Abnormal uterine bleeding clinical discussion
Reading File
Finding Sources
Finding Sources
Searching PubMed
"abnormal uterine bleeding"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, multi-source content to deliver a complete clinical discussion. Let me compose the full answer:
Abnormal Uterine Bleeding (AUB) - Clinical Discussion
Normal Menstrual Physiology (Baseline)
Understanding AUB requires grounding in normal physiology. A normal menstrual cycle spans 21-35 days, flow lasts 4-8 days, and blood loss averages 35 mL (heavy menstrual bleeding defined as >80 mL/cycle). The cycle is governed by the HPO axis: FSH drives follicular growth and estradiol production in the follicular phase; the LH surge triggers ovulation; the corpus luteum then produces progesterone in the luteal phase. When implantation does not occur, progesterone and estrogen fall, causing synchronized endometrial shedding.
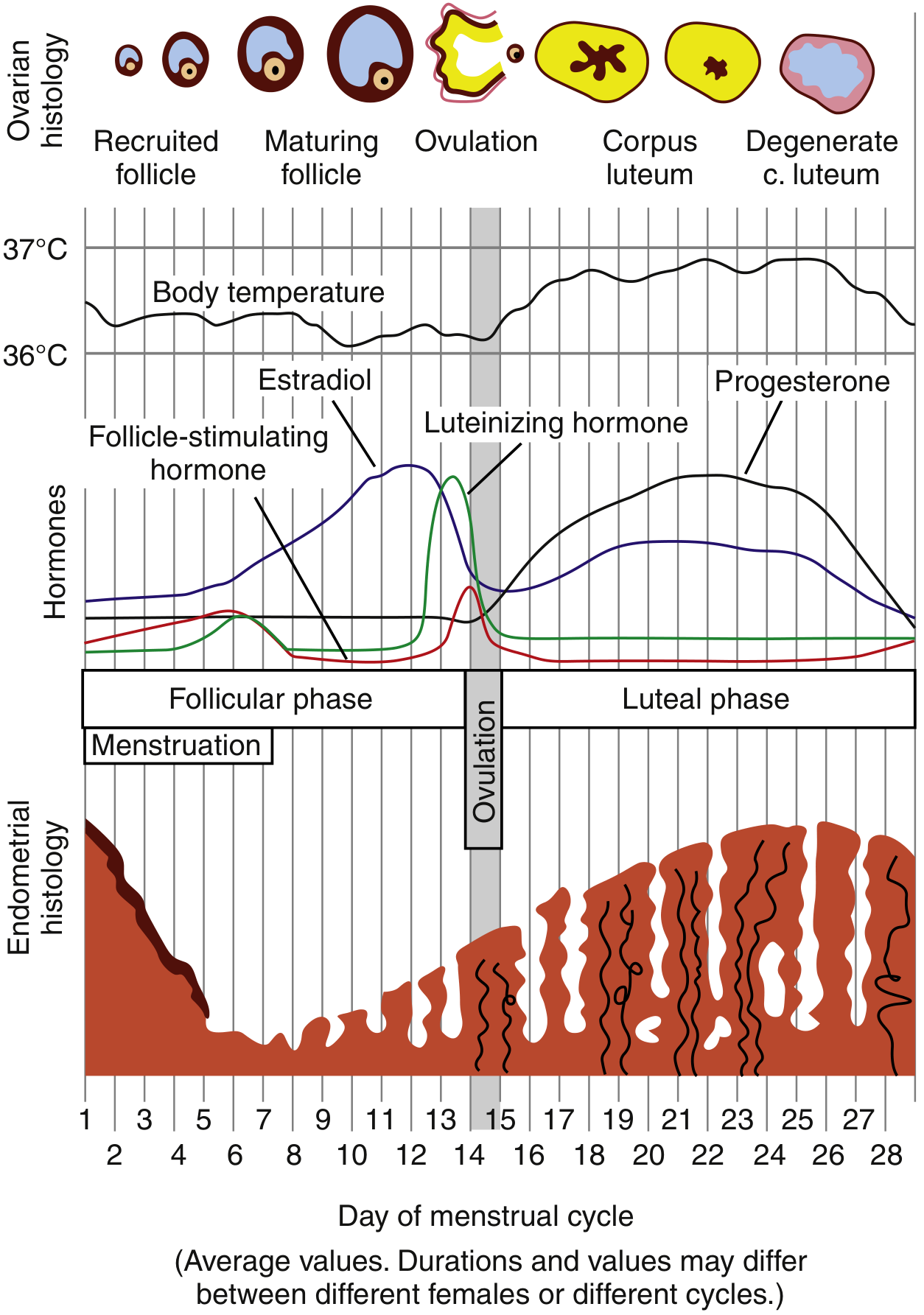
Normal Menstrual Cycle - Rosen's Emergency Medicine
Definition and Terminology
AUB has replaced older, imprecise terms such as menorrhagia, menometrorrhagia, and dysfunctional uterine bleeding (DUB). The term DUB should no longer be used. AUB describes irregularities in frequency, cyclicity, duration, and volume of menstrual flow outside of pregnancy. Up to one-third of women between menarche and menopause experience AUB symptoms at some point.
Preferred descriptors (FIGO/ACOG):
| Parameter | Abnormal extremes |
|---|---|
| Regularity | Absent / Irregular |
| Frequency | Infrequent (<21 days) or Frequent (>35 days) |
| Duration | Shortened or Prolonged (>7 days) |
| Volume | Light or Heavy (>80 mL/cycle) |
- Berek & Novak's Gynecology, p. 436
PALM-COEIN Classification (FIGO, 2011)
The PALM-COEIN system is the internationally accepted classification (FIGO 2011, endorsed by ACOG). It divides causes into structural (PALM) and non-structural (COEIN):
PALM - Structural Causes (diagnosable by imaging or histology)
| Category | Notes |
|---|---|
| P - Polyp (AUB-P) | Endometrial polyps cause intermenstrual, heavy, and postmenopausal bleeding. Associated with tamoxifen use and infertility. Diagnosed by TVUS (endometrial thickening), sonohysterography, or hysteroscopy. Malignant transformation risk is low in premenopausal women (0-13%), higher postmenopausally. |
| A - Adenomyosis (AUB-A) | Ectopic endometrial glands within the myometrium; causes heavy, painful menstrual bleeding. Classically a bulky, globular uterus on exam. |
| L - Leiomyoma (AUB-L) | Submucosal fibroids (AUB-LSM) most symptomatic; others (AUB-LO). Distort the endometrial cavity and increase surface area. Treated medically (elagolix, relugolix) or surgically (myomectomy, UAE, hysterectomy). |
| M - Malignancy/Hyperplasia (AUB-M) | Endometrial hyperplasia and cancer. Any postmenopausal bleeding must be evaluated urgently. Endometrial biopsy or D&C required. |
COEIN - Non-structural Causes
| Category | Notes |
|---|---|
| C - Coagulopathy (AUB-C) | 5-20% of women with heavy menstrual bleeding have an underlying coagulopathy, most commonly von Willebrand disease. Suspect if heavy bleeding since menarche, family history, or multi-system bleeding signs. |
| O - Ovulatory Dysfunction (AUB-O) | Most commonly caused by PCOS, hypothyroidism, hyperthyroidism, hyperprolactinemia, hypothalamic dysfunction, and primary ovarian insufficiency (POI). Anovulation leads to unopposed estrogen, causing estrogen breakthrough bleeding. |
| E - Endometrial (AUB-E) | Normal ovulatory cycles with disordered local endometrial hemostasis (prostaglandin, fibrinolysis dysregulation). Diagnosis of exclusion when no structural cause found. |
| I - Iatrogenic (AUB-I) | Oral contraceptives (30-40% of users), progestin-only methods (DMPA, implants, LNG-IUS), anticoagulants, antipsychotics (via hyperprolactinemia). |
| N - Not Otherwise Classified (AUB-N) | Rare causes: AV malformations, myometrial hypertrophy. |
- Sabiston Textbook of Surgery, p. 2937; Berek & Novak's Gynecology, pp. 437-442
Pathophysiology of Anovulatory Bleeding
This is the single most common mechanism underlying AUB (75% of cases with no demonstrable organic cause):
- Without ovulation, no corpus luteum forms and no progesterone is produced
- The endometrium proliferates under unopposed estrogen
- Low sustained estrogen → irregular, prolonged bleeding
- High sustained estrogen → amenorrhea followed by acute, heavy breakthrough bleeding
- Healing is dyssynchronous and fragile - unlike the uniform shedding of normal menses
About 20% of all AUB is in adolescents (immature HPO axis) and 50% is perimenopausal (incipient ovarian failure). - Goldman-Cecil Medicine, p. 2555
Causes by Age Group
| Age Group | Primary Causes |
|---|---|
| Infancy | Maternal estrogen withdrawal |
| Prepubertal | Vulvovaginitis, vaginal foreign body, precocious puberty, tumor |
| Adolescent | Anovulation (HPO immaturity), coagulopathy (von Willebrand), PCOS, pregnancy, STIs |
| Reproductive | Pregnancy complications, exogenous hormones, anovulation (PCOS), fibroids, polyps, thyroid disease |
| Perimenopausal | Anovulation, fibroids, polyps, thyroid disease |
| Postmenopausal | Atrophy (most common), endometrial cancer, polyps, HRT |
Postmenopausal bleeding is NOT included in PALM-COEIN and is considered its own entity - any such bleeding must be investigated for malignancy. - Sabiston, p. 2943
Clinical Evaluation
History
- Characterize bleeding: frequency, duration, volume (clots? flooding? pad count)
- Menstrual history (age at menarche, prior cycle regularity)
- Reproductive history, contraceptive use
- Medications (anticoagulants, hormones, antipsychotics)
- Systemic symptoms: weight change, heat/cold intolerance, galactorrhea, hirsutism, acne
- Family history of bleeding disorders
- STI risk factors
Physical Examination
- Vital signs (hemodynamic stability)
- Signs of anemia (pallor, tachycardia)
- Signs of androgen excess (hirsutism, acne)
- Thyroid exam
- Pelvic exam: uterine size/contour, adnexal masses, cervical lesions, signs of infection
Laboratory Workup
| Test | Indication |
|---|---|
| Urine/serum hCG | All reproductive-age women - must exclude pregnancy first |
| CBC + platelet count | All cases; assess anemia and thrombocytopenia |
| TSH | Thyroid dysfunction (both hypo- and hyperthyroidism cause AUB) |
| Prolactin | If anovulation or galactorrhea |
| Coagulation screen (PT, PTT, vWF) | If heavy since menarche, family history, multi-system bleeding |
| Cervical cancer screening | If not up to date |
| STI screening | If risk factors present; Chlamydia linked to AUB via endometrial inflammation |
| Fasting glucose | Metabolic syndrome / PCOS workup |
- Sabiston, p. 2939; Rosen's Emergency Medicine, p. 1419
Imaging
- Transvaginal ultrasound (TVUS): First-line imaging. Identifies fibroids, polyps, endometrial thickening. In postmenopausal women, endometrial thickness <4-5 mm reliably excludes endometrial cancer.
- Sonohysterography (saline infusion sonography): Superior to TVUS alone for intracavitary lesions (polyps, submucosal fibroids).
- Hysteroscopy: Gold standard for direct visualization and biopsy of intracavitary lesions.
- MRI: Best for characterizing adenomyosis and mapping fibroids pre-operatively.
Endometrial Sampling - Indications
Endometrial biopsy is indicated to exclude hyperplasia/malignancy in:
-
All women ≥45 years with AUB
-
Women <45 years with: obesity, chronic anovulation/PCOS (unopposed estrogen), persistent AUB refractory to medical management, elevated familial cancer risk (Lynch syndrome)
-
Sabiston, p. 2941
Management
Acute/Emergency Management (Heavy Bleeding, Hemodynamic Instability)
- Resuscitation: IV fluids, blood products as needed
- IV conjugated equine estrogen: 25 mg IV every 4-6 hours (up to 3 doses) - achieves hemostasis in anovulatory bleeding by rapidly proliferating the denuded endometrium. Start simultaneous progestin (medroxyprogesterone acetate 5-10 mg orally).
- High-dose oral contraceptive pills: 1 combined OCP every 6 hours for 5-7 days - effective for hemodynamically stable patients with profuse anovulatory bleeding. Expect heavy withdrawal bleed 2-4 days after stopping.
- Intrauterine tamponade: 26-French Foley catheter inflated with 30 mL saline as a temporary measure.
- Surgical: Urgent D&C, uterine artery embolization, endometrial ablation, or hysterectomy for refractory cases.
Non-Acute / Maintenance Medical Management
| Agent | Use |
|---|---|
| Combined OCPs (cyclically) | Anovulatory AUB - regulates cycle, prevents endometrial build-up, reduces flow volume |
| Progestin-only therapy (MPA 5-10 mg x 10 days, norethindrone 5 mg/day) | When estrogen contraindicated; induces withdrawal bleed |
| LNG-IUS (Mirena) | Most effective medical treatment for HMB; reduces flow by 80-90%; good for fibroids and adenomyosis |
| NSAIDs (mefenamic acid, ibuprofen) | Reduces blood loss ~25-30% in ovulatory HMB; also for breakthrough bleeding with contraceptives |
| Tranexamic acid | Antifibrinolytic; reduces heavy menstrual blood loss ~40-50% |
| GnRH agonists (leuprolide) | Pre-surgical fibroid reduction; also for adenomyosis |
| GnRH antagonists (elagolix, relugolix 40 mg/day) | Approved for uterine fibroid-related HMB; oral administration advantage |
| Thyroid/prolactin correction | When AUB is secondary to endocrine cause |
- Goldman-Cecil, p. 2556; Berek & Novak's, p. 440
Surgical Management
| Procedure | Indication |
|---|---|
| Endometrial ablation | Refractory HMB with completed family; not 100% effective |
| Hysteroscopic polypectomy | AUB-P |
| Myomectomy / UAE | Symptomatic leiomyoma with fertility preservation desired |
| Hysterectomy | Definitive; for refractory AUB, adenomyosis, failed ablation, or confirmed malignancy |
| D&C | Acute bleeding control; diagnostic and therapeutic |
Special Considerations
Adolescents
- Prioritize coagulopathy workup (von Willebrand disease is underdiagnosed in this group)
- HPO axis immaturity is common for up to 3 years post-menarche
- Rule out pregnancy and STIs
Postmenopausal Bleeding
- Most common cause: endometrial atrophy
- But endometrial carcinoma must be excluded in every case
- TVUS (endometrial thickness <4-5 mm) and/or endometrial biopsy required
Primary Ovarian Insufficiency (POI)
- Occurs in ~1/100 women by age 40, 1/1,000 by age 30
- Presents with oligomenorrhea or irregular bleeding before amenorrhea
- Often significantly delayed in diagnosis; menstrual cycle is a "vital sign" for ovarian health
- Berek & Novak's, p. 440
Iatrogenic Bleeding
- Breakthrough bleeding on OCPs: affects 30-40% of users; typically resolves by cycle 3
- LNG-IUS: initial irregular bleeding is expected and should be counseled pre-insertion
- Always screen for Chlamydia in women with new-onset AUB while on hormonal contraception
Key Differential Diagnosis Points
| Feature | Suggests |
|---|---|
| Irregular, unpredictable heavy bleeding | Anovulation (PCOS, perimenopausal) |
| Heavy but regular cycles | Structural lesion (fibroid, polyp, adenomyosis) or coagulopathy |
| Heavy since menarche | Von Willebrand disease or other coagulopathy |
| Intermenstrual / postcoital bleeding | Cervical lesion, polyp, STI, endometrial pathology |
| Postmenopausal bleeding | Atrophy, cancer, polyp, HRT |
| Associated with galactorrhea | Hyperprolactinemia |
| Associated with weight gain, cold intolerance | Hypothyroidism |
| Associated with hirsutism / acne | PCOS |
Sources
- Berek & Novak's Gynecology, pp. 436-443
- Goldman-Cecil Medicine, pp. 2555-2556
- Sabiston Textbook of Surgery, pp. 2937-2945
- Rosen's Emergency Medicine, pp. 1419-1420
- Harrison's Principles of Internal Medicine 22E (2025), p. 743
This is a shared conversation. Sign in to Orris to start your own chat.