Diabetes mellitus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetes mellitus" AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive material across classification, pathogenesis, diagnosis, treatment, and complications. Let me compile the full answer.
Diabetes Mellitus - Comprehensive Overview
Definition
Diabetes mellitus (DM) is a heterogeneous group of metabolic disorders with distinct genetic, etiologic, immunologic, and pathophysiologic mechanisms that result in glucose intolerance and chronic hyperglycemia. Patients develop insulin deficiency, impaired peripheral insulin action, or both. Chronic exposure to hyperglycemia and glycemic variability causes both acute (DKA, hyperosmolar state, hypoglycemia) and long-term (micro- and macrovascular) complications.
- Textbook of Family Medicine 9e
Classification (ADA 1997 Revised Criteria)
The ADA revised its classification in 1997, replacing the older terms IDDM/NIDDM and juvenile-onset/adult-onset with the current four-category system. Classification is based on etiology, not treatment.
| Type | Key Feature |
|---|---|
| Type 1 DM (T1DM) | Autoimmune destruction of pancreatic β-cells → absolute insulin deficiency |
| Type 2 DM (T2DM) | Insulin resistance + progressive β-cell failure; ~90% of all cases |
| Gestational DM (GDM) | Hyperglycemia first recognised during pregnancy |
| Other specific types | Monogenic (MODY, neonatal DM), exocrine pancreatic disease (cystic fibrosis, pancreatitis), endocrinopathies (Cushing's, acromegaly, glucagonoma), drugs (glucocorticoids, thiazides, antiretrovirals) |
- Tietz Textbook of Laboratory Medicine, 7th Edition
Type 1 Diabetes Mellitus
-
Represents 5-10% of all DM cases.
-
Caused by autoimmune destruction of β-cells; patients have insulinopenia and are dependent on insulin to survive and prevent ketosis.
-
Most patients carry autoantibodies (islet cell antibodies, anti-GAD65, anti-IA-2, anti-ZnT8).
-
Peak incidence in childhood/adolescence; ~75% present before age 18, but onset may occur at any age.
-
Three staged model:
- Stage 1: Normoglycemic, multiple islet autoantibodies present
- Stage 2: Dysglycemia (IFG/IGT) + multiple autoantibodies
- Stage 3: Overt hyperglycemia with clinical symptoms
-
~30% present initially with diabetic ketoacidosis (DKA).
-
Tietz Textbook of Laboratory Medicine, 7th Edition
Type 2 Diabetes Mellitus
-
Represents ~90% of all DM cases worldwide.
-
Characterized by insulin resistance and progressive β-cell failure.
-
Patients are not ketosis-prone and are not dependent on insulin to survive (though many require it for glycemic control).
-
Strongly associated with obesity - weight loss alone can improve hyperglycemia.
-
Usually presents after age 40, but increasingly seen in children and adolescents as obesity prevalence rises (in some Asian populations, T2DM represents 50-90% of youth-onset diabetes).
-
Genetic underpinning: genome-wide association studies have identified 18+ polymorphisms increasing susceptibility.
-
Textbook of Family Medicine 9e
Diagnostic Criteria (ADA)
Any one of the following confirms diabetes:
| Test | Diabetes | Prediabetes (IFG/IGT) |
|---|---|---|
| Fasting Plasma Glucose (FPG) | ≥126 mg/dL (7.0 mmol/L) | 100-125 mg/dL |
| 2-hour OGTT (75g) | ≥200 mg/dL (11.1 mmol/L) | 140-199 mg/dL |
| HbA1c | ≥6.5% (48 mmol/mol) | 5.7-6.4% |
| Random plasma glucose + symptoms | ≥200 mg/dL | - |
In the absence of symptoms, a single abnormal test should be confirmed by repeat testing.
Pathophysiology
T1DM
Autoimmune T-cell-mediated attack on β-cells → progressive β-cell loss → absolute insulin deficiency → unopposed glucagon action → hyperglycemia, lipolysis, ketogenesis → DKA.
T2DM - "Ominous Octet" (key mechanisms)
- Insulin resistance in muscle, liver, and adipose tissue
- β-cell failure (patients with prediabetes have already lost ~80% of β-cell function)
- Increased hepatic glucose production
- Decreased incretin effect (GIP/GLP-1 impairment)
- Increased glucagon secretion
- Increased renal glucose reabsorption
- Neurotransmitter dysfunction
- Adipocyte dysfunction (increased free fatty acid release)
Clinical Presentation
Classic symptoms (hyperglycemia):
- Polyuria, polydipsia, polyphagia
- Unexplained weight loss
- Fatigue, blurred vision
- Frequent infections (urinary, skin, fungal)
T1DM - usually acute onset, often presenting with DKA
T2DM - often insidious; many patients are asymptomatic at diagnosis; discovered on routine screening
T2DM - often insidious; many patients are asymptomatic at diagnosis; discovered on routine screening
Acute Complications
1. Diabetic Ketoacidosis (DKA)
- Life-threatening emergency, predominantly in T1DM
- Caused by absolute or relative insulin deficiency → elevated ketone bodies (acetoacetate, β-hydroxybutyrate)
- Features: hyperglycemia, anion-gap metabolic acidosis, ketonemia/ketonuria, dehydration
- Treatment: IV fluids, insulin infusion, electrolyte replacement (especially potassium)
2. Hyperglycemic Hyperosmolar State (HHS)
- Predominantly in T2DM
- Extreme hyperglycemia (>600 mg/dL), hyperosmolarity, profound dehydration, minimal ketosis
- High mortality if not treated promptly
3. Hypoglycemia
- Most common acute complication of insulin/sulfonylurea therapy
- Symptoms: diaphoresis, tremor, palpitations, confusion, seizure
- Treatment: 15-15 rule (15g fast-acting carbs, recheck in 15 minutes); severe cases: glucagon IM or IV dextrose
Chronic Complications
Microvascular
| Complication | Notes |
|---|---|
| Diabetic nephropathy | Leading cause of end-stage renal disease (ESRD); microalbuminuria is earliest marker |
| Diabetic retinopathy | Leading cause of new-onset blindness in working-age adults; annual retinal exams essential |
| Diabetic neuropathy | Most common - distal symmetric polyneuropathy (stocking-glove); also autonomic neuropathy |
Macrovascular
- Coronary artery disease (2-4x increased risk) - leading cause of death in T2DM
- Cerebrovascular disease (stroke)
- Peripheral arterial disease → foot ulcers, gangrene, amputation
All from: Textbook of Family Medicine 9e; Histology: A Text and Atlas
Management
Type 1 DM
- Insulin replacement is mandatory - no alternative
- Regimens: basal-bolus (multiple daily injections) or continuous subcutaneous insulin infusion (insulin pump)
- Carbohydrate counting and regular SMBG/CGM
- HbA1c target: <7% for most adults
Type 2 DM - Step-Up Algorithm
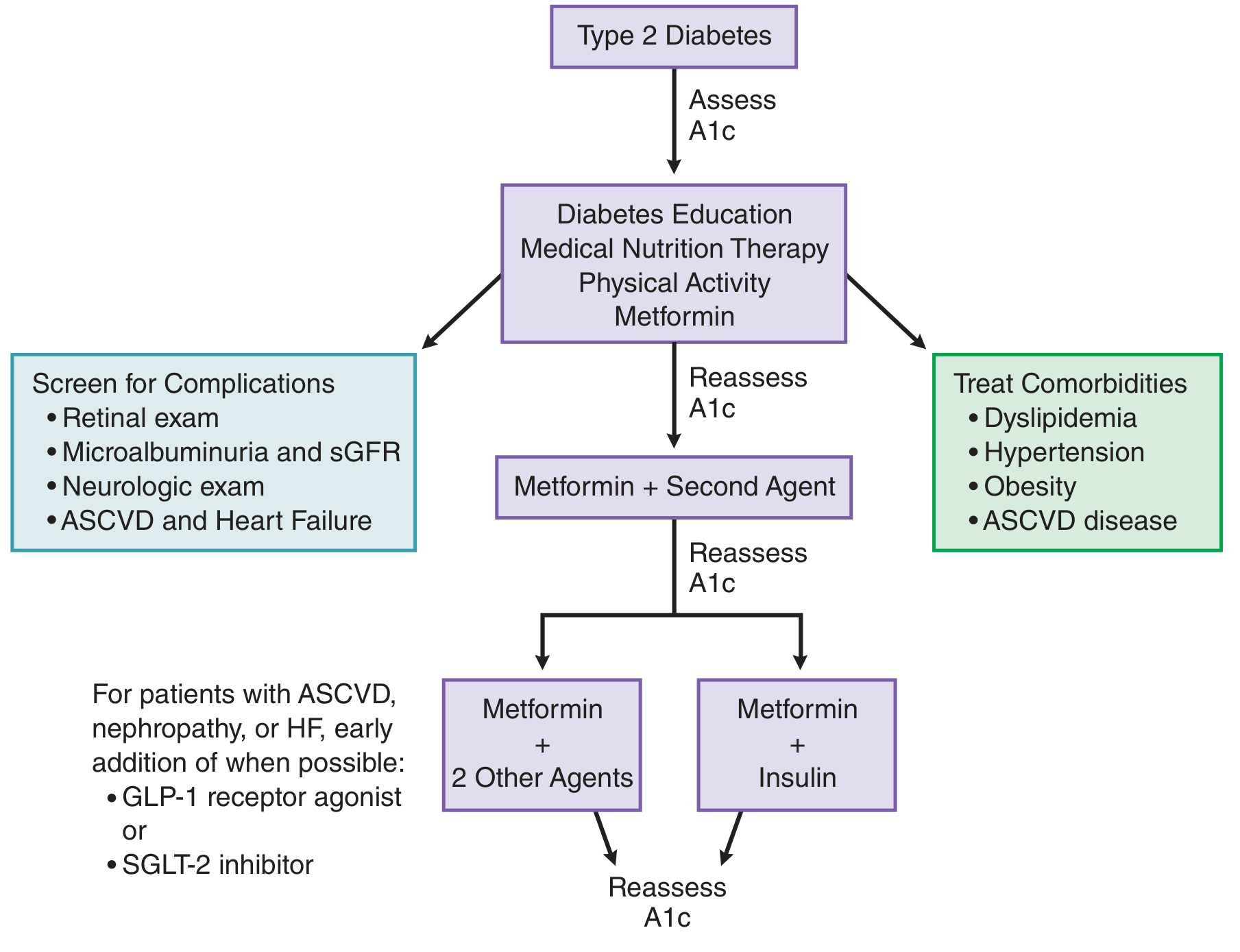
Step 1 - Lifestyle + Metformin (first-line at diagnosis):
- Medical nutrition therapy, weight loss, ≥150 min/week moderate aerobic activity
- Metformin: reduces hepatic glucose production; first-line per ADA and most major guidelines; also beneficial for cardiovascular outcomes (UKPDS)
Step 2 - Add a second agent if A1c target not met within 2-3 months:
| Drug Class | Examples | Key Advantage |
|---|---|---|
| Sulfonylureas | Glipizide, glyburide, glimepiride | Inexpensive, proven |
| SGLT-2 inhibitors | Empagliflozin, canagliflozin, dapagliflozin | Heart failure, CKD benefit; weight loss |
| GLP-1 receptor agonists | Liraglutide, semaglutide, dulaglutide | ASCVD benefit; weight loss |
| DPP-4 inhibitors | Sitagliptin, saxagliptin | Weight neutral |
| Thiazolidinediones | Pioglitazone | Insulin sensitizer |
| Basal insulin | Glargine, detemir, degludec | Powerful glycemic control |
Key 2022 guidance: For patients with established ASCVD, heart failure, or diabetic nephropathy, a GLP-1 receptor agonist or SGLT-2 inhibitor should be added early in the treatment course.
Step 3: Metformin + 2 additional agents, OR metformin + insulin
- Goodman & Gilman's The Pharmacological Basis of Therapeutics; Textbook of Family Medicine 9e
Monitoring
| Parameter | Frequency | Target |
|---|---|---|
| HbA1c | Every 3 months until stable, then every 6 months | <7% (most adults) |
| Fasting blood glucose | Daily (T1DM), variable (T2DM) | 80-130 mg/dL |
| Postprandial glucose | Per clinical need | <180 mg/dL |
| Blood pressure | Each visit | <130/80 mmHg |
| Lipids | Annually | LDL <70 mg/dL (high risk) |
| Urine albumin:creatinine | Annually | <30 mg/g |
| Retinal exam | Annually | - |
| Foot exam | Annually + each visit | - |
Prediabetes Management
Patients with prediabetes (IFG/IGT/HbA1c 5.7-6.4%) have already lost ~80% of β-cell function and are maximally insulin resistant. Key interventions:
-
Weight loss of 5-7% of body weight
-
≥150 min/week moderate physical activity
-
Metformin (especially if A1c trending above 6% despite lifestyle changes)
-
Annual monitoring for progression to T2DM
-
Textbook of Family Medicine 9e
Recent Evidence (2024-2026)
- Digital Interventions for T2DM Self-Management (2024) - Systematic review/meta-analysis confirming digital tools improve glycemic outcomes [PMID: 39037772]
- GLP-1 RA gastrointestinal adverse effects (2025) - Systematic review characterizing GI side effects of GLP-1 receptor agonists (nausea, vomiting, diarrhea most common) [PMID: 40499738]
- Triglyceride-glucose index (TyG) (2024) - Meta-analysis validating TyG index as a useful marker of insulin resistance and cardiovascular risk in diabetes [PMID: 39180024]
Summary Table: T1DM vs T2DM
| Feature | Type 1 | Type 2 |
|---|---|---|
| Proportion of DM | 5-10% | ~90% |
| Onset | Acute, usually childhood | Insidious, usually >40 yrs |
| Mechanism | Autoimmune β-cell destruction | Insulin resistance + β-cell failure |
| Autoantibodies | Present (anti-GAD, anti-IA-2) | Absent |
| Ketosis prone | Yes | Rarely |
| Body habitus | Normal or thin | Often obese |
| C-peptide | Low/absent | Normal or elevated initially |
| Insulin required | Always | Eventually in many |
| First-line therapy | Insulin | Metformin + lifestyle |
This is a shared conversation. Sign in to Orris to start your own chat.