area involved, PASI score, quality of life impact).
Topical Therapy (mild-moderate disease)
- Corticosteroids - first-line; various potencies depending on site
- Vitamin D analogues (calcipotriol/calcitriol) - antiproliferative, reduce keratinocyte differentiation abnormalities; often combined with topical steroids
- Calcineurin inhibitors (tacrolimus, pimecrolimus) - especially for face and flexures
- Coal tar - antiproliferative, anti-inflammatory
- Salicylic acid - keratolytic
- Anthralin (dithranol) - antiproliferative
- Roflumilast cream (PDE4 inhibitor) - newer FDA-approved topical
- Tapinarof cream (aryl hydrocarbon receptor modulator) - newer FDA-approved topical
Phototherapy
- Narrowband UVB (NB-UVB) - preferred phototherapy; effective for plaque and guttate psoriasis
- PUVA (psoralen + UVA) - photochemotherapy; very effective, but higher skin cancer risk
- Excimer laser - targeted 308 nm UVB for limited disease
Systemic Agents (moderate-severe disease)
| Drug | Mechanism | Key Notes |
|---|---|---|
| Methotrexate | Antimetabolite; immunomodulatory | First-line systemic; monitor LFTs; risk of hepatotoxicity and myelosuppression |
| Cyclosporine | Calcineurin inhibitor; suppresses T-cell activation | Rapid onset; limited to short courses due to nephrotoxicity/hypertension |
| Acitretin | Oral retinoid | Teratogenic; avoid in women of childbearing age; good for pustular/erythrodermic |
| Apremilast | Oral PDE4 inhibitor | Modest efficacy; weight loss, diarrhea as side effects; no immunosuppression |
Note: Oral corticosteroids should NOT be used - psoriasis may worsen severely ("rebound") upon discontinuation.
Biologic Therapy (moderate-severe, refractory disease)
Biologics are more effective than oral treatments overall. Newer agents (ixekizumab, brodalumab, guselkumab, risankizumab, bimekizumab) appear more effective than older ones (etanercept, secukinumab, adalimumab).
Anti-TNF-α agents:
- Infliximab - chimeric anti-TNF monoclonal antibody (IV); highly effective
- Adalimumab - fully human anti-TNF IgG1 (SC)
- Etanercept - TNF receptor-Fc fusion protein (SC); binds primarily soluble TNF
- Certolizumab pegol - pegylated Fab' fragment; approved for psoriatic arthritis
- Infliximab and adalimumab are slightly more effective than etanercept, likely because they bind both soluble and membrane-bound TNF
Anti-IL-12/23 (p40 subunit):
- Ustekinumab - blocks shared p40 subunit of IL-12 and IL-23; slightly more effective than etanercept
Anti-IL-23 (p19 subunit - selective):
- Guselkumab, risankizumab, tildrakizumab - highly selective and effective; among the most efficacious biologics available
Anti-IL-17A:
- Secukinumab - fully human anti-IL-17A antibody
- Ixekizumab - humanized anti-IL-17A antibody
- IL-17A biologics are among the most effective drugs available for psoriasis
Anti-IL-17 receptor:
- Brodalumab - targets IL-17 receptor α chain; FDA-approved with screening requirement for depression/suicidal ideation
Pre-biologic screening: TB (Mantoux/IGRA), HIV, hepatitis B and C.
Comorbidities
Psoriasis is a systemic inflammatory disease with significant comorbidities:
- Psoriatic arthritis (~30%)
- Metabolic syndrome (obesity, hypertension, dyslipidemia, type 2 diabetes)
- Cardiovascular disease (increased risk of MI, stroke)
- Depression and anxiety
- Non-alcoholic fatty liver disease
- Inflammatory bowel disease
- Uveitis
Severity Assessment
- PASI (Psoriasis Area and Severity Index): composite score of erythema, induration, scaling, and body surface area; PASI-75 (75% improvement) is the standard efficacy endpoint in clinical trials
- BSA (Body Surface Area): <3% mild, 3-10% moderate, >10% severe
- DLQI (Dermatology Life Quality Index): captures quality of life impact
Sources: Fitzpatrick's Dermatology in General Medicine, Vol. 1-2; Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.