Detailed notes on Pulmonary artery hypertension in systemic sclerosis: Screening, diagnosis and recent trends in treatment. From rheumatology textbooks and major journals
"pulmonary arterial hypertension" AND "systemic sclerosis" AND screening
pulmonary arterial hypertension systemic sclerosis screening diagnosis treatment 2024 2025 guidelines
PMID: 41708122
PMID: 41085415
https://pmc.ncbi.nlm.nih.gov/articles/PMC12536151
"systemic sclerosis" AND "pulmonary arterial hypertension" AND sotatercept
PMID: 38531379
PMID: 40905396
PMID: 41594679
Pulmonary Arterial Hypertension in Systemic Sclerosis: Detailed Clinical Notes
1. Epidemiology and Clinical Significance
- Fishman's Pulmonary Diseases: "PAH (WHO Group 1) occurs in approximately 10% of cases of systemic sclerosis and is primarily seen in the limited cutaneous form (CREST syndrome)."
- Goldman-Cecil Medicine, p. 814: "The prevalence of pulmonary arterial hypertension [in SSc] is in the range of 7 to 12%."
2. Pathophysiology
2a. Vascular Pathology
- Obliterative intimal lesions with matrix accumulation (see histology below)
- Smooth muscle hyperplasia and medial thickening
- Adventitial expansion
- Endothelial dysfunction with reduced nitric oxide (NO) and prostacyclin production, and increased endothelin-1 (ET-1) secretion
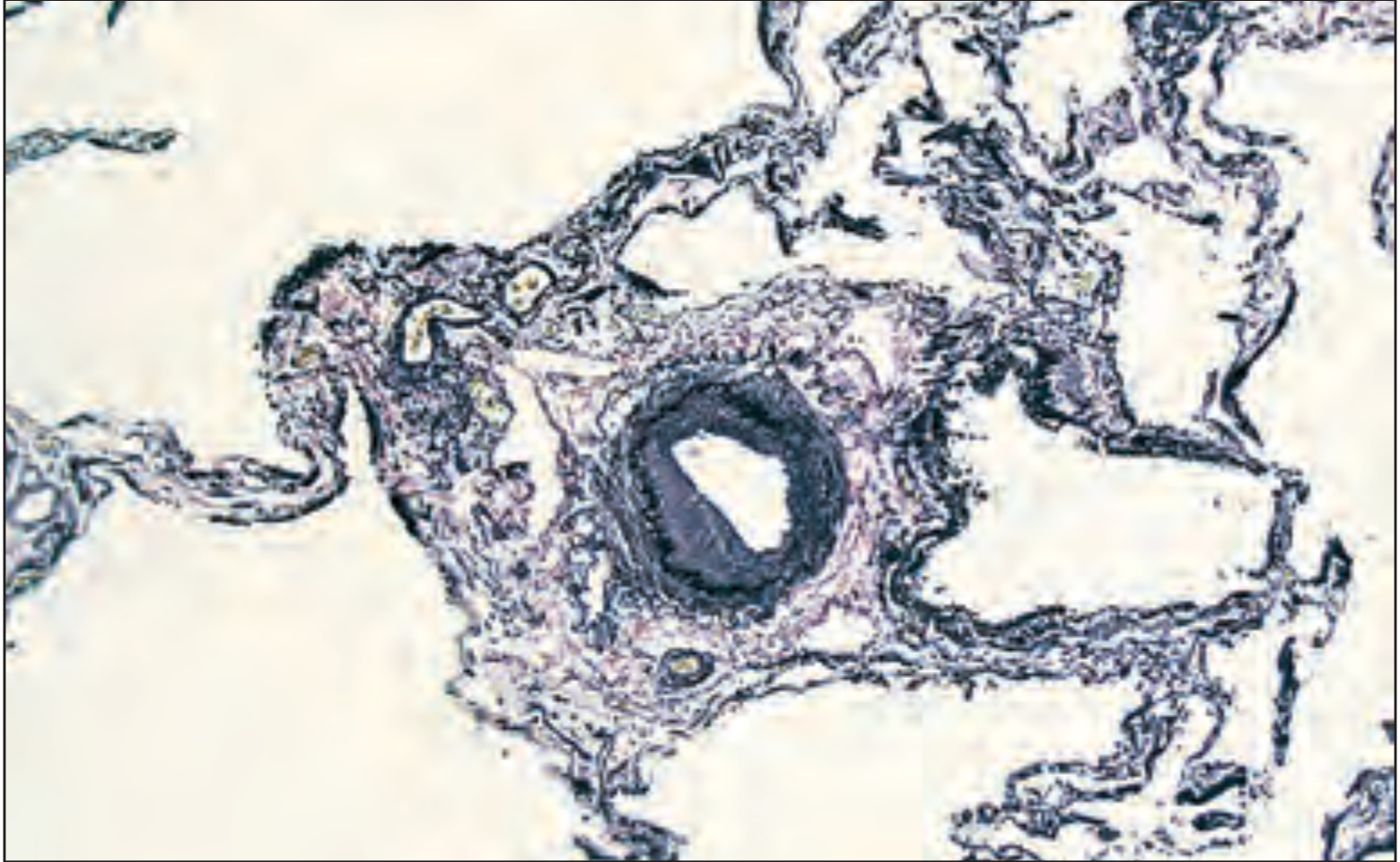
- Pulmonary veno-occlusive disease (PVOD) is rare in iPAH but common in SSc-PAH, contributing to poor response to vasodilators
- Plexogenic lesions are rare in SSc-PAH (unlike iPAH)
- Pulmonary thrombosis is more prevalent in SSc-PAH
- Patients with SSc-PAH show impaired RV-PA coupling at much lower RV afterload levels than iPAH, linked to increased interstitial RV cardiac fibrosis
- Rheumatology 2022 (Elsevier), p. 6565: "Pulmonary venoocclusive disease, which is rare in idiopathic PAH, occurs frequently in SSc-PAH, along with evidence of pulmonary thrombosis."
2b. Immune and Molecular Mechanisms
- Immune dysregulation: T-cell activation, B-cell dysregulation, autoantibody production
- Chronic inflammation: IL-6, IL-8, VEGF, TGF-β overexpression
- Activin/TGF-β pathway dysregulation: now a recognized therapeutic target
- BMPR2 pathway impairment (as in iPAH), contributing to impaired vascular repair
- Endothelin-1 excess: a potent vasoconstrictor and proliferative mediator - the basis for ERA therapy
3. Screening
3a. Who to Screen
| Risk Factor | Significance |
|---|---|
| Longer disease duration (>3 years) | Increased cumulative risk |
| Older age | Independent predictor |
| Severe Raynaud's/digital ulcers | Reflects vasculopathy severity |
| Multiple/large telangiectasias | Marker of vascular disease extent |
| Isolated DLCO decline | Surrogate of pulmonary vascular disease |
| FVC%/DLCO% ratio >1.6 | Suggests vascular >parenchymal disease |
| NT-proBNP elevation (>395 pg/mL) | Right heart strain |
| Anti-centromere antibody | Strongly associated with lcSSc-PAH |
| Anti-U1-RNP, U3-RNP, Th/To antibodies | Additional PAH risk markers |
| Anti-Ro52 antibodies | Emerging risk marker |
3b. Screening Tests
- DLCO is typically significantly reduced, often to <40-60% predicted, frequently years before PAH becomes manifest
- The FVC%/DLCO% ratio >1.6 is a strong clue to pulmonary vascular disease (as opposed to ILD, where both FVC and DLCO fall)
- An isolated low DLCO without significant restriction or obstruction should trigger further evaluation
- Rheumatology 2022 (Elsevier): "The diffusing capacity for carbon monoxide (DLCO) almost always is significantly decreased long before PAH develops, often as low as 40%."
- First-line noninvasive screening tool; recommended annually in all SSc patients
- The 2022 ESC/ERS guidelines updated the echocardiographic threshold: TRV >2.8 m/s (previously 2.9 m/s) is now the cut-off for intermediate-high probability of PH, especially combined with other echocardiographic signs
- RVSP >45 mmHg predicts PAH by RHC with ~95% accuracy
- Additional echo signs of PH: RV/LV basal diameter ratio ≥1.0, interventricular septal flattening, TAPSE/sPAP ratio <0.55 mm/mmHg, PA diameter >25 mm, RVOT acceleration time <105 ms
- Echo alone carries important false-positive and false-negative rates in SSc, necessitating RHC for confirmation
- NT-proBNP: even modest elevations >395 pg/mL indicate right heart strain and should trigger evaluation
- BNP: used alongside NT-proBNP for risk stratification
- FVC%/DLCO% ratio: composite PFT biomarker
- Autoantibodies: anti-centromere, U1-RNP, U3-RNP, Th/To, Ro52 as risk stratification tools
- Can be normal early; as disease progresses shows RV hypertrophy, right axis deviation, right heart strain pattern
3c. The DETECT Algorithm
- Disease duration >3 years
- DLCO <60% predicted
- FVC ≥40% predicted (excludes severe ILD)
- FVC%/DLCO% ratio
- NT-proBNP
- Serum urate
- Any telangiectasias
- Anti-centromere antibody
- Right axis deviation on ECG → If score exceeds threshold: proceed to echocardiography
- TRV (tricuspid regurgitation velocity)
- Right atrial area → If combined score exceeds threshold: refer for RHC
- Murray & Nadel's Respiratory Medicine: "These analyses identified eight clinical variables that, when applied in a two-step algorithm, predicted the presence of PH on RHC with a low rate (4%) of missed PAH diagnoses."
- Firestein & Kelley's: "DETECT has been validated across many general scleroderma cohorts exhibiting a consistently high sensitivity and negative predictive value, but modest specificity and positive predictive value."
3d. ASIG (Australian Scleroderma Interest Group) Algorithm
4. Diagnosis
4a. Hemodynamic Definition
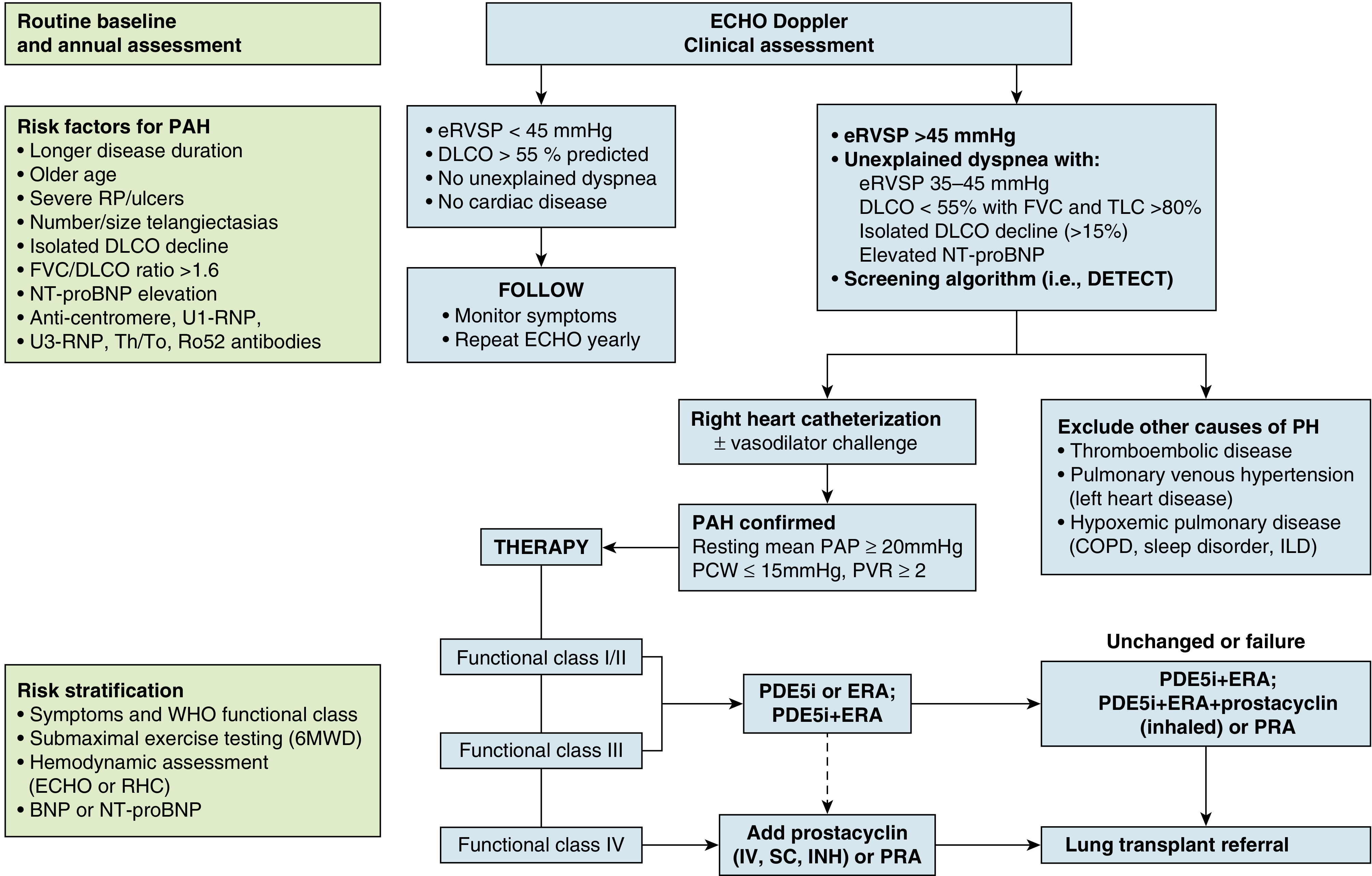
- Mean pulmonary arterial pressure (mPAP) ≥20 mmHg (lowered from >25 mmHg)
- Pulmonary capillary wedge pressure (PCWP) ≤15 mmHg
- Pulmonary vascular resistance (PVR) >2 Wood Units (lowered from ≥3 WU)
- Firestein & Kelley's, p. 1859: "It is now defined as resting mean pulmonary arterial pressure equal to or greater than 20 mm Hg, with normal pulmonary capillary wedge pressure equal to or less than 15 mm Hg and pulmonary vascular resistance >3 wood units, although this threshold has been recently lowered to >2 wood units in the 2022 ESC/ERS guidelines."
4b. Right Heart Catheterization (RHC)
- eRVSP >45 mmHg on ECHO
- Unexplained dyspnea with eRVSP 35-45 mmHg + additional echo signs
- DETECT/ASIG algorithm threshold reached
- Low DLCO + normal FVC + elevated BNP/NT-proBNP, even with normal ECHO
- Dyspnea without ILD and progressive DLCO decline
- Direct measurement of mPAP, PCWP, cardiac output, PVR
- Differentiation of PAH from left heart disease (group 2 PH) - especially important in SSc where diastolic dysfunction and PVOD co-exist
- Vasodilator challenge (acute vasoreactivity testing) - though acute response is rare in SSc-PAH and calcium-channel blocker therapy is generally not appropriate
4c. Distinguishing PH Types in SSc
- Group 1 PAH (pure pulmonary vascular disease) - most common in lcSSc
- Group 2 PH (left heart disease) - diastolic dysfunction, elevated PCWP
- Group 3 PH (ILD-associated) - must have significant ILD + mPAP >35 mmHg or PVR >5 WU
- PVOD phenotype - SSc-specific, poor prognosis, risk of pulmonary edema with vasodilators
4d. Additional Diagnostic Investigations
- HRCT chest: assess for ILD (NSIP pattern most common in SSc), exclude significant fibrosis driving group 3 PH; also can show PA enlargement
- V/Q scan: exclude chronic thromboembolic PH (group 4) - important to rule out in all patients
- 6-minute walk test (6MWT): baseline functional assessment; poor correlation with hemodynamic severity in SSc compared to iPAH
- Cardiopulmonary exercise testing (CPET): may improve diagnostic accuracy, especially for "exercise-induced PH" (mPAP >30 mmHg on exercise RHC); role not yet standardized
- Cardiac MRI: identifies subclinical RV dysfunction and myocardial fibrosis
- Nailfold capillaroscopy: "late" SSc pattern (avascular areas, giant capillaries) correlates with end-organ vascular disease including PAH (Ickinger et al., Best Pract Res Clin Rheumatol 2026 [PMID: 41826085])
5. Clinical Approach (Flowchart)
6. Risk Stratification at Diagnosis and Follow-Up
- Low risk: FC I-II, 6MWD >440 m, NT-proBNP <300 ng/L, low/normal RV function, mPAP <35-40 mmHg, PVR <5 WU
- Intermediate-low risk
- Intermediate-high risk
- High risk: FC IV, 6MWD <165 m, NT-proBNP >1400 ng/L, pericardial effusion, CI <2.0 L/min/m², RA area >26 cm²
- If not achieving low-risk at 3-6 months: escalate therapy
- High-risk category: consider listing for lung transplant
7. Treatment
7a. General Principles
- Rheumatology 2022 (Elsevier): "Scleroderma patients do not respond as well to these many treatments compared to those with idiopathic PAH. Thus in scleroderma, once the diagnosis of PAH is confirmed by RHC, treatment with at least one drug should be instituted."
7b. Conventional Vasodilator Therapies
Endothelin Receptor Antagonists (ERAs)
| Drug | Selectivity | Route | Dosing | Key Adverse Effects |
|---|---|---|---|---|
| Bosentan | Non-selective (ETA+ETB) | Oral | 62.5 mg BD x 4 wks, then 125 mg BD | LFT elevation (10%), teratogenic, fluid retention, reduces oral anticoagulant effect |
| Ambrisentan | ETA-selective | Oral | 5-10 mg OD | Teratogenic, fluid retention, peripheral edema |
| Macitentan | Non-selective (tissue-specific) | Oral | 10 mg OD | Teratogenic, fluid retention, anemia |
PDE-5 Inhibitors (Nitric Oxide Pathway)
| Drug | Route | Dosing | Comments |
|---|---|---|---|
| Sildenafil | Oral | 20 mg TDS | Well tolerated; headache, visual disturbance |
| Tadalafil | Oral | 40 mg OD | Longer duration of action |
Soluble Guanylate Cyclase (sGC) Stimulator
| Drug | Route | Comments |
|---|---|---|
| Riociguat | Oral 2.5 mg BD | Cannot be used with PDE5i; reserved for severe disease or PDE5i failure |
Prostacyclin Pathway
| Drug | Route | Dosing | Comments |
|---|---|---|---|
| Epoprostenol (prostacyclin) | Continuous IV | Titrated | Gold-standard for FC IV; only prostacyclin with RCT specifically in SSc-PAH showing improved 6MWD, functional class, hemodynamics |
| Treprostinil | SC/IV/inhaled/oral | Titrated | SC site pain; less abrupt deterioration than epoprostenol if interrupted |
| Iloprost | Inhaled | 6-9x daily | Licensed for PAH |
| Selexipag (IP receptor agonist) | Oral | BD | GRIPHON trial included CTD-PAH; recently approved |
7c. Combination Therapy - Key Trials
- Initial combination vs. monotherapy in treatment-naive PAH
- Sub-analysis of CTD-PAH/SSc-PAH patients:
- Risk of clinical failure 52% lower with combination vs. monotherapy in CTD-PAH (HR 0.483)
- 54% lower in SSc-PAH specifically (HR 0.463)
- Combination ambrisentan + tadalafil is now the preferred initial strategy for most SSc-PAH patients
- Rheumatology 2022 (Elsevier), p. 2964
- Ambrisentan in SSc patients with mildly elevated mPAP (21-24 mmHg) - to assess benefit of early intervention in "borderline" PAH
- Important in context of lowered diagnostic threshold
- Rheumatology 2022 (Elsevier), p. 2979
- Bearzi P et al., Clin Exp Rheumatol 2024 [PMID: 38819960]: Bosentan reduces echocardiographic systolic PAP in SSc-related PH
7d. Sotatercept - Major Recent Advance
- Mechanism: Sequesters activin ligands (particularly activin A) that drive vascular smooth muscle proliferation and remodeling
- STELLAR trial: Demonstrated significant improvement in 6MWD, hemodynamics, and clinical worsening in patients already on background dual/triple PAH therapy
- ZENITH trial (Humbert M et al., NEJM 2025): Sotatercept in high-risk PAH patients showed markedly improved outcomes [PMID referenced in Villa et al. 2026]
- SSc-PAH patients were included in these trials; the activin pathway is particularly relevant given the pro-fibrotic milieu in SSc
- SSc-PAH-specific data are emerging (NCT06865118 observational protocol 2025)
- Current 2024 7th WSPH treatment algorithm incorporates sotatercept as an add-on therapy for patients not at low risk despite dual therapy
7e. Immunosuppressive Therapy in SSc-PAH
- Cyclophosphamide, mycophenolate mofetil: Limited role; may benefit inflammatory phenotypes or overlap CTD-PAH
- Rituximab (anti-CD20): Emerging evidence; Touil A et al. systematic review (Expert Rev Respir Med 2026, PMID: 40905396): RTX appeared effective and safe in CTD-PH including SSc cases; primarily prospective data from Russia and USA; improvement in clinical/paraclinical parameters; limited to 6 studies
- IL-6 receptor inhibitors (tocilizumab): Under investigation given IL-6's role in vascular remodeling in SSc
- Glucocorticoids: Low-dose may have a role in inflammatory phenotypes but high-dose steroids risk SSc renal crisis
7f. 7th WSPH 2024 Treatment Algorithm
- Initial risk stratification (4-strata model)
- Low/intermediate-low risk (FC I-II): Upfront dual therapy (ERA + PDE5i; ambrisentan + tadalafil preferred)
- Intermediate-high/high risk (FC III-IV): Upfront dual or triple therapy; consider adding prostacyclin pathway agent early; IV epoprostenol for FC IV
- Re-assess at 3-6 months: If not achieving low risk, escalate
- Sotatercept: Add-on for patients not at low risk on background oral therapy (per STELLAR/ZENITH data)
- Lung transplant referral: Failed maximal medical therapy
- Lower threshold for early combination therapy
- Lower threshold for escalation
- Comorbidities (ILD, cardiac fibrosis, GI disease) must be actively managed alongside PAH therapy
- Avoid acute vasoreactivity testing with calcium-channel blockers
7g. Surgical/Interventional Options
- Balloon pulmonary angioplasty (BPA): For CTEPH (Group 4); not indicated in SSc-PAH group 1
- Atrial septostomy: Rarely used; may provide palliative benefit in refractory high-risk PAH
- Lung transplant: Considered when PAH therapy fails; outcomes in SSc are complicated by extrapulmonary SSc disease (esophageal dysmotility, bowel disease, systemic fibrosis); careful patient selection required
8. Prognosis and Follow-Up Monitoring
- Older age at diagnosis
- Worse baseline hemodynamics (lower CI, higher PVR)
- Lower 6MWD
- Elevated NT-proBNP
- FC III/IV at diagnosis
- RV dysfunction (TAPSE, tricuspid annular plane systolic excursion)
- Impaired RV-PA coupling (TAPSE/sPAP ratio)
- Co-existing ILD
- ECHO + TRV, TAPSE, RA area, RV/LV ratio
- 6-minute walk test
- NT-proBNP/BNP
- WHO functional class
- Blood tests: FBC, LFTs (for bosentan), renal function
- Repeat RHC if clinical deterioration or escalation decision needed
- Annual PFT
9. Summary of Key Points
| Topic | Key Points |
|---|---|
| Prevalence | 7-15% of all SSc; leading cause of SSc mortality |
| Subset | Mainly lcSSc; also diffuse SSc with nucleolar ANA |
| Prognosis | Worse than iPAH; 3-year survival ~75% (PHAROS) |
| Pathology | Obliterative intimal lesions, PVOD, no plexiform lesions |
| Screening tool | DETECT algorithm (2-step), annual ECHO, PFTs, biomarkers |
| Diagnosis | RHC: mPAP ≥20 mmHg, PCWP ≤15 mmHg, PVR >2 WU (2022 ESC/ERS) |
| Vasoreactivity | Rarely positive; CCBs generally not used |
| Initial treatment | Upfront combination ERA + PDE5i (ambrisentan + tadalafil; AMBITION data) |
| Severe disease | IV epoprostenol + combination oral therapy |
| New agent | Sotatercept (activin inhibitor, 2024 FDA-approved) - add-on therapy |
| Immunosuppression | Limited role in SSc-PAH; rituximab emerging (CTD-PAH reviews) |
| Transplant | Considered in refractory cases; careful patient selection |
Key References
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set (2022), Chapter 85
- Rheumatology, 2-Volume Set (Elsevier, 2022), Chapter 150/152
- Goldman-Cecil Medicine, International Edition (2022), Chapter 69
- Murray & Nadel's Textbook of Respiratory Medicine (6th ed.), Chapter 83/84
- Braunwald's Heart Disease (15th ed.), Chapter 13
- Villa A et al. "Management of pulmonary arterial hypertension in systemic sclerosis: from classical treatments to new horizons." Eur Respir Rev 2026. [PMID: 41708122] - Systematic review identifying SSc-PAH management gaps
- Sari A et al. "Screening for Pulmonary Hypertension in Connective Tissue Diseases: Literature Review and Multidisciplinary Consensus Statement." Anatol J Cardiol 2025. [PMID: 41085415]
- Cullivan S et al. "Pulmonary Hypertension in Systemic Sclerosis." Semin Respir Crit Care Med 2024. [PMID: 38531379]
- Yokoyama Y et al. "Connective Tissue Disease-Associated PAH: Current Therapeutic Strategies and Future Prospects." Biomolecules 2026. [PMID: 41594679]
- Touil A et al. "Rituximab treatment for CTD-associated pulmonary hypertension." Expert Rev Respir Med 2026. [PMID: 40905396]
- Bearzi P et al. "Bosentan effect on echocardiographic systolic PAP in SSc-related PH." Clin Exp Rheumatol 2024. [PMID: 38819960]
- Coghlan JG et al. "Evidence-based detection of PAH in systemic sclerosis: the DETECT study." Ann Rheum Dis 2014;73:1340-1349. (Foundation screening study)
- Humbert M et al. "2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension." Eur Respir J 2023;61:2200879.
Discuss in detail about the various trials in the management of ANCA associated Vasculitis. From journals and rheumatology textbooks
"ANCA-associated vasculitis" AND "clinical trial"
ANCA associated vasculitis clinical trials 2024 2025 avacopan rituximab maintenance treatment guidelines
"ANCA vasculitis" AND "maintenance" AND "rituximab"
"ANCA vasculitis" AND "plasma exchange" AND "cyclophosphamide"
PMID: 38123922
PMID: 40720835
"PEXIVAS" AND "plasma exchange" AND vasculitis
PMID: 36155131
PMID: 38251577
"MAINRITSAN" OR "RITAZAREM" AND "ANCA vasculitis" AND rituximab maintenance
https://rheumnow.com/news/2025-bsr-recommendations-anca-asso…
"ANCA vasculitis" AND "mepolizumab" AND eosinophilic granulomatosis
Clinical Trials in the Management of ANCA-Associated Vasculitis
1. Background and Treatment Framework
- Induction of remission (intensive phase, 3-6 months)
- Maintenance of remission (2-4 years)
- Treatment of relapse
- Which immunosuppressant and route for induction (CYC vs. RTX; oral vs. IV CYC)?
- What is the role of plasma exchange?
- How much glucocorticoid is necessary?
- Which agent for maintenance and for how long?
- Can glucocorticoids be replaced (avacopan)?
- Disease-specific agents for EGPA?
2. Induction Trials
CYCLOPS Trial - IV vs. Oral Cyclophosphamide
| Parameter | Detail |
|---|---|
| Study | CYCLOPS (de Groot et al., ARD 2009) - European Vasculitis Study Group |
| Design | Multicenter RCT |
| Population | 149 newly diagnosed GPA/MPA, GFR >15 mL/min |
| Intervention | IV pulse CYC (0.35-0.5 g/m² every 2-3 weeks) vs. oral CYC 2 mg/kg/day, both × 3-6 months + GC |
| Primary endpoint | Time to remission |
| Result | Comparable remission rates; IV pulse: significantly lower cumulative CYC dose (8.2 g vs. 15.9 g); leukopenia less common (35% vs. 51%) |
| Long-term | Higher relapse rate observed with IV CYC at 18-month follow-up |
| Conclusion | IV pulse CYC is preferred for reducing cumulative dose/toxicity; oral CYC may offer marginally lower relapse rates in some settings |
- Comprehensive Clinical Nephrology 7th Ed.: "IV cyclophosphamide has similar remission rates as oral cyclophosphamide while reducing the total cyclophosphamide dose."
NORAM Trial - Methotrexate vs. Cyclophosphamide in Limited Disease
| Parameter | Detail |
|---|---|
| Study | NORAM (de Groot et al., ARD 2005) |
| Design | RCT, European Vasculitis Study Group |
| Population | Early limited GPA/MPA without severe organ involvement; creatinine <150 µmol/L |
| Intervention | MTX (15 mg/wk escalating to 25 mg/wk) vs. oral CYC 2 mg/kg/day × 12 months |
| Result | MTX remission comparable to CYC at 6 months (89.8% vs. 93.5%, NS); but slower onset, especially with pulmonary disease |
| Relapse rate | MTX: 69.5% vs. CYC: 46.5% - significantly higher |
| Conclusion | MTX acceptable for non-severe, non-renal AAV; NOT for renal disease; higher relapse rate limits use |
RAVE Trial - Rituximab vs. Cyclophosphamide (Induction) - Landmark
| Parameter | Detail |
|---|---|
| Study | RAVE (Stone et al., NEJM 2010) |
| Design | Phase III, randomized, double-blind, double-dummy, noninferiority RCT |
| Population | 197 patients with GPA (75%) or MPA (24%), newly diagnosed AND relapsing |
| Intervention | RTX 375 mg/m² IV × 4 weekly doses vs. oral CYC 2 mg/kg/day (×3 months then AZA); both with GC taper |
| Primary endpoint | Complete remission (BVAS/WG = 0 + completed prednisone taper) at 6 months |
| Overall result | RTX 64% vs. CYC 55% (p = 0.21); noninferiority met (p < 0.001) |
| Relapsing disease subgroup | RTX superior: 67% vs. 42% remission (p = 0.01) |
| PR3-ANCA subgroup | RTX trend toward superiority |
| 18-month extension | Specks et al., NEJM 2013: sustained benefit maintained; RTX still superior for relapsing disease |
| Adverse events | Similar between groups |
| Conclusion | RTX non-inferior to CYC for induction overall; superior for relapsing disease and PR3-ANCA patients; established RTX as first-line alongside CYC |
- Rheumatology 2022 Elsevier: "Subgroup analysis showed that RTX was more efficacious than cyclophosphamide in patients with relapsing disease at baseline."
RITUXVAS Trial - Rituximab vs. Cyclophosphamide in Renal AAV
| Parameter | Detail |
|---|---|
| Study | RITUXVAS (Jones et al., NEJM 2010) |
| Design | RCT, European Vasculitis Study Group |
| Population | 44 patients with new-onset ANCA-associated renal vasculitis; GFR <45 mL/min (or dialysis-dependent) |
| Intervention | RTX 375 mg/m² × 4 + 2 IV CYC pulses (days 1 and 15) vs. IV CYC × 3-6 months + AZA; both with GC |
| Primary endpoint | Sustained remission at 12 months |
| Result | RTX group 76% vs. control 82% sustained remission (p = 0.68) - no significant difference |
| Adverse events | Similar early severe AEs |
| Conclusion | RTX comparable to IV CYC for severe renal AAV; validated FDA/EMA approval for renal disease |
| Feature | RAVE | RITUXVAS |
|---|---|---|
| RTX dose | 375 mg/m² × 4 alone | 375 mg/m² × 4 + 2 CYC pulses |
| Comparator | Oral CYC then AZA | IV CYC then AZA |
| Population | New + relapsing | New onset, severe renal only |
| Primary outcome | Non-inferior | Non-inferior |
| Relapse benefit | Yes (for relapsing disease) | Not powered |
WGET Trial - Etanercept (TNF Inhibitor) in GPA
| Parameter | Detail |
|---|---|
| Study | WGET (Stone et al., NEJM 2003) |
| Design | RCT (n = 180) |
| Intervention | Etanercept added to standard therapy vs. standard therapy alone |
| Result | No benefit in remission or relapse reduction; 6 solid tumors in etanercept arm vs. 0 in placebo |
| Conclusion | TNF inhibitors are contraindicated in GPA/AAV - increased malignancy risk |
3. Plasma Exchange Trials
MEPEX Trial - Plasma Exchange vs. IV Methylprednisolone
| Parameter | Detail |
|---|---|
| Study | MEPEX (Jayne et al., JASN 2007) |
| Design | RCT, European Vasculitis Study Group |
| Population | 137 patients with severe ANCA-associated GN; serum creatinine >5.8 mg/dL (dialysis-risk) |
| Intervention | Plasma exchange (7 sessions over 14 days) vs. IV methylprednisolone 3 g; both with oral CYC + GC |
| Primary endpoint | Renal recovery (dialysis independence) at 3 months |
| Result | PE: 69% renal recovery vs. pulse MP: 49% (p = 0.02) - PE significantly superior for early renal recovery |
| 5-year follow-up | No significant difference in ESKD-free survival (45% vs. 43%); limited by sample size |
| Conclusion | PE improves early renal recovery in dialysis-dependent AAV; long-term benefit unproven - led directly to PEXIVAS |
PEXIVAS Trial - Practice-Changing Study on Plasma Exchange and GC Dosing
| Parameter | Detail |
|---|---|
| Study | PEXIVAS (Walsh et al., NEJM 2020; Jayne et al. full report PMID: 36155131) |
| Design | International (95 centres, Europe/North America/Australia/Japan), open-label, 2×2 factorial RCT |
| Population | 704 patients with GPA or MPA; GFR <50 mL/min/1.73 m² OR diffuse alveolar haemorrhage (DAH) |
| Arms | (1) PE × 7 sessions within 14 days vs. no PE; AND (2) standard-dose GC vs. reduced-dose GC (60% less cumulative oral GC by month 6) |
| Primary outcome | Composite all-cause mortality + ESKD |
| PE result | Primary endpoint: PE 28% vs. no PE 31% (HR 0.86; 95% CI 0.65-1.13; p = 0.3) - NO BENEFIT |
| Reduced GC result | Non-inferiority met (risk difference 2.3%, p = 0.5); serious infections: IRR 0.69 (0.52-0.93) - significantly fewer |
| DAH subgroup (2024) | Fussner et al., AJRCCM 2024 [PMID: 38346237]: PE not beneficial even in DAH subgroup |
| Early kidney function (2025) | Odler et al., Kidney Int 2025 [PMID: 39708998]: PE improved early kidney recovery only transiently |
| Conclusion | Plasma exchange no longer routinely recommended in AAV - even for severe renal disease or DAH. Reduced-dose GC is the new standard (same efficacy, fewer infections) |
- Firestein & Kelley's: "The reduced-dose regimen met its noninferiority endpoint for the efficacy outcome of death or end-stage renal disease, and patients in the lower-dose group had fewer infections (IRR 0.69; CI 0.52–0.93)."
- 2025 BSR: "Adjunctive plasmapheresis is not routinely recommended for pulmonary haemorrhage without severe kidney involvement."
4. Glucocorticoid Reduction Trials
PEXIVAS Reduced-Dose GC Arm (see above)
LOVAS Trial - Low-Dose GC in Non-Severe AAV
| Parameter | Detail |
|---|---|
| Study | LOVAS (Furuta et al., ARD 2021) |
| Design | RCT; Japan |
| Population | 140 patients with non-severe (non-organ-threatening) AAV |
| Intervention | Standard prednisolone (1 mg/kg/day) vs. reduced prednisolone (0.5 mg/kg/day) |
| Primary endpoint | Remission at 6 months |
| Result | Reduced dose 71.0% vs. standard 69.2% - noninferiority met |
| Adverse events | Serious AEs: 18.8% vs. 36.9% (p = 0.02); serious infections: 7.2% vs. 20.0% (p = 0.04) |
| Conclusion | Reduced GC (0.5 mg/kg, LoVAS schedule) for non-severe AAV - same efficacy, fewer AEs |
- Firestein & Kelley's: "Thus it is probable that standard glucocorticoid schedules developed over the past 50 years have used unnecessarily high doses."
5. The ADVOCATE Trial - Avacopan as Glucocorticoid Replacement
Scientific Basis
Phase II - CLEAR Trial (Jayne et al., JASN 2017)
Phase III - ADVOCATE Trial (Jayne et al., NEJM 2021) - Landmark
| Parameter | Detail |
|---|---|
| Design | Phase III, double-blind, double-dummy, active-controlled, multinational RCT |
| Population | 331 patients with newly diagnosed or relapsing GPA or MPA |
| Intervention | Avacopan 30 mg BD × 52 weeks (replacing prednisone taper) vs. Standard prednisone taper (45-60 mg/day, tapering over 26 weeks); both groups received background RTX or CYC per physician choice |
| Primary endpoint 1 | Remission at week 26 (BVAS = 0) |
| Primary endpoint 2 | Sustained remission at week 52 |
| Week 26 result | Avacopan 72.3% vs. prednisone 70.1% (noninferiority: p < 0.0001) |
| Week 52 result | Avacopan 65.7% vs. prednisone 54.9% (superiority: p = 0.007) |
| GFR improvement | Avacopan +7.3 vs. prednisone +4.1 mL/min/1.73 m² - significant renal benefit |
| GC toxicity | Glucocorticoid Toxicity Index significantly lower with avacopan (Patel et al., Lancet Rheumatol 2023 [PMID: 38251609]) |
| Quality of Life | Significant HRQoL improvements favouring avacopan (Strand et al., Lancet Rheumatol 2023 [PMID: 38251577]): SF-36 physical component, EQ-5D health utilities |
| Adverse events | Serious AEs: avacopan 42.4% vs. prednisone 45.5% (similar); liver enzyme elevations: 11% vs. 8% |
| Regulatory approval | FDA: October 2021; EMA: January 2022 |
-
Elderly patients (≥65 years): Avacopan effective and well-tolerated (Geetha et al. Rheumatology 2025 [PMID: 40037556])
-
CYC background: Avacopan effective with both RTX and CYC (Geetha et al. RMD Open 2025 [PMID: 41052893])
-
Low GFR (<20 mL/min): Greater renal recovery benefit in most severely impaired patients
-
Respiratory disease: Effective in patients with respiratory tract AAV manifestations (Specks et al., ACR Open Rheumatol 2025)
-
2025 BSR Guidelines: Avacopan is now a recommended replacement for the prednisone taper as part of induction therapy for GPA/MPA (GRADE 1A).
-
2022 EULAR: Avacopan recommended as part of induction regimen for GPA/MPA.
6. Maintenance Trials
CYCAZAREM - Azathioprine vs. Cyclophosphamide for Maintenance
| Parameter | Detail |
|---|---|
| Study | CYCAZAREM (Jayne et al., NEJM 2003) |
| Design | RCT, European Vasculitis Study Group (n = 144) |
| Population | GPA/MPA in remission after CYC + GC induction |
| Intervention | Continue oral CYC 1.5 mg/kg/day vs. switch to AZA 2 mg/kg/day at 3 months of remission |
| Result | Relapse at 18 months: CYC 15.5% vs. AZA 13.7% (p = NS); adverse events similar |
| Conclusion | AZA equivalent to CYC for maintenance - CYC not required beyond remission induction; AZA established as standard maintenance |
WEGENT - Azathioprine vs. Methotrexate for Maintenance
| Parameter | Detail |
|---|---|
| Study | WEGENT (French Vasculitis Study Group) |
| Design | RCT |
| Intervention | AZA 2 mg/kg/day vs. MTX 0.3 mg/kg/wk (max 25 mg) for maintenance |
| Result | No significant difference in relapse rate or toxicity between AZA and MTX |
| Conclusion | MTX as effective as AZA for maintenance; avoid in GFR <30 mL/min |
IMPROVE - Mycophenolate Mofetil vs. Azathioprine
| Parameter | Detail |
|---|---|
| Study | IMPROVE (Hiemstra et al., ARD 2010) |
| Design | RCT, European Vasculitis Study Group |
| Intervention | MMF 2 g/day vs. AZA 2 mg/kg/day |
| Result | MMF significantly inferior: higher relapse rate (HR 1.69; 95% CI 1.06-2.70) |
| Cancers | AZA arm: 2 bladder + 3 skin cancers; MMF arm: 1 skin cancer |
| Conclusion | MMF inferior to AZA for maintenance - not recommended as first-line; 2025 BSR recommends MMF only if RTX/AZA/MTX contraindicated/not tolerated |
MAINRITSAN 1 - Rituximab vs. Azathioprine Maintenance - Landmark
| Parameter | Detail |
|---|---|
| Study | MAINRITSAN (Guillevin et al., NEJM 2014) |
| Design | RCT, French Vasculitis Study Group |
| Population | 115 patients with GPA, MPA, or renal-limited vasculitis in complete remission after CYC induction |
| Intervention | RTX 500 mg IV at day 0, day 14, then every 6 months × 18 months vs. AZA 2 mg/kg/day (tapered over 22 months) |
| Primary endpoint | Major relapse rate at 28 months |
| Result | Major relapses: RTX 5% vs. AZA 29% (p < 0.001) |
| 60-month follow-up | Severe relapses off treatment: RTX 28.1% vs. AZA 50.6% (HR 2.51 for AZA, p = 0.003) - benefit persists but accelerates after stopping |
| Adverse events | Similar severe infections, malignancy |
| Conclusion | RTX greatly superior to AZA for maintenance; established RTX as preferred maintenance agent for AAV |
MAINRITSAN 2 - Fixed vs. Tailored Rituximab Dosing
| Parameter | Detail |
|---|---|
| Study | MAINRITSAN 2 (Terrier et al., Ann Intern Med 2021) |
| Design | RCT (n = 162) |
| Population | GPA/MPA in complete remission after CYC induction |
| Intervention | Fixed schedule: RTX 500 mg every 6 months vs. Tailored: RTX 500 mg upon CD19+ B-cell reappearance OR ANCA titer doubling |
| Result | Major relapse at 28 months: fixed 9.9% vs. tailored 17.3% (p = 0.22) - not significantly different |
| Infusions | Fixed: median 5; tailored: median 3 - fewer infusions with tailored |
| Conclusion | Tailored dosing non-inferior; reduces drug burden and infusion frequency |
MAINRITSAN 3 - Extended RTX vs. Placebo (Post-Maintenance Extension)
| Parameter | Detail |
|---|---|
| Study | MAINRITSAN 3 (Terrier et al., ARD 2021) |
| Design | RCT placebo-controlled extension |
| Population | Patients completing MAINRITSAN 2 |
| Intervention | Continue RTX 500 mg biannually vs. placebo |
| Result | Major relapse-free survival: RTX 100% vs. placebo 87% (p = 0.009) |
| Adverse events | Similar |
| Conclusion | Extended maintenance beyond 2 years reduces relapse; supports longer-term RTX therapy |
RITAZAREM - Rituximab vs. Azathioprine in Relapsing AAV
| Parameter | Detail |
|---|---|
| Study | RITAZAREM (Smith et al., ARD 2019) |
| Design | RCT (n = 170) |
| Population | Relapsing ANCA vasculitis in remission after RTX induction (1 g × 2 doses) - key difference from MAINRITSAN 1 |
| Intervention | RTX 1000 mg IV every 4 months × 5 doses (more frequent/higher dose than MAINRITSAN) vs. AZA 2 mg/kg/day |
| Primary endpoint | Relapse rate at 24 months |
| Result | During treatment: relapses 13/85 (RTX) vs. 32/85 (AZA); HR 0.35 (0.18-0.66) |
| Severe relapses | 6 (RTX) vs. 17 (AZA) |
| Serious AEs | RTX 22% vs. AZA 36% during treatment period |
| 36-month (off treatment) | Benefit sustained: HR 0.41 (0.27-0.61) |
| Conclusion | RTX markedly superior to AZA for relapsing AAV; higher RTX dose (1000 mg/4 months) supports use in higher-risk patients |
- Firestein & Kelley's: "Fewer relapses were seen in the rituximab group (HR, 0.35; 96% CI, 0.18–0.66). Including a follow-up period off treatment (to 36 months since enrollment), fewer relapses were still seen in the rituximab group (HR, 0.41; 95% CI, 0.27–0.61)."
B-Cell-Guided vs. ANCA-Guided RTX Maintenance (Zonozi et al. 2024)
| Parameter | Detail |
|---|---|
| Study | Zonozi R et al., Ann Rheum Dis 2024 [PMID: 38123922] |
| Design | Prospective, single-centre, open-label RCT (n = 115) |
| Population | ANCA vasculitis in remission after ≥2 years of fixed-schedule RTX |
| Intervention | B-cell arm: RTX upon CD19+ B-cell repopulation vs. ANCA arm: RTX upon significant ANCA rise |
| Primary endpoint | Clinical relapse (modified BVAS/WG >0) by 36 months |
| Result | Relapse at 3 years: B-cell arm 4.1% vs. ANCA arm 20.5% (p = 0.045) |
| Safety | Total SAEs and deaths equivalent; COVID-19 SAEs higher in B-cell arm |
| RTX exposure | B-cell arm: 3.6 infusions vs. ANCA arm: 0.5 infusions per patient |
| Conclusion | B-cell-guided dosing is superior to ANCA-guided for preventing relapse; preferred long-term maintenance strategy |
Duration Comparison - Karras et al. (AZA 24 vs. 48 Months)
7. TMP-SMX as Adjunct Maintenance
Stegeman et al. RCT (NEJM 1996)
| Parameter | Detail |
|---|---|
| Population | GPA patients in remission |
| Intervention | TMP-SMX 960 mg BD vs. placebo |
| Result | TMP-SMX reduced relapses (23% vs. 40%; p = 0.02) and infections - especially upper respiratory |
| Mechanism | Eliminates nasal Staphylococcus aureus colonization - major relapse trigger in GPA |
| Conclusion | TMP-SMX recommended as adjunct in GPA with nasal/sinus involvement; not a substitute for standard immunosuppression; also provides Pneumocystis jirovecii prophylaxis |
8. Trials in EGPA
Five Factor Score (FFS) - Risk Stratification Framework
- Serum creatinine >1.58 mg/dL
- Proteinuria >1 g/day
- Severe GI involvement
- Cardiomyopathy
- CNS involvement
MIRRA Trial - Mepolizumab in EGPA - Landmark
| Parameter | Detail |
|---|---|
| Study | MIRRA (Wechsler et al., NEJM 2017) |
| Design | Phase III, double-blind, placebo-controlled RCT (n = 136) |
| Population | Relapsing or refractory EGPA on oral GC ≥7.5 mg/day |
| Intervention | Mepolizumab 300 mg SC every 4 weeks × 52 weeks vs. placebo; both with standard of care |
| Primary endpoints | (1) Accrued weeks of remission (BVAS = 0, prednisolone ≤4 mg/day); (2) Proportion in remission at weeks 36 and 48 combined |
| Remission rate | Mepolizumab: 28% vs. placebo: 3% in remission at weeks 36 and 48 (OR 5.91; p < 0.001) |
| Accrued remission | Significantly superior (26% vs. 8% of study weeks in full remission) |
| Steroid sparing | Daily prednisolone at 48 weeks: 4.0 mg (mepolizumab) vs. 10.0 mg (placebo) |
| Relapse | Lower relapse rate; eosinophil counts normalized |
| Adverse events | Similar; nasopharyngitis most common |
| Mechanism | Anti-IL-5 monoclonal antibody - reduces eosinophil survival and differentiation |
| Approval | FDA: December 2017; EMA: September 2018 - first targeted biologic for EGPA |
| Conclusion | Mepolizumab is the standard biologic therapy for relapsing/refractory EGPA; significant steroid-sparing |
Rituximab for EGPA - Phase III Trial (Terrier et al. 2025)
| Parameter | Detail |
|---|---|
| Study | Terrier B et al., Ann Intern Med 2025 [PMID: 40720835] |
| Design | Phase III, multicenter, double-blind, randomized, superiority RCT; France (n = 105) |
| Population | Newly diagnosed or relapsing EGPA (BVAS ≥3) |
| Intervention | RTX 1 g × 2 doses (2 weeks apart) + GC vs. conventional strategy (GC alone or GC + CYC for severe forms) |
| Primary endpoint | Remission (BVAS = 0 + prednisolone ≤7.5 mg/day) at day 180 |
| Result | RTX 63.5% vs. control 60.4% (RR 1.05; 95% CI 0.78-1.42; p = 0.75) - not superior |
| Duration of remission | RTX 48.5 weeks vs. control 49.1 weeks (p = 0.41) |
| Adverse events | No significant differences |
| Conclusion | RTX not superior to conventional therapy for EGPA; unlike GPA/MPA, RTX is not first-line; ANCA-positive EGPA patients may benefit more (post-hoc observation) |
Azathioprine vs. CYC for EGPA Maintenance
9. Emerging Trials (2022-2026)
ALEVIATE - Alemtuzumab in Refractory AAV
| Parameter | Detail |
|---|---|
| Study | ALEVIATE (Gopaluni et al., Arthritis Res Ther 2022 [PMID: 35365179]) |
| Design | Randomized, dose-ranging, phase II/III trial |
| Population | Refractory primary systemic vasculitis including AAV |
| Intervention | Alemtuzumab (anti-CD52 monoclonal antibody) at different doses |
| Result | Dose-dependent efficacy in refractory disease; significant infectious complications and secondary autoimmune events |
| Conclusion | Alemtuzumab may rescue refractory disease; significant toxicity profile; not standard care |
IFX-1 - Anti-C5a Monoclonal Antibody
Novel Anti-CD20 Agents
Long-Term Avacopan Duration Trial (NCT06072482, Ongoing)
10. Summary Table of Major Trials
| Trial | Year | Design | Question | Key Result | Conclusion |
|---|---|---|---|---|---|
| CYCLOPS | 2009 | RCT | IV vs. oral CYC induction | Equal remission; IV = lower CYC dose | IV pulse CYC preferred |
| NORAM | 2005 | RCT | MTX vs. CYC (limited GPA) | MTX comparable at 6m; higher relapse rate | MTX only for limited non-renal disease |
| RAVE | 2010 | Phase III RCT | RTX vs. oral CYC induction | Non-inferior; RTX superior in relapsing | RTX = CYC; RTX preferred for relapsing/PR3 |
| RITUXVAS | 2010 | RCT | RTX+2CYC vs. CYC (renal AAV) | No difference at 12m | RTX comparable to CYC in severe renal |
| WGET | 2003 | RCT | Etanercept in GPA | No benefit; increased solid tumors | TNF inhibitors contraindicated in AAV |
| MEPEX | 2007 | RCT | PE vs. IV MP (severe renal) | PE better early renal recovery | PE for dialysis-dependent; long-term unclear |
| PEXIVAS | 2020 | Factorial RCT (n=704) | PE vs. no PE; reduced vs. standard GC | PE: no benefit; reduced GC: non-inferior + fewer infections | PE not recommended; use reduced GC |
| LOVAS | 2021 | RCT | Reduced vs. standard GC (non-severe) | Non-inferior; fewer AEs with reduced dose | Reduced GC (0.5 mg/kg) for non-severe AAV |
| Stegeman | 1996 | RCT | TMP-SMX adjunct in GPA remission | Fewer relapses; fewer infections | TMP-SMX adjunct for upper tract GPA |
| CYCAZAREM | 2003 | RCT | AZA vs. CYC maintenance | Equivalent relapse/toxicity | AZA replaces CYC after remission |
| WEGENT | 2008 | RCT | AZA vs. MTX maintenance | Equivalent | AZA or MTX for maintenance |
| IMPROVE | 2010 | RCT | MMF vs. AZA maintenance | MMF inferior (higher relapse) | AZA preferred over MMF |
| MAINRITSAN 1 | 2014 | RCT | RTX vs. AZA maintenance | RTX: 5% vs. AZA: 29% major relapse | RTX is preferred maintenance agent |
| MAINRITSAN 2 | 2021 | RCT | Fixed vs. tailored RTX | No significant difference; tailored = fewer infusions | Tailored dosing acceptable |
| MAINRITSAN 3 | 2021 | RCT | Extended RTX vs. placebo | RTX: 100% vs. placebo: 87% relapse-free survival | Extended maintenance beneficial |
| RITAZAREM | 2019 | RCT | RTX vs. AZA (relapsing AAV) | HR 0.35 favoring RTX | RTX markedly superior in relapsing disease |
| B-cell vs ANCA-guided (Zonozi 2024) | 2024 | RCT | B-cell vs. ANCA-triggered RTX | B-cell: 4.1% vs. ANCA: 20.5% relapse | B-cell guided dosing preferred |
| ADVOCATE | 2021 | Phase III RCT | Avacopan vs. prednisone taper | Superior at W52; better QoL/renal function | Avacopan replaces prednisone taper |
| MIRRA | 2017 | Phase III RCT | Mepolizumab vs. placebo (EGPA) | 28% vs. 3% remission; major steroid-sparing | Mepolizumab first-line for relapsing EGPA |
| RTX for EGPA (Terrier 2025) | 2025 | Phase III RCT | RTX vs. conventional (EGPA) | Not superior | RTX not first-line in EGPA |
| ALEVIATE | 2022 | Phase II/III RCT | Alemtuzumab in refractory AAV | Efficacy but significant toxicity | Reserved for refractory disease |
11. Current Guideline Recommendations (2025 BSR / 2022 KDIGO / 2022 EULAR)
Induction of Remission (GPA/MPA)
- IV pulsed CYC or RTX + GC for all active GPA/MPA (GRADE 1A)
- RTX preferred for relapsing disease (GRADE 1B)
- CYC + RTX combination may be considered for life/organ-threatening disease
- GC: PEXIVAS reduced-dose regimen (target 5 mg/day by month 4-5); IV methylprednisolone pulses NOT routinely recommended
- Avacopan (30 mg BD × 52 weeks) replaces prednisone taper as part of induction (GRADE 1A, BSR 2025)
Maintenance of Remission (GPA/MPA)
- RTX 500-1000 mg every 4-6 months preferred (GRADE 1)
- B-cell-guided dosing preferred over ANCA-guided dosing
- Alternatives: AZA 2 mg/kg/day or MTX 0.25-0.3 mg/kg/wk
- MMF only if RTX/AZA/MTX not tolerated
- Duration: 24-48 months (risk-stratified)
EGPA
- GC alone for FFS = 0; CYC + GC for FFS ≥1
- Mepolizumab (300 mg SC every 4 weeks) for relapsing/refractory EGPA
- RTX not first-line in EGPA (negative phase III RCT, 2025)
Key References
- Firestein & Kelley's Textbook of Rheumatology (2022), Chapters 86-87
- Comprehensive Clinical Nephrology 7th Ed., Chapter 26
- Brenner & Rector's The Kidney (2-Vol), Chapters 18-19
- NKF Primer on Kidney Diseases 8th Ed., Chapter 2
- Goldman-Cecil Medicine (2022), Chapter 69
- Harrison's Principles of Internal Medicine 22nd Ed. (2025), Chapter 375
- Stone JH et al. (RAVE). NEJM 2010;363:221-232
- Jones RB et al. (RITUXVAS). NEJM 2010;363:211-220
- Walsh M et al. (PEXIVAS). NEJM 2020;382:622-631 [Full report: PMID 36155131]
- Jayne DRW et al. (ADVOCATE). NEJM 2021;384:599-609
- Guillevin L et al. (MAINRITSAN). NEJM 2014;371:1771-1780
- Terrier B et al. (MAINRITSAN 2). Ann Intern Med 2021
- Terrier B et al. (MAINRITSAN 3). ARD 2021
- Smith RM et al. (RITAZAREM). ARD 2019
- Wechsler ME et al. (MIRRA). NEJM 2017;377:1521-1531
- Zonozi R et al. Ann Rheum Dis 2024 [PMID: 38123922]
- Terrier B et al. (RTX in EGPA). Ann Intern Med 2025 [PMID: 40720835]
- Fussner LA et al. (PEXIVAS-DAH). AJRCCM 2024 [PMID: 38346237]
- Patel NJ et al. (ADVOCATE-GTI). Lancet Rheumatol 2023 [PMID: 38251609]
- Strand V et al. (ADVOCATE-QoL). Lancet Rheumatol 2023 [PMID: 38251577]
- Geetha D et al. (ADVOCATE elderly). Rheumatology 2025 [PMID: 40037556]
Generate a PowerPoint presentation summarizing all major AAV trials and current treatment algorithms
ls -la /home/daytona/workspace/ 2>/dev/null | head -20
mkdir -p /home/daytona/workspace/aav-trials-pptx && ls /home/daytona/workspace/aav-trials-pptx/
Continue
Generate a PowerPoint presentation summarizing all major AAV trials and current treatment algorithms
Write a detailed notes on Kikuchis disease from rheumatology textbooks and journals
"Kikuchi disease" OR "Kikuchi-Fujimoto" AND lymphadenitis
Kikuchi-Fujimoto disease 2024 2025 diagnosis treatment review rheumatology
PMID: 36056828
PMID: 37383134
PMID: 40610704
"Kikuchi-Fujimoto disease" AND pathogenesis AND etiology
PMID: 39915303
"Kikuchi" AND "histopathology" AND "diagnosis" AND lymphadenitis
PMID: 33169134
https://pmc.ncbi.nlm.nih.gov/articles/PMC10294163
Kikuchi-Fujimoto Disease (Histiocytic Necrotizing Lymphadenitis): Detailed Notes
1. Introduction and Historical Background
- Masahiro Kikuchi - described it as "lymphadenitis showing focal reticulum cell hyperplasia with nuclear debris and phagocytosis"
- Y. Fujimoto - reported similar cases as "cervical subacute necrotizing lymphadenitis"
- Quick Compendium of Clinical Pathology: "The first of these entities is Kikuchi-Fujimoto disease (histiocytic necrotizing lymphadenitis), a lesion typically found in cervical lymph nodes of young females, consisting of partial nodal involvement by fields of karyorrhectic cell death, neutrophil-poor, in association with histiocytes (anomalously myeloperoxidase+), plasmacytoid dendritic cells (CD123+), and T cells (CD8+)."
- Goldman-Cecil Medicine: "Kikuchi disease (histiocytic necrotizing lymphadenitis) is a disease of unknown origin that most commonly affects young women."
2. Epidemiology
| Feature | Detail |
|---|---|
| Prevalence | Rare; exact prevalence unknown |
| Geographic distribution | Originally described in Japan and East Asia; now recognized worldwide; higher reported frequency in Asian populations |
| Sex predilection | Predominantly females (F:M ratio approximately 3:1 to 4:1) |
| Age | Most commonly young adults (teens to 30s); mean age ~25-30 years; pediatric cases well-documented |
| Racial predilection | More common in Asians, but occurs in all ethnic groups |
| Recurrence rate | ~3-4% of patients experience relapse (sometimes years later) |
3. Etiology and Pathogenesis
3a. Infectious Trigger Hypothesis
- Viruses: Epstein-Barr virus (EBV), Human Herpesvirus-6 (HHV-6), HHV-7, HHV-8, cytomegalovirus (CMV), parvovirus B19, HTLV-1, HIV, enteroviruses, SARS-CoV-2
- Bacteria: Yersinia, Brucella, Bartonella henselae (cat-scratch disease), Toxoplasma gondii
- Evidence: HHV-6 genomes have been found within affected lymph nodes; viral particles have been identified ultrastructurally in lymphocytes and histiocytes
- Recent data: SARS-CoV-2 infection is now recognized as a trigger for KFD - systematic review (Cahuapaza-Gutierrez et al. Clin Rheumatol 2025, PMID: 40610704) documented 16 new-onset KFD cases post-COVID-19 infection (mean age 27 years), and 36 cases following COVID-19 vaccination (predominantly mRNA vaccines - Pfizer-BioNTech 75%, Moderna 11%; mostly after first dose)
3b. Autoimmune Mechanism Hypothesis
- HLA class II gene associations: Specific HLA-DPA1 and HLA-DPB1 alleles are overrepresented in KFD, suggesting genetic immune susceptibility
- KFD shares striking clinical and histological overlap with SLE (see below)
- Association with other autoimmune diseases (Hashimoto's thyroiditis, primary Sjogren's syndrome, APS)
- Spontaneous resolution without treatment, pattern of recurrence, and concurrent autoimmune features all support immune dysregulation
- Scott-Brown's Otorhinolaryngology: "An autoimmune aetiology has been proposed as some human leucocyte antigen (HLA) class II genes are more frequent in patients with KD. An association with systemic lupus erythematosus has also been reported."
3c. Cytotoxic T-Cell / Perforin-Mediated Apoptosis
- The abundant apoptosis in KFD lymph nodes is driven by CD8+ cytotoxic T lymphocytes and plasmacytoid dendritic cells (pDCs)
- Perforin-2 (MPEG1) is dramatically overexpressed in KFD (92% of cases in a 2025 study) - Lyapichev et al. Virchows Arch 2025 [PMID: 39915303]
- Perforin-2 mediates pore formation and is essential for type I interferon-induced JAK/STAT signaling and elimination of viral infection
- Hypothesis: an exaggerated cytotoxic immune response following viral infection drives the massive lymphocyte apoptosis characteristic of KFD
- Type I interferon signaling is likely central (explaining the overlap with interferonopathies and SLE)
4. Clinical Features
4a. Cardinal Manifestations
| Feature | Frequency | Details |
|---|---|---|
| Lymphadenopathy | ~100% | Firm to rubbery; predominantly cervical (posterior > anterior); may be tender; usually <3 cm |
| Fever | 30-50% | Persistent or intermittent; low-grade to high fever (up to 39-40°C) |
| Tenderness of nodes | Common | May be painful on palpation |
| Weight loss | Severe cases | Constitutional symptom |
| Night sweats | Variable | Common in severe disease |
| Fatigue/malaise | Common | May precede lymphadenopathy |
4b. Lymphadenopathy Distribution
- Cervical: Most common (posterior cervical > anterior cervical) - 70-98% of cases
- Generalized lymphadenopathy: Less common; suggests overlap with SLE or more severe disease
- Other sites: Axillary, inguinal, mediastinal, mesenteric (reported)
- Node size: Usually 1-3 cm; occasionally larger
- Consistency: Firm to rubbery (not hard/fixed as in malignancy; not soft/fluctuant as in abscess)
- Overlying skin: Usually uninvolved; rarely erythematous
4c. Cutaneous Manifestations
- Facial erythema (malar distribution - raises concern for SLE overlap)
- Erythematous macules, papules, plaques - non-specific
- Morbilliform/acneiform eruptions
- Erythematous papulosquamous lesions
- Urticarial lesions
- Skin histology: Interface dermatitis pattern - histologically similar to cutaneous lupus
- Cutaneous KFD (with skin biopsy showing similar necrotizing histiocytic infiltrate) is a distinct entity listed in Fitzpatrick's Dermatology
4d. Systemic and Extranodal Manifestations
| System | Manifestation |
|---|---|
| Hepatic | Hepatomegaly; mildly elevated liver enzymes |
| Splenic | Splenomegaly (especially in severe/generalized disease) |
| Articular | Arthralgia, arthritis (reported) |
| Neurological | Aseptic meningitis; encephalitis (rare) - potentially fatal manifestations |
| Renal | Membranous nephropathy; mesangial nephritis (rare but documented; Falbo 2023) |
| Cardiac | Myocarditis; cardiomegaly (rare; case reports of KFD with cardiac involvement) |
| Ocular | Anaemic retinopathy (rare) |
| Haematological | Haemophagocytic lymphohistiocytosis (HLH) - association documented; overlap syndrome |
4e. Special Populations
- Less common than in adults; mean age ~10-14 years
- Higher rates of fever (>90%), hepatosplenomegaly more common
- Leukopenia more pronounced
- May present as macrophage activation syndrome (MAS) in children
- Overlapping diagnosis with HSS/KFD has been reported
- Similar clinical course but perhaps higher rate of systemic manifestations
5. Laboratory Findings
| Investigation | Findings |
|---|---|
| Full blood count | Leukopenia (particularly lymphopenia) in ~50%; atypical lymphocytes may be present; thrombocytopenia uncommon |
| ESR | Elevated in most patients |
| CRP | Usually elevated |
| LDH | Elevated - marker of tissue necrosis and disease severity |
| Liver enzymes (ALT, AST) | Mildly elevated in ~30% |
| Serum ferritin | May be elevated (especially when associated with HLH) |
| ANA | Negative in pure KFD; positive ANA should prompt evaluation for SLE |
| Anti-dsDNA | Negative in pure KFD; if positive, suggests SLE |
| Complement (C3, C4) | Normal in KFD; low in SLE |
| Blood cultures | Negative (excludes bacterial lymphadenitis) |
| Bone marrow biopsy | Rarely needed; may show haemophagocytosis in HLH-KFD overlap |
6. Histopathology - The Diagnostic Cornerstone
6a. Gross Pathology
- Lymph node enlarged, pale, may show areas of necrosis on cut section
- Capsule usually intact (unlike malignancy)
- Partial nodal involvement - key feature
6b. Histological Phases (Proliferative → Necrotizing → Xanthomatous)
- Paracortical expansion by a heterogeneous mixture of T cells, histiocytes, and plasmacytoid dendritic cells
- Mitotically active, immunoblast-like cells
- Crescentic and twisted nuclei
- Patchy, well-circumscribed areas of coagulative/karyorrhectic necrosis in the paracortex
- Abundant nuclear debris (karyorrhexis) - fragmented apoptotic nuclei
- ABSENCE of neutrophils - a cardinal distinguishing feature
- Histiocytes engulfing karyorrhectic debris
- CD8+ T cells and plasmacytoid dendritic cells predominate
- Myeloperoxidase (MPO)-positive histiocytes (anomalous feature, as MPO is normally a granulocyte marker)
- Plasmacytoid dendritic cells (CD123+, CD68+, CD43+) in large numbers
- Foamy xanthomatous histiocytes predominate
- Decreasing necrosis
- Less cellular activity
6c. Immunohistochemistry Profile
| Marker | Expression |
|---|---|
| CD68 | + (histiocytes) |
| CD123 | + (plasmacytoid dendritic cells - prominent) |
| MPO | + (histiocytes - aberrant) |
| CD8 | + (predominant T cells) |
| CD4 | Variable/reduced |
| CD20 | Few scattered B cells |
| Ki-67 | High proliferation index |
| CD3 | + (T cells) |
| C4d endothelial staining | Negative in KFD (vs. positive in lupus lymphadenitis - key distinction) |
- Quick Compendium of Clinical Pathology: "...partial nodal involvement by fields of karyorrhectic cell death, neutrophil-poor, in association with histiocytes (anomalously myeloperoxidase+), plasmacytoid dendritic cells (CD123+), and T cells (CD8+)."
6d. Key Histological Distinction: KFD vs. Lupus Lymphadenitis
| Feature | KFD | Lupus Lymphadenitis |
|---|---|---|
| Mean age | ~25 years | ~33 years |
| Biopsy site | Cervical (most) | May be non-cervical more often |
| Generalized lymphadenopathy | Less common | More common (56% vs. 23%) |
| Necrosis area | Smaller, focal | Larger, more extensive |
| Histiocytic infiltrates in necrosis | Prominent | Less prominent |
| Interfollicular pattern | Uncommon (4%) | More common (26%) |
| Plasma cell infiltrates | Rare | More frequent |
| Xanthomatous infiltrates | Rare | Present in 32% |
| C4d endothelial staining | Negative | Positive (65% in necrotic area) |
| Hematoxylin bodies | Absent | Present (specific for SLE) |
- Yu et al., Rheumatology (Oxford) 2021 [PMID: 33169134]: C4d immunohistochemical staining in the necrotic area distinguishes lupus lymphadenitis from KFD with high sensitivity; machine learning integration further improves accuracy.
6e. Fine Needle Aspiration Cytology (FNAC)
- Usually shows non-specific reactive lymphadenitis - not reliable for definitive diagnosis
- May reveal crescentic histiocytes engulfing karyorrhectic debris (suggestive)
- FNAC alone is insufficient; open/core biopsy is often required
- Mahajan et al. 2023: "Fine needle aspiration cytology mostly has features of nonspecific reactive lymphadenitis and immunohistochemistry studies usually show variable features of uncertain diagnostic value. Since its diagnosis is exclusively from histopathology, it needs to be evaluated more carefully."
7. Diagnosis
7a. Diagnostic Approach
- Clinical suspicion: Young female with cervical lymphadenopathy + fever + leukopenia
- Exclude infection: Blood cultures, viral serology (EBV, CMV, toxoplasma, HIV)
- Basic labs: FBC, ESR, CRP, LFTs, LDH, ANA, anti-dsDNA
- Imaging: Ultrasound neck (assess node characteristics); CT neck/chest/abdomen if generalized
- Lymph node biopsy (excisional/core): For histopathology + immunohistochemistry
- Evaluate for SLE (mandatory): ANA, anti-dsDNA, complement, urinalysis, renal function
- Long-term follow-up for SLE development
7b. Clinical Diagnostic Criteria (No Validated Criteria)
- Karyorrhectic/coagulative paracortical necrosis
- Absence of neutrophils
- Histiocytic infiltration with karyorrhexis
- CD8+ T cell and CD123+ plasmacytoid dendritic cell predominance
7c. Imaging
- Ultrasound: Enlarged hypoechoic lymph nodes with increased vascularity; may help characterize node architecture; useful as screening
- CT neck/chest/abdomen: Useful in generalized disease to assess extent; shows enlarged nodes without obvious necrotic breakdown; mediastinal adenopathy may be present
- MRI: Not routinely used
- PET scan: Shows FDG avidity in involved nodes (may mimic lymphoma on imaging - hence biopsy is essential)
8. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Non-Hodgkin lymphoma | Most important to exclude; persistent/progressive nodes; biopsy shows clonal lymphocyte proliferation; lymphoma markers positive |
| Hodgkin lymphoma | Reed-Sternberg cells on biopsy; CD30+, CD15+ |
| SLE lymphadenitis | ANA/anti-dsDNA positive; complement low; hematoxylin bodies on biopsy; C4d+ |
| Cat-scratch disease | History of cat exposure; Bartonella serology positive; stellate microabscesses with neutrophils |
| Infectious mononucleosis (EBV) | Heterophile antibody (Monospot) positive; EBV IgM positive; atypical lymphocytosis |
| Tubercular lymphadenitis | Caseating granulomas; AFB stain/culture; IGRA/TST positive |
| Toxoplasmosis | Toxoplasma serology positive; no necrosis (monocytoid B-cell hyperplasia pattern) |
| Still's disease (AOSD) | Quotidian fever, arthritis, salmon-colored rash, markedly elevated ferritin; lacks necrotizing lymphadenitis histology |
| Sarcoidosis | Non-caseating granulomas; serum ACE elevated; bilateral hilar adenopathy |
| Sweet's syndrome | Painful erythematous plaques; neutrophilic dermatosis histology |
| Drug-induced lymphadenopathy | Drug history; eosinophilia; drug lymphadenitis on biopsy |
| IgG4-related disease | IgG4+ plasma cell infiltration; storiform fibrosis; raised serum IgG4 |
- Mahajan et al. 2023: "It is often mistaken for non-Hodgkin lymphoma while lupus lymphadenitis, cat-scratch disease, Sweet's syndrome, Still's disease, drug eruptions, infectious mononucleosis, and viral or tubercular lymphadenitis are other common differentials."
9. KFD and the SLE-KFD Relationship
Nature of the Relationship
- KFD preceding SLE (SLE develops later - sometimes months to years)
- KFD concurrent with SLE (simultaneous diagnosis)
- KFD in established SLE (SLE patient develops KFD as a feature)
- Systematic review (Zaccarelli et al. Curr Rheumatol Rev 2023, PMID: 36056828): 43 studies included; overlap found with multiple autoimmune diseases. Autoimmune disease was "preceding" in 11 cases, "simultaneous" in 20 cases, and "post-KFD" in 8 cases.
Shared Clinicopathological Features
| Feature | KFD | SLE |
|---|---|---|
| Female predominance | Yes | Yes |
| Young adults | Yes | Yes |
| Cervical lymphadenopathy | Dominant feature | Common feature |
| Fever | Yes | Yes |
| Malar rash | Sometimes | Classic |
| Interface dermatitis (skin biopsy) | Yes | Yes |
| Paracortical necrosis without neutrophils | Yes | Yes |
| Absence of significant immune complex deposition | Yes | Variable |
| Response to steroids | Yes | Yes |
Why the Relationship Matters Clinically
- KFD can be the presenting manifestation of SLE - patients who appear to have isolated KFD may evolve to full SLE
- Lupus lymphadenitis and KFD are histologically very similar - C4d immunostaining helps distinguish
- ALL patients with KFD should be:
- Tested for ANA, anti-dsDNA, complement, urinalysis
- Monitored long-term for development of SLE
- Rheumatology 2022 Elsevier: "patients who present with Kikuchi syndrome should be investigated further for SLE and be monitored long term"
- The autoimmune overlap includes: JIA (reported), Sjögren's syndrome, antiphospholipid syndrome, Hashimoto's thyroiditis, systemic sclerosis
HLH-KFD Association
10. COVID-19 and KFD (Recent Update)
- Mean age: 27.25 ± 16.87 years
- Manifestations: fever, fatigue, cough, weight loss
- All cases resolved with supportive care; no mortality
- Mean age: 30.8 ± 12.63 years
- Predominantly female
- mRNA vaccines: Pfizer-BioNTech (75%), Moderna (11.1%)
- Mostly after first dose (75%)
- Cervical lymphadenopathy predominant in both groups
- Favorable outcomes in all cases
11. Natural History and Prognosis
- KFD is typically self-limiting, resolving within 1-4 months (range: 2 weeks to 6 months)
- Most patients recover completely without specific treatment
- Recurrence: Occurs in ~3-4% of patients; may recur months to years later; recurrent episodes are generally milder
- Mortality: Extremely rare; reported only in cases with severe neurological involvement (aseptic meningoencephalitis), massive HLH, or cardiac involvement
- Goldman-Cecil Medicine: "Treatment is symptomatic, and manifestations usually resolve within weeks or months."
- Firestein & Kelley's: "Kikuchi-Fujimoto disease, characterized by cervical lymphadenopathy, fever, and weight loss, may mimic SLE."
- Generalized lymphadenopathy
- High fever
- Marked leukopenia
- Elevated LDH
- Association with SLE or HLH
- Neurological manifestations
12. Treatment
12a. General Measures
- NSAIDs: First-line for symptomatic relief - reduce fever, pain, and lymph node tenderness
- Analgesics/antipyretics as needed
- Rest and reassurance
12b. Corticosteroids
- Indicated for severe disease: High fever unresponsive to NSAIDs, severe systemic symptoms, neurological involvement, HLH-associated KFD, or SLE-overlap cases
- Dose: Prednisolone 0.5-1 mg/kg/day, typically for 2-4 weeks then tapered
- Response is generally good
- Mahajan et al. 2023: "Treatment with systemic corticosteroids, hydroxychloroquine, or antimicrobial agents mostly remains empirical."
12c. Hydroxychloroquine (HCQ)
- Used especially in cases with SLE overlap or when steroids are not well-tolerated
- May help prevent relapse
- Dose: 200-400 mg/day
- Particularly useful given shared pathogenesis with SLE/interferonopathy
12d. IV Immunoglobulin (IVIG)
- Reported in severe or steroid-refractory KFD
- May be considered in HLH-associated KFD
12e. What Does NOT Work
- Antibiotics: KFD does not respond to antibiotics - important to avoid unnecessary antibiotic courses
- Scott-Brown's Otorhinolaryngology: "The disease is usually self-limiting and does not respond to antibiotic therapy."
12f. Treatment Algorithm
KFD Confirmed by Biopsy
|
├── Mild disease (fever + cervical lymphadenopathy only)
| └── NSAIDs/analgesics + observation
| → Resolve in 1-4 months
|
├── Moderate-severe disease (high fever, systemic symptoms, leukopenia)
| └── Corticosteroids (prednisolone 0.5 mg/kg) ± HCQ
|
├── SLE overlap features (ANA+, anti-dsDNA+, cytopenias)
| └── Treat as SLE + HCQ + consider corticosteroids
|
└── HLH-associated KFD (hyperferritinaemia, haemophagocytosis)
└── HLH protocol + corticosteroids ± etoposide
13. Follow-Up Recommendations
| Time Point | Action |
|---|---|
| At diagnosis | ANA, anti-dsDNA, complement (C3/C4), urinalysis, FBC, renal function |
| 6 weeks | Repeat FBC, inflammatory markers; clinical reassessment |
| 3-6 months | Reassess for SLE features; repeat ANA if initially negative |
| 6-12 monthly × 2 years | Screen for SLE development; urinalysis, FBC, ANA |
| Any new symptoms | Prompt re-evaluation - new rash, renal involvement, serositis |
| Recurrence | Re-biopsy to confirm KFD; re-evaluate for SLE |
14. Key Teaching Points and Clinical Pearls
- "Young Asian woman + cervical lymphadenopathy + fever + leukopenia" = Think KFD first
- Diagnosis is histopathological - biopsy is mandatory (FNAC is insufficient)
- The absence of neutrophils in necrotic areas is the most important histological clue
- KFD closely mimics lymphoma on imaging and FNAC - never diagnose lymphoma without excisional biopsy
- Always screen for SLE in every KFD patient - may be the heralding presentation
- C4d immunostaining distinguishes KFD (negative) from lupus lymphadenitis (positive)
- KFD does NOT respond to antibiotics - avoid empirical antibiotic therapy
- NSAIDs are first-line; reserve corticosteroids for severe/SLE-overlap disease
- COVID-19 (infection and mRNA vaccination) is a recognized newer trigger
- Perforin-2 overexpression (2025 data) suggests KFD is a virus-triggered cytotoxic immune response with massive apoptosis as the pathological hallmark
- HLH can complicate KFD - check ferritin in severe cases
- WHO-5 now classifies KFD under "tumor-like lesions with T-cell predominance" - reflecting lymphoma-mimicking potential
Key References
- Goldman-Cecil Medicine (2022), Chapter on Lymphadenopathy
- Rheumatology 2-Vol Set (Elsevier, 2022), Chapter 117 (SLE - lymphatic involvement)
- Firestein & Kelley's Textbook of Rheumatology (2022), Chapter on SLE manifestations
- Quick Compendium of Clinical Pathology 5th Ed., Section 4.3.7.5.1
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1 & 2
- Harrison's Principles of Internal Medicine 22nd Ed. (2025)
- Mahajan VK et al. "Kikuchi-Fujimoto disease: A comprehensive review." World J Clin Cases 2023 [PMID: 37383134]
- Zaccarelli F et al. "Kikuchi-Fujimoto Disease: A Distinct Pathological Entity but also an Overlap Autoimmune Syndrome." Curr Rheumatol Rev 2023 [PMID: 36056828]
- Yu SC et al. "Distinguishing lupus lymphadenitis from Kikuchi disease based on clinicopathological features and C4d immunohistochemistry." Rheumatology (Oxford) 2021 [PMID: 33169134]
- Cahuapaza-Gutierrez NL et al. "Kikuchi-Fujimoto in the light of the COVID-19: infection and vaccination - A systematic review." Clin Rheumatol 2025 [PMID: 40610704]
- Lyapichev KA et al. "Perforin-2 is overexpressed in Kikuchi-Fujimoto disease." Virchows Arch 2025 [PMID: 39915303]