Lymphoma in HIV patients with MTB Negative and CD 4 count more than 200
Reading File
Finding Sources
Finding Sources
Searching PubMed
lymphoma HIV "CD4 count" immunocompromised
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the answer.
Lymphoma in HIV Patients: MTB Negative, CD4 Count >200
This is a clinically important scenario. HIV patients with a CD4 count >200/μL and no evidence of tuberculosis (MTB negative) can still develop lymphoma - and understanding which types, why, and how they present is key.
Why Lymphoma Still Occurs at CD4 >200?
The most important concept here, emphasized by Robbins & Cotran Pathologic Basis of Disease, is:
"Even in the face of effective ART, the overall rate of lymphoma in the HIV-infected population remains elevated, even in those with normal CD4+ T-cell counts. Most of the lymphomas that arise in patients with preserved CD4 T-cell counts are not associated with EBV or HHV8."
The mechanism is germinal center B-cell hyperplasia, which occurs early in HIV infection even before significant immunodeficiency develops. During germinal center reactions, B cells undergo:
- Class switching
- Somatic hypermutation via Activation-Induced Cytidine Deaminase (AID)
Both processes involve DNA breaks and are error-prone, leading to oncogene translocations (e.g., MYC, BCL6).
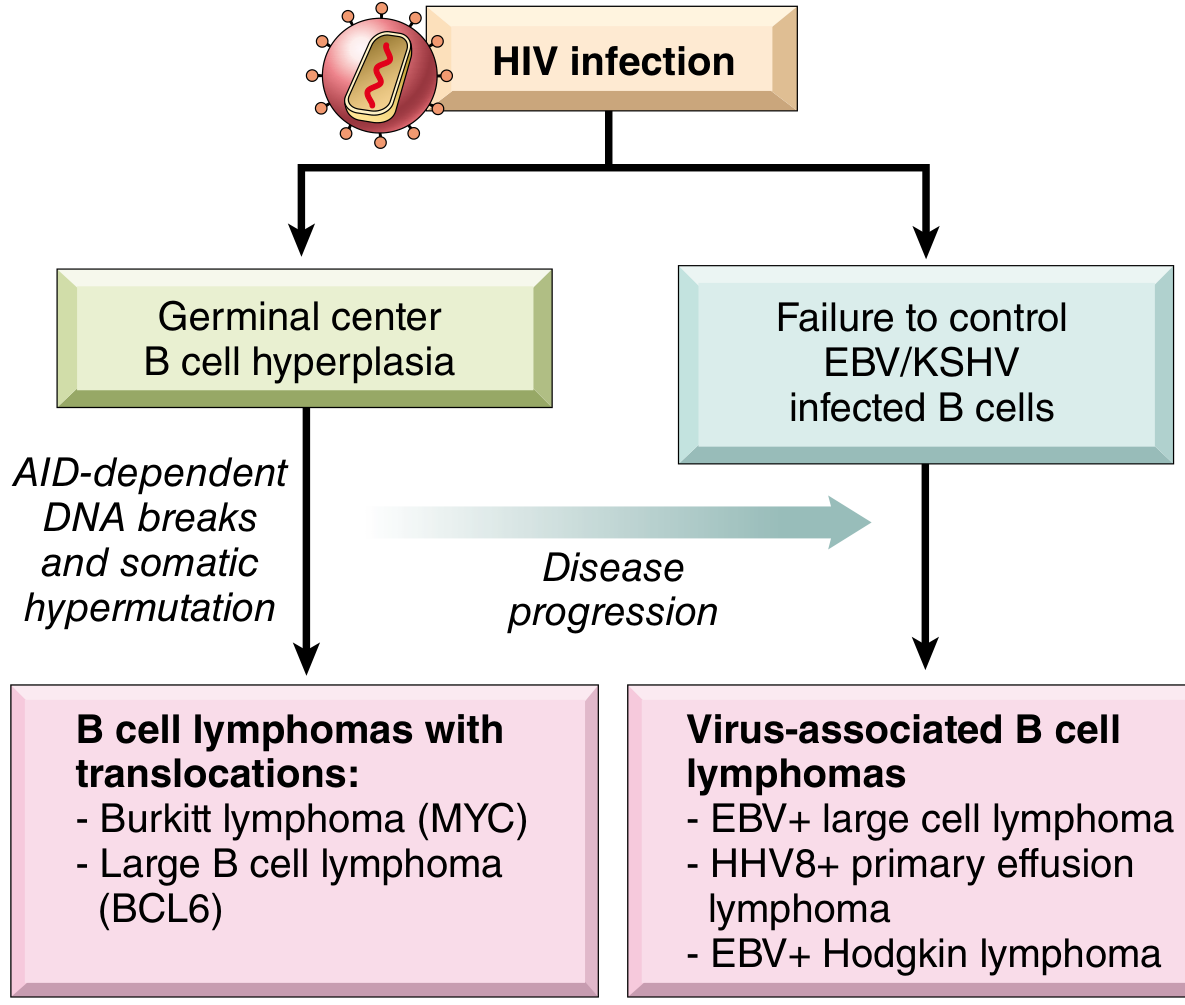
Fig. 6.43 - A model for pathogenesis of B-cell lymphomas in HIV. AID-dependent DNA breaks lead to translocations (MYC → Burkitt, BCL6 → DLBCL), while failure to control EBV/KSHV-infected B cells leads to virus-associated lymphomas. - Robbins & Cotran
Types of Lymphoma Most Likely at CD4 >200 (MTB Negative)
| Lymphoma Type | CD4 Threshold | EBV/HHV8 | Key Features |
|---|---|---|---|
| Systemic DLBCL (immunoblastic) | Can occur at CD4 >200 (mean ~226/μL) | Often EBV- | ~60% of HIV lymphomas; extranodal common |
| Burkitt's Lymphoma | Relatively preserved CD4 | 50% EBV+ | c-MYC translocation t(8;14); most common in age 10-19 |
| Hodgkin Lymphoma | Variable; some at CD4 >200 | EBV+ (Reed-Sternberg cells) | 30-fold higher risk vs general population |
Harrison's Principles (22nd Ed., 2025): "Systemic lymphoma is seen at earlier stages of HIV infection than primary CNS lymphoma. In one series the mean CD4+ T cell count was 226/μL."
Primary CNS Lymphoma is less likely here - it typically presents with median CD4 ~50/μL and is EBV-positive in nearly 100% of cases.
Two Pathogenic Mechanisms (Robbins & Cotran)
Mechanism 1 - Germinal Center Hyperplasia (CD4-independent):
- Occurs early in HIV infection
- AID-dependent DNA breaks → oncogene translocations
- Produces Burkitt lymphoma (MYC translocation) and DLBCL (BCL6 translocation)
- These are EBV/HHV8-negative - more typical in patients with preserved immunity
Mechanism 2 - Failure to Control Oncogenic Viruses (CD4-dependent):
- T-cell depletion removes EBV/KSHV surveillance
- Activated EBV-infected B-cell clones proliferate and acquire mutations
- Produces EBV+ large B-cell lymphoma, HHV8+ Primary Effusion Lymphoma (PEL), and EBV+ Hodgkin lymphoma
- More typical at lower CD4 counts
Clinical Presentation (Harrison's 22E)
- >80% present with extranodal disease (CNS, gut, orbit, lungs, bone marrow)
- B symptoms (fever, night sweats, weight loss) in ~80% of cases
- Oral cavity involvement (immunoblastic lymphoma of hard palate) is characteristic
- Ann Arbor stage is typically advanced (Stage III-IV) at presentation
- Performance status is often poor
Why MTB Negative Matters Here
In a TB-negative HIV patient with CD4 >200, the differential for lymphadenopathy or constitutional symptoms should include:
- AIDS-related systemic lymphoma (especially DLBCL, Burkitt) - most likely
- Hodgkin lymphoma - do not miss; significantly elevated risk
- Multicentric Castleman disease (HHV8-associated; can mimic lymphoma)
- Primary effusion lymphoma (PEL) - presents as pleural/peritoneal effusions
With MTB ruled out, empirical anti-TB therapy should not be started. Tissue biopsy for histology, immunophenotyping, and viral testing (EBV, HHV8) is the next step.
Summary Table
| Feature | Detail |
|---|---|
| Incidence | ~10% of AIDS patients develop lymphoma; 10-20x general population risk |
| Most common type | DLBCL (immunoblastic) - 60% of HIV lymphomas |
| CD4 at systemic lymphoma diagnosis | Mean ~226/μL |
| CD4 at CNS lymphoma diagnosis | Median ~50/μL |
| EBV association | >50% of all HIV lymphomas; 40% per Henry's Clinical Diagnosis |
| Burkitt's incidence increase | >1000-fold vs general population |
| Hodgkin lymphoma increase | ~30-fold vs general population |
| Effect of ART | Reduced incidence but risk remains elevated even with normal CD4 |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th Ed.), pp. 244-245 - on B-cell lymphoma pathogenesis and CD4-independent mechanism
- Harrison's Principles of Internal Medicine (22nd Ed., 2025), p. 1657 - on types, CD4 thresholds, and CNS vs systemic lymphoma
- Henry's Clinical Diagnosis and Management by Laboratory Methods - HIV-associated lymphomas section
This senario in the patient who is taking ART more than 2 years
Finding Sources
Finding Sources
Searching PubMed
lymphoma HIV "antiretroviral therapy" "immune reconstitution"
Reading File
Finding Sources
Reading Article
PMID: 40647389
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information. Here is the detailed, focused answer for this specific clinical scenario.
Lymphoma in HIV Patient on ART >2 Years, CD4 >200, MTB Negative
This is a distinct and increasingly recognized clinical scenario - the so-called "ART-era lymphoma." It behaves differently from pre-ART HIV lymphoma and demands specific diagnostic and management thinking.
The Core Paradox: Why Lymphoma Despite ART?
The 2025 Cancers review (Dolcetti et al., 2025 - PMID 40647389) states directly:
"Although efficiently managed by cART, chronic HIV infection remains associated with a high incidence of malignant lymphomas."
And from Robbins & Cotran:
"Even in the face of effective ART, the overall rate of lymphoma in the HIV-infected population remains elevated, even in those with normal CD4+ T-cell counts."
There are three mechanisms that explain why this happens specifically on long-term ART:
Mechanism 1: Persistent Germinal Center Dysregulation (Most Important at CD4 >200 on ART)
ART suppresses viral replication but does not fully normalize B-cell biology. Early and sustained HIV infection drives:
- Profound germinal center B-cell hyperplasia
- Chronic AID (Activation-Induced Cytidine Deaminase) activity
- Error-prone somatic hypermutation and class switching → oncogene translocations (MYC, BCL6)
These changes are set in motion early and persist even after immune reconstitution. Lymphomas arising through this pathway are typically:
- EBV-negative, HHV8-negative
- Burkitt lymphoma (MYC translocation) or DLBCL germinal-center subtype (BCL6)
- More likely at relatively preserved CD4 counts
Goldman-Cecil Medicine: "Although the risk for HIV-associated Burkitt lymphoma increases with advancing immunodeficiency, it may be seen in patients with relatively preserved CD4 cell counts. Antiretroviral therapy reduces but does not eliminate the risk for Burkitt lymphoma in HIV-1-infected persons."
Mechanism 2: Immune Reconstitution and Unmasking (IRIS-Type Lymphoma)
In patients starting or continuing ART with immune recovery, a paradoxical immune reconstitution inflammatory syndrome (IRIS)-like phenomenon can occur. A previously subclinical lymphoma (often EBV-driven) gets unmasked as the immune system partially reconstitutes and mounts an inflammatory response around the tumor. This is more likely in the first 6-24 months of ART, but can occur later.
Mechanism 3: Ongoing Chronic Immune Activation
Even on suppressive ART, HIV-infected individuals have:
- Persistent microbial translocation from the gut → chronic systemic inflammation
- Elevated IL-6, IL-10 (B-cell growth factors)
- Residual immune dysregulation
This chronic inflammatory milieu sustains B-cell proliferative pressure independent of CD4 count.
Which Lymphoma Type Is Most Likely?
| Lymphoma Type | Why on ART with CD4 >200 | EBV/HHV8 | Key Feature |
|---|---|---|---|
| Burkitt Lymphoma | Germinal center dysregulation; c-MYC translocation; occurs at preserved CD4 | 50% EBV+ | Fastest-growing tumor; t(8;14); B symptoms + rapid mass |
| DLBCL (Systemic) | Most common; germinal center or activated B-cell subtype | Variably EBV+ | Mean CD4 ~226/μL at diagnosis; extranodal common |
| Hodgkin Lymphoma | PARADOXICALLY MORE COMMON on ART - rises with immune reconstitution | EBV+ (Reed-Sternberg) | Mixed cellularity subtype; "paradox of ART" |
| Multicentric Castleman Disease (MCD) | Incidence has INCREASED in ART era | HHV8+ | Not true lymphoma but mimics it; fever, LAD, hepatosplenomegaly |
| Primary Effusion Lymphoma (PEL) | Rare; lower CD4; HHV8+EBV coinfection | EBV + HHV8 | Effusions without mass; less likely at CD4 >200 |
The ART-Era Paradox for Hodgkin Lymphoma
Harrison's 22E: Hodgkin lymphoma does not share the dramatic decrease seen with other AIDS-defining conditions in the ART era. In fact, it may increase as CD4 recovers, because the inflammatory microenvironment around Reed-Sternberg cells depends on reconstituted immune effector cells.
Harrison's: "The incidence of AIDS-associated systemic lymphomas has not experienced a dramatic decrease as a consequence of the widespread use of effective ART."
Harrison's on MCD: "While the incidence of Kaposi's sarcoma has decreased, the incidence of multicentric Castleman's disease has increased in the setting of ART."
Clinical Presentation on ART
Key features that should trigger suspicion in this patient:
| Feature | Detail |
|---|---|
| B symptoms | Fever, night sweats, weight loss >10% - present in ~80% |
| Extranodal disease | >80% at presentation - GI tract (~25%), bone marrow (~20%), liver/lung (~10%), CNS (~33%) |
| Rapid lymphadenopathy | Especially cervical, mediastinal, or retroperitoneal |
| Oral cavity mass | Hard palate immunoblastic lymphoma - characteristic in HIV |
| Unexplained LDH elevation | Tumor burden marker |
| CNS symptoms | Headache, focal deficits, seizures - suggest primary CNS lymphoma (but CNS lymphoma usually CD4 <100) |
Diagnostic Approach
MTB negative + CD4 >200 + on ART >2 years + lymphadenopathy/mass
↓
Lymphoma must be ACTIVELY excluded
↓
1. Excisional biopsy (preferred over FNA)
→ Histology + immunophenotype (CD20, CD10, BCL6, MUM1, Ki-67)
→ EBV (EBER in-situ hybridization)
→ HHV8 (if effusion or suspected MCD/PEL)
→ FISH for MYC, BCL2, BCL6 (double/triple hit lymphoma)
2. Staging CT chest/abdomen/pelvis (PET-CT preferred)
3. Bone marrow biopsy
4. LP if any neurological symptoms (CSF EBV PCR if CNS lesion)
5. HIV viral load + CD4 count (confirm ART efficacy)
6. Serum LDH, uric acid, beta-2 microglobulin
Management on ART
The standard is chemotherapy concurrent with continued ART:
| Lymphoma | Regimen | Notes |
|---|---|---|
| DLBCL | R-CHOP (rituximab + cyclophosphamide + doxorubicin + vincristine + prednisone) | First-line for CD20+ tumors |
| DLBCL (high-grade) | R-EPOCH (rituximab + etoposide + prednisone + vincristine + doxorubicin) | Preferred for high-grade/MYC-rearranged |
| Burkitt | Intensive regimens (CODOX-M/IVAC or DA-EPOCH-R) | Medical emergency; doubling time 24-48h |
| Primary CNS Lymphoma | High-dose methotrexate-based (NOT R-CHOP - poor BBB penetration) | + Radiation (palliative) |
| Hodgkin Lymphoma | ABVD or BEACOPP | Continue ART throughout |
KJ Lee's Otolaryngology: "The standard treatment consists primarily of chemotherapy with concurrent ART. The outcomes have improved in the ART era, with 3-year overall survival approaching 50% for all comers."
Harrison's 22E: "Response rates as high as 72% with a median survival of 33 months and disease-free intervals up to 9 years have been reported." Concerns about bone marrow toxicity overlap between ART and chemotherapy are mitigated by avoiding myelosuppressive antiretrovirals (e.g., zidovudine/AZT) during chemotherapy.
Prognosis Determinants in This Patient
Poor prognostic factors (International Prognostic Index adapted for HIV):
- Age >60 years
- Advanced stage (III/IV)
- Elevated LDH
- Poor performance status (ECOG >1)
- More than one extranodal site
- Low CD4 at time of lymphoma diagnosis (despite being on ART)
Favorable factors in this specific patient:
- CD4 >200 (better immune reserve)
- Already on ART >2 years (viral suppression likely)
- MTB negative (no competing infectious burden)
- More likely to tolerate full-dose chemotherapy
Key Takeaway Points
- ART does not eliminate lymphoma risk - it reduces but does not abolish it; germinal center dysregulation from prior HIV infection persists
- Burkitt lymphoma and DLBCL are the most likely diagnoses at CD4 >200 on long-term ART - both often EBV-negative
- Hodgkin lymphoma paradoxically increases with immune reconstitution on ART
- Multicentric Castleman Disease incidence has risen in the ART era and mimics lymphoma
- Concurrent ART + chemotherapy is standard; avoid myelosuppressive ARVs (AZT) during chemo
- Outcomes are better in the ART era vs. pre-ART, with survival approaching that of HIV-negative lymphoma patients
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th Ed.), p. 244 - pathogenesis of B-cell lymphoma in HIV
- Harrison's Principles of Internal Medicine (22nd Ed., 2025), pp. 1656-1658 - lymphoma types, CD4 thresholds, treatment outcomes
- Goldman-Cecil Medicine (International Ed.) - Burkitt lymphoma on ART
- KJ Lee's Essential Otolaryngology - management regimens and survival data
- Dolcetti R et al., Cancers 2025 - PMID 40647389 - oncogenic pathways and therapeutic opportunities in ART-era HIV lymphoma
This is a shared conversation. Sign in to Orris to start your own chat.