Hepatic encephalopathy
Reading File
Finding Sources
Searching PubMed
"hepatic encephalopathy"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full, detailed answer.
Hepatic Encephalopathy (HE)
Definition
Hepatic encephalopathy encompasses a wide array of transient, reversible neurologic and psychiatric manifestations in patients with chronic liver disease and portal hypertension, or with acute liver failure (ALF). HE develops in 50% to 70% of patients with cirrhosis and is a poor prognostic indicator - projected 1- and 3-year survival rates without liver transplant (LT) are 42% and 23%, respectively.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1815
Pathophysiology
Multiple overlapping mechanisms operate simultaneously:
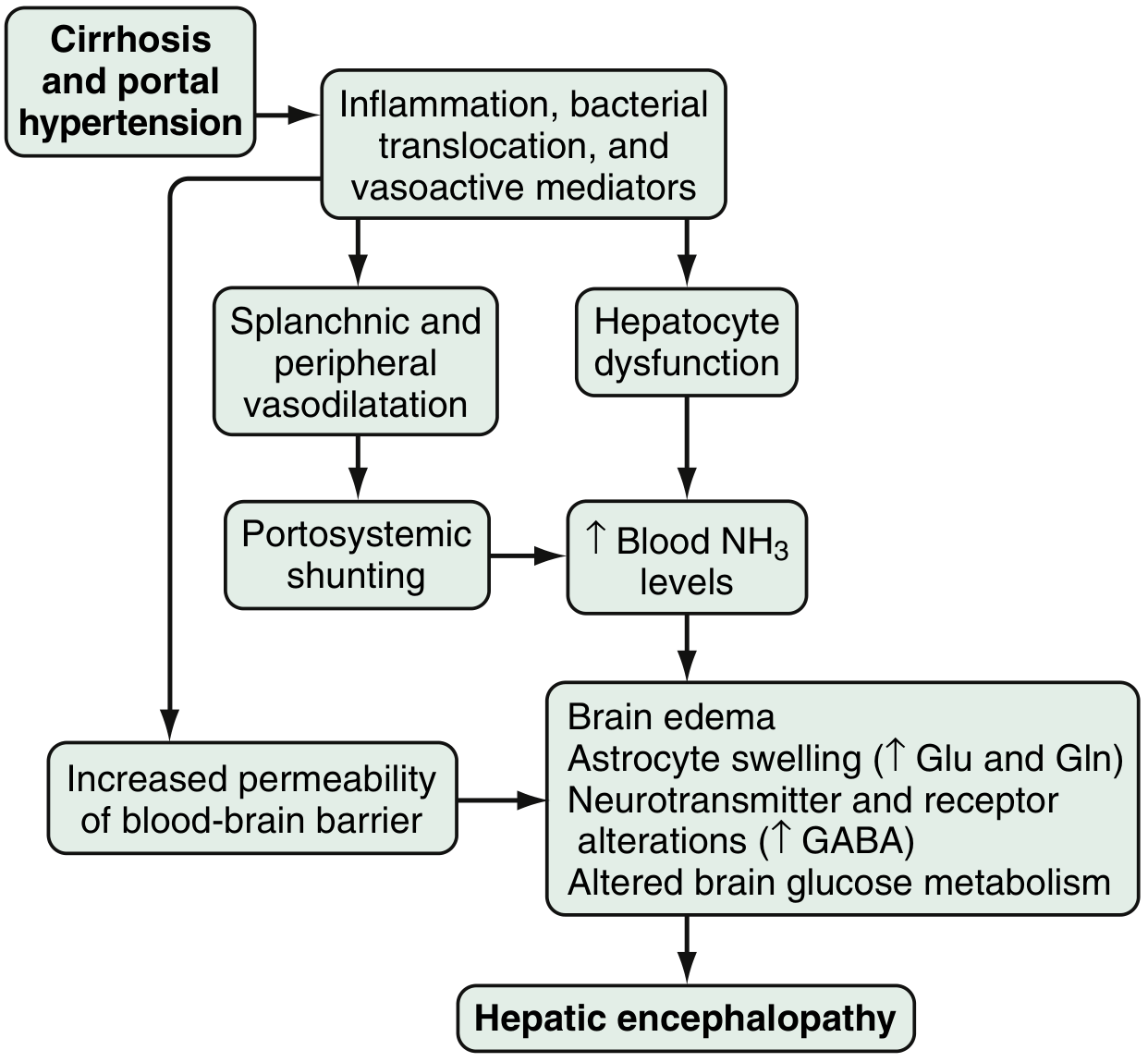
Fig. 94.1 - Proposed pathophysiology of HE (Sleisenger & Fordtran)
1. Ammonia Toxicity
- The best-described neurotoxin is ammonia, produced primarily in the colon by bacterial metabolism of proteins/nitrogen-based products, and by enterocyte synthesis from glutamine
- Under normal conditions, hepatocytes metabolize and clear portal ammonia; in cirrhosis, reduced hepatocyte function plus portosystemic shunting causes hyperammonemia
- Arterial hyperammonemia occurs in up to 90% of HE patients
- Increased blood-brain barrier permeability leads to enhanced uptake by the cerebellum and basal ganglia
- Ammonia directly causes brain edema, astrocyte swelling, and disrupts transport of neuroactive compounds (e.g., myoinositol)
- In ALF, ammonia increases astrocyte glutamine production (via glutamine synthetase), raising glutamine/glutamate levels - contributing to cytotoxic edema
2. GABA-Benzodiazepine System
- Increased sensitivity of the astrocyte peripheral-type benzodiazepine receptor enhances GABA-benzodiazepine activation
- A feed-forward loop: astrocytes produce neurosteroids (allopregnanolone, tetrahydrodeoxycorticosterone) that further activate GABA-A receptors
3. Other Neurotransmitter Changes
- Serotonin (5-HT), nitric oxide (NO), circulating opioid peptides, manganese, and excess oxygen free radicals also contribute
- Manganese causes dopaminergic dysfunction
- Other implicated agents: mercaptans, beta-phenylethylamine, tyramine, octopamine
4. Gut Microbiota
-
Differences in colonic mucosal microbiota in cirrhotic patients with vs. without HE influence production of ammoniagenic substances
-
Distinct allelic mutations in the glutaminase gene increase overt HE risk, potentially by increasing ammonia and glutamate levels
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1815-1816
Classification
By Underlying Disease (Type)
| Type | Underlying Cause |
|---|---|
| Type A | Associated with acute liver failure (ALF) |
| Type B | Portosystemic shunts WITHOUT hepatocellular disease |
| Type C | Chronic/end-stage liver disease with portal hypertension (most common) |
By Severity - West Haven Criteria & SONIC Classification
| West Haven Grade | Intellectual Function | Neuromuscular Function | SONIC Category |
|---|---|---|---|
| 0 | Normal | Normal | Unimpaired |
| Minimal | Normal exam; subtle changes in work/driving | Minor abnormalities on psychometric/visual perception tests | Covert HE |
| 1 | Personality changes, attention deficits, irritability, depression | Tremor, incoordination | Covert HE |
| 2 | Sleep-wake cycle changes, lethargy, behavioral/mood changes, cognitive dysfunction | Asterixis, ataxic gait, slow/slurred speech | Overt HE |
| 3 | Somnolence, confusion, disorientation, amnesia | Rigidity, nystagmus, clonus, Babinski sign, hyporeflexia | Overt HE |
| 4 | Stupor and coma | Oculocephalic reflex, unresponsive to noxious stimuli | Overt HE |
- Covert/Minimal HE affects ~50% of all cirrhotic patients and is commonly overlooked
- Disorientation to time is the key feature distinguishing Grade 1 from Grade 2 (covert from overt HE)
By Time Course
- Episodic - recurrent HE (multiple episodes within 6 months)
- Persistent - altered behavior always present, with relapses
By Precipitating Factors
-
Spontaneous (no identifiable trigger)
-
Precipitated - by GI bleeding, electrolyte abnormalities (especially hypokalemia), infections, sedating medications (benzodiazepines, narcotics), dehydration, constipation
-
Sleisenger and Fordtran's, p. 1815-1816; Bradley and Daroff's Neurology in Clinical Practice, p. 3520-3525
Clinical Features
- Early/covert: Forgetfulness, altered handwriting, difficulty driving, reversal of sleep-wake cycle
- Progressive (overt): Asterixis (flapping tremor - characteristic sign), agitation, disinhibited behavior, disorientation, ataxia, slurred speech
- Severe: Stupor, seizures (10-30% of patients), coma, decerebrate/decorticate posturing
- ALF-specific: Cerebral edema and intracranial hypertension are invariably present in Stage 4, with brainstem herniation being the most common cause of death
Asterixis is pathognomonic but not exclusive to HE - it also occurs in other metabolic encephalopathies (uremia, CO2 narcosis, etc.)
Diagnosis
No Gold Standard Laboratory Test
- Blood ammonia levels are not sensitive or specific for HE
- False elevations: GI bleeding, tourniquet use during blood draw, delayed lab processing, diuretics, alcohol, narcotics, valproic acid
- Arterial ammonia offers no advantage over venous ammonia in chronic liver disease
Neuropsychometric Testing
- Portosystemic encephalopathy (PSE) syndrome test and Stroop test - evaluate attention, concentration, fine motor skills, orientation
- EncephalApp (smartphone-based Stroop test) - validated for covert/minimal HE detection
- Critical flicker frequency (CFF) test - reliable marker for minimal HE
Neurophysiological
- EEG: Early slowing of alpha rhythm progressing to delta frequencies; triphasic waves in later stages (poor prognosis)
- MR spectroscopy and T1 TAPIR mapping - research tools to quantify HE parameters
Differential Diagnosis of Hyperammonemia (Box 94.1)
Includes: ALF, chronic kidney disease, GI bleeding, urea cycle defects, medications (valproic acid, diuretics, alcohol, narcotics), muscle ischemia, portosystemic shunts
- Sleisenger and Fordtran's, p. 1816-1817
Treatment
1. Correct/Eliminate Precipitating Factors
This is the primary therapeutic approach: treat GI bleeding, infections (SBP, UTI), electrolyte disturbances (especially hypokalemia), dehydration, and remove offending medications.
2. Dietary Management
- Protein restriction is no longer recommended - it is harmful and does not benefit HE
- Vegetable and dairy proteins are preferable to animal proteins (more favorable calorie-to-nitrogen ratio)
- Branched-chain amino acid (BCAA) supplementation may benefit HE, but does not clearly reduce mortality
3. Reduce Intestinal Ammonia - First-Line
Lactulose (or lactitol)
- Non-absorbable disaccharide metabolized by colonic bacteria
- Mechanism: causes catharsis, acidifies the colon (inhibits ammonia absorption), and decreases transit time
- Effective for acute and chronic HE vs. placebo
- Dose: titrate to 2-3 soft stools/day
- Side effects: abdominal cramping, flatulence, diarrhea, electrolyte imbalance
- Can be given per rectum as an enema in patients at aspiration risk
4. Oral Antibiotics - Second-Line or Add-On
Rifaximin 550 mg twice daily (FDA-approved 2010)
- Used for chronic HE and prevention of recurrence of overt HE
- Superior tolerability vs. lactulose; main limitation is cost
- Other antibiotics studied (neomycin, metronidazole, vancomycin) - not clearly established for chronic HE
5. Other Agents
| Agent | Mechanism | Evidence |
|---|---|---|
| Probiotics | Modify gut flora, reduce ammonia generation | Probably improve recovery, overt HE, QoL, and plasma ammonia (Cochrane review) - not mortality |
| Acarbose | Alpha-glucosidase inhibitor; shifts colonic flora from proteolytic to saccharolytic | RCT shows benefit in mild HE with diabetes |
| L-ornithine L-aspartate (LOLA) | Activates urea cycle, enhances ammonia clearance | Possible benefit (Cochrane); NOT available in the USA |
| Zinc supplementation | Zinc deficiency common in cirrhosis; zinc activates ornithine transcarbamylase | Possible benefit; clear efficacy not established |
| Sodium benzoate/phenylacetate | Alternate ammonia excretion pathways | FDA-approved for urea cycle defects; efficacy in cirrhosis not well established; high sodium load |
| MARS (Molecular Adsorbent Recirculating System) | Extracorporeal albumin dialysis | Reduces ammonia in acute-on-chronic liver failure |
6. Liver Transplant (LT)
-
Definitive treatment - generally reverses HE
-
Should be considered before permanent neurologic damage
-
Sleisenger and Fordtran's, p. 1817-1818
Acute vs. Chronic HE - Key Distinguishing Features
| Feature | Acute Liver Failure | Portal Systemic Encephalopathy (Chronic) |
|---|---|---|
| Onset | Usually acute | Varies; may be insidious |
| Mental state | Mania evolving to deep coma | Blunted consciousness |
| Precipitant | Viral infection or hepatotoxin | GI hemorrhage, protein load, drugs, uremia, infection |
| Prior liver disease | No | Usually yes |
| Cerebral edema | Common, severe | Less prominent |
Special Considerations: Pediatric HE
-
In children, irritability and lethargy are the most common initial signs
-
Neurological findings: pyramidal signs → hypotonia → focal signs → early parkinsonism, ataxia, tremor, dysarthria
-
Asterixis is present but less prominent as a discriminating feature
-
Clinically evident HE is less common in children with chronic liver disease than in adults, but 50% of children with chronic liver disease have minimal HE on neuropsychological testing
-
Seizures occur in 10-30% of pediatric patients
-
Common pediatric causes: fulminant viral/autoimmune hepatitis, drug ingestion (acetaminophen, salicylates, valproate), Reye syndrome, Wilson disease, mitochondrial diseases
-
Bradley and Daroff's Neurology, p. 1252-1253
Prognosis
- Overt HE: 1-year survival 20-40%, 3-year survival ~15% without transplant
- Cerebral edema (Stage 4) - brainstem herniation is the leading cause of death
- Minimal HE predicts progression to overt HE and negatively impacts driving ability and quality of life
Recent Evidence Update (PubMed 2025-2026)
A 2025 meta-analysis (PMID 40812534) found that proton pump inhibitor (PPI) use is associated with increased risk of hepatic encephalopathy in cirrhotic patients - clinicians should avoid unnecessary PPI prescription in this population. A 2026 systematic review (PMID 41942881) evaluated risk prediction models for HE in liver cirrhosis, noting that MELD score, serum ammonia, and Child-Pugh score are the most commonly incorporated predictors.
This is a shared conversation. Sign in to Orris to start your own chat.