tell me everything about Cardio Valvular disease infectious and non too in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"valvular heart disease" AND management
I now have comprehensive data from multiple authoritative sources. Let me compile the complete, detailed answer.
Cardiovascular Valvular Heart Disease: Infectious and Non-Infectious - A Comprehensive Review
OVERVIEW
Valvular heart disease (VHD) encompasses a spectrum of structural and functional abnormalities of the cardiac valves - the mitral, aortic, tricuspid, and pulmonary - that disrupt normal unidirectional blood flow. Disease may result from direct infection of valve tissue (infective) or from degenerative, autoimmune, congenital, hemodynamic, or systemic processes (non-infective). The global burden is substantial: aortic stenosis affects ~15% of individuals over 65 years, and rheumatic heart disease remains the leading cause of acquired heart disease in children in low-income countries.
(Braunwald's Heart Disease, p.1036; Goldman-Cecil Medicine, p.3044)
PART I: INFECTIOUS VALVULAR DISEASE
1. Infective Endocarditis (IE)
Definition and Classification
Infective endocarditis is a microbial infection of the heart valves or endocardium leading to formation of vegetations composed of thrombotic debris and organisms, often with destruction of the underlying cardiac tissue. The aorta, aneurysmal sacs, other blood vessels, and prosthetic devices may also become infected.
IE is classified as acute or subacute based on the tempo and severity of the clinical course - distinctions related to the virulence of the microbe and whether underlying cardiac disease is present.
- Acute IE: Rapidly progressive, destructive infections with substantial morbidity and mortality even with appropriate therapy
- Subacute IE: Insidious onset; protracted course over weeks to months; most patients recover with antibiotic therapy
(Robbins & Kumar Basic Pathology, p.367-368)
Epidemiology and Risk Factors
Predisposing cardiac conditions include:
- Rheumatic heart disease
- Mitral valve prolapse (now the leading preexistent risk factor in developed countries)
- Bicuspid aortic valves
- Calcific valvular stenosis
- Prosthetic heart valves - account for 10-20% of all IE cases
- Sterile platelet-fibrin deposits at pacemaker lines, indwelling catheters, or endocardial damage from flow "jets"
Host risk factors: neutropenia, immunodeficiency, malignancy, diabetes, alcohol use, intravenous drug use
Causative Organisms
| Organism | Setting | Form |
|---|---|---|
| Streptococcus viridans (50-60% community) | Damaged/deformed valves, oral procedures | Subacute |
| Staphylococcus aureus | Healthcare settings, IV drug users, healthy valves | Acute |
| Enterococci | GI/GU procedures, elderly | Variable |
| HACEK group (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella) | Oral flora | Subacute |
| Gram-negative bacilli, fungi | Immunocompromised | Aggressive |
| Culture-negative (~10%) | Prior antibiotics, fastidious organisms | Variable |
Tricuspid valve is a frequent target in IV drug users (right-sided IE). Left-sided IE predominantly affects mitral and aortic valves.
(Robbins & Kumar Basic Pathology, p.367-368)
Pathogenesis
Bacteremia seeds the bloodstream from: dental/surgical procedures, IV drug injection, occult GI/oral sources, or trivial skin injuries. Organisms adhere to sterile platelet-fibrin thrombi at sites of endothelial damage, then proliferate within the vegetation while protected from host defenses.
Morphology (Gross and Microscopic)
In both acute and subacute forms, friable, bulky, and potentially destructive vegetations containing fibrin, inflammatory cells, and microorganisms form on valves. Key features:
- Aortic and mitral valves most commonly affected
- Vegetations may be single or multiple, and may involve more than one valve
- Can erode into myocardium to produce ring abscess (abscess cavity)
- Shedding of septic emboli is common - leads to septic infarcts and mycotic aneurysms at embolization sites
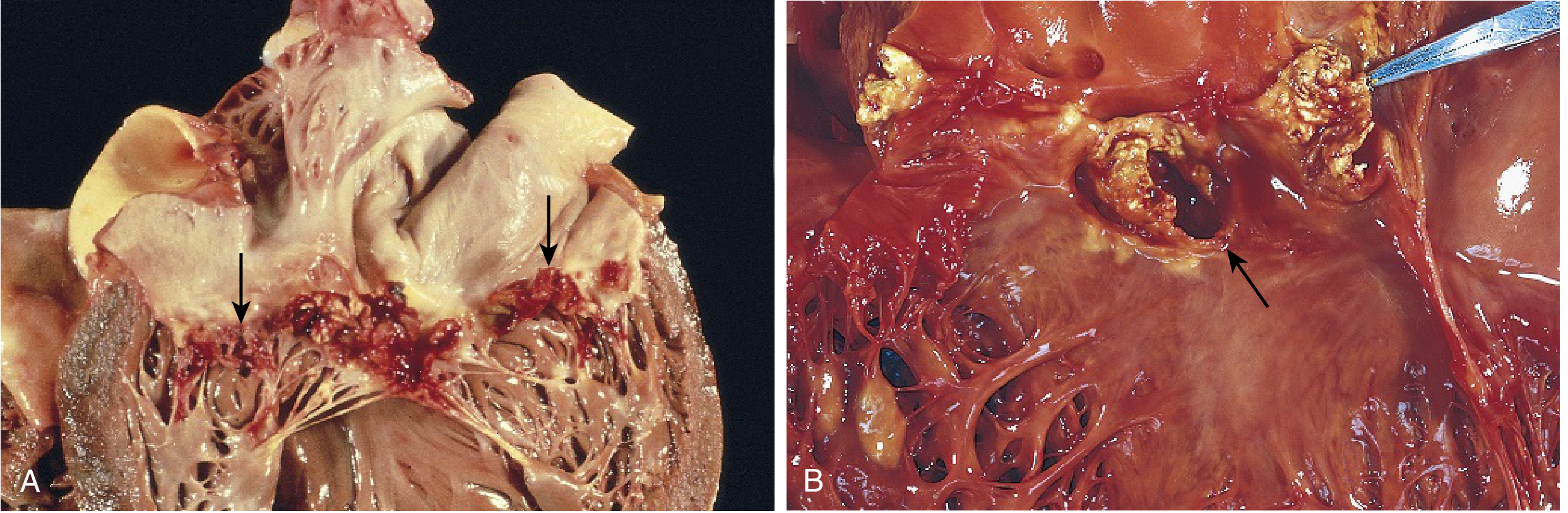
Infective endocarditis. (A) Subacute endocarditis caused by Streptococcus viridans on a previously myxomatous mitral valve - large friable vegetations (arrows). (B) Acute endocarditis caused by Staphylococcus aureus on a congenitally bicuspid aortic valve with extensive cuspal destruction and ring abscess (arrow). - Robbins & Kumar Basic Pathology, p.368
Clinical Features
- Fever - the most consistent sign
- In subacute IE (especially elderly): nonspecific fatigue, weight loss, flu-like syndrome; splenomegaly common
- Acute IE: rapidly developing fever, chills, lassitude
- Murmurs present in 90% of left-sided lesions
- Peripheral stigmata (from microemboli):
- Petechiae
- Nail bed (splinter) hemorrhages
- Roth spots - retinal hemorrhages
- Janeway lesions - painless erythematous lesions of palm/sole
- Osler nodes - painful fingertip nodules
- Diagnosis: positive blood cultures + echocardiographic findings
Complications and Prognosis
- Glomerulonephritis - immune complex deposition; hematuria, albuminuria, renal failure
- Arrhythmias (extension to conduction system)
- Systemic embolization - stroke, splenic/renal infarcts
- Heart failure from valvular destruction
- Left untreated: generally fatal
- With appropriate antibiotics ± valve replacement: mortality significantly reduced
(Robbins & Kumar Basic Pathology, p.368-369)
Diagnosis
- Echocardiography (TTE/TEE): strongly supported in virtually all suspected IE cases
- TEE preferred when: TTE is poor quality, negative findings with high suspicion, prosthetic valve involvement, staphylococcal bacteremia, or elderly patients with valvular abnormalities
- TEE is particularly important for prosthetic valve endocarditis where TTE is less sensitive
(Braunwald's Heart Disease, p.1221-1240)
Prevention (AHA 2021 Guidelines)
Antibiotic prophylaxis (AP) is indicated before invasive dental procedures for high-risk patients:
- Presence of prosthetic cardiac valve or material
- Transcatheter implanted prosthetic valves
- Cardiac valve repair with annuloplasty rings
- Prior history of IE
- Unrepaired or recently repaired cyanotic congenital heart defects
- Ventricular assist devices and implantable hearts (added 2021)
Regimen updates (AHA 2021):
- Amoxicillin remains preferred (90% of penicillin-allergic patients have negative skin testing and can receive it)
- Clindamycin eliminated as alternative due to Clostridioides difficile risk
- Doxycycline added as alternative for truly penicillin-allergic patients
- Shared decision-making with patient education emphasized
- Good oral health maintenance is fundamental
(Braunwald's Heart Disease, citing AHA 2021)
PART II: NON-INFECTIOUS VALVULAR DISEASE
2. Rheumatic Valvular Disease (Rheumatic Heart Disease)
Pathogenesis
Rheumatic fever is an acute, immunologically mediated, multisystem inflammatory disease occurring after group A beta-hemolytic streptococcal infections (usually pharyngitis). Rheumatic heart disease (RHD) is the cardiac manifestation, involving inflammation of all parts of the heart, but valvular inflammation and scarring produce the most important clinical features.
The mechanism involves molecular mimicry: streptococcal antigens resemble cardiac tissue antigens, triggering cross-reactive immune responses that damage valve leaflets.
(Robbins & Kumar Basic Pathology, p.369)
Epidemiology
- 35-72% of acute rheumatic fever patients develop clinical carditis
- RHD has declined greatly in high-income countries due to improved socioeconomic conditions, rapid streptococcal treatment, and reduced streptococcal virulence
- In low-income countries, RHD remains the most important form of acquired heart disease in children and young adults
- Remains a leading cause of bacterial endocarditis and cardiovascular morbidity in endemic regions
Valve Involvement Pattern
- Mitral valve: affected nearly 100% of the time
- Aortic valve: involved in 20-30% of cases (regurgitation more common than stenosis)
- Tricuspid valve: histologic evidence of disease in 15-40%, but usually not clinically relevant
- Pulmonic valve: rarely involved
Mitral regurgitation is the most common valvular pathology in acute RHD. Mitral stenosis develops after progressive scarring - RHD is essentially the only cause of acquired mitral stenosis worldwide.
(Goldman-Cecil Medicine, p.3044; Robbins & Kumar Basic Pathology, p.369)
Morphology
Acute phase:
- Small, warty inflammatory vegetations along the lines of valve closure (1-2 mm)
- Unlike infective endocarditis, these are NOT destructive
- Aschoff bodies (pathognomonic) - granulomatous foci with large cells (Aschoff giant cells) in the myocardium
- Pancarditis: pericarditis, myocarditis, endocarditis
Chronic phase (Rheumatic heart disease):
- Progressive fibrosis and thickening of valve leaflets
- Fusion of commissures
- Calcification
- Chordae tendineae thicken, fuse, and shorten
- Classic "fish-mouth" or "buttonhole" deformity of mitral valve in stenosis
Clinical Presentation and Management
- Classic murmurs present on auscultation; echocardiography key to diagnosis
- Secondary prophylaxis: intramuscular benzathine penicillin G to prevent recurrent acute rheumatic fever and disease progression
- Severe valvular disease typically appears in the 3rd-4th decade of life
- In endemic regions, echocardiographic screening can detect latent RHD to guide prophylaxis
3. Degenerative / Calcific Valvular Disease
Calcific Aortic Stenosis (AS)
The most common form of valvular heart disease in older adults.
Epidemiology: Present in ~15% of individuals ≥65 years; severe AS (valve area <1 cm²) in ~2%.
Pathogenesis:
- Calcification of a trileaflet aortic valve (tricuspid AV) - majority of older patients
- Patients with congenital bicuspid valves present 1-2 decades earlier (4th-5th decade)
- Process resembles atherosclerosis: lipid deposition, inflammation, calcification along mechanical stress lines
Hemodynamic Consequences: Progressive outflow obstruction → LV pressure overload → LV hypertrophy → reduced compliance → eventually LV failure
Classic Triad of Symptoms (appear late, mean survival after onset):
- Angina: 3-5 years survival
- Syncope (exertional): 2-3 years
- Heart failure (dyspnea): 1-2 years
Echocardiographic Criteria for Severe AS:
- Aortic valve area <1.0 cm² (or <0.6 cm²/m² BSA)
- Mean gradient ≥40 mmHg
- Peak flow velocity ≥4 m/sec
- LV stroke volume index ≥35 mL/m² (classic high flow, high gradient)
- Low-flow, low-gradient AS: >40% of older patients have lower gradients; about half also have LV stroke volume index <35 mL/m²
Management:
- Surgical AVR (SAVR): Standard for lower-risk patients
- Transcatheter AVR (TAVR): Transformative for high-risk and intermediate-risk surgical patients; now proven in low-risk patients (composite risk death/stroke/hospitalization at 1 year: 8.5% TAVR vs. 15.1% SAVR in low-risk trial)
- ACC/AHA 2020 guidelines: SAVR or TAVR after shared decision-making for symptomatic patients ages 65-80 years; TAVR preferred ≥80 years
- Tissue valve generally preferred over mechanical in older patients (avoid anticoagulation)
- Bioprosthetic valves deteriorate more slowly in older patients
(Braunwald's Heart Disease, p.1036-1042)
Mitral Annular Calcification
- Degenerative calcification of the mitral annulus
- Common in the elderly, especially women
- Rarely causes significant valvular dysfunction alone but increases risk of arrhythmias, conduction disturbances, and stroke
4. Myxomatous Degeneration / Mitral Valve Prolapse (MVP)
Pathogenesis
Primary MVP: Intrinsic extracellular matrix defect - thinning of the fibrosa layer of the valve with expansion of the spongiosa layer due to increased mucoid (myxomatous) material deposition. Can be familial (autosomal dominant, variable penetrance) or sporadic.
Secondary MVP: Associated with identifiable genetic disorders such as Marfan syndrome, Ehlers-Danlos syndrome, osteogenesis imperfecta.
Morphology
- Ballooning (hooding) of the mitral leaflets - enlarged, redundant, thick, rubbery leaflets
- Chordae tendineae are elongated, thinned, occasionally rupture
- In primary mitral disease: concomitant tricuspid valve involvement in 20-40% of cases; aortic and pulmonic valves less commonly affected
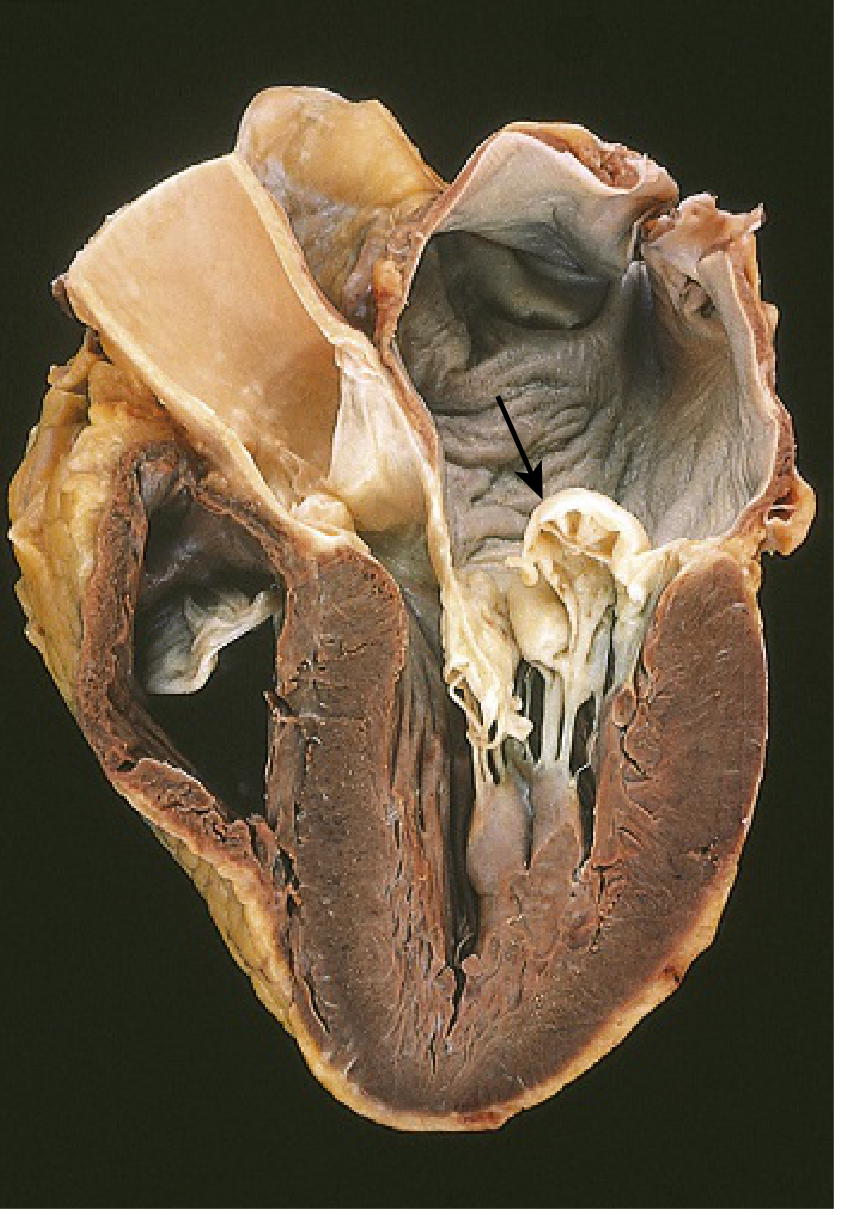
Myxomatous degeneration of the mitral valve with prominent hooding (prolapse) of the posterior mitral leaflet into the left atrium. - Robbins & Kumar Basic Pathology
Clinical Features
- Most patients are asymptomatic - valvular abnormality discovered incidentally
- Minority: palpitations, dyspnea, atypical chest pain
- Auscultation: midsystolic click (pathognomonic) ± regurgitant murmur
- ~3% develop complications:
- Hemodynamically significant mitral regurgitation and CHF (especially with chordal/leaflet rupture)
- Infective endocarditis (increased risk)
- Sudden cardiac death from ventricular arrhythmias
- Stroke/systemic infarcts from left atrial thrombi (rare)
(Robbins & Kumar Basic Pathology, p.901-916)
5. Nonbacterial Thrombotic Endocarditis (NBTE) / Marantic Endocarditis
Definition
NBTE is characterized by deposition of sterile thrombi on cardiac valves in patients with underlying hypercoagulable states. In contrast to infective endocarditis, the lesions are non-destructive.
Pathogenesis and Causes
- Vegetations are small (1-5 mm), usually on previously normal valves
- Hypercoagulable states are the usual precursor
- Underlying malignancy is the most common cause - particularly mucinous adenocarcinomas (colon, pancreas, lung), related to circulating mucin and procoagulants
- Other causes: chronic DIC, hyperestrogenic states, endocardial trauma from indwelling catheters
Morphology
- Small, bland, nondestructive vegetations along the line of valve closure (compare to IE: large, irregular, destructive; compare to RHD: small, at line of closure, inflammatory)
- Histology: bland thrombus, virtually no inflammation in the valve cusp; thrombus only loosely attached
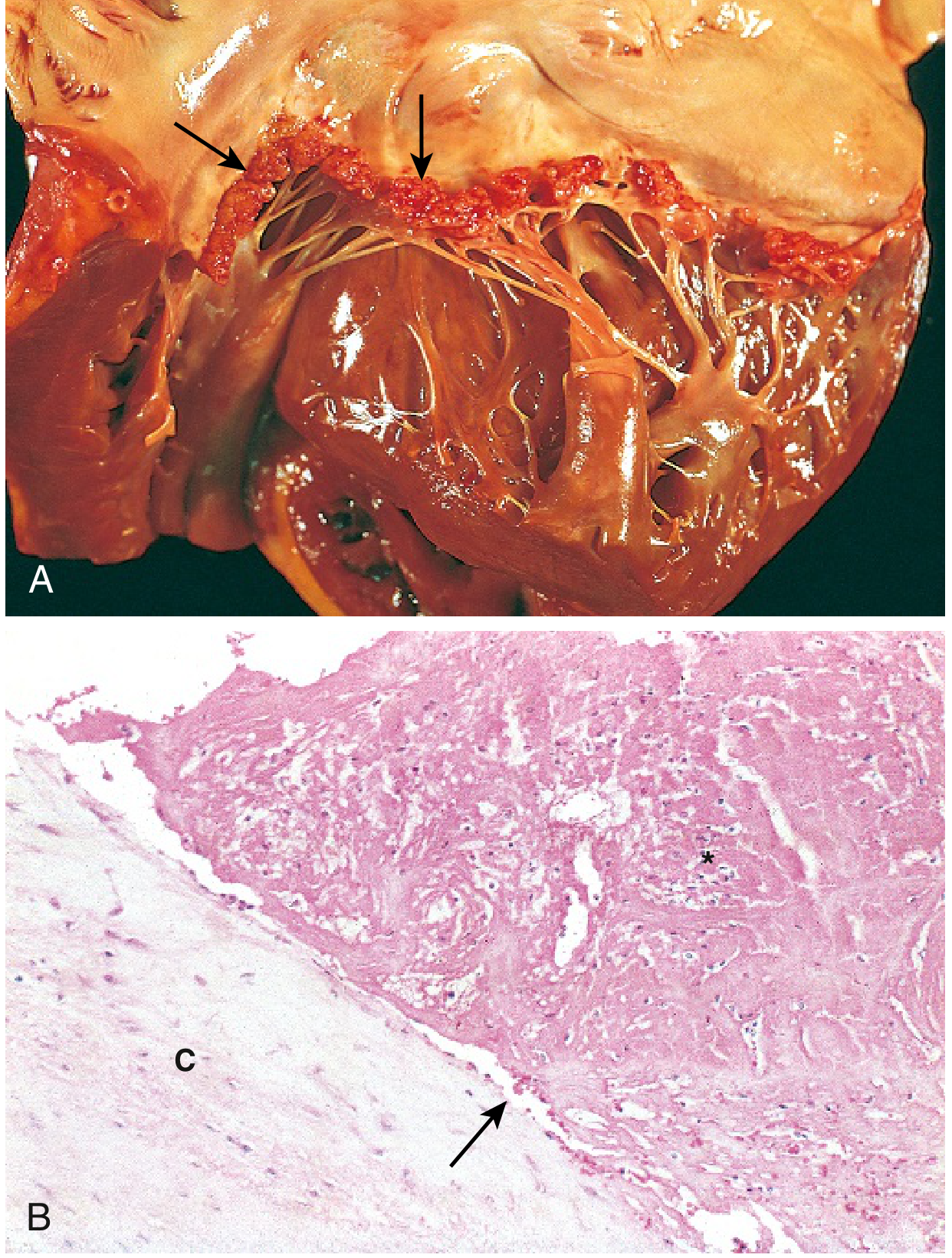
NBTE. (A) Small thrombotic vegetations along the line of closure of the mitral valve leaflets (arrows). (B) Photomicrograph showing bland thrombus with virtually no inflammation; thrombus only loosely attached to the cusp (arrow). - Robbins & Kumar Basic Pathology, p.369
Clinical Consequences
- Local valvular effect usually trivial
- Major risk: emboli from easily-dislodged, inflammation-free vegetations → infarcts in brain, heart, kidneys, spleen
- NBTE can serve as a nidus for bacterial colonization → development of infective endocarditis (bridge between non-infective and infective disease)
(Robbins & Kumar Basic Pathology, p.369-370)
6. Libman-Sacks Endocarditis (LSE)
Definition
Libman-Sacks endocarditis is a form of NBTE characterized by sterile vegetations on valves of patients with systemic lupus erythematosus (SLE).
Pathogenesis
- Probable mechanism: immune complex deposition with associated inflammation and fibrinoid necrosis of the valve adjacent to the vegetation
- Subsequent fibrosis and serious deformity can result in lesions resembling chronic RHD
- Similar lesions occur in antiphospholipid antibody syndrome
Morphology
- Small to medium-sized inflammatory vegetations that can be attached on either side of the valve leaflets (unique - unlike other endocarditis types)
- Can occur on chordae, atrial, or ventricular endocardium
- Heal with scarring
(Robbins & Kumar Basic Pathology, p.370)
7. Individual Valve Lesions - Summary
Mitral Stenosis (MS)
- Etiology: Almost exclusively RHD; rarely congenital
- Pathophysiology: Fixed obstruction to LV inflow → LA hypertension → pulmonary hypertension → right heart failure
- PH affects >50% of MS patients; tracks strongly with symptoms
- Patients with PASP >60 mmHg have higher restenosis rates after valvuloplasty and decreased 3-year survival after valvotomy
- Intervention: Balloon mitral valvuloplasty (BMV) for pliable valves; mitral valve replacement for rigid/calcified valves
Mitral Regurgitation (MR)
- Etiologies: Primary (degenerative/MVP, ruptured chordae, RHD, IE) vs. secondary/functional (LV dilatation, ischemic cardiomyopathy)
- Pathophysiology: Volume overload of LA and LV → LV dilatation → eventually LV dysfunction
- Moderate/severe PH observed in >50% of severe primary MR patients
- Average 5-year survival ~25% less with PH compared to those without
- Intervention: Surgical repair preferred over replacement; MitraClip transcatheter repair for high-risk patients
Aortic Stenosis (AS)
(See detailed section above under Degenerative Disease)
Aortic Regurgitation (AR)
- Etiologies: Valve leaflet disease (bicuspid AV, IE, RHD) or aortic root disease (aortic dissection, Marfan, syphilitic aortitis, hypertension)
- Pathophysiology: Volume + pressure overload of LV → eccentric hypertrophy → eventual LV dilatation and systolic dysfunction
- Clinical signs: Wide pulse pressure, water-hammer (Corrigan's) pulse, Duroziez sign, Quincke pulse
- When AR is combined with MR: Blood may reflux from aorta through both left heart chambers into pulmonary veins - a severe and poorly tolerated combination
- Intervention: AVR when symptomatic or when LV EF <55% or LV end-systolic dimension >50 mm
(Braunwald's Heart Disease, p.2399-2409; Fuster's The Heart 15th Ed., p.597-624)
Tricuspid Valve Disease
- Tricuspid regurgitation (TR): Most commonly functional (from RV dilatation/pulmonary hypertension) rather than primary organic disease
- Organic TR: carcinoid syndrome (deposits on RV side), IE in IV drug users, Ebstein anomaly, RHD
- Carcinoid heart disease: Fibrous plaques on RV endocardium, tricuspid and pulmonic valves → regurgitation + stenosis; relates to serotonin/substance P excess
Pulmonary Valve Disease
- Rarest clinically significant valvular disease
- Pulmonary stenosis: Usually congenital (isolated or part of Tetralogy of Fallot)
- Pulmonary regurgitation: Usually secondary to pulmonary hypertension
8. Pulmonary Hypertension in Valvular Disease
All forms of left-sided VHD can cause pulmonary hypertension through elevated left-sided filling pressures:
- Aortic stenosis: 30-36% of asymptomatic AS patients have at least mild PH; severe PH in 20%
- Mitral stenosis: PH in >50% of patients; key determinant of management and outcomes
- Mitral regurgitation: Moderate/severe PH in >50% of severe primary MR
- Secondary MR (HFpEF): ~40% PH prevalence
(Braunwald's Heart Disease, p.941-945)
9. Multivalvular Disease
Common combinations and their clinical implications:
| Combination | Notes |
|---|---|
| AS + MR | Most frequent MVD in developed countries (older patients); MR often functional; TAVR patients with severe MR have significantly higher mortality |
| AR + MR | Poorly tolerated; severe volume overload; LV dilatation; higher risk of postoperative LV dysfunction; often from RHD, myxomatous degeneration, or IE |
| AS + MS | Rare in developed countries; leads to important decrease in cardiac output; both lesions underestimate severity; CT calcium scoring useful |
| AR + MS | Opposing effects on LV loading; clinical signs of AR (wide pulse pressure) may be blunted; PHT method invalid for MS area calculation |
Surgical management: Timing driven by the more severe predominant lesion. Poorer outcomes for combined AR + MR than other combinations. Higher operative threshold for multivalvular vs. single-valve surgery.
(Braunwald's Heart Disease, p.2394-2410; Fuster's The Heart, p.595-624)
COMPARATIVE SUMMARY: Types of Endocarditis
| Feature | Infective (IE) | Rheumatic (RHD) | NBTE | Libman-Sacks (SLE) |
|---|---|---|---|---|
| Cause | Bacteria (S. aureus, S. viridans, etc.) | Group A Strep (immune-mediated) | Hypercoagulability/malignancy | Immune complexes (SLE/APS) |
| Vegetation size | Large, irregular, bulky, friable | Small, warty, beaded | Small, bland (1-5 mm) | Small-medium |
| Location | Valve leaflet surface (any) | Line of valve closure | Line of valve closure | Either side of leaflet |
| Destruction | Yes (major) | No (acute phase minimal) | No | Fibrosis → scarring |
| Sterile? | No | No | Yes | Yes |
| Emboli | Septic emboli common | Rare | Non-septic emboli common | Rare |
| Organisms on culture | Yes | No | No | No |
| Key association | IV drug use, prosthetic valve | Pharyngeal Strep infection | Adenocarcinoma, DIC | SLE, APS |
(Robbins & Kumar Basic Pathology, p.365-370)
KEY DIAGNOSTIC TOOLS
- Echocardiography (TTE/TEE): First-line for all VHD - anatomy, hemodynamics, severity grading
- Doppler: Gradients, valve areas, regurgitant volumes, pulmonary pressures
- CT/MDCT: Aortic valve calcium scoring (especially for low-flow AS), structural planning before TAVR
- Cardiac catheterization: Hemodynamic assessment when non-invasive data discordant
- Blood cultures x3: Before antibiotics in all suspected IE
- 3D echocardiography: Better morphological assessment of complex valvular lesions
KEY MANAGEMENT PRINCIPLES
- Antibiotics are curative for IE; valve repair/replacement when significant destruction occurs
- Rheumatic fever: Primary prevention (treat strep throat); secondary prevention (benzathine penicillin prophylaxis for years to life)
- Symptomatic severe AS: SAVR or TAVR based on age, surgical risk, anatomy
- Chronic severe MR: Surgery when symptomatic OR before significant LV dysfunction (EF <60%, ESD >40 mm)
- Watchful waiting with serial echocardiography for asymptomatic mild-moderate disease
- NBTE: Treat underlying cause; anticoagulation for embolic events; address malignancy
- Libman-Sacks: Treat SLE; antithrombotic therapy for APS
Sources:
- Robbins & Kumar Basic Pathology, pp. 365-370 (endocarditis, RHD, NBTE, LSE, MVP)
- Braunwald's Heart Disease, 12th Ed., pp. 1036-1042; 2394-2410 (AS, multivalvular disease, IE prevention/management)
- Goldman-Cecil Medicine, p. 3044 (rheumatic heart disease)
- Fuster and Hurst's The Heart, 15th Ed., pp. 595-624 (multivalvular disease, individual lesion combinations)
- AHA 2021 Scientific Statement on IE Prevention - cited within Braunwald's
- Recent PubMed: Carcinoid heart disease surgical management meta-analysis, 2024 [PMID: 38572311]; Aortic stenosis with cardiac amyloidosis meta-analysis, 2025 [PMID: 39955158]
This is a shared conversation. Sign in to Orris to start your own chat.