
I am plastic surgery third year resident. I want to do tempo Ro parietal fascia flap in above patient for post auricular defect. Kindly give me relevant Anatomy, types of flap, STA anatomy, incision and operative techniques in detail from standard plastic surgery textbook. Also give me crisp point for the same topic and give me viva questions asked from above topic. Also include images of incision, operative steps and anatomical diagram.
temporoparietal fascia flap post auricular reconstruction anatomy operative technique
temporoparietal fascia flap anatomy STA operative technique incision types
temporoparietal fascia flap operative technique steps incision layers anatomy STA facial nerve
temporoparietal fascia flap anatomical diagram layers STA incision images surgical steps
Clinical Assessment of the Patient Image
TEMPOROPARIETAL FASCIA FLAP (TPFF)
A Complete Guide for the Plastic Surgery Resident
PART 1: SURGICAL ANATOMY
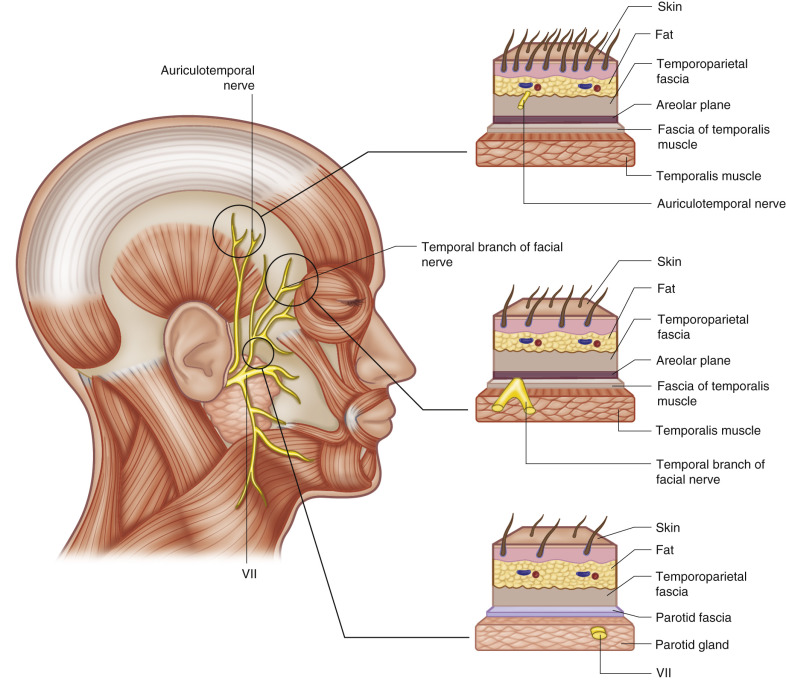
Layers of the Temporal Region (Superficial to Deep)
| Layer | Details |
|---|---|
| 1. Skin | Hair-bearing scalp |
| 2. Subcutaneous fat | Contains hair follicles |
| 3. Temporoparietal Fascia (TPF) | The flap itself - thin, well-vascularized, STA runs within it |
| 4. Loose areolar plane (innominate fascia) | The correct dissection plane - avascular |
| 5. Deep temporal fascia | Thick, white, invests the temporalis muscle (split into superficial & deep layers below temporal line) |
| 6. Temporalis muscle |
Key Anatomical Facts about the TPF
- Also called: superficial temporal fascia, epicranial aponeurosis, galeal extension
- Continuous with: SMAS inferiorly, galea superiorly, frontalis anteriorly, occipitalis posteriorly
- Thickness: 2-3 mm
- The transition from TPF to galea occurs at the temporal line
- Above the temporal line: fibrous connections between dermis and fascia become more numerous, making dissection tedious
- Below the temporal line: loose areolar plane separates TPF from deep temporal fascia (easy dissection)
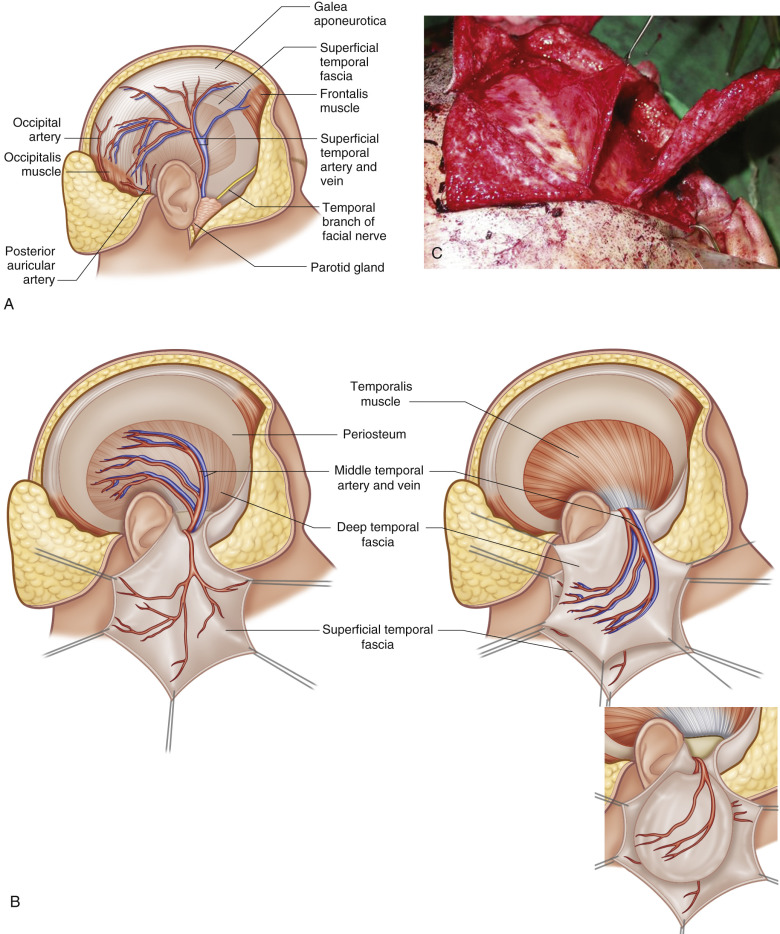
PART 2: SUPERFICIAL TEMPORAL ARTERY (STA) ANATOMY
Origin and Course
- Origin: Terminal branch of the external carotid artery (ECA), arises within the parotid gland
- The STA gives off the transverse facial artery at or just below the level of the zygomatic arch
- After crossing the zygomatic arch, it enters the temporoparietal fascia
- Bifurcation: Occurs 3-5 cm above the zygomatic arch into:
- Frontal (anterior) branch: Runs toward the forehead; temporal branch of facial nerve crosses under this
- Parietal (posterior) branch: Runs toward the parietal scalp; connects with posterior auricular and occipital arteries
Vessel Caliber
- At the zygomatic arch level: ~2 mm diameter
- Distal branches: ~1.5 mm diameter
- Pedicle length: Minimum 4 cm; can be extended to at least 3 cm below a large TPFF by dissecting inferiorly into the parotid gland
- Important note: The STA is prone to vasospasm - handle with great care; papaverine-soaked pledgets are helpful
Venous Drainage
- Superficial temporal vein parallels the STA, running just posterior to it
- Drains into the retromandibular vein
- Critical: The vein is superficial to the fascia, making it vulnerable during harvest
Vascular Supply Variations
- 88.2% supplied by STA
- 8.6% by posterior auricular artery
- 3.2% by occipital artery
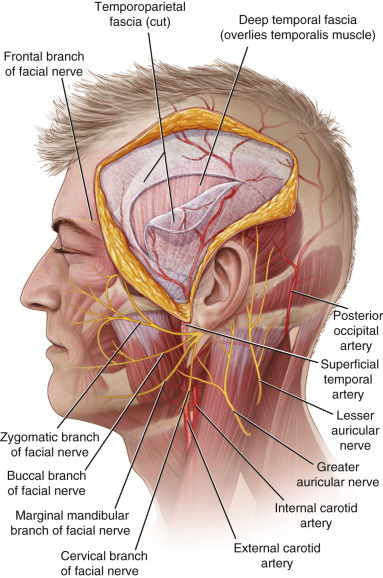
Important Nerves at Risk
-
Frontal (temporal) branch of facial nerve (CN VII):
- Runs on the undersurface of the TPF
- Course: From a point just inferior to the tragus to the lateral brow (Pitanguy's line)
- Most vulnerable nerve during dissection
- Located: in the fascia plane between TPF and the innominate fascia
- Identified with nerve stimulator set at 10 mA before incision
-
Auriculotemporal nerve (branch of V3):
- Lies posterior to the STA
- Provides sensation to the lateral scalp
- Usually divided during flap elevation - creates an insensate area on the lateral scalp
PART 3: FLAP DESIGN AND DIMENSIONS
Flap Dimensions
- Maximum size: 14-17 cm in height x 10-14 cm in width
- Flap may extend up to 3-4 cm superior to the origin of the temporalis muscle
- Pedicle base: At least 2-3 cm of tissue preserved around pedicle at the pretragal level
Flap Classification
- Type A fasciocutaneous flap (Mathes & Nahai) - direct cutaneous pedicle (STA)
PART 4: TYPES OF TPFF
Based on Composition
| Type | Contents | Uses |
|---|---|---|
| Fascial only | TPF alone | Post-auricular, orbital, periorbital defects; skin-grafted |
| Fasciocutaneous | TPF + overlying hair-bearing scalp | Total ear reconstruction, nasal reconstruction |
| Composite (osteo-fascial) | TPF + split-thickness calvarial bone | Orbit, mandible reconstruction |
| Two-layered | TPF + deep temporal fascia | Large defects requiring extra bulk |
| Free flap | TPF harvested on STA vessels for microsurgery | Hand, lower extremity reconstruction |
Based on Pedicle Orientation
| Type | Pedicle | Application |
|---|---|---|
| Anteriorly pedicled (standard) | Frontal branch of STA | Forehead, periorbital, anterior defects |
| Posteriorly pedicled | Parietal branch / posterior auricular artery | Post-auricular, temporal, ear reconstruction |
| Inferiorly pedicled | Main STA trunk | Maximum arc of rotation |
PART 5: INDICATIONS AND CONTRAINDICATIONS
Indications
- Post-auricular defects (skin coverage after trauma, tumor, or implant extrusion - as in your patient)
- Auricular reconstruction (Brent technique: cartilage covered by TPFF + STSG)
- Partial or total ear reconstruction
- Orbital and periorbital reconstruction
- Forehead reconstruction
- Skull base defects
- Nasal reconstruction
- Facial contour defects
- Oral mucosal defects (free flap)
- Tendon gliding surface (free flap)
Contraindications
- Absolute: Prior sacrifice or injury to the STA (check with handheld Doppler preoperatively)
- Relative: Prior surgery/trauma disrupting the TPF layer; bald patients or receding hairline (visible scar); prior radiation with tissue fibrosis; hemifacial microsomia (hypoplastic STA)
PART 6: PREOPERATIVE PLANNING
- Handheld Doppler to trace the course of STA from pretragal region to vertex
- Mark the STA course - a line from the pretragal region to the vertex marks the STA course
- Assess hair density (scar visibility)
- Note any prior surgery or trauma in the temporal region
- Assess defect size and determine flap dimensions needed
- Use nerve stimulator (10 mA) to identify the approximate course of the frontal branch transcutaneously before incision
PART 7: INCISION DESIGN
Standard Incision Options
-
"Y"-shaped incision (most common): Preauricular rhytidectomy incision that bifurcates into a Y shape 1-2 fingerbreadths above the helical root. Provides wide exposure and conceals scar.
-
"T"-shaped incision: Vertical limb from helical crus superiorly 12-14 cm, with a horizontal limb at the top. Good anterior and posterior exposure.
-
"V" (inverted V) at the top: Modification of the vertical incision for better exposure superiorly.
-
Lazy-S or zigzag: Alternative incisions to break up scar line.
-
Simple linear incision: For narrow flaps.
Key Incision Principles
- Incision begins anterior to the ear in the preauricular crease
- Runs posterior to and parallel to the STA
- Bifurcates 1-2 fingerbreadths above the upper pole of the ear
- Incision should be made just over the temporal vessels (they can be palpated or Doppler-located)
- In the post-auricular approach for posterior defects: a posterior auricular incision extended superiorly gives access to posterior TPF

PART 8: OPERATIVE TECHNIQUE - STEP BY STEP
Patient Positioning and Setup
- Supine with ipsilateral shoulder roll, head turned contralaterally
- Entire scalp and face prepped
- Shave only along the incision line (not entire scalp - preserves camouflage)
- Marking pen to delineate STA course (Doppler-guided)
- Loupe magnification used throughout
Step 1: Identifying the Superficial Temporal Vessels
- Palpate and Doppler-mark the STA anterior to the tragus
- Use nerve stimulator to map the frontal branch of CN VII transcutaneously
Step 2: Incision
- Begin the preauricular incision in the rhytidectomy crease
- Carry incision superiorly, bifurcating into Y/T shape approximately 1-2 cm above the helical root
- Depth: Carry incision down to the level of the temporoparietal fascia
- Best plane: first identify the plane containing the superficial temporal vessels several centimeters above the ear
Step 3: Identifying the Correct Plane
- The TPF plane is best identified by staying in the plane containing the STA/STV
- This plane lies just below the hair follicles
- The dissection is immediately deep to the subcutaneous fat - there is no avascular plane between skin and fascia; meticulous sharp dissection required
Step 4: Elevation of the Overlying Skin Flaps
- Elevate the anterior and posterior scalp skin off the fascia (not with it)
- This step is tedious and cannot be rushed without injuring the flap
- The frontal branch of CN VII runs on the undersurface of the TPF - identify it with the nerve stimulator
- Once identified, do NOT dissect the TPF below that level
- The plane becomes more superficial as you go superiorly
Step 5: Marking and Incising the Flap
- Mark the desired flap dimensions based on defect size
- Incise the TPF along the marked perimeter
- Leave at least 2-3 cm around the pedicle at the pretragal level
- The TPF flap may be based on parietal branch (for post-auricular reach)
Step 6: Elevating the Flap
- Elevate TPF from the deep temporal fascia by blunt dissection in the loose areolar plane
- This is the avascular plane - easier than the superficial dissection
- Proceed from distal to proximal
- Preserve the middle temporal artery (which perforates to supply deep temporal fascia)
Step 7: Lengthening the Pedicle (if needed)
- Dissect the STA and STV proximally in the pretragal region (within parotid gland) under loupe magnification
- This provides an additional 3+ cm of pedicle length
- Vessel caliber at this level increases to ~2 mm
Step 8: Tunneling/Transferring to the Post-Auricular Defect
- For post-auricular defects: tunnel the flap either over or under the helix/ear
- Alternatively, for very posterior defects, the flap can be passed through a subcutaneous tunnel posterior to the ear
- Avoid kinking the pedicle at the pivot point
- For turndown flap technique: fold the fascial flap over the defect
Step 9: Flap Inset and Coverage
- The TPFF alone does NOT provide skin coverage - requires a split-thickness skin graft (STSG) over the fascial surface
- The TPFF accepts skin grafts on both surfaces (unique advantage)
- STSG is harvested (usually from thigh) and applied over the flap
- Bolster dressing applied over STSG
Step 10: Donor Site Closure
- Donor site: close scalp in layers over suction drains
- Preauricular incision: close with fine suture in face-lift fashion (5-0 or 6-0 nylon)
- Head dressed with gentle pressure using Kerlix rolls over cotton
- Scalp staples removed at Day 10
Post-Operative Care
- Careful hair washing from Day 3-4 with mild baby shampoo
- Antibiotic solution reapplied to incision line
- Glasses modification if they apply pressure to preauricular area
PART 9: ADVANTAGES AND DISADVANTAGES
Advantages
- Thinnest, most pliable flap in the body
- Highly vascularized with reliable pedicle
- Accepts skin graft on both surfaces
- Donor site well camouflaged in hair-bearing scalp
- Large flap possible (up to 14 x 17 cm)
- Two-team simultaneous harvest
- Can incorporate hair-bearing skin, calvarial bone, or two fascial layers
- Proximity to head and neck defects
- Minimal donor site morbidity
- Pedicle diameter large enough for microsurgical anastomosis when free flap needed
Disadvantages (K.J. Lee's Essential Otolaryngology)
- Small-caliber donor vessels
- Vein is superficial to fascia - vulnerable during harvest
- Risk of injury to the frontal branch of CN VII (most feared complication)
- Risk of alopecia at donor site (from flap elevation, tension, or scarring)
- Does not provide primary skin coverage (needs STSG)
- Cannot be used if STA previously sacrificed
- Lateral scalp sensory loss (auriculotemporal nerve usually divided)
PART 10: COMPLICATIONS
| Complication | Cause | Prevention |
|---|---|---|
| Frontal branch CN VII palsy | Deep dissection through fascia | Nerve stimulator guidance, staying in correct plane |
| Alopecia | Injury to hair follicles, tension | Gentle dissection, avoid electrocautery near follicles |
| Flap failure/necrosis | Pedicle kinking, STA injury | Doppler pre-op, gentle handling, papaverine |
| STSG loss | Poor contact with flap | Bolster dressing, adequate hemostasis |
| Hematoma | Inadequate hemostasis | Suction drains, pressure dressing |
| Seroma | Dead space | Closed suction drains |
| Visible scar | Hairless patient | Relative contraindication in bald patients |
PART 11: CRISP POINT SUMMARY FOR QUICK REVISION
- TPFF = thinnest, most pliable flap in the body; up to 14 x 17 cm
- Blood supply: STA (88.2%), posterior auricular (8.6%), occipital (3.2%)
- STA origin: ECA, within parotid gland; crosses zygomatic arch; bifurcates 3-5 cm above zygomatic arch
- STA diameter: ~2 mm at arch; ~1.5 mm distally; prone to vasospasm
- STA vein runs posterior to artery; drains into retromandibular vein
- Correct dissection plane: Loose areolar (innominate fascia) between TPF and deep temporal fascia
- TPF is continuous with SMAS below, galea above, frontalis anteriorly, occipitalis posteriorly
- Most feared complication: Frontal branch CN VII palsy (runs on undersurface of TPF)
- Auriculotemporal nerve usually divided - creates lateral scalp sensory loss
- Incision: Preauricular Y/T shape; bifurcation 1-2 fingerbreadths above helical root
- TPFF does NOT provide skin - needs STSG (accepts graft on both surfaces)
- Flap classification: Type A fasciocutaneous (Mathes & Nahai)
- Pre-op essential: Handheld Doppler to trace STA; nerve stimulator for frontal branch
- Pedicle lengthening: Dissect STA into parotid gland - 3+ cm extra length, vessel caliber ~2 mm
- Donor closure: Over suction drains; scalp staples out Day 10
- For post-auricular defects: Posteriorly-pedicled TPFF based on parietal branch OR turndown technique
- Composite options: + calvarial bone (orbital/mandible); + hair-bearing skin (ear framework); + deep temporal fascia (two-layered flap)
- Contraindicated: Prior STA sacrifice, significant temporal radiation fibrosis, bald patients (relative)
PART 12: VIVA QUESTIONS WITH ANSWERS
Basic Science / Anatomy
Primary: Superficial temporal artery (terminal branch of ECA). It bifurcates 3-5 cm above the zygomatic arch into frontal and parietal branches. STA arises within the parotid gland. Minor alternative pedicles: posterior auricular artery and occipital artery.
Skin - Subcutaneous fat - Temporoparietal fascia (STA/STV within it) - Loose areolar plane (innominate fascia) - Deep temporal fascia (superficial layer over temporal fat pad, deep layer over temporalis) - Temporalis muscle - Periosteum - Temporal bone.
The superficial temporal vein runs just posterior to the STA within the TPF. It drains into the retromandibular vein. The vein is superficial to the fascia, making it vulnerable during elevation.
The frontal (temporal) branch of the facial nerve (CN VII). It runs on the undersurface of the TPF, along a line from a point just inferior to the tragus to the lateral brow (Pitanguy's line). Injury causes ipsilateral brow ptosis and inability to raise the forehead.
A line from 0.5 cm below the tragus to 1.5 cm above the lateral eyebrow - represents the course of the frontal branch of the facial nerve. This branch enters the deep surface of the frontalis muscle.
Operative Technique
Deep to the TPF in the loose areolar (innominate fascia) plane, which separates the TPF from the deep temporal fascia. This is the avascular cleavage plane. The superficial dissection (skin off fascia) has no avascular plane and requires meticulous sharp dissection.
Dissect the STA and STV proximally within the preauricular region and into the parotid gland under loupe magnification. This provides at least 3 additional cm of pedicle length and increases vessel caliber to approximately 2 mm.
Most likely pedicle kinking or compression (especially at tunnel entry point) or STA vasospasm. Management: relieve tension, ensure no kinking at pivot point, apply warm papaverine-soaked pledgets, optimize blood pressure, ensure normothermia, and ensure adequate venous drainage (check vein position).
Preauricular incision in the rhytidectomy crease, carried superiorly and bifurcating into a Y or T shape 1-2 fingerbreadths above the helical root. The incision runs posterior to and parallel to the STA (Doppler-marked preoperatively). For a post-auricular defect, the flap is based on the parietal branch of the STA; the flap is passed in a subcutaneous tunnel posterior to the ear.
The TPFF is a fascial flap with no skin component. The raw (deep) surface exposed after transfer is covered with an STSG. The unique advantage is that the TPFF accepts skin grafts on BOTH surfaces (superficial and deep), making it extremely versatile.
Clinical Decision Making
TPFF is preferred when: the defect is large (>2-3 cm), involves exposed bare cartilage (where STSG alone would fail), there is poor local tissue quality (scarred, irradiated), when a thin and pliable vascularized bed is needed over a cartilaginous framework, or when the local tissue is insufficient to close primarily.
The Brent technique for total ear reconstruction uses autologous costal cartilage framework covered with TPFF + STSG. The fascial flap provides a vascularized envelope that allows the cartilage to survive and the STSG to take, creating a well-contoured ear reconstruction.
Absolute: Prior sacrifice or confirmed absence of STA (check with Doppler preoperatively). Relative: Previous surgery/trauma disrupting TPF, prior radiation with fibrosis to the temporal region, baldness (visible scar), hypoplastic STA (as in hemifacial microsomia).
The STA and STV are divided at their origin near the zygomatic arch, providing approximately 2 mm caliber vessels. For hand reconstruction: recipient arteries - radial artery (end-to-side preferred), posterior interosseous artery; recipient veins - cephalic vein, dorsal venous arch.
14-17 cm in height and 10-14 cm in width (larger dimensions reported up to 17 x 14 cm in some series). Flap may extend up to 3-4 cm superior to the temporal line.
- K.J. Lee's Essential Otolaryngology, 11th Edition (textbook)
- StatPearls: Temporoparietal Fascia Flaps
- Plastic Surgery Key: TPFF Chapter
- Iowa Head and Neck Protocols: TPFF
- Medsci: Versatile Use of TPFF (57 cases)
- Mathes SJ, Nahai F - Reconstructive Surgery: Principles, Anatomy & Technique