Perthes disease
Reading File
Finding Sources
Searching PubMed
Legg-Calve-Perthes disease
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
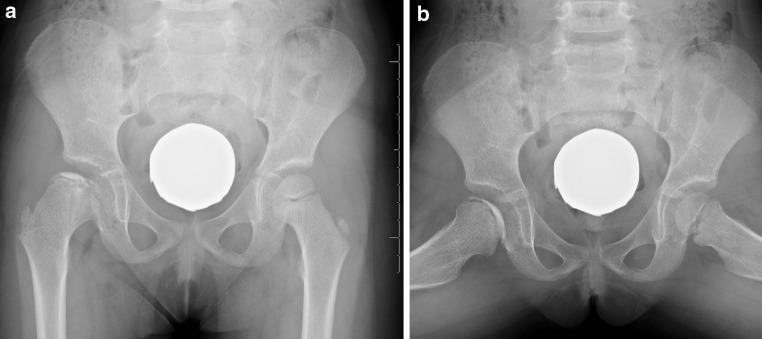
Legg-Calvé-Perthes disease hip X-ray stages
Reading File
Here is a comprehensive overview of Legg-Calvé-Perthes Disease (LCPD).
Legg-Calvé-Perthes Disease
Definition & Pathophysiology
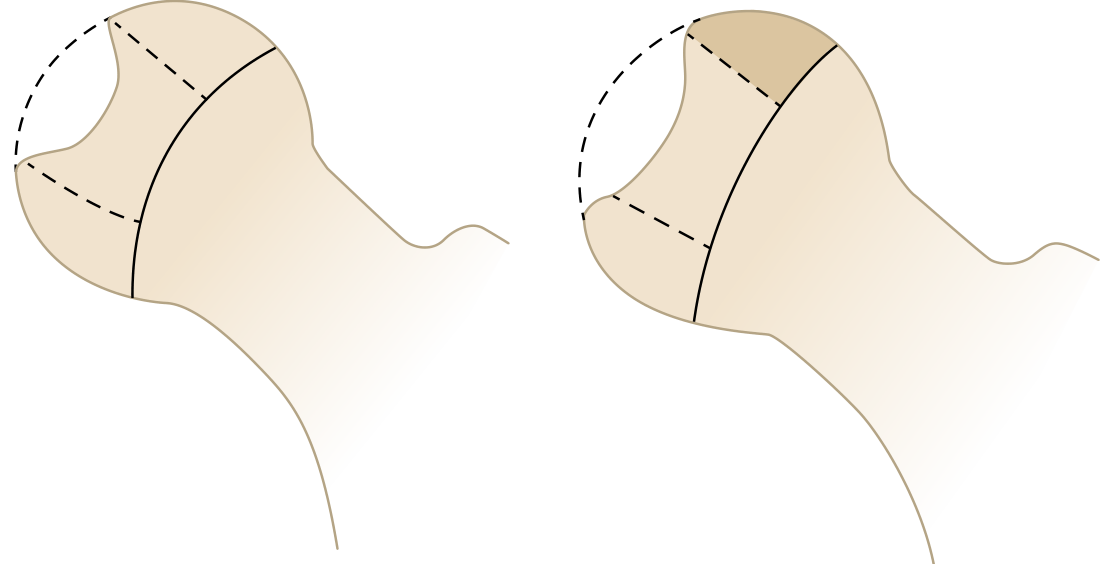
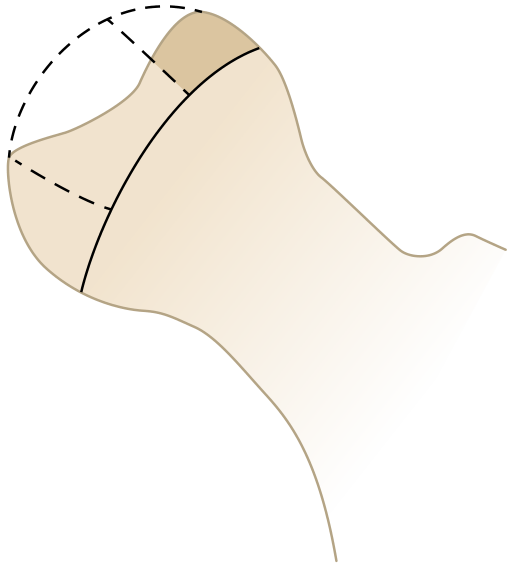
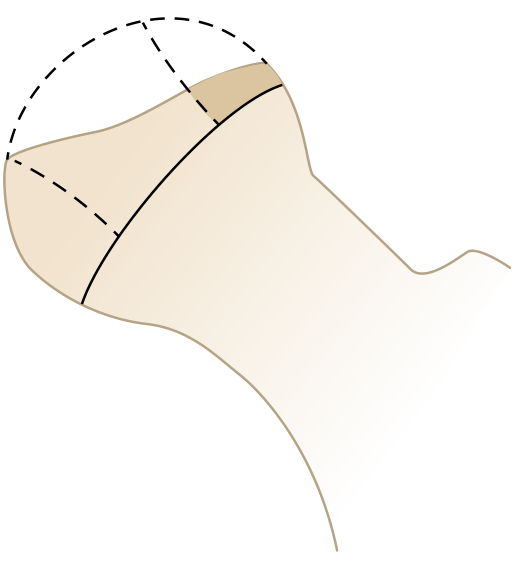
LCPD is idiopathic avascular necrosis (osteonecrosis) of the capital femoral epiphysis — a non-inflammatory deformity of the proximal femur caused by interruption of the blood supply of unknown origin. The vascular insult leads to death of the femoral head epiphysis, followed by revascularization, resorption via creeping substitution, and eventual remodeling. Throughout this process, the dominance of resorption over bone reformation causes femoral head deformity and mechanical weakening.
Epidemiology
- Sex: Boys >> Girls (boys far more commonly affected; female sex is a poor prognostic factor)
- Age: Peak incidence 4–8 years (range 3–11 years); delayed skeletal maturation typical
- Laterality: Unilateral in ~85%; bilateral in 10–15% (bilateral cases are asymmetric and usually not simultaneous)
- Risk factors: Positive family history, low birth weight, abnormal birth presentation, ADHD, very active lifestyle
- Later onset (bone age >6 years) = worse prognosis
Clinical Presentation
| Feature | Detail |
|---|---|
| Limp | Most common presenting sign |
| Pain | Insidious; hip, groin, thigh, or referred knee pain |
| Activity | Pain worse with activity, relieved by rest |
| ROM | Decreased abduction and internal rotation |
| Gait | Trendelenburg gait |
| Late signs | Buttock/thigh/calf muscle atrophy, limb length discrepancy up to 2.5 cm |
Early in disease, hip motion is generally preserved. Hip pain with synovitis and effusion may be present.
Imaging
First-line: AP pelvis + frog-leg lateral radiographs.
Early films may be normal. If symptoms persist >6 weeks with normal X-rays → MRI (most sensitive for early ischemia).
Radiographic Signs (by stage)
- Crescent sign — subchondral fracture, pathognomonic
- Cessation of ossific nucleus growth
- Medial joint space widening
- Fragmentation and collapse of the epiphysis
- Eventually sclerosis, reossification, residual deformity
Stages — Waldénström Classification
| Stage | Description |
|---|---|
| Initial | Sclerotic epiphysis + joint space widening (X-rays may be normal for 4–6 months) |
| Fragmentation | Bone resorption + collapse; most prognostically important stage |
| Reossification | New bone formation; femoral head reshaping (may last up to 18 months) |
| Healed/Remodeled | Continued remodeling until skeletal maturity |
Classification — Herring Lateral Pillar (Most Prognostic)
Assessed during the fragmentation stage on AP radiograph, based on height of the lateral pillar:
| Group | Lateral Pillar | Prognosis |
|---|---|---|
| A | Little/no involvement; normal height maintained | Uniformly good outcome |
| B | >50% of height maintained | Good if bone age <6 yrs; worse if older |
| B/C | Borderline (narrow pillar, minimal ossification, or depressed) | Intermediate |
| C | <50% of height maintained | Poor in all age groups |
Prognosis
The most important prognostic factor is maintaining sphericity of the femoral head (containment in acetabulum). Aspherical heads → early degenerative hip disease.
Poor Prognostic Factors
- Older age at onset (bone age >6 years)
- Female sex
- Lateral pillar group C (regardless of age)
- Decreased hip ROM (especially abduction)
Catterall "Head-at-Risk" Radiographic Signs
- Lateral calcification
- Gage sign (V-shaped defect at lateral physis)
- Lateral subluxation
- Metaphyseal cyst formation
- Horizontal growth plate
Differential Diagnosis
- Septic arthritis (urgent exclusion)
- Transient synovitis
- Blood dyscrasias (sickle cell, Gaucher's)
- Hypothyroidism
- Multiple epiphyseal dysplasia (bilateral LCPD mimics MED → obtain skeletal survey)
Management
Goals: Relief of symptoms · Restoration of ROM · Containment of the femoral head within the acetabulum
Non-Surgical
- Rest, activity restriction, partial weight-bearing with crutches
- Anti-inflammatory medications (NSAIDs)
- Physical therapy / traction
- Petrie cast (abduction) to maintain ROM
- Bracing
Surgical (for older patients >8 years chronologic / >6 years bone age, with Group B or B/C hips)
| Procedure | Indication |
|---|---|
| Proximal femoral varus osteotomy | Containment |
| Salter / Triple / Dega / Pemberton pelvic osteotomy | Containment |
| Shelf osteotomy | Prevent lateral subluxation / epiphyseal overgrowth |
| Valgus femoral osteotomy | Salvage for hinge abduction |
| Chiari pelvic osteotomy | Salvage for uncontainable hips |
Lateral pillar C hips generally have poor outcomes regardless of treatment, due to lack of sphericity at skeletal maturity.
Imaging Example

Recent Evidence (2024–2026)
- A 2024 systematic review/meta-analysis (PMID 39261944) quantified the prevalence of LCPD in children presenting with transient synovitis — highlighting the clinical overlap and diagnostic challenge.
- A 2026 systematic review (PMID 41308557) evaluated diffusion-weighted MRI (DWI) for LCPD diagnosis, supporting its role as a sensitive early imaging modality.
Sources: Miller's Review of Orthopaedics 9th Ed. · Rosen's Emergency Medicine · Tintinalli's Emergency Medicine · Grainger & Allison's Diagnostic Radiology
Mrcs style review
Here is an MRCS-style review of Legg-Calvé-Perthes Disease, covering the high-yield facts most likely to appear in SBAs and EMQs.
Legg-Calvé-Perthes Disease — MRCS Style Review
SBA-Style Questions
Q1. A 6-year-old boy presents with a 3-week history of limp and left knee pain. Examination reveals decreased internal rotation and abduction of the left hip with a Trendelenburg gait. AP pelvis X-ray shows medial joint space widening and a crescent sign.
What is the most likely diagnosis?
A. Septic arthritis
B. Transient synovitis
C. Legg-Calvé-Perthes disease
D. Slipped capital femoral epiphysis
E. Developmental dysplasia of the hip
Answer & Explanation
C — Legg-Calvé-Perthes disease
The crescent sign (subchondral fracture) is pathognomonic for LCPD. The age group (4–8 years), sex (male), referred knee pain, and Trendelenburg gait are all classic. Septic arthritis would present acutely with fever and a systemically unwell child. SCFE occurs in older, typically obese adolescents.
Q2. A child is diagnosed with LCPD. During the fragmentation stage, AP pelvis X-ray shows that the lateral pillar has collapsed to 40% of its original height.
According to the Herring lateral pillar classification, which group does this child belong to, and what is the prognosis?
A. Group A — uniformly good
B. Group B — good if bone age <6 years
C. Group B/C — borderline
D. Group C — poor in all age groups
E. Group D — salvage required
Answer & Explanation
D — Group C: poor in all age groups
Group C = <50% of lateral pillar height maintained → poor prognosis regardless of age. Group B = >50% maintained. Group B/C is borderline (narrow pillar, little ossification, or depressed vs central pillar).
Q3. A 5-year-old girl is diagnosed with LCPD. Initial X-rays are normal, but symptoms have persisted for 8 weeks.
What is the most appropriate next investigation?
A. CT pelvis
B. Bone scan (technetium-99m)
C. Ultrasound of the hip
D. MRI of the hip
E. Repeat X-ray in 4 weeks
Answer & Explanation
D — MRI of the hip
MRI is the most sensitive modality for early LCPD when X-rays are normal but symptoms persist >6 weeks. It detects early ischaemia and marrow changes before radiographic changes appear. Ultrasound may show effusion but is non-specific. CT carries radiation risk and is not indicated.
Q4. A 9-year-old boy with LCPD (Herring Group B, bone age 7 years) fails conservative management with physiotherapy and bracing.
What is the most appropriate surgical treatment?
A. Hip replacement
B. Proximal femoral varus osteotomy
C. Hip arthroscopy and labral repair
D. Chiari osteotomy
E. Valgus femoral osteotomy
Answer & Explanation
B — Proximal femoral varus osteotomy
Containment surgery is indicated in older children (>8 years chronological / >6 years bone age) with Group B or B/C hips. The goal is to seat the femoral head within the acetabulum to promote spherical remodeling. Options include proximal femoral varus osteotomy or pelvic osteotomies (Salter, Triple, Dega, Pemberton).
Chiari and valgus femoral osteotomy are salvage procedures for uncontainable hips or hinge abduction — not first-line.
Q5. Which of the following is NOT a Catterall "head-at-risk" radiographic sign in LCPD?
A. Gage sign
B. Lateral calcification
C. Crescent sign
D. Metaphyseal cyst
E. Horizontal growth plate
Answer & Explanation
C — Crescent sign
The crescent sign is a sign of subchondral fracture indicating disease (pathognomonic for LCPD), but it is NOT a Catterall head-at-risk sign.
The 5 head-at-risk signs are:
- Lateral calcification
- Gage sign (V-shaped defect at lateral physis)
- Lateral subluxation
- Metaphyseal cyst formation
- Horizontal (horizontal orientation) growth plate
Q6. A 7-year-old boy presents with bilateral hip pain and limp. X-rays show bilateral epiphyseal changes. LCPD is suspected.
What investigation should be arranged to exclude a mimicking condition?
A. Thyroid function tests
B. Skeletal survey
C. Full blood count and film
D. Echocardiogram
E. Hip arthroscopy
Answer & Explanation
B — Skeletal survey
Bilateral LCPD (10–15% of cases) must prompt exclusion of multiple epiphyseal dysplasia (MED). A skeletal survey evaluates all epiphyses systemically. Hypothyroidism and blood dyscrasias (sickle cell, Gaucher's) should also be considered, but the MED mimic specifically warrants skeletal survey.
High-Yield Summary Table
| Feature | Key Fact |
|---|---|
| Pathology | Idiopathic AVN of capital femoral epiphysis |
| Peak age | 4–8 years (boys >> girls) |
| Bilateral | 10–15% (asymmetric, not simultaneous) |
| Classic triad | Limp + hip/knee pain + ↓ IR & abduction |
| Pathognomonic sign | Crescent sign (subchondral fracture) |
| Staging | Waldénström: Initial → Fragmentation → Reossification → Healed |
| Best prognostic tool | Herring lateral pillar (assessed at fragmentation stage) |
| Worst group | Group C (<50% lateral pillar height) = poor all ages |
| Early imaging | MRI if X-ray normal after 6 weeks |
| Treatment goal | Containment of femoral head in acetabulum |
| Surgery threshold | Age >8 years (or bone age >6) + Group B or B/C |
| Containment surgery | Proximal femoral varus OR pelvic osteotomy |
| Salvage | Valgus osteotomy / Chiari osteotomy |
| Poor prognostic factors | Older age, female sex, Group C, ↓ ROM |
| MED mimic | Bilateral cases → skeletal survey |
EMQ Theme: Paediatric Hip Disorders
Options: Transient synovitis · LCPD · SCFE · Septic arthritis · DDH · Juvenile idiopathic arthritis
| Scenario | Answer |
|---|---|
| Obese 13-year-old boy, limp, obligate external rotation on hip flexion | SCFE |
| 6-year-old boy, 3-week limp, crescent sign on X-ray | LCPD |
| 4-year-old, 2-day history, fever 38.5°C, refuses to move hip, elevated CRP | Septic arthritis |
| 5-year-old, sudden-onset limp after URTI, normal X-ray, ultrasound shows effusion, afebrile | Transient synovitis |
| Newborn girl, asymmetric skin folds, positive Barlow/Ortolani | DDH |
One-Liners for the Exam
- Crescent sign = subchondral fracture = LCPD confirmed on X-ray
- Gage sign = V-shaped defect at lateral physis = head-at-risk
- Herring Group C = <50% lateral pillar = bad regardless of age
- MRI = investigation of choice when X-ray is normal but LCPD suspected
- Bilateral LCPD → always exclude MED with skeletal survey
- Treatment = containment; surgery for older children with Group B/B/C
- Trendelenburg gait + decreased internal rotation + referred knee pain in a boy aged 4–8 = LCPD until proven otherwise
This is a shared conversation. Sign in to Orris to start your own chat.