Chronic suppurative otitis media
Reading File
Finding Sources
Searching PubMed
"chronic suppurative otitis media" AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
chronic suppurative otitis media tympanic membrane perforation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Chronic Suppurative Otitis Media (CSOM)
Definition
CSOM is a complication of acute otitis media (AOM) characterized by persistent tympanic membrane (TM) perforation accompanied by purulent otorrhea, with mastoiditis invariably present. The diagnosis requires discharge lasting more than 2–6 weeks. — Goldman-Cecil Medicine; Textbook of Family Medicine 9e
Classification
CSOM is classified into two types based on the location of pathology:
| Type | TM Involvement | Cholesteatoma | Terminology |
|---|---|---|---|
| Tubotympanic (Safe) | Pars tensa retraction/perforation | Absent | "Safe ear" |
| Atticoantral (Unsafe) | Pars flaccida retraction | Commonly present | "Unsafe ear" |
— K.J. Lee's Essential Otolaryngology
Epidemiology & Risk Factors
- Most common in children under 2 years; disproportionately high incidence in Native Americans, Inuit, Native Australians, and Māori
- Occurs predominantly in areas with limited health resources and low socioeconomic status
- Risk factors:
- Multiple episodes of AOM; AOM in early infancy
- Chronic secretory OM
- Eustachian tube dysfunction
- Tympanostomy tube or TM perforation (allows EAC contamination of middle ear)
- Nasopharyngeal reflux
- Genetic predisposition
— K.J. Lee's Essential Otolaryngology
Pathophysiology
Eustachian Tube (ET) Dysfunction
- Abnormal ET function → decreased aeration of middle ear space
- Nitrogen-absorbing mastoid cells → volume reduction of middle ear
- Negative pressure → TM retraction (most susceptible: pars flaccida)
Biofilm Formation — Central to CSOM
Biofilms are highly organized, sessile bacterial communities that:
- Escape phagocytosis and humoral immunity via impenetrable polysaccharide matrix
- Show markedly increased antibiotic resistance (efflux pumps, decreased metabolic rate, altered gene expression)
- Are frequently polymicrobial, making targeted therapy difficult
- Can be adherent to respiratory epithelium, within mucus, or intracellular (intracellular aggregates found in middle ear specimens)
Pseudomonas aeruginosa is the most common pathogen in OM biofilms; fungal overgrowth (particularly Candida spp.) occurs in up to 35% of ears treated with topical ciprofloxacin.
— K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology
Clinical Features
Symptoms
- Chronic or recurrent otorrhea — often malodorous (hallmark symptom)
- Hearing loss — typically low-frequency conductive (mixed if cochlea involved)
- Aural fullness
Signs
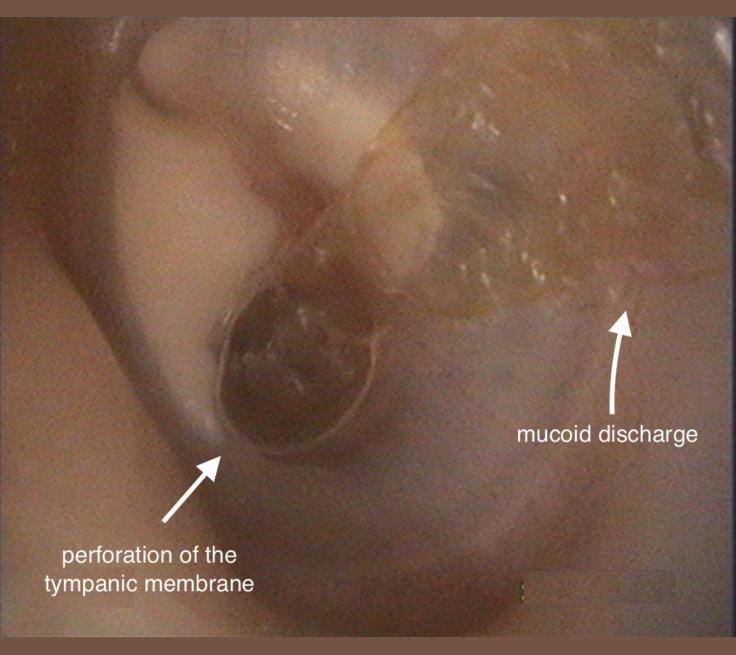
- TM perforation (compensatory mechanism for middle ear aeration)
- Inflammation of middle ear mucosa
- Granulation tissue / aural polyps — often obscure anatomical landmarks
- TM retraction pockets ± cholesteatoma
Complications (if untreated)
Extracranial: Facial nerve palsy, labyrinthitis (vertigo), subperiosteal abscess, bone destruction, petrositis
Intracranial: Brain abscess, subdural/epidural abscess, meningitis, septic venous sinus thrombosis
— K.J. Lee's Essential Otolaryngology; Textbook of Family Medicine 9e
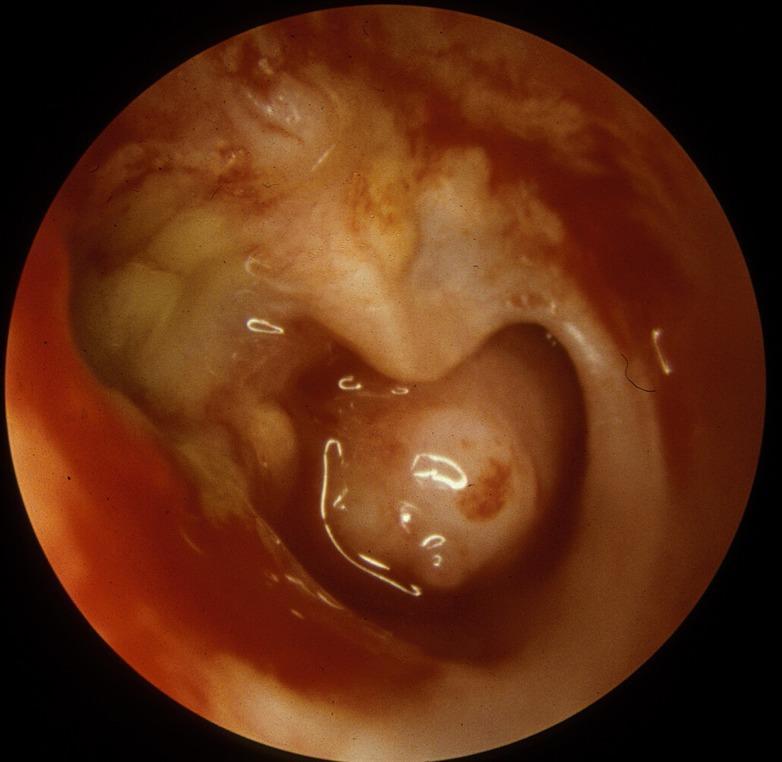
Otoscopic Appearance
Microbiology
| Organism | Notes |
|---|---|
| Pseudomonas aeruginosa | Most common in biofilms |
| Staphylococcus aureus | Common; includes MRSA |
| Non-typable H. influenzae | Common |
| M. catarrhalis | Common |
| Anaerobes | Mixed flora |
| Candida spp. | Fungal superinfection after antibiotic therapy |
— K.J. Lee's Essential Otolaryngology; Harriet Lane Handbook
Diagnosis
Key diagnostic objective: identify or exclude cholesteatoma
- An aural polyp must be considered cholesteatoma until proven otherwise
Investigations:
- Otomicroscopy with pneumatic insufflation — define perforation, retraction pockets
- Audiometry — characterize hearing loss
- High-resolution CT of temporal bones — surgical planning; indicated for complicated CSOM, cholesteatoma on exam, revision surgery
- MRI with contrast — suspected intracranial complications
- Biopsy of granulation tissue — unresponsive to topical therapy to exclude malignancy
— K.J. Lee's Essential Otolaryngology; Goldman-Cecil Medicine
Treatment
Goal: Create a Safe, Dry Ear
- Dry = no otorrhea
- Safe = no keratin debris accumulation, reduced suppurative complication risk
1. Medical Management (First-line)
- Aural toilet (microsuction/dry mopping) — essential to clear debris and biofilm; enhances topical drug penetration
- Topical antibiotics (4–6 week course after debridement):
- Fluoroquinolones (ciprofloxacin/ofloxacin ear drops) — first choice; effective against Pseudomonas
- Polymyxin B or neomycin ± steroid
- Note: biofilms are frequently resistant to topical medication
- Topical antiseptics: acetic acid/alcohol solution
A 2025 Cochrane meta-analysis (PMID 40484405) evaluated systemic antibiotics for CSOM — topical therapy remains the mainstay, with systemic agents reserved for complications or systemic illness.
2. Surgical Management
| Procedure | Indication | Notes |
|---|---|---|
| Tympanoplasty | TM perforation without cholesteatoma | 60–90% success rate; better outcomes in patients who can insufflate air through perforation |
| Tympanomastoidectomy | Cholesteatoma, refractory otorrhea | TM closure rate NOT improved by adding mastoidectomy |
| Canal Wall Up (CWU) | Preferred in children | Second-look surgery may be needed |
| Canal Wall Down (CWD) | Extensive disease, recurrent cholesteatoma | Open cavity requires regular debridement |
| Mastoid obliteration | CWD cavities | Reduces need for ongoing cavity maintenance |
Goals of surgery:
- Remove all cholesteatoma and granulation tissue
- Restore continuity between the middle ear cleft and mastoid cavity
- Permanent hearing restoration
Optimal age for tympanoplasty: Generally delayed until ~10 years; meta-analyses suggest better closure rates in older children (surgery earlier if troublesome otorrhea or hearing loss). Healthy contralateral ear is a more reliable predictor of success than age alone.
— Cummings Otolaryngology; K.J. Lee's Essential Otolaryngology
CSOM and Cochlear Implantation
Cochlear implantation was previously considered contraindicated in CSOM, but retrospective studies show OM prevalence/severity does not increase post-implantation. Current practice: implant if the ear is dry at the time of surgery, with antimicrobial prophylaxis. Multiple surgical staging protocols exist, reflecting the complexity of managing CSOM in CI candidates. — Cummings Otolaryngology
Recent Evidence
- [PMID 40178730] (Systematic Review, 2025) — Global prevalence of CSOM estimated; burden highest in low- and middle-income countries
- [PMID 40484405] (Cochrane, 2025) — Systematic review on systemic antibiotics for CSOM; current guidance favors topical therapy as primary treatment
This is a shared conversation. Sign in to Orris to start your own chat.