Hepatitis pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the key content and images. Let me compile the comprehensive answer.
Hepatitis - Pathology
Source: Robbins & Kumar Basic Pathology, Robbins Cotran & Kumar Pathologic Basis of Disease
Overview
"Hepatitis" covers two overlapping concepts: (1) diseases caused by hepatotropic viruses (HAV, HBV, HCV, HDV, HEV) with specific liver tropism, and (2) a pattern of acute or chronic hepatic injury that can also be produced by other viruses (EBV, CMV), autoimmune reactions, drugs, and toxins. Serologic and molecular studies are essential to distinguish the specific cause.
The Hepatotropic Viruses - Comparison
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|---|
| Virus type | ssRNA picornavirus | dsDNA hepadnavirus | ssRNA flavivirus | ssRNA (defective) | ssRNA hepevirus |
| Transmission | Fecal-oral | Parenteral, sexual, perinatal | Parenteral (mainly) | Parenteral (needs HBV) | Fecal-oral (waterborne) |
| Incubation | 2-6 weeks | 4-26 weeks | 2-26 weeks (mean 6-12) | Weeks | 2-8 weeks |
| Chronic hepatitis | No | Yes (~5-10% adults, >90% neonates) | Yes (~80%) | Yes (>80% superinfection) | No (except immunocompromised) |
| Carrier state | No | Yes | Yes | Yes | No |
| HCC risk | No | Yes | Yes | Yes | No |
Hepatitis A Virus (HAV)
- Nonenveloped, positive-strand RNA picornavirus (genus Hepatovirus)
- Transmission: fecal-oral route - contaminated water/food, shellfish, infected food handlers
- Incubation: 2-6 weeks; shed in stool 2-3 weeks before and 1 week after jaundice onset
- Course: self-limited; does NOT cause chronic hepatitis; fulminant hepatitis in ~0.1%
- HAV is not cytopathic - injury is mediated by cytotoxic CD8+ T cells
- Serology: IgM anti-HAV = acute infection marker; IgG anti-HAV = past infection/immunity (persists lifelong)
Fig. 14.8 - Serologic markers in acute Hepatitis A:
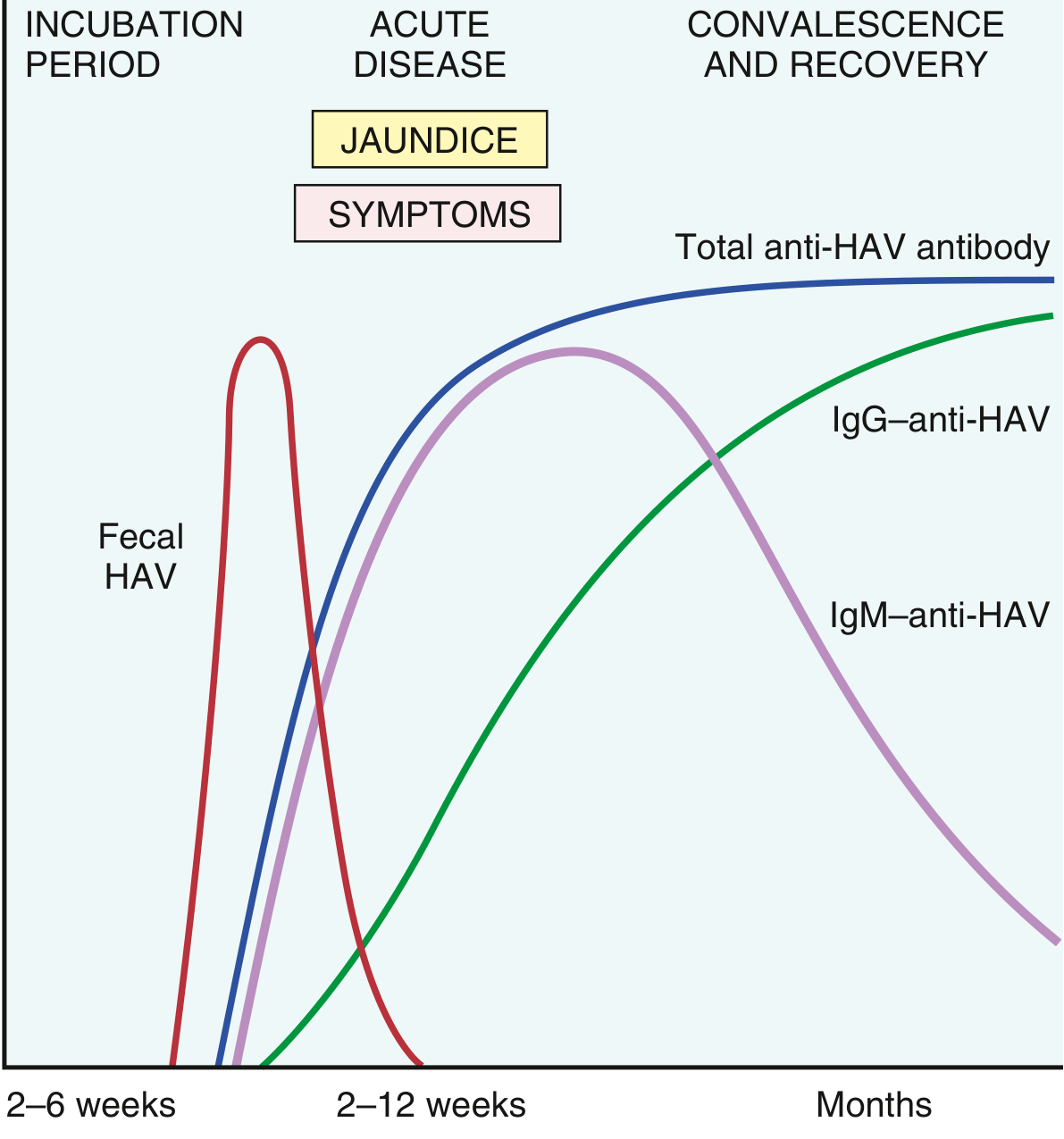
Fecal HAV peaks before symptoms. IgM appears at symptom onset and declines over months. IgG anti-HAV persists lifelong.
Hepatitis B Virus (HBV)
-
Member of Hepadnaviridae; partially double-stranded circular DNA (~3200 nucleotides)
-
Four key proteins encoded:
- HBcAg - nucleocapsid core protein (stays in hepatocytes)
- HBeAg - secreted precore polypeptide; marker of active replication
- HBsAg - envelope glycoprotein; massive quantities secreted (non-infective particles); marker of infection
- HBx protein - required for replication; may transactivate cellular growth genes (role in HCC)
- Pol - DNA polymerase + reverse transcriptase (target of antiviral drugs); genome replicates via DNA→RNA→DNA
-
Epidemiology: 2 billion infected worldwide; 250 million chronic infections; 75% of carriers in Asia/Western Pacific
-
Transmission: perinatal (high-prevalence regions), horizontal child-to-child (intermediate), sexual/IV drug use (low-prevalence)
Outcomes of HBV infection:
- Acute hepatitis with recovery and viral clearance
- Nonprogressive chronic hepatitis
- Progressive chronic disease → cirrhosis
- Fulminant hepatitis with massive liver necrosis
- Asymptomatic "healthy" carrier state
Risk of chronicity is age-dependent: >90% after perinatal infection vs. ~5-10% in adults.
Hepatitis C Virus (HCV)
- Enveloped, positive-strand RNA flavivirus
- High chronicity rate (~80%) - the major cause of chronic viral hepatitis globally
- Transmission: primarily parenteral (IV drug use, transfusions before 1992 screening); sexual and perinatal transmission less efficient than HBV
- HCV has high genetic variability due to error-prone RNA replication → immune evasion → chronicity
- Associated with cryoglobulinemia (~35% of chronic HCV) and membranoproliferative glomerulonephritis
Fig. 14.12 - HCV serology - Acute resolution (A) vs. progression to chronic disease (B):
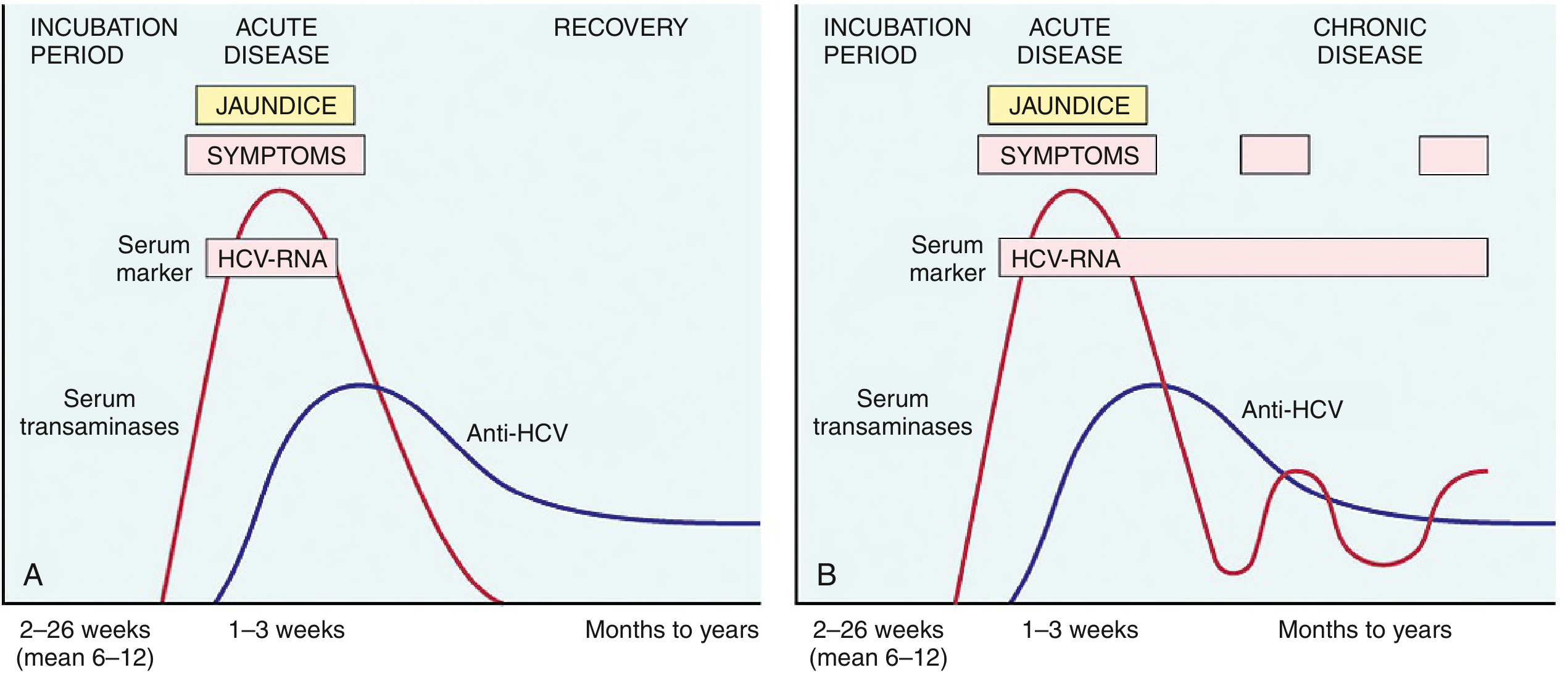
In chronic HCV (B), HCV-RNA persists indefinitely with fluctuating transaminases. Anti-HCV does not confer protective immunity.
Hepatitis D Virus (HDV)
- "Delta agent" - defective RNA virus; requires HBV (uses HBsAg as its envelope) for infection
- Two patterns:
- Coinfection (HDV + HBV simultaneously): usually self-limiting; higher acute liver failure risk in IV drug users
- Superinfection (HDV on chronic HBV carrier): >80% progress to chronic HDV; accelerates cirrhosis and HCC
- Affects ~15 million people worldwide; highest prevalence in Amazon basin, Africa, Middle East, Southern Italy
- Prevention: HBV vaccination protects against HDV (since HDV cannot exist without HBV)
Hepatitis E Virus (HEV)
- Enterically transmitted, waterborne; ssRNA hepevirus
- Zoonotic reservoir: pigs, monkeys, cats, dogs
- Typically self-limiting; accounts for 30-60% of sporadic acute hepatitis in India
- Key distinguishing feature: mortality ~20% in pregnant women (unique among hepatitis viruses)
- Does not typically cause chronic liver disease (exception: immunocompromised patients)
Histopathology / Morphology
Acute Viral Hepatitis
- Liver may be normal, enlarged (inflammation), or shrunken (massive necrosis)
- Microscopically:
- Portal and lobular lymphocytic infiltrate (lymphocytes + plasma cells + eosinophils)
- Hepatocyte injury - necrosis or apoptosis (acidophil/Councilman bodies = apoptotic hepatocytes)
- Ballooning degeneration of hepatocytes (swollen, pale)
- Confluent necrosis in severe cases; can progress to bridging necrosis (connecting portal tracts/central veins) or panlobular necrosis (= massive hepatic necrosis/acute liver failure)
Chronic Viral Hepatitis
The defining histologic feature is portal lymphocytic or lymphoplasmacytic inflammation with fibrosis
- Inflammatory cells cross the limiting plate → interface hepatitis (periportal hepatocyte injury)
- Fibrosis progression:
- Portal/periportal fibrosis →
- Fibrous septa with portoportal bridging fibrosis →
- Cirrhosis (end stage)
Virus-Specific Histologic Clues:
| Feature | Virus |
|---|---|
| "Ground-glass" hepatocytes (ER swollen with HBsAg) | Chronic HBV (confirmed by immunostaining) |
| Large lymphoid aggregates in portal tracts | Chronic HCV |
| Steatosis (fatty change in scattered hepatocytes) | Chronic HCV |
| Bile duct injury mimicking primary biliary cholangitis | Chronic HCV |
Clinicopathologic Syndromes
- Acute asymptomatic infection - elevated transaminases or antiviral antibodies found incidentally
- Acute symptomatic infection - incubation → preicteric phase (malaise, nausea, RUQ discomfort) → icteric phase (jaundice) → convalescence
- Acute liver failure (fulminant hepatitis) - massive hepatic necrosis; viral hepatitis = ~10% of cases; HAV most common worldwide; HBV more common in Asia/Mediterranean
- Chronic hepatitis - defined as symptomatic, biochemical, or serologic evidence of hepatic disease for >6 months; may progress to cirrhosis and HCC
- Carrier state - harbor and transmit virus without symptoms (HBV, HCV, HDV)
Autoimmune Hepatitis
- Chronic, progressive; female predominance (78%)
- Associated with HLA-DR3/DR4 in type 1
- Type 1: ANA + anti-smooth muscle antibody (ASMA, 65%) + anti-SLA/LP (25-35%) - most common form
- Type 2: Anti-LKM-1 + anti-LC1 + anti-SLA/LP - children/teenagers
- Up to 30% of adult-onset cases already have cirrhosis at diagnosis
Morphology of Autoimmune Hepatitis:
- Interface hepatitis or confluent (perivenular/bridging) necrosis
- Plasma cell predominance in the inflammatory infiltrate (distinguishes from viral hepatitis)
- Hepatocyte "rosettes" - circular arrangement of regenerating hepatocytes around dilated canaliculi
- Responds well to immunosuppression (90% remission rate)
Autoimmune hepatitis - H&E showing lobular hepatitis with prominent plasma cells:
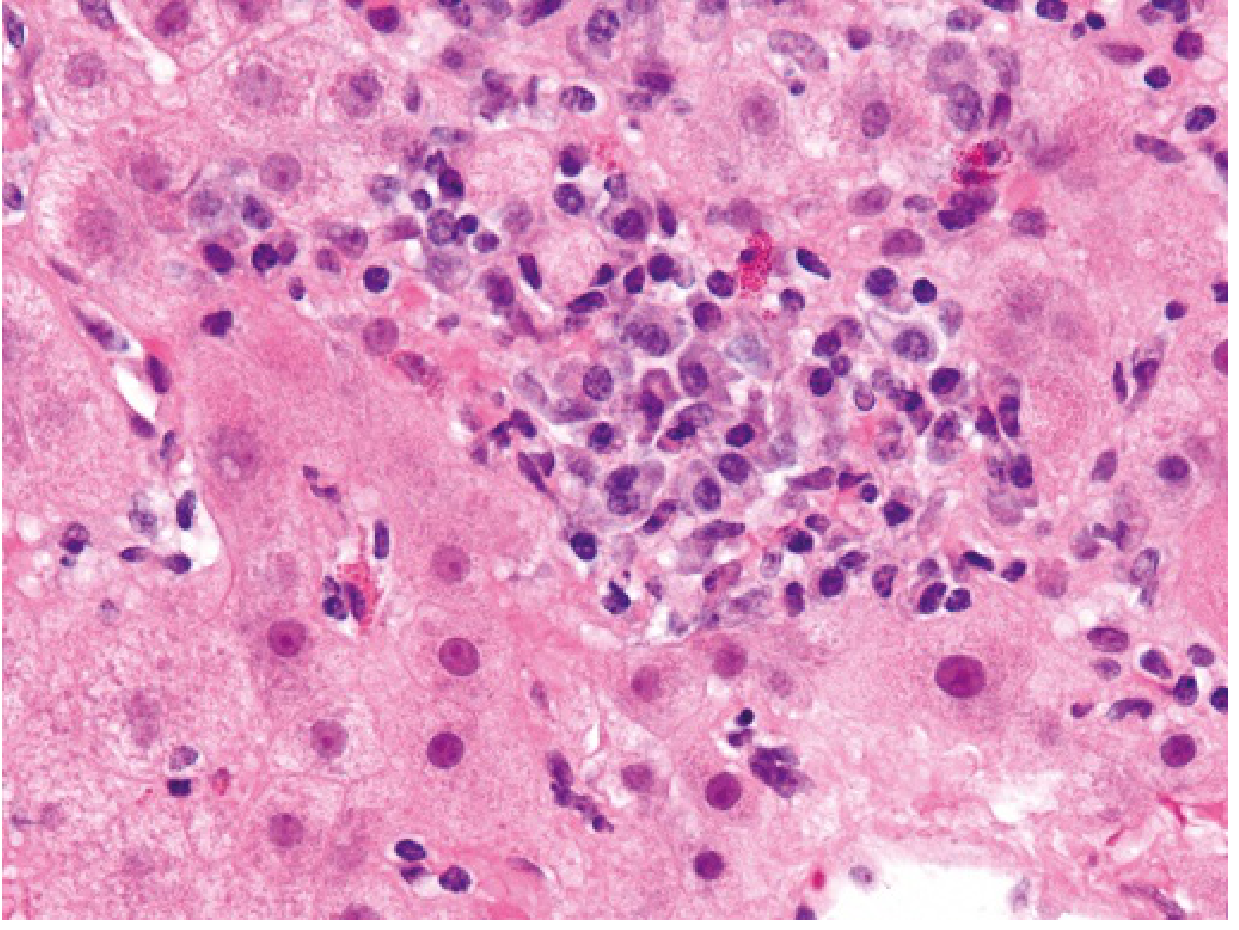
Dense mononuclear infiltrate with numerous plasma cells is the hallmark. Note the disruption of the hepatic parenchyma.
Key Complications
| Complication | Associated Viruses |
|---|---|
| Cirrhosis | HBV, HCV, HDV |
| Hepatocellular carcinoma (HCC) | HBV (via HBx protein + integration), HCV |
| Cryoglobulinemia | HCV (~35%) |
| Membranoproliferative GN | HBV (immune complex), HCV |
| Vasculitis | HBV, HCV |
| Acute liver failure | HAV (rare), HBV+HDV, HEV (in pregnancy) |
Sources: Robbins & Kumar Basic Pathology (9780323790185), pp. 600-607 | Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
Describe Hurqatul Baul (burning micturition) and enlist its causes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
I have all the content needed for a thorough answer. Let me compile it now.
Hurqatul Baul (حرقة البول) - Burning Micturition / Dysuria
Definition
Hurqatul Baul (Arabic/Urdu: حرقة البول, literally "burning of urine") is the traditional Unani/Islamic medicine term for dysuria - painful or burning urination. It refers to any discomfort, burning, stinging, or pain experienced during or immediately after passing urine.
In clinical terms, it is defined as a symptom of pain, discomfort, or burning sensation localized to the urethra or bladder during the act of micturition.
Description
Location of Pain
The character and site of pain give important diagnostic clues:
- In men: Pain is typically felt in the distal urethra; it is present only with voiding and disappears soon after micturition is completed
- In women: Pain is usually localized to the urethra or vulva
- Suprapubic pain at the end of voiding suggests bladder inflammation (cystitis)
- Pain at the beginning of urination typically points to urethral pathology
- Pain throughout voiding suggests involvement of both the bladder and urethra
Types of Dysuria
Clinically, dysuria is classified into two important types based on origin:
| Type | Description | Common Cause |
|---|---|---|
| Internal dysuria | Pain felt inside (deep, suprapubic) | UTI, urethritis (STI) |
| External dysuria | Pain felt at the urethral meatus or vulva, often on contact with urine | Vaginitis, vulvitis, herpes |
Associated Symptoms
Dysuria rarely occurs alone. Common accompanying features:
- Frequency - voiding small volumes repeatedly
- Urgency - sudden, strong urge to void
- Hematuria - blood in urine (present in ~50% of UTI cases)
- Suprapubic discomfort
- Vaginal discharge / pruritus - suggests vaginitis rather than UTI
- Fever, chills, flank pain - suggest upper UTI (pyelonephritis) or prostatitis
- Purulent urethral discharge - suggests STI (gonorrhea, chlamydia)
Clinical Significance
- Dysuria significantly increases the probability of UTI
- In women with dysuria + frequency without vaginal discharge, probability of cystitis is >90%
- Dysuria with vaginal discharge or odor lowers the likelihood of UTI and raises suspicion for vaginitis or STI
- Empirical treatment based on dysuria alone leads to unnecessary antibiotic use - other symptoms must be incorporated
Causes of Hurqatul Baul (Burning Micturition)
I. Infective Causes (Most Common)
A. Lower Urinary Tract Infections (UTI / Cystitis)
- The most common cause overall
- Pathogens: E. coli (~75%), Klebsiella pneumoniae, Proteus mirabilis, Staphylococcus saprophyticus, Enterococcus
- More common in women (short urethra), pregnant women, diabetics, elderly, patients with indwelling catheters
- Presents with internal dysuria + frequency + urgency + suprapubic pain
B. Upper UTI - Pyelonephritis
- Ascending infection reaching the kidney
- Dysuria with fever, chills, flank pain, costovertebral angle tenderness, nausea/vomiting
- Elderly may present atypically with confusion, lethargy
C. Urethritis
- Gonococcal urethritis (Neisseria gonorrhoeae): purulent discharge + dysuria; abrupt onset
- Non-gonococcal urethritis (NGU) (Chlamydia trachomatis, Ureaplasma urealyticum): scant mucoid discharge; may be asymptomatic; gradual onset
- History of new/multiple sexual partners is a key clue
- More common in young, sexually active individuals
D. Vaginitis (in women)
Causes external dysuria (urine contacts inflamed vulva):
- Bacterial vaginosis (Gardnerella vaginalis): fishy odor, grey discharge
- Candidal vaginitis (Candida albicans): white cottage-cheese discharge, intense pruritus
- Trichomoniasis (Trichomonas vaginalis): frothy, greenish-yellow, malodorous discharge; dysuria + dyspareunia
E. Prostatitis (in men)
- Acute bacterial prostatitis: fever, chills, perineal pain, dysuria, difficulty voiding; exquisitely tender prostate on DRE
- Chronic prostatitis/pelvic pain syndrome: recurrent dysuria, pelvic discomfort
F. Herpes Simplex Virus (HSV)
- Genital HSV (HSV-2 usually) causes painful vesicles/ulcers on genitalia
- Dysuria is severe, particularly external; associated with inguinal lymphadenopathy
G. Other Infections
- Epididymitis/Orchitis (Chlamydia, Gonorrhea in young men; E. coli in older men)
- Tuberculosis of the urinary tract - chronic dysuria, sterile pyuria, frequency
- Schistosomiasis (S. haematobium) - terminal hematuria + dysuria
II. Non-Infective Inflammatory Causes
| Cause | Notes |
|---|---|
| Interstitial cystitis | Chronic bladder pain syndrome; sterile urine; mainly women |
| Radiation cystitis | After pelvic radiotherapy |
| Chemical/allergic cystitis | Spermicides, douches, soaps, bubble baths, latex condoms |
| Drug-induced cystitis | Cyclophosphamide (hemorrhagic cystitis), NSAIDs |
| Vulvitis / Vulvar conditions | Lichen sclerosus, contact dermatitis, atrophic vaginitis |
III. Obstructive / Structural Causes
| Cause | Notes |
|---|---|
| Urinary calculi (kidney/ureteral/bladder stones) | Stone irritates mucosa; colicky pain + hematuria |
| Benign prostatic hyperplasia (BPH) | Older men; obstructive + irritative symptoms |
| Meatal stenosis | Narrowing of urethral meatus; congenital or acquired |
| Urethral stricture | Post-traumatic, post-inflammatory; hesitancy + weak stream + dysuria |
| Urethral diverticulum (women) | Post-void dribbling + recurrent UTI + dysuria |
| Bladder neck contracture | Post-surgical; obstruction → secondary inflammation |
IV. Neoplastic Causes
| Cause | Notes |
|---|---|
| Bladder carcinoma | Painless hematuria + dysuria; transitional cell carcinoma most common |
| Prostate carcinoma | Advanced disease causing obstruction and inflammation |
| Penile carcinoma | Dysuria + local lesion |
| Vulvovaginal neoplasms | Rare but important to exclude |
V. Other / Miscellaneous Causes
- Psychogenic / functional dysuria - no organic cause found; associated with anxiety
- Urethral syndrome - predominantly in women; internal dysuria + pyuria with negative culture; caused by subclinical infections or pelvic floor dysfunction
- Radiation proctitis/cystitis - pelvic radiation effects
- Reactive arthritis (Reiter's syndrome) - triad of urethritis + arthritis + conjunctivitis; sterile dysuria
- Behcet's disease - genital ulcers + dysuria
- Atrophic urethritis/vaginitis - post-menopausal women; decreased estrogen → thin mucosa → burning
Summary of Causes (Quick Reference)
HURQATUL BAUL - CAUSES
INFECTIVE
├── Bacterial UTI (cystitis) ← most common
├── Pyelonephritis
├── Urethritis (gonococcal / non-gonococcal)
├── Vaginitis (bacterial, candidal, trichomonal)
├── Prostatitis (acute / chronic)
├── Herpes genitalis (HSV)
└── Others: TB, Schistosomiasis, Epididymitis
INFLAMMATORY (non-infective)
├── Interstitial cystitis
├── Radiation cystitis
├── Chemical/drug-induced cystitis
└── Vulvitis / atrophic vaginitis
OBSTRUCTIVE / STRUCTURAL
├── Urinary calculi
├── BPH
├── Meatal stenosis / urethral stricture
└── Urethral diverticulum
NEOPLASTIC
├── Bladder carcinoma
├── Prostate carcinoma
└── Vulvovaginal neoplasms
OTHERS
├── Psychogenic
├── Reactive arthritis
└── Behcet's disease
Diagnostic Approach (Brief)
- History: onset (sudden vs. gradual), discharge, sexual history, medication use, hygiene products
- Urinalysis: leukocyte esterase + nitrite dipstick; microscopy (pyuria = ≥10 WBC/mm³)
- Urine culture: midstream clean-catch specimen
- STI screen: NAAT for Chlamydia and Gonorrhea if risk factors present
- Pelvic exam in women: assess for vaginitis, cervicitis
- Imaging (USG/CT): if stones, obstruction, or pyelonephritis suspected
- Cystoscopy: if hematuria, recurrent symptoms, or malignancy suspected
Sources: Smith and Tanagho's General Urology 19e, p. 49 | Textbook of Family Medicine 9e, p. (Table 40-3) | Rosen's Emergency Medicine, Table 85.1 | Harrison's Principles of Internal Medicine 22e
Antihelminthic drug modern pharmacology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Anthelmintic Drugs - Modern Pharmacology
Sources: Katzung's Basic and Clinical Pharmacology 16e (Ch. 53) | Goodman & Gilman's Pharmacological Basis of Therapeutics | Lippincott Illustrated Reviews: Pharmacology
Overview
Helminths (worms) are multicellular invertebrates classified into three major groups:
| Group | Examples |
|---|---|
| Nematodes (roundworms) | Ascaris, hookworms, pinworms, Strongyloides, filarial worms |
| Trematodes (flukes) | Schistosoma, Fasciola, Clonorchis, Paragonimus |
| Cestodes (tapeworms) | Taenia solium/saginata, Echinococcus, Diphyllobothrium |
Anthelmintic drugs target metabolic pathways present in parasites but absent from or different in the host. More than 1 billion people are infected with intestinal nematodes worldwide. The WHO estimated 1.24 billion people received anthelmintic drugs through mass drug administration (MDA) programs in 2019 alone.
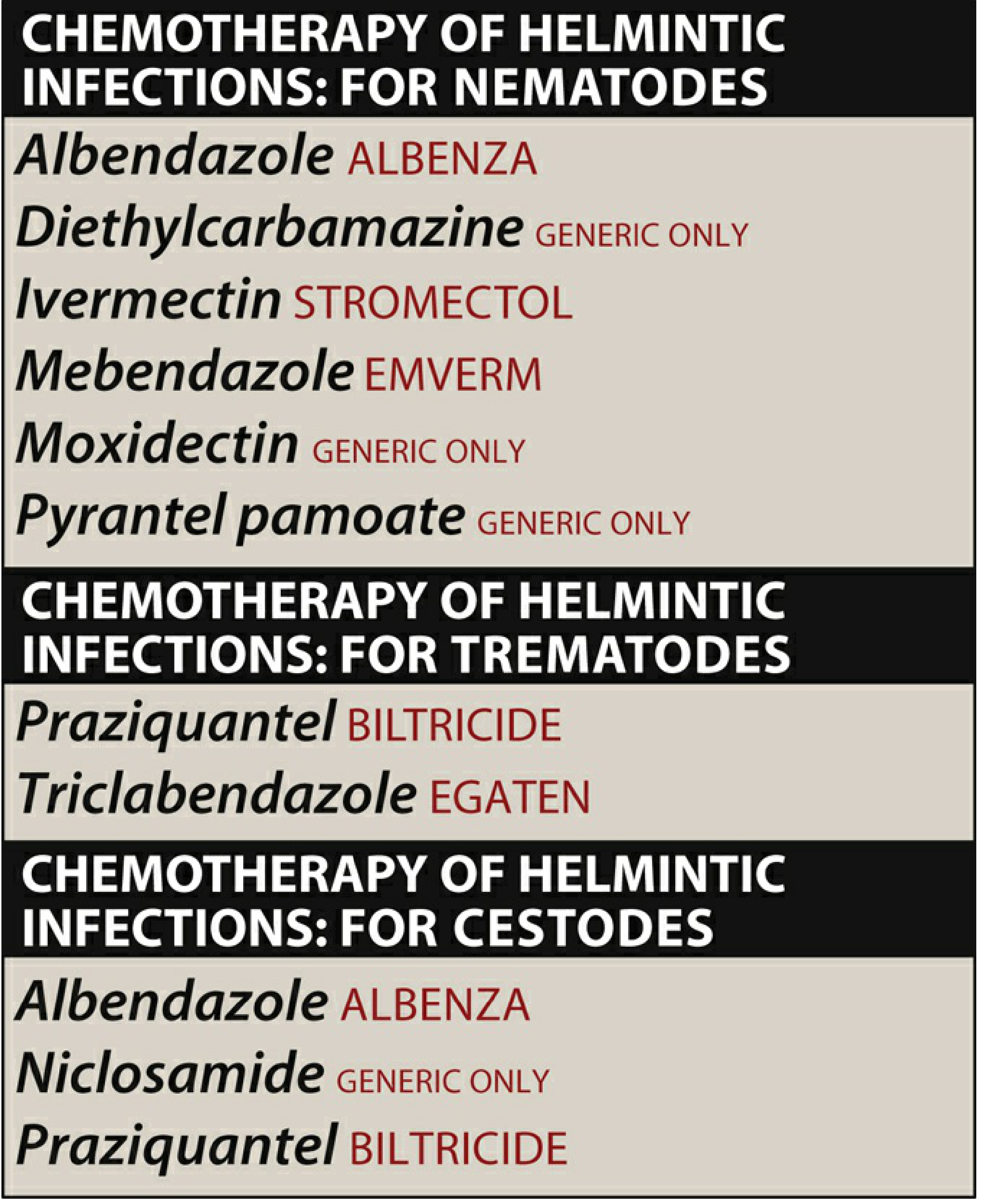
Summary of Anthelmintic Agents by Class:
Drug of Choice by Organism (Katzung Table 53-1)
Nematodes
| Organism | Drug of Choice | Alternatives |
|---|---|---|
| Ascaris lumbricoides | Albendazole or Pyrantel pamoate or Mebendazole | Ivermectin, Piperazine |
| Trichuris trichiura (whipworm) | Mebendazole or Albendazole | Ivermectin, Oxantel pamoate |
| Hookworm (Necator, Ancylostoma) | Albendazole or Mebendazole or Pyrantel pamoate | - |
| Strongyloides stercoralis | Ivermectin | Albendazole, Thiabendazole |
| Enterobius vermicularis (pinworm) | Mebendazole or Pyrantel pamoate | Albendazole |
| Trichinella spiralis | Mebendazole or Albendazole + corticosteroids | - |
| Wuchereria bancrofti / Brugia (filariasis) | Diethylcarbamazine (DEC) | Ivermectin + Albendazole |
| Onchocerca volvulus (river blindness) | Ivermectin | - |
| Loa loa | DEC | - |
Trematodes (Flukes)
| Organism | Drug of Choice | Alternatives |
|---|---|---|
| Schistosoma (all species) | Praziquantel | Oxamniquine (S. mansoni), Metrifonate (S. haematobium) |
| Fasciola hepatica (sheep liver fluke) | Triclabendazole | Bithionol |
| Clonorchis sinensis / Opisthorchis | Praziquantel | Albendazole |
| Paragonimus westermani (lung fluke) | Praziquantel | Bithionol |
| Fasciolopsis buski | Praziquantel or Niclosamide | - |
Cestodes (Tapeworms)
| Organism | Drug of Choice | Alternatives |
|---|---|---|
| Taenia saginata / solium | Praziquantel or Niclosamide | Mebendazole |
| Cysticercosis (larval T. solium) | Albendazole | Praziquantel |
| Echinococcus (hydatid disease) | Albendazole | Surgery |
| Hymenolepis nana (dwarf tapeworm) | Praziquantel | Niclosamide |
| Diphyllobothrium latum (fish tapeworm) | Praziquantel or Niclosamide | - |
Individual Drug Profiles
1. BENZIMIDAZOLES
A. Albendazole
| Feature | Details |
|---|---|
| Class | Benzimidazole carbamate |
| Mechanism | Binds to parasite β-tubulin → inhibits microtubule polymerization → impairs glucose uptake and cellular transport → parasite death |
| Spectrum | Broad: intestinal nematodes, cysticercosis, hydatid disease, some trematodes |
| Pharmacokinetics | Erratically absorbed orally; absorption increased by fatty meal; undergoes first-pass metabolism in liver to active metabolite - albendazole sulfoxide; half-life 8-12 hours; sulfoxide is highly protein-bound and distributed to tissues including CNS, bile, and CSF |
| Clinical uses | Hydatid disease (drug of choice), neurocysticercosis (drug of choice), ascariasis, pinworm, hookworm, trichuriasis, strongyloidiasis, filariasis (combination therapy) |
| Dosing | 400 mg once (intestinal nematodes); 400 mg BID × 28 days (hydatid/cysticercosis) |
| Adverse effects | Short courses: headache, nausea (mild/transient). Long courses: hepatotoxicity, agranulocytosis, pancytopenia - monitor LFTs and CBC every 2 weeks. Neurocysticercosis: headache, vomiting, fever, seizures (inflammatory response to dying parasites) |
| Contraindications | Pregnancy (teratogenic in animals); cirrhosis (caution) |
B. Mebendazole
| Feature | Details |
|---|---|
| Class | Synthetic benzimidazole |
| Mechanism | Binds to parasite β-tubulin → inhibits microtubule synthesis and polymerization → impairs glucose and nutrient uptake; parent drug is the active form; also kills helminth eggs |
| Spectrum | Whipworm, pinworm, hookworm, roundworm (Ascaris); drug of choice for trichuriasis |
| Pharmacokinetics | Poorly absorbed orally (~5-10%); tablets should be chewed; efficacy varies with GI transit time and infection intensity |
| Clinical uses | Pinworm (100 mg once, repeat in 2 weeks); Ascariasis, hookworm, trichuriasis (100 mg BID × 3 days); Intestinal capillariasis (200 mg BID × 21 days) |
| Adverse effects | Short courses: minimal - abdominal pain, diarrhea. High-dose: hypersensitivity (rash, urticaria), agranulocytosis, alopecia, elevated LFTs |
| Contraindications | Pregnancy (teratogenic); caution in children <2 years (rare convulsions); levels reduced by carbamazepine, phenytoin, ritonavir |
C. Triclabendazole
| Feature | Details |
|---|---|
| Class | Benzimidazole derivative |
| Mechanism | Inhibits tubulin function + protein and enzyme synthesis in parasite |
| Spectrum | Narrow: Fasciola hepatica and F. gigantica only (fascioliasis) |
| Clinical uses | Drug of choice for fascioliasis (liver fluke) |
| Adverse effects | Abdominal pain, hyperhidrosis (sweating), nausea |
| Contraindications | Caution in pregnancy (limited data) |
D. Thiabendazole
- Older benzimidazole; largely replaced by ivermectin/albendazole
- Alternative for strongyloidiasis and cutaneous larva migrans
- Rapidly absorbed; chelating agent (forms complexes with metals, but not calcium)
- Significant adverse effect profile: nausea, vomiting, dizziness, hepatotoxicity - limits use
2. MACROCYCLIC LACTONES
A. Ivermectin
| Feature | Details |
|---|---|
| Class | Macrocyclic lactone (avermectin derivative) |
| Mechanism | Selectively binds to glutamate-gated chloride channels (GluCl) in invertebrate nerve and muscle cells → enhances chloride ion influx → hyperpolarization → spastic paralysis and death of parasite. Does NOT readily cross the blood-brain barrier in humans (P-glycoprotein efflux) |
| Spectrum | Strongyloides (drug of choice), Onchocerca (microfilariae - not curative of adult worms), cutaneous larva migrans, lymphatic filariasis (combination), scabies, pediculosis (lice) |
| Pharmacokinetics | Well absorbed orally; does not cross BBB (P-gp efflux); metabolized in liver; excreted mainly in feces |
| Clinical uses | Strongyloidiasis (200 mcg/kg × 1-2 days); Onchocerciasis (150 mcg/kg annually); Lymphatic filariasis (triple therapy: IVM + DEC + albendazole - superior efficacy) |
| Adverse effects | Generally well-tolerated. In onchocerciasis: Mazzotti reaction - fever, headache, dizziness, somnolence, hypotension (due to microfilarial killing; severity proportional to parasite load; treat with antihistamines/steroids) |
| Contraindications | Pregnancy; caution in patients with Loa loa high microfilarial loads (risk of encephalopathy); children <15 kg |
| Special note | Also active against ectoparasites (scabies, head lice - topical formulation) |
B. Moxidectin
- Newer macrocyclic lactone; similar mechanism to ivermectin (GluCl channel agonist)
- FDA-approved (2018) for onchocerciasis in patients ≥12 years
- Longer half-life than ivermectin; single-dose efficacy
- Being evaluated for lymphatic filariasis and other nematode infections
3. PRAZIQUANTEL
| Feature | Details |
|---|---|
| Class | Isoquinoline-pyrazine compound |
| Mechanism | Increases membrane permeability to calcium ions → massive calcium influx → contracture and spastic paralysis of the worm's musculature → tegument disruption → exposure to host immune attack → worm death |
| Spectrum | All species of Schistosoma; most trematodes (except Fasciola); intestinal and tissue cestodes (Taenia, Diphyllobothrium, Hymenolepis, Echinococcus) |
| Pharmacokinetics | Rapidly absorbed orally; should be taken with food; extensively metabolized in liver (first-pass); inactive metabolites excreted mainly in urine |
| Clinical uses | Drug of choice for schistosomiasis (all species); Taeniasis; fish and pork tapeworm; Hymenolepis nana; liver/lung/intestinal flukes; alternative for neurocysticercosis |
| Adverse effects | Dizziness, malaise, headache, abdominal cramps, nausea/vomiting; in neurocysticercosis: inflammatory reactions in CNS |
| Drug interactions | CYP3A4 inducers (phenytoin, rifampin, carbamazepine) increase praziquantel metabolism → reduce efficacy; concomitant use contraindicated |
| Contraindications | Ocular cysticercosis (destruction of parasite in the eye → irreversible damage); caution in pregnancy |
4. DIETHYLCARBAMAZINE (DEC)
| Feature | Details |
|---|---|
| Class | Synthetic piperazine derivative |
| Mechanism | Immobilizes microfilariae and alters their surface structure → displaces them from tissues → enhanced susceptibility to host immune destruction. Mechanism against adult worms: unknown |
| Spectrum | Lymphatic filariasis (W. bancrofti, B. malayi, B. timori), loiasis (L. loa), tropical pulmonary eosinophilia |
| Pharmacokinetics | Rapidly absorbed orally; peak plasma levels in 1-2 hours; half-life 2-3 hours (acidic urine) or ~10 hours (alkaline urine - Henderson-Hasselbalch trapping); distributed to all tissues except fat; excreted in urine; dose reduce in renal impairment |
| Clinical uses | Lymphatic filariasis: 2 mg/kg TID × 12 days; Loiasis: same regimen × 2-3 weeks; often requires several courses; now used as triple therapy (DEC + ivermectin + albendazole) for superior microfilarial clearance |
| Adverse effects | Mild: headache, malaise, anorexia, nausea. Allergic reactions (antihistamines for first few days). Mazzotti-like reactions with heavy L. loa loads → risk of encephalopathy |
| Contraindications | Onchocerca infections (replaced by ivermectin due to severe Mazzotti reactions); high L. loa microfilarial loads |
5. PYRANTEL PAMOATE
| Feature | Details |
|---|---|
| Class | Tetrahydropyrimidine derivative |
| Mechanism | Depolarizing neuromuscular blocking agent → causes release of acetylcholine AND inhibits cholinesterase → sustained muscle depolarization → spastic paralysis → expulsion from gut. Does NOT affect eggs or migratory tissue stages |
| Spectrum | Pinworm (>95% cure), Ascaris (85-100% cure), hookworm, Trichostrongylus; NOT effective against Trichuris or Strongyloides |
| Pharmacokinetics | Poorly absorbed from GI tract (acts locally on luminal organisms); >50% recovered unchanged in feces; peak plasma levels in 1-3 hours |
| Clinical uses | Pinworm: 11 mg/kg once, repeat at 2 weeks; Ascariasis: single dose; Hookworm: 3-day course for heavy N. americanus infections; available OTC in the USA for pinworm |
| Adverse effects | Mild, transient: nausea, vomiting, diarrhea, abdominal cramps, dizziness; caution in liver disease (transient aminotransferase elevations) |
| Note | Do NOT combine with piperazine (antagonistic mechanisms - piperazine is a flaccid paralytic, pyrantel is spastic) |
6. NICLOSAMIDE
| Feature | Details |
|---|---|
| Class | Salicylanilide derivative |
| Mechanism | Inhibits mitochondrial oxidative phosphorylation (inhibits ADP phosphorylation) in the tapeworm → lethal for the scolex and proglottids; NOT effective against ova |
| Spectrum | Cestodes: Taenia saginata, T. solium, Diphyllobothrium latum, Hymenolepis nana |
| Clinical uses | Alternative to praziquantel for taeniasis; no longer available in the USA |
| Special precaution | A laxative is given prior to use to purge the bowel of dead segments (prevents liberation and hatching of eggs within the gut, which could cause cysticercosis). Alcohol avoided for 24 hours |
| Adverse effects | Minimal: nausea, abdominal discomfort |
7. PIPERAZINE
- Mechanism: Flaccid paralysis of worms (GABA receptor agonist → hyperpolarization of muscle)
- Alternative for Ascaris lumbricoides and Enterobius
- Largely replaced by benzimidazoles in current practice
- Antagonistic with pyrantel (opposing mechanisms - do not combine)
Mechanisms of Action - Summary Table
| Drug | Mechanism | Target |
|---|---|---|
| Albendazole, Mebendazole, Triclabendazole | Bind β-tubulin → inhibit microtubule polymerization | Nematodes, cestodes, Fasciola |
| Ivermectin, Moxidectin | Agonist at glutamate-gated Cl⁻ channels → hyperpolarization → paralysis | Nematodes, ectoparasites |
| Praziquantel | Increase Ca²⁺ permeability → spastic paralysis + tegument disruption | Trematodes, cestodes |
| Diethylcarbamazine | Immobilizes microfilariae, alters surface → immune clearance | Filarial nematodes |
| Pyrantel pamoate | ACh release + cholinesterase inhibition → depolarizing paralysis | Intestinal nematodes |
| Niclosamide | Inhibits mitochondrial oxidative phosphorylation (ADP phosphorylation) | Cestodes |
| Metrifonate | Organophosphate → cholinesterase inhibition → flaccid paralysis | S. haematobium |
| Piperazine | GABA agonist → flaccid paralysis | Ascaris, Enterobius |
Pregnancy Safety
Most anthelmintics should be avoided in pregnancy, particularly in the first trimester:
- Avoid throughout pregnancy: Ivermectin, Thiabendazole, Piperazine
- Avoid in first trimester (may use 2nd/3rd in MDA programs): Mebendazole, Albendazole
- Caution: Praziquantel, Triclabendazole (limited data)
- DEC - avoid in pregnancy; associated with adverse fetal effects
Special Clinical Scenarios
- Neurocysticercosis: Albendazole (preferred) + corticosteroids to reduce inflammatory edema around dying parasites
- Hydatid disease (Echinococcus): Albendazole + surgical/PAIR procedure; must monitor LFTs/CBC
- Hyperinfection strongyloidiasis (in immunocompromised/HTLV-1/steroid users): Ivermectin urgently; mortality up to 90% untreated
- Lymphatic filariasis MDA: Triple therapy - DEC + Ivermectin + Albendazole (superior efficacy)
- Ocular cysticercosis: Praziquantel contraindicated; albendazole with caution; surgical management preferred
Sources: Katzung's Basic and Clinical Pharmacology 16e, Ch. 53 (pp. 1460-1471) | Lippincott Illustrated Reviews: Pharmacology, Ch. 36 (pp. 1194-1204) | Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 68
Antiviral drug modern pharmacology reference
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have extensive content from Katzung covering all major antiviral drug classes. I have enough comprehensive information to write a thorough, well-structured answer. Let me compile the full pharmacology reference now.
Antiviral Drugs - Modern Pharmacology
Primary reference: Katzung's Basic and Clinical Pharmacology, 16th Edition (Chapter 49)
Principle: Sites of Action
Viruses are obligate intracellular parasites - their replication depends on host cell synthetic processes. All antiviral drugs are virustatic (active only against replicating viruses, not latent virus). They target specific steps in the viral life cycle:
Fig 49-1 - Major Sites of Antiviral Drug Action:
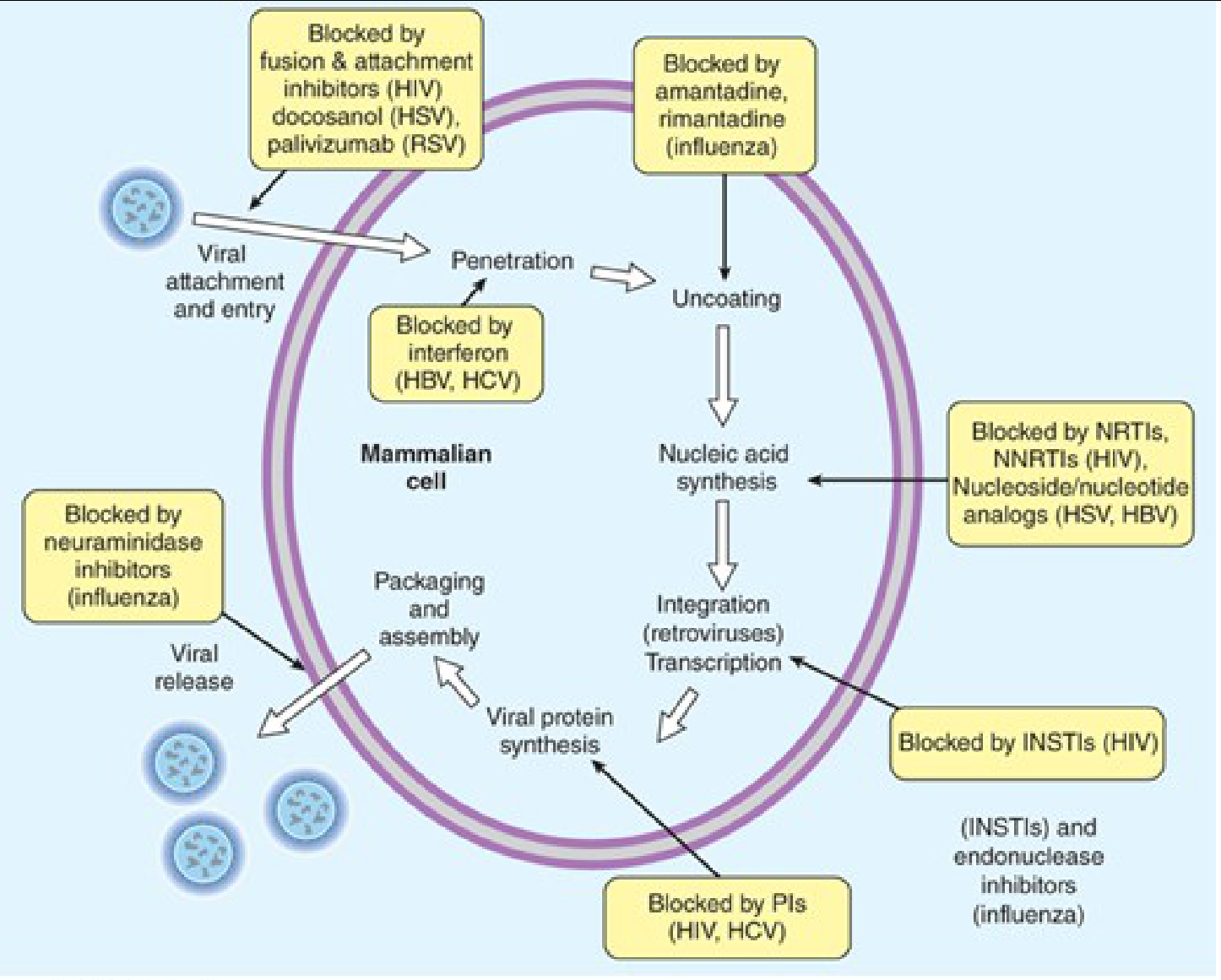
Key steps targeted: Attachment/entry → Uncoating → Nucleic acid synthesis → Integration → Viral protein synthesis → Packaging/release
Classification of Antiviral Drugs
ANTIVIRAL DRUGS
│
├── ANTI-HERPESVIRUS AGENTS
│ ├── Nucleoside Analogs: Acyclovir, Valacyclovir, Famciclovir, Penciclovir
│ ├── Anti-CMV: Ganciclovir, Valganciclovir, Cidofovir, Foscarnet, Letermovir
│ └── Others: Docosanol, Trifluridine (topical)
│
├── ANTI-INFLUENZA AGENTS
│ ├── Neuraminidase Inhibitors: Oseltamivir, Zanamivir, Peramivir
│ ├── Cap-endonuclease Inhibitor: Baloxavir marboxil
│ └── M2 Ion Channel Blockers: Amantadine, Rimantadine (Influenza A only)
│
├── ANTI-HIV (ANTIRETROVIRAL) AGENTS
│ ├── NRTIs: Zidovudine, Tenofovir, Emtricitabine, Lamivudine, Abacavir, Stavudine
│ ├── NNRTIs: Efavirenz, Nevirapine, Rilpivirine, Doravirine, Etravirine
│ ├── Protease Inhibitors: Ritonavir, Darunavir, Atazanavir, Lopinavir, Saquinavir
│ ├── INSTIs: Raltegravir, Elvitegravir, Dolutegravir, Bictegravir, Cabotegravir
│ ├── Entry/Fusion Inhibitors: Enfuvirtide, Maraviroc
│ └── Pharmacokinetic Booster: Cobicistat, Ritonavir
│
├── ANTI-HBV AGENTS
│ ├── Nucleoside Analogs: Entecavir, Tenofovir, Lamivudine, Adefovir, Telbivudine
│ └── Interferon: Pegylated IFN-α2a/2b
│
├── ANTI-HCV (DAA) AGENTS
│ ├── NS5B Polymerase Inhibitors: Sofosbuvir
│ ├── NS5A Inhibitors: Ledipasvir, Velpatasvir, Pibrentasvir
│ └── NS3/4A Protease Inhibitors: Glecaprevir, Grazoprevir, Simeprevir
│
├── ANTI-RSV AGENTS
│ └── Palivizumab, Nirsevimab (monoclonal antibodies); Ribavirin
│
└── BROAD-SPECTRUM
└── Ribavirin, Interferons
I. ANTI-HERPESVIRUS AGENTS
A. Acyclovir
| Feature | Details |
|---|---|
| Class | Acyclic guanosine nucleoside analog |
| Mechanism | Requires 3-step activation: (1) Viral thymidine kinase (TK) phosphorylates acyclovir → acyclovir monophosphate; (2) cellular kinases convert to triphosphate; (3) Acyclovir-TP competitively inhibits viral DNA polymerase AND acts as an obligate chain terminator (lacks 3'-OH group → DNA chain elongation stops). Highly selective - depends on viral TK for first phosphorylation step |
| Spectrum | HSV-1, HSV-2, VZV (less potent); EBV, CMV (minimal) |
| Pharmacokinetics | Oral bioavailability 15-30% (poor); IV for severe infections; eliminated by renal tubular secretion; dose-adjust in renal impairment; penetrates CNS |
| Clinical uses | Genital herpes (first episode, recurrence, suppression); herpes encephalitis (IV 10 mg/kg q8h × 14-21 days); neonatal HSV (IV 20 mg/kg q8h × 21 days); herpes labialis; herpes keratitis (topical); VZV (higher doses required) |
| Adverse effects | Oral: nausea, headache. IV: nephrotoxicity (crystalline nephropathy - must hydrate well), neurotoxicity (tremor, confusion) at high doses; not myelosuppressive |
| Resistance | Mutations in viral TK (most common) or viral DNA polymerase; TK-deficient strains treated with foscarnet or cidofovir |
B. Valacyclovir
- L-valine ester prodrug of acyclovir; oral bioavailability 54% (vs 15-30% for acyclovir)
- Converted to acyclovir by intestinal/hepatic valacyclovirase after absorption
- Same mechanism, spectrum, and adverse effects as acyclovir; allows less frequent dosing
- Preferred over acyclovir for most oral HSV/VZV indications
C. Famciclovir / Penciclovir
- Famciclovir = oral prodrug of penciclovir (diacetyl ester); oral bioavailability ~77%
- Mechanism: same as acyclovir (viral TK activation → DNA polymerase inhibition/chain termination)
- Unlike acyclovir, penciclovir-TP does NOT act as obligate chain terminator but has a longer intracellular half-life (10-20 hours)
- Clinical uses: genital HSV, herpes labialis (1500 mg single dose), herpes zoster
- Penciclovir is also available topically for herpes labialis
D. Ganciclovir / Valganciclovir
| Feature | Details |
|---|---|
| Class | Acyclic guanosine nucleoside analog (similar to acyclovir) |
| Mechanism | Phosphorylated by CMV-encoded UL97 kinase (CMV lacks thymidine kinase) → ganciclovir triphosphate → inhibits CMV DNA polymerase (UL54); also acts as chain terminator |
| Spectrum | CMV (primary indication), also HSV, VZV, EBV |
| Pharmacokinetics | Ganciclovir IV only (oral bioavailability 6-9%). Valganciclovir = oral prodrug with 60% bioavailability; converted to ganciclovir. Eliminated renally; dose-reduce in renal impairment |
| Clinical uses | CMV retinitis (induction + maintenance in AIDS), CMV disease in transplant patients, CMV prophylaxis, CMV esophagitis/colitis |
| Adverse effects | Myelosuppression (neutropenia, thrombocytopenia) - major dose-limiting toxicity; monitor CBC weekly; nephrotoxicity; CNS effects; teratogenic and gonadotoxic |
| Resistance | Mutations in UL97 (most common) or UL54 (DNA polymerase) |
E. Cidofovir
| Feature | Details |
|---|---|
| Class | Acyclic nucleoside phosphonate (monophosphate already attached) |
| Mechanism | Does not require viral kinase for initial phosphorylation (already a nucleotide) → cellular kinases convert to cidofovir diphosphate → potently inhibits viral DNA polymerase; very long intracellular half-life (allows infrequent dosing) |
| Spectrum | CMV, acyclovir-resistant HSV, adenovirus, smallpox, BK virus |
| Pharmacokinetics | IV only; eliminated by renal tubular secretion; long intracellular half-life (17-65 hours) |
| Clinical uses | CMV retinitis in AIDS (when ganciclovir fails); acyclovir/foscarnet-resistant HSV; adenovirus infection in transplant patients |
| Adverse effects | Nephrotoxicity (major - dose-limiting; must prehydrate with IV saline + give probenecid to block tubular secretion); neutropenia; ocular hypotony; potential carcinogenicity |
| Administration | Always given with probenecid + IV saline prehydration |
F. Foscarnet (Phosphonoformate)
| Feature | Details |
|---|---|
| Class | Inorganic pyrophosphate analog |
| Mechanism | Does NOT require intracellular phosphorylation; directly inhibits viral DNA polymerase (and HIV reverse transcriptase) at the pyrophosphate binding site → blocks pyrophosphate release → DNA chain elongation stops. Active against TK-deficient (acyclovir-resistant) herpesvirus |
| Spectrum | CMV, acyclovir-resistant HSV/VZV, HBV, HIV |
| Pharmacokinetics | IV only; 10-28% deposited in bone (long-term sequestration); renal elimination |
| Clinical uses | CMV retinitis; acyclovir/ganciclovir-resistant CMV, HSV, VZV; used in immunocompromised patients |
| Adverse effects | Nephrotoxicity (major - must hydrate); electrolyte disturbances (hypocalcemia, hypomagnesemia, hypokalemia, hypophosphatemia - can cause seizures, cardiac arrhythmias); penile/vulvar ulcers (local irritation from urinary excretion); anemia |
G. Letermovir
- Novel anti-CMV drug targeting CMV terminase complex (UL56 subunit) - completely different mechanism from ganciclovir/foscarnet/cidofovir
- Active against ganciclovir-resistant CMV
- Approved for CMV prophylaxis in CMV-seropositive hematopoietic stem cell transplant recipients
- Adverse effects: nausea, diarrhea, edema; CYP3A4 interactions
II. ANTI-INFLUENZA AGENTS
A. Neuraminidase Inhibitors (first-line)
| Drug | Route | Mechanism | Uses |
|---|---|---|---|
| Oseltamivir (Tamiflu) | Oral (prodrug → carboxylate) | Competitively inhibits viral neuraminidase → prevents cleavage of sialic acid from host cell receptors → virions remain aggregated, cannot spread | Influenza A & B treatment (within 48h onset) and prophylaxis |
| Zanamivir (Relenza) | Inhaled powder | Same mechanism | Influenza A & B; caution in asthma/COPD (bronchospasm) |
| Peramivir (Rapivab) | IV | Same mechanism | Severe/hospitalized influenza |
- Resistance: H275Y mutation in neuraminidase (common in H1N1); use baloxavir as alternative
- Key points: Must begin within 48 hours of symptom onset for maximum benefit; reduce duration of illness by ~1-1.5 days; also reduce complications
B. Baloxavir Marboxil (Xofluza)
- Mechanism: Inhibits cap-dependent endonuclease (PA subunit of viral RNA polymerase complex) → blocks initiation of viral mRNA transcription ("cap snatching") - novel mechanism
- Active against Influenza A and B, including strains resistant to neuraminidase inhibitors
- Single oral dose; prodrug converted to active baloxavir acid
- Adverse effects: diarrhea, headache; should not combine with polyvalent cation-containing products (dairy, antacids) - reduce absorption
C. M2 Ion Channel Blockers (largely obsolete)
- Amantadine, Rimantadine
- Mechanism: Block M2 ion channel of Influenza A → prevent viral uncoating
- Active only against Influenza A (Influenza B lacks M2 protein)
- Nearly 100% resistance among circulating H3N2 and H1N1 strains - no longer recommended for treatment/prophylaxis
- Amantadine also used in Parkinson's disease (dopaminergic effect)
- Adverse effects: CNS (confusion, insomnia, hallucinations - more with amantadine), GI
III. ANTIRETROVIRAL (HIV) AGENTS
HIV treatment requires combination antiretroviral therapy (cART) - typically 2 NRTIs + 1 INSTI (preferred backbone). Treatment is lifelong.
A. Nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NRTIs)
Mechanism (class): Prodrugs requiring intracellular phosphorylation to active triphosphate form → competitively inhibit HIV reverse transcriptase AND act as obligate chain terminators (lack 3'-OH) → prevent synthesis of viral DNA from RNA template
| Drug | Key Features | Adverse Effects |
|---|---|---|
| Zidovudine (AZT) | First HIV drug (1987); thymidine analog; good CNS penetration; used in PMTCT | Myelosuppression (anemia, neutropenia), mitochondrial toxicity, lipoatrophy, lactic acidosis |
| Tenofovir DF (TDF) | Nucleotide (already monophosphate); active against HIV + HBV; backbone of most regimens | Nephrotoxicity (Fanconi syndrome, proximal tubular injury), decreased bone density |
| Tenofovir AF (TAF) | Newer prodrug of tenofovir; better renal/bone safety profile than TDF at lower dose | Less renal/bone toxicity; weight gain |
| Emtricitabine (FTC) | Fluorinated lamivudine analog; very long intracellular t½ (≥24h → once daily); active vs HIV + HBV; TDF/FTC = PrEP regimen | Headache, diarrhea, rash; hyperpigmentation of palms/soles (especially in African Americans); HBV flare if stopped |
| Lamivudine (3TC) | Active vs HIV + HBV; well tolerated; selects M184V mutation (reduces viral fitness) | Headache, nausea; HBV flare if stopped; do NOT combine with emtricitabine |
| Abacavir (ABC) | Active vs HIV; used in ABC/3TC backbone | HLA-B*5701 hypersensitivity reaction (must screen before use - negative predictive value ~100%); possible ↑ cardiovascular risk; avoid in CAD |
| Stavudine (d4T) | Thymidine analog; largely replaced | Severe lipoatrophy, peripheral neuropathy, lactic acidosis |
B. Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs)
Mechanism (class): Bind to an allosteric hydrophobic pocket adjacent to the HIV-1 reverse transcriptase active site (non-competitive) → conformational change → inhibit RT. Do NOT require intracellular phosphorylation. Active only against HIV-1 (not HIV-2 or HBV)
| Drug | Key Features | Adverse Effects |
|---|---|---|
| Efavirenz (EFV) | Long half-life (40-55h) → once daily; CNS penetration | CNS effects (vivid dreams, dizziness, depression) - worse in first 2-4 weeks; teratogenic (neural tube defects - avoid in first trimester); strong CYP3A4 inducer |
| Nevirapine (NVP) | Older agent; used in PMTCT; can cause hepatitis (especially in women with CD4 >250) | Severe hepatotoxicity (especially first 18 weeks), Stevens-Johnson syndrome/toxic epidermal necrolysis; rash |
| Rilpivirine (RPV) | Second-generation; must take with food (>500 kcal meal) and avoid PPIs; low pill burden | Rash, insomnia, headache; less CNS side effects than efavirenz |
| Doravirine (DOR) | Newest NNRTI; no food restriction; low drug interaction profile; minimal dyslipidemia | Nausea, headache, dizziness |
| Etravirine (ETR) | Active against some NNRTI-resistant strains; twice daily | Rash, nausea |
C. Protease Inhibitors (PIs)
Mechanism (class): Inhibit HIV-1 protease (aspartyl protease) → prevents cleavage of gag-pol polyprotein into mature functional proteins → immature, non-infectious viral particles released
All PIs are CYP3A4 substrates and many are also CYP3A4 inhibitors → extensive drug interactions. Always given with pharmacokinetic booster (ritonavir or cobicistat) to increase plasma levels.
| Drug | Key Features | Adverse Effects |
|---|---|---|
| Ritonavir | Now used primarily as PK booster (low-dose 100-200 mg/day); potent CYP3A4 inhibitor | GI intolerance; numerous drug interactions |
| Darunavir (DRV) | Preferred PI in current guidelines; high barrier to resistance; once or twice daily (with ritonavir/cobicistat) | Rash (sulfonamide moiety - caution in sulfa allergy), hepatotoxicity, dyslipidemia, GI |
| Atazanavir (ATV) | Once daily; does NOT raise LDL; requires gastric acid for absorption (avoid PPIs) | Indirect hyperbilirubinemia (jaundice/scleral icterus without liver damage - UGT1A1 inhibition), nephrolithiasis, PR prolongation |
| Lopinavir/r (LPV/r) | Co-formulated with ritonavir; older agent | Dyslipidemia, GI, QT prolongation |
| Class adverse effects | Dyslipidemia (↑LDL, ↑TG), lipodystrophy (peripheral fat loss + central fat accumulation), insulin resistance/hyperglycemia, hepatotoxicity, increased bleeding in hemophiliacs |
D. Integrase Strand Transfer Inhibitors (INSTIs)
Mechanism (class): Bind to HIV integrase-DNA complex (strand transfer complex) → prevent integration of viral DNA into host chromosome. Block the "strand transfer" step (Mg²⁺-chelating mechanism). Currently the preferred third agent in first-line cART.
| Drug | Key Features | Adverse Effects |
|---|---|---|
| Raltegravir (RAL) | First INSTI (2007); twice daily; minimal CYP interactions; used in pregnancy | Nausea, headache, CPK elevation; rarely rhabdomyolysis; UGT1A1 substrate (rifampin reduces levels) |
| Elvitegravir (EVG) | Requires cobicistat booster; once daily; component of Stribild/Genvoya | GI; many drug interactions (cobicistat) |
| Dolutegravir (DTG) | High genetic barrier to resistance; once daily (no booster needed); active against raltegravir-resistant strains; preferred in current WHO guidelines | Insomnia, headache, weight gain; neural tube defect risk in periconception exposure (caution in women who may become pregnant); creatinine elevation (blocks tubular secretion - not true nephrotoxicity) |
| Bictegravir (BIC) | Newest; highest resistance barrier; no booster; component of Biktarvy (BIC/TAF/FTC) | Nausea, headache; weight gain |
| Cabotegravir (CAB) | Long-acting injectable (monthly/every-2-months) combined with rilpivirine; also approved for PrEP | Injection site reactions |
E. Entry/Fusion Inhibitors
| Drug | Mechanism | Clinical Notes |
|---|---|---|
| Maraviroc (MVC) | CCR5 co-receptor antagonist → blocks gp120-CCR5 interaction → prevents HIV entry. Only active against CCR5-tropic (R5) virus. Tropism testing required before use | Well tolerated; hepatotoxicity risk; used in treatment-experienced patients with R5-tropic virus |
| Enfuvirtide (T-20) | Fusion inhibitor - synthetic peptide mimicking HR2 domain of gp41 → prevents conformational change in gp41 → blocks fusion of viral and cell membranes. SC injection | Injection site reactions (nearly universal); costly; reserved for salvage therapy |
| Ibalizumab | Monoclonal antibody against CD4 (extracellular domain 2) → blocks HIV entry without blocking MHC-II function. IV infusion every 2 weeks | Used in multidrug-resistant HIV |
| Fostemsavir | Prodrug of temsavir; attachment inhibitor targeting gp120 → blocks CD4 receptor binding; oral | Used in heavily treatment-experienced patients with limited options |
IV. ANTI-HBV AGENTS
HBV uses a reverse transcriptase-like polymerase. Most NRTIs active against HIV are also active against HBV.
| Drug | Mechanism | Key Points |
|---|---|---|
| Entecavir | Guanosine nucleoside analog → inhibits HBV polymerase (priming, reverse transcription, DNA synthesis) | High barrier to resistance; first-line for HBV; minimal resistance if HBV-naive; active against lamivudine-resistant strains |
| Tenofovir (TDF/TAF) | Nucleotide → inhibits HBV reverse transcriptase | First-line for HBV; high barrier to resistance; also covers HIV; TAF preferred in renal impairment |
| Lamivudine | Cytosine analog → HBV RT inhibitor | Low barrier to resistance (YMDD mutation M204V/I develops in ~70% by year 5); now largely replaced by entecavir/tenofovir |
| Adefovir | Nucleotide analog → HBV RT inhibitor | Active against lamivudine-resistant HBV; nephrotoxic at higher doses; largely replaced |
| Pegylated IFN-α2a/2b | Multiple mechanisms: immunomodulatory (enhances innate/adaptive immunity), antiviral (induces ISGs), antiproliferative | Finite duration (48 weeks); HBeAg seroconversion in ~30%; cannot use in decompensated cirrhosis; significant side effects (flu-like syndrome, depression, myelosuppression, autoimmune reactions) |
HBV treatment endpoint: HBsAg loss (rare but ideal); HBeAg seroconversion; HBV DNA suppression
V. ANTI-HCV (DIRECT-ACTING ANTIVIRALS - DAAs)
Modern DAA regimens achieve sustained virologic response (SVR) >95% - effectively a cure. Treatment is 8-12 weeks (genotype-dependent).
HCV Targets
| Target | Drug Class | Drugs |
|---|---|---|
| NS3/4A serine protease | NS3/4A Protease Inhibitors ("-previr") | Glecaprevir, Grazoprevir, Simeprevir |
| NS5A (replication complex protein) | NS5A Inhibitors ("-asvir") | Pibrentasvir, Velpatasvir, Ledipasvir, Daclatasvir |
| NS5B RNA-dependent RNA polymerase | NS5B nucleotide analog ("-buvir") | Sofosbuvir |
Key Regimens (pangenotypic preferred)
| Regimen | Composition | Duration | Notes |
|---|---|---|---|
| Sofosbuvir/Velpatasvir (Epclusa) | NS5B + NS5A inhibitor | 12 weeks | Pangenotypic (all HCV genotypes 1-6) |
| Glecaprevir/Pibrentasvir (Mavyret) | NS3/4A + NS5A inhibitor | 8 weeks (treatment-naive, no cirrhosis) | Pangenotypic; NS5B-free regimen |
| Sofosbuvir/Ledipasvir (Harvoni) | NS5B + NS5A inhibitor | 8-12 weeks | Genotypes 1, 4, 5, 6 |
| Sofosbuvir/Velpatasvir/Voxilaprevir (Vosevi) | NS5B + NS5A + NS3/4A | 12 weeks | Pan-genotypic; DAA-experienced patients |
Sofosbuvir is the backbone of most HCV regimens - very high barrier to resistance, excellent safety, active against all HCV genotypes. Key interaction: strong P-gp inducers (rifampin, carbamazepine, St. John's wort) reduce sofosbuvir levels.
VI. ANTI-RSV AGENTS
| Drug | Type | Mechanism | Use |
|---|---|---|---|
| Palivizumab | Humanized monoclonal antibody (anti-F protein) | Binds to RSV fusion (F) protein → prevents viral attachment and cell fusion | Prophylaxis in high-risk infants (premature, congenital heart disease, chronic lung disease); monthly IM injections during RSV season |
| Nirsevimab | Long-acting monoclonal antibody (anti-F protein) | Same mechanism; modified Fc region for extended half-life | Single-dose RSV prophylaxis in infants; approved 2023 |
| Ribavirin | Nucleoside analog | Multiple mechanisms: inhibits inosine monophosphate dehydrogenase (IMPDH) → depletes GTP; also inhibits viral RNA capping; immunomodulatory | Inhaled for severe RSV in hospitalized infants; systemic for HCV (now largely replaced by DAAs); hemorrhagic fever viruses (Lassa, Hanta) |
VII. BROAD-SPECTRUM / MISCELLANEOUS
Ribavirin
- Purine nucleoside analog (guanosine analog)
- Mechanisms: (1) Inhibits IMPDH → depletes GTP pool; (2) inhibits viral RNA capping; (3) immunomodulatory (Th1 shift); (4) mutagen (lethal mutagenesis in some viruses)
- Uses: Chronic HCV (historical - with pegylated interferon); inhaled RSV; Lassa fever; hantavirus; ribavirin + valganciclovir for congenital CMV
- Adverse effects: Hemolytic anemia (dose-limiting); teratogenic (absolute contraindication in pregnancy - contraception required during treatment and 6 months after in both partners); rash, cough (inhaled)
Interferons (IFN-α)
- Mechanism: Bind to cell surface receptors → activate JAK-STAT pathway → induce expression of interferon-stimulated genes (ISGs) → antiviral state; also enhance NK cell and T cell activity
- Pegylated IFN-α2a and 2b: PEGylation extends half-life (once weekly dosing)
- Uses (historical): Chronic HBV, chronic HCV (largely replaced by DAAs), hairy cell leukemia, Kaposi sarcoma, condyloma acuminata
- Adverse effects: Flu-like syndrome (universal; fever, chills, myalgia, fatigue); myelosuppression (neutropenia, thrombocytopenia); neuropsychiatric (depression, suicidality); autoimmune disorders; thyroid dysfunction; alopecia; injection site reactions
Summary: Mechanisms of Action
| Drug / Class | Target Step | Mechanism |
|---|---|---|
| Acyclovir, Valacyclovir, Famciclovir | DNA synthesis | TK-dependent activation → DNA polymerase inhibition + chain termination |
| Ganciclovir, Valganciclovir | DNA synthesis | UL97 kinase activation → CMV DNA pol inhibition + chain termination |
| Cidofovir | DNA synthesis | No viral kinase needed → DNA pol inhibition (long half-life) |
| Foscarnet | DNA synthesis | Direct DNA pol inhibition at pyrophosphate site (no phosphorylation needed) |
| Letermovir | CMV DNA cleavage/packaging | Terminase complex inhibition |
| Oseltamivir, Zanamivir | Viral release | Neuraminidase inhibition → virion aggregation |
| Baloxavir | mRNA transcription | Cap-endonuclease (PA) inhibition |
| Amantadine, Rimantadine | Uncoating | M2 ion channel block (Influenza A only) |
| NRTIs | RT/DNA synthesis | RT inhibition + obligate chain termination (after phosphorylation) |
| NNRTIs | RT/DNA synthesis | Allosteric RT inhibition (no phosphorylation needed; HIV-1 only) |
| Protease Inhibitors | Protein maturation | Aspartyl protease inhibition → immature virions |
| INSTIs | Integration | Integrase strand-transfer inhibition |
| Maraviroc | Entry | CCR5 co-receptor blockade (R5-tropic HIV only) |
| Enfuvirtide | Fusion | gp41 conformational change inhibition |
| DAAs (HCV) | Replication | NS3/4A protease, NS5A, NS5B polymerase inhibition |
| Ribavirin | Multiple | IMPDH inhibition + RNA capping inhibition + mutagenesis |
| Interferons | Multiple | Induction of antiviral ISG state via JAK-STAT |
Sources: Katzung's Basic and Clinical Pharmacology 16e, Chapter 49 (pp. 1346-1420) | Goodman & Gilman's Pharmacological Basis of Therapeutics | Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.