Sernia classification of sln
Reading File
Finding Sources
Searching the Web
Serna classification sentinel lymph node SLN
Finding Sources
Searching the Web
"Sernia classification" lymph node
Finding Sources
Searching the Web
Starz classification sentinel lymph node melanoma SLN metastasis grading
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC3737095/
Reading Article
PMID: 11391592
I now have comprehensive information. "Sernia classification" is the Starz S-classification of sentinel lymph node (SLN) metastases — the phonetic similarity between "S-class" (Starz) and "Sernia" explains the query. Here is the full answer:
Starz (S-Classification) of Sentinel Lymph Node (SLN) Metastases
"Sernia classification" is a phonetic variant of the Starz S-classification — a micromorphometric system for classifying melanoma micrometastases in sentinel lymph nodes. It was developed by Starz et al. (2001) and is widely used to predict non-sentinel lymph node (NSLN) involvement and guide decisions about completion lymph node dissection (CLND).
Basis of the Classification
The system uses two micromorphometric parameters:
- n — Number of 1 mm SLN slices containing melanoma cells
- d — Maximum centripetal depth of metastatic invasion (distance from intra-nodal tumor cells to the inner margin of the SLN capsule, in mm)
Classification Categories
| Stage | Criteria | Pathological Description |
|---|---|---|
| S0 | n = 0 | No detectable tumor cells — negative SLN |
| S1 | 1 ≤ n ≤ 2 AND d ≤ 0.3 mm | Peripheral/subcapsular involvement only — localized peripheral tumor cell deposits |
| S2 | n > 2 AND 0.3 < d ≤ 1 mm | Extended or multifocal peripheral involvement — more extended peripheral metastases |
| S3 | d > 1 mm | Deep metastatic infiltration — invasion deeper than 1 mm below the capsular level |
(Note: Some studies use d ≤ 1 mm for S1, while the refined criteria use d ≤ 0.3 mm for S1 to better distinguish from S2.)
Clinical Significance
The S-classification is a strong independent predictor of:
- NSLN metastasis (non-sentinel node involvement at CLND)
- Distant metastasis
- Overall survival
| Stage | NSLN Positivity at CLND | Implication |
|---|---|---|
| S1 | ~0% | CLND may be safely omitted |
| S2 | ~15–40% | Intermediate risk; individualize decision |
| S3 | ~60% | High risk; CLND strongly recommended |
Clinical Application
- S1 patients have near-zero risk of NSLN involvement → strong candidates for observation alone instead of CLND
- S3 patients have high NSLN metastasis rates → CLND (or systemic therapy) is warranted
- The classification complements the TNM system by refining the "N" component
Key Reference
Starz H, Balda BR, et al. "A micromorphometry-based concept for routine classification of sentinel lymph node metastases and its clinical relevance for patients with melanoma." Cancer. 2001;91(11):2110–21. PMID: 11391592
Cernea classification
Finding Sources
Searching the Web
Cernea classification external branch superior laryngeal nerve thyroidectomy
Reading File
Reading File
Reading File
Loading Image
Cernea Classification
The Cernea classification describes the anatomical relationship of the External Branch of the Superior Laryngeal Nerve (EBSLN) to the superior thyroid artery (STA) and the superior pole of the thyroid gland. It is used during thyroidectomy to identify, preserve, and predict the risk of iatrogenic injury to the EBSLN.
Background
The EBSLN arises from the superior laryngeal nerve (branch of the vagus) and innervates the cricothyroid muscle, which controls voice pitch and projection. Injury causes subtle dysphonia — loss of high-pitched voice (particularly important in singers). Its course is variable, making it vulnerable during ligation of the superior thyroid pedicle.
Classification Types
The nerve is classified based on where it crosses the superior thyroid artery relative to a transverse plane through the upper border of the superior thyroid pole:
| Type | Criteria | Risk of Injury |
|---|---|---|
| Type 1 | EBSLN crosses the STA ≥1 cm above the superior thyroid pole | Low — nerve is well above the operative field |
| Type 2a | EBSLN crosses the STA <1 cm above the superior thyroid pole | Moderate — near the superior pedicle; careful dissection required |
| Type 2b | EBSLN crosses the STA below the upper border of the superior pole (under cover of the pole) | High — most at-risk type; can easily be included in a ligature |
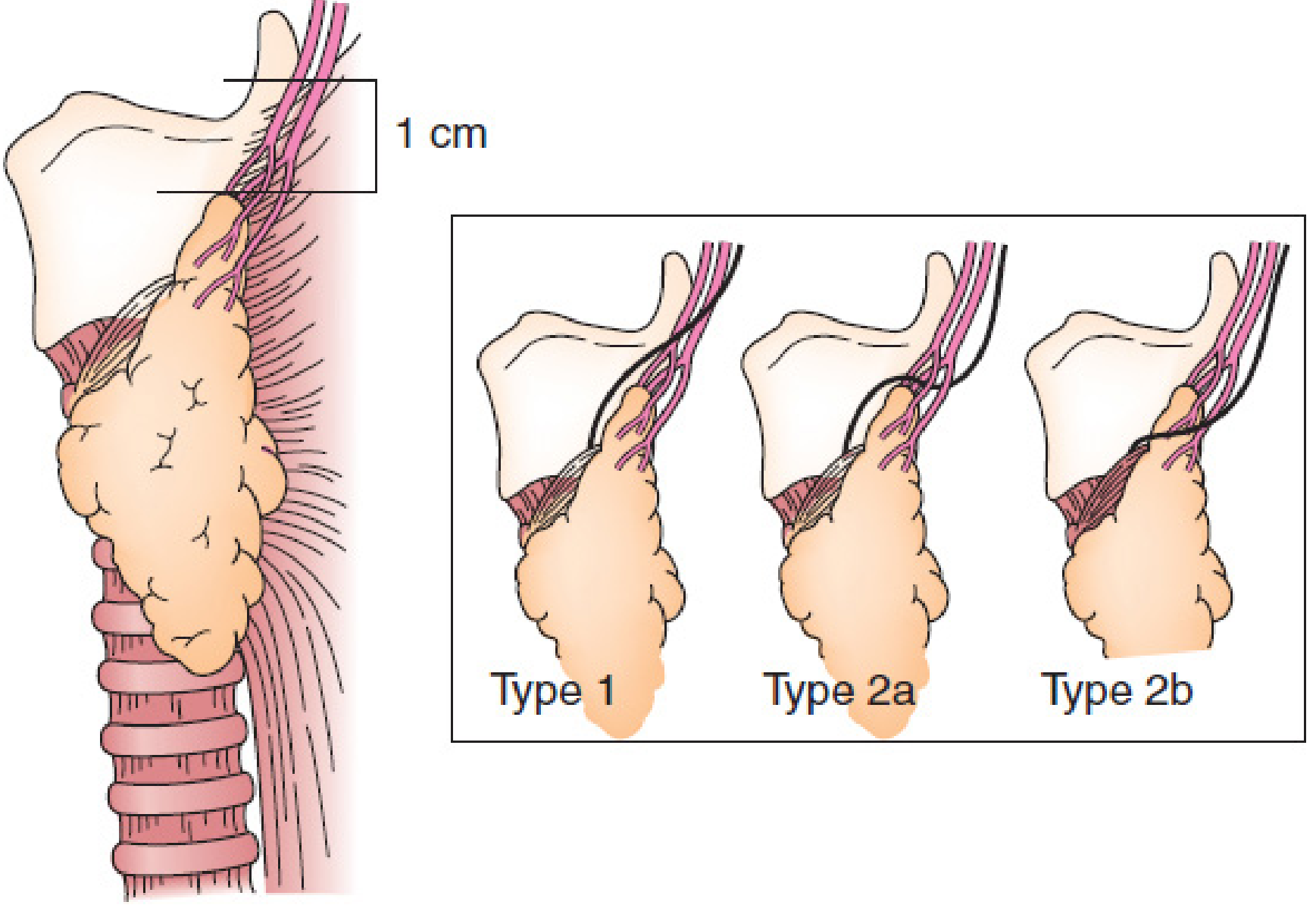
Cernea classification showing Type 1, Type 2a, and Type 2b variants of the EBSLN in relation to the superior thyroid pole.
Prevalence (approximate)
| Type | Small goiters | Large goiters |
|---|---|---|
| Type 1 | ~68% | ~23% |
| Type 2a | ~11% | ~15% |
| Type 2b | ~14% | ~54% |
Large goiters significantly shift the nerve downward, dramatically increasing the proportion of Type 2b — the highest-risk variant.
Surgical Relevance
- Type 2a and 2b are at greatest risk during ligation of the superior thyroid pedicle, particularly when mass ligation is performed rather than individual vessel ligation
- The nerve should be identified in Joll's triangle (bounded by the superior pole of thyroid, the sternothyroid muscle, and the inferior constrictor muscle) before dividing the superior pedicle
- Intraoperative neural monitoring (IONM) has been proposed to assist identification, especially in large goiters where anatomical landmarks are distorted
Sources: Mulholland & Greenfield's Surgery 7e; Current Surgical Therapy 14e; Schwartz's Principles of Surgery 11e
This is a shared conversation. Sign in to Orris to start your own chat.