Difference between aldolase and aldose reductase
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple textbooks. Here is a detailed comparison:
Aldolase vs. Aldose Reductase
These two enzymes share a similar-sounding name but are completely different in every meaningful way - their reactions, pathways, cofactors, tissue distribution, and clinical relevance.
1. ALDOLASE
| Feature | Detail |
|---|---|
| Full name | Fructose-bisphosphate aldolase (EC 4.1.2.13) |
| Reaction type | Lyase - cleaves a C-C bond (aldol cleavage) |
| Pathway | Glycolysis (and gluconeogenesis in reverse) |
| Substrate | Fructose-1,6-bisphosphate |
| Products | Dihydroxyacetone phosphate (DHAP) + Glyceraldehyde-3-phosphate (G3P) |
| Cofactor | None (no NAD+, no NADPH) |
| Reaction direction | Reversible; not regulated |
| Structure | 159 kDa tetramer (4 x 40 kDa subunits) |
| Step in glycolysis | Step 4 (of 10) |
Isoforms of Aldolase
There are three isoenzymes:
- Aldolase A - expressed in muscle and red blood cells (also in most tissues)
- Aldolase B - predominant in the liver, kidney, and small intestinal mucosa; uniquely cleaves both fructose-1,6-bisphosphate AND fructose-1-phosphate (involved in dietary fructose metabolism)
- Aldolase C - found in the brain
"Aldolase cleaves fructose 1,6-bisphosphate to dihydroxyacetone phosphate (DHAP) and glyceraldehyde 3-phosphate. The reaction is reversible and not regulated." - Biochemistry, 8th ed. Lippincott Illustrated Reviews
Clinical significance of Aldolase
- Hereditary fructose intolerance (HFI): Caused by a deficiency of aldolase B (specifically, its fructose-1-phosphate cleaving activity). Fructose-1-phosphate accumulates, causing severe hypoglycemia and liver toxicity after fructose ingestion.
- Aldolase A deficiency (OMIM 611881): Very rare; causes chronic hemolytic anemia, and sometimes myopathy or rhabdomyolysis.
- Serum aldolase is a useful lab marker elevated in muscle diseases (myopathies, muscular dystrophy, dermatomyositis) and liver disease.
2. ALDOSE REDUCTASE
| Feature | Detail |
|---|---|
| Full name | Aldose reductase (EC 1.1.1.21) |
| Reaction type | Oxidoreductase - reduces an aldehyde to an alcohol |
| Pathway | Polyol pathway (sorbitol pathway) |
| Substrate | Glucose (or galactose) |
| Product | Sorbitol (or galactitol) |
| Cofactor | NADPH (oxidized to NADP+) |
| Reaction direction | Essentially irreversible under physiological conditions |
| Km for glucose | High - only activated under hyperglycemia |
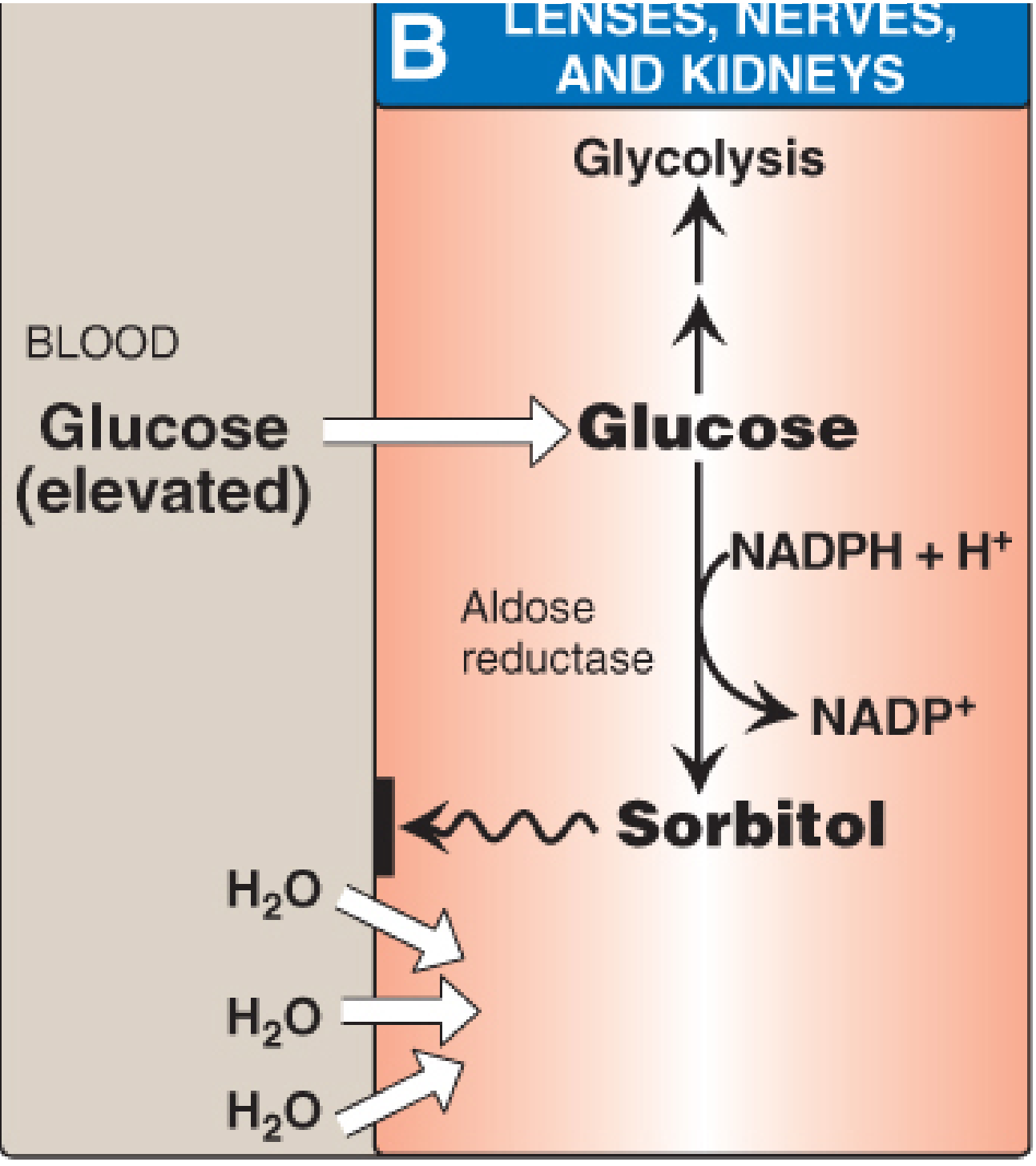
Aldose Reductase Reaction
Glucose + NADPH + H⁺ → Sorbitol + NADP⁺
(Aldose reductase)
Sorbitol can then be further oxidized to fructose by sorbitol dehydrogenase (uses NAD+), completing the two-step polyol pathway.
Tissue distribution
Aldose reductase is found in tissues that do not require insulin for glucose uptake: retina, lens, kidneys, peripheral nerves, ovaries, and seminal vesicles. This is important - in hyperglycemia, glucose floods these cells unrestricted.
Clinical significance of Aldose Reductase
Aldose reductase is directly responsible for diabetic microvascular and neural complications:
- Sorbitol accumulation: Sorbitol cannot exit cells efficiently, causing osmotic swelling and cell damage.
- Cataract formation: In the lens, accumulated sorbitol (and galactitol in galactosemia) causes osmotic cataracts.
- Diabetic neuropathy: Sorbitol accumulation in peripheral nerves reduces myoinositol, disrupts phosphoinositide metabolism, and impairs Na+/K+-ATPase activity.
- Nephropathy and retinopathy: Microvascular damage in kidneys and retina.
- NADPH depletion: The reaction consumes NADPH, which is also needed to regenerate reduced glutathione (an antioxidant) - this compounds oxidative stress in diabetic tissues.
"Use of NADPH in the aldose reductase reaction decreases the generation of reduced glutathione, an important antioxidant, and may also be related to complications of diabetes." - Biochemistry, 8th ed. Lippincott Illustrated Reviews
Aldose reductase inhibitors (ARIs)
Drugs like epalrestat (used clinically in some countries) inhibit aldose reductase to prevent diabetic neuropathy and other complications.
Side-by-Side Summary
| Feature | Aldolase | Aldose Reductase |
|---|---|---|
| Enzyme class | Lyase | Oxidoreductase |
| Pathway | Glycolysis / Gluconeogenesis | Polyol (sorbitol) pathway |
| Substrate | Fructose-1,6-bisphosphate | Glucose |
| Product | DHAP + G3P | Sorbitol |
| Cofactor required | None | NADPH |
| Reversibility | Reversible | Essentially irreversible |
| Primary tissue | Muscle, liver, RBCs | Lens, retina, nerves, kidney |
| Isoforms | A (muscle/RBC), B (liver), C (brain) | One main form |
| Clinical relevance | Hereditary fructose intolerance (B); myopathy marker (A) | Diabetic cataracts, neuropathy, nephropathy, retinopathy |
| Deficiency | Hemolytic anemia (rare) | Overactivity causes harm (inhibition is therapeutic) |
The key memory trick: Aldolase splits (a lyase that aldol-cleaves in glycolysis), while Aldose reductase reduces (an oxidoreductase that makes sorbitol using NADPH in the polyol pathway under hyperglycemia).
Sources: - Biochemistry, 8th ed. Lippincott Illustrated Reviews - Tietz Textbook of Laboratory Medicine, 7th Ed. - Harper's Illustrated Biochemistry, 32nd Ed. - Basic Medical Biochemistry, 6th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.