Diff between adult and child SSPE presentation, EEG , pThology, treatment and what is MIBE
Reading File
Finding Sources
Finding Sources
Searching the Web
SSPE adult vs child presentation EEG pathology MIBE measles inclusion body encephalitis
Reading File
Reading File
Searching PubMed
adult onset SSPE subacute sclerosing panencephalitis clinical features
Reading File
Reading Web Page
https://cpsp.cps.ca/uploads/publications/RA-subacute-scleros…
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
SSPE: Adult vs Child - Complete Comparison
Background & Pathogenesis
SSPE (Subacute Sclerosing Panencephalitis) is a rare, late, and almost universally fatal complication of measles virus infection. It results from persistent, non-productive measles virus infection of neurons and glia in immunocompetent patients. Aberrant M (matrix) protein and other envelope proteins prevent viral assembly and budding - the virus stays intracellular and spreads by cell-to-cell contact, evading immune clearance.
- Bradley & Daroff's Neurology, p. 1678
1. Clinical Presentation: Child vs Adult
| Feature | Childhood / Adolescent (Classic) | Adult-Onset (Atypical) |
|---|---|---|
| Age at onset | 5-15 years (median ~8 yrs after measles) | Mean 25.4 years (range 20-35) |
| Age of measles infection | Most infected <2 years; boys > girls (3:1) | Higher proportion with no documented measles history |
| Latent interval | 2-12 years (median 8 years) | May be longer or undocumented |
| Stage I (weeks-months) | Behavioral change, personality shift, declining school performance | Psychiatric features dominate - misdiagnosed as schizophrenia or mood disorder; cognitive dysfunction, difficulty with simple tasks |
| Stage II | Myoclonic jerks (massive, repetitive), intellectual decline, seizures, ataxia | Myoclonus may be less prominent initially; seizures and motor changes |
| Stage III | Rigidity, spasticity, autonomic dysfunction, decerebrate posturing | Similar but course is faster - lower mean survival of only a few months |
| Stage IV | Vegetative state, death | Vegetative state, death |
| Psychiatric misdiagnosis | Less common | More common; can mimic psychosis or dementia in elderly |
| Pregnancy association | N/A | SSPE can present during pregnancy with cognitive dysfunction; children born to affected mothers are typically healthy |
| Course | Progressive over 1-3 years (mean 18 months) | Tends to be more fulminant with rapid decline |
| Spontaneous remission | ~5% estimated | Rarer in adults |
Key point: Adult-onset SSPE is often atypical and missed. It may present predominantly with psychiatric symptoms before neurological signs appear. Later onset correlates with more rapid decline.
- StatPearls SSPE
- CPSP SSPE review
- Bradley & Daroff's Neurology, p. 1678
2. EEG Findings
Classic (Childhood) EEG - Radermecker Complexes
The hallmark EEG finding (seen in 65-83% of cases) is the Radermecker complex: generalized, bilaterally synchronous slow-wave complexes with a regular periodicity. Features:
- Complexes last up to 3 seconds
- Occur at regular intervals of 4-14 seconds
- Background shows diffuse depression between complexes
- These high-amplitude bursts coincide with the myoclonic jerks (Stage II)
Adult EEG
-
The same periodic complexes may be seen, but atypical EEG patterns are more common in adults
-
Some adults show: lack of rhythmicity, varying intervals between complexes, or even alpha coma pattern (psychiatric illness presentations)
-
EEG may be normal or non-specifically abnormal early in adult disease, contributing to diagnostic delay
-
Bradley & Daroff's Neurology, p. 1679; Radiopaedia SSPE
3. Pathology
Both child and adult SSPE share the same fundamental histopathological substrate - there are no proven age-specific pathological differences, but the same lesions cause more rapid functional deterioration in adults.
Gross Pathology
- Brain atrophy (diffuse cortical and white matter involvement)
- Relative sparing of the cerebellum
- Sclerosis of white matter (hence "sclerosing")
Histopathology (the same in both age groups)
The cardinal features are:
- Cowdry type A intranuclear inclusion bodies - eosinophilic, glassy inclusions in neurons and glial cells (the "hallmark" - visible in the image below)
- Cytoplasmic inclusions - cigar-shaped, within pyramidal neurons
- Nucleocapsids within oligodendrocytes
- Perivascular lymphocytic cuffing (inflammatory infiltrate around vessels)
- Diffuse gliosis (astrocytic reaction)
- Neuronal loss with demyelination in white matter
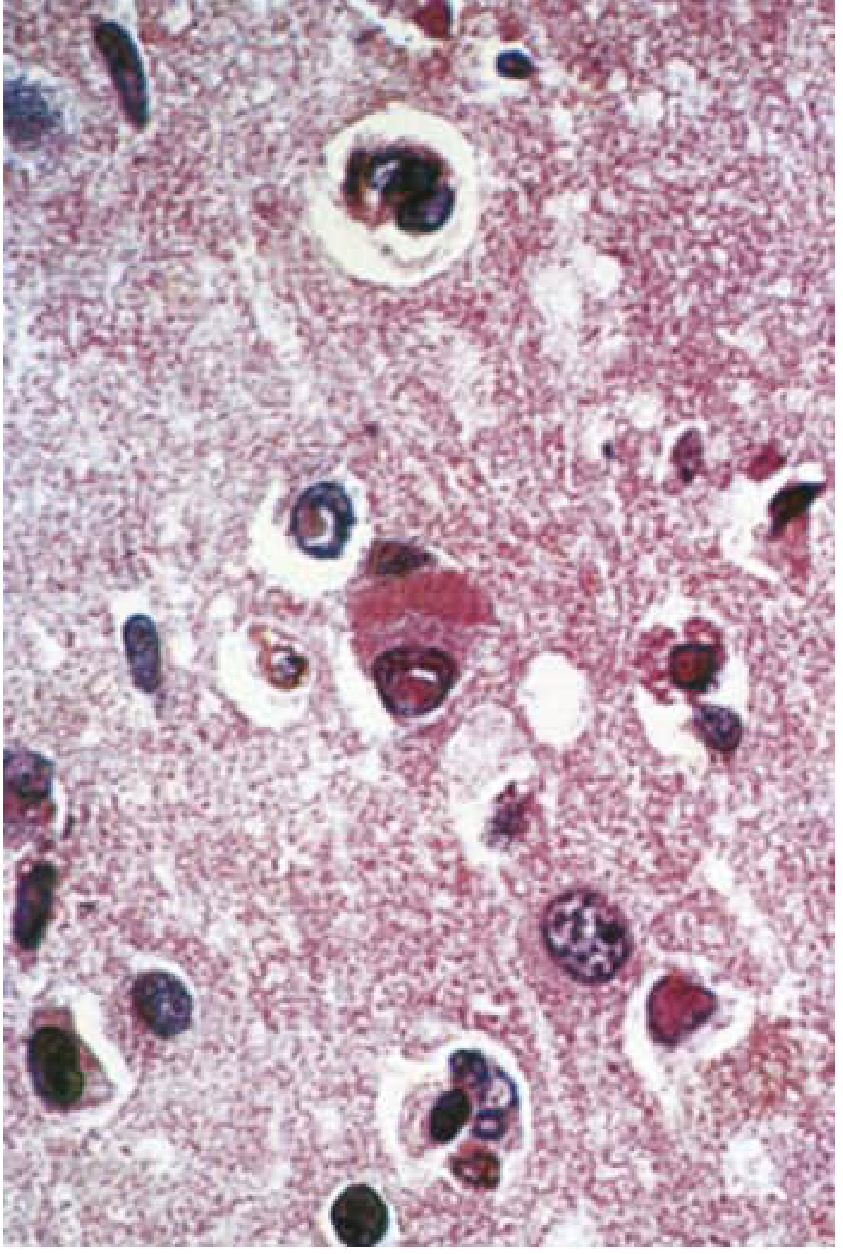
Cerebral cortex in SSPE: pyramidal neuron with Cowdry-type A intranuclear inclusion + cigar-shaped cytoplasmic inclusion. Cowdry A inclusions also in glial nuclei. (H&E x350) - Bradley & Daroff's Neurology, Fig. 78.8
CSF (both age groups)
- CSF pleocytosis: absent
- Glucose: normal
- Protein: normal or elevated
- High titers of anti-measles IgG in CSF and serum - key diagnostic finding
- CSF/serum antibody ratio indicates high intrathecal synthesis
- Gammaglobulin >20% of total CSF protein
MRI (early stage)
-
High T2/FLAIR signal in posterior gray and subcortical white matter of hemispheres early
-
Progresses to diffuse atrophy with widespread white matter changes
-
Bradley & Daroff's Neurology, p. 1679
4. Treatment
There is no known curative therapy for SSPE. Management aims to slow progression. The same approach is used regardless of age:
Antiviral / Immunomodulatory Regimens
| Agent | Dose / Route | Notes |
|---|---|---|
| Intraventricular Interferon-alfa (via Ommaya reservoir) | Start 100,000 U/m² BSA/day, titrate up to 10⁶ U/m²/day over 5 days; then 10⁶ U/m² twice weekly for 6 months | ~30-35% improve or stabilize |
| Oral Isoprinosine (Inosiplex) | 100 mg/kg/day (max 3 g/day) in 3 divided doses for 6 months | Combined with IFN-alfa for synergy |
| IV Ribavirin + Intrathecal IFN-alfa | Case reports of response | Used when standard therapy fails |
| Systemic (SC) IFN-alfa | Up to 5 million units daily | Targets peripheral virus reservoirs (lymphoid, glandular tissue) |
| Levetiracetam | Standard AED dosing | Symptomatic improvement in myoclonus and encephalopathy |
Monitoring
- Laboratory endpoint: eradication of measles antigen from CSF
Risks of Prolonged Treatment
- Meningitis (from Ommaya reservoir)
- IFN-alfa-induced encephalopathy
- IFN-alfa upper and lower motor neuron toxicity
Prognosis
- Spontaneous remission: ~5%
- Most die within 1-3 years of diagnosis (mean 18 months)
- Adult onset = faster decline, shorter mean survival of months
Prevention (the only real "treatment")
-
MMR / MMRV vaccine: 1st dose at 12-15 months, 2nd dose at 4-6 years
-
Children infected with measles under age 1 have 16x greater risk of SSPE than those infected at age ≥5
-
Bradley & Daroff's Neurology, p. 1719-1720
5. MIBE - Measles Inclusion Body Encephalitis
MIBE is a distinct CNS complication of measles, often confused with SSPE but critically different:
Definition
Measles Inclusion Body Encephalitis (MIBE) = a rapidly progressive, usually fatal encephalitis caused by direct viral attack on brain cells in immunodeficient patients, occurring months after measles exposure (not years).
Key Differences from SSPE
| Feature | SSPE | MIBE |
|---|---|---|
| Host immune status | Immunocompetent | Immunodeficient (T-cell defect) |
| Onset after measles | 2-12 years | 1-9 months |
| Course | Slow, progressive | Rapidly progressive |
| Fever | Absent | Absent |
| CSF | Normal cell count, high measles Ab | Normal (no inflammatory response) |
| Measles Ab titers | High in CSF and serum | May be low or absent |
| Pathogenesis | Slow viral infection, immune escape | Direct viral cytopathic effect |
| Diagnosis | CSF serology + EEG | PCR for measles virus in brain or CSF |
| Treatment | IFN-alfa + isoprinosine | Supportive + reduce immunosuppression + passive immunoglobulin |
| Vaccine strain | Not caused by vaccine strain | Can be caused by vaccine strain measles (reported in immunodeficient children) |
Clinical Features of MIBE
- Behavior changes
- Myoclonus
- Refractory focal or generalized seizures (prominent)
- Delirium
- Coma
- Develops in patients with T-cell deficiency (e.g., HIV, transplant recipients, congenital immunodeficiency)
Why MIBE Differs Pathologically
In SSPE, the immune system is intact and generates abundant anti-measles antibodies - but the virus hides intracellularly. In MIBE, there is defective cell-mediated immunity so the virus replicates more openly, producing classic inclusion bodies (hence the name) but without effective immune control, leading to rapid fatal progression.
A notable case: A previously healthy infant who received MMR vaccine developed MIBE 8.5 months later and died - measles antigens found on brain biopsy from the vaccine strain.
- Bradley & Daroff's Neurology, p. 1678
- Harrison's Principles of Internal Medicine 22E, p. 1685
- CPSP review
Quick Summary Table: SSPE Child vs Adult vs MIBE
| Child SSPE | Adult SSPE | MIBE | |
|---|---|---|---|
| Immune status | Competent | Competent | Deficient |
| Latency | 2-12 yr | >10 yr possible | 1-9 months |
| First symptoms | Behavior/school | Psychiatric/psychosis | Seizures, delirium |
| Myoclonus | Prominent | Variable | Present, refractory seizures |
| EEG | Classic Radermecker | Atypical, may be absent | Non-specific |
| CSF | High measles IgG, no cells | Same, possibly less typical | Normal |
| Course | 1-3 yr | Months (faster) | Weeks-months |
| Treatment | IFN-alfa + isoprinosine | Same | Supportive + reduce immunosuppression |
Give me answer
The full detailed answer is already above in my previous response. Here is a concise summary of everything covered:
SSPE: Adult vs Child + MIBE - Key Points
Presentation
Child (Classic):
- Age 5-15 yrs, latency 2-12 yrs after measles (median 8 yrs)
- Boys > girls (3:1)
- Stage I: behavior change, declining school performance
- Stage II: myoclonic jerks (massive, repetitive), seizures, intellectual decline, ataxia
- Stage III: rigidity, spasticity, autonomic dysfunction
- Stage IV: vegetative state → death
- Course: 1-3 years (mean 18 months)
Adult (Atypical):
- Mean onset age 25.4 yrs (range 20-35)
- Often no documented measles history
- Stage I dominated by psychiatric symptoms (misdiagnosed as schizophrenia/depression)
- Myoclonus less prominent early
- Course is faster - survival often only a few months
- Can present during pregnancy
EEG
Child: Classic Radermecker complexes - generalized, bilaterally synchronous slow-wave bursts lasting up to 3 sec, at regular intervals of 4-14 sec, on a background of depressed activity. Coincides with myoclonic jerks. Present in 65-83% of cases.
Adult: Same pattern may occur but atypical findings are more common - irregular periodicity, varying intervals, or alpha coma pattern. EEG may be normal early, causing diagnostic delay.
Pathology
Same in both age groups:
- Cowdry type A intranuclear inclusions in neurons and glia (eosinophilic, glassy)
- Cigar-shaped cytoplasmic inclusions in pyramidal neurons
- Nucleocapsids within oligodendrocytes
- Perivascular lymphocytic cuffing
- Diffuse gliosis + neuronal loss + demyelination
- Relative sparing of cerebellum
- CSF: no cells, normal glucose, high anti-measles IgG (intrathecal synthesis), gammaglobulin >20% of total CSF protein
Treatment
No cure. Same regimen regardless of age:
- Intraventricular IFN-alfa via Ommaya reservoir - start 10⁵ U/m²/day, titrate to 10⁶ U/m²/day, then twice weekly for 6 months
- Oral Isoprinosine (Inosiplex) - 100 mg/kg/day (max 3 g/day) in 3 doses for 6 months
- Ribavirin + intrathecal IFN-alfa - in refractory cases
- Levetiracetam - symptomatic control of myoclonus
- Systemic SC IFN-alfa - targets peripheral viral reservoirs
- Spontaneous remission ~5%
- Prevention: MMR vaccine is the only effective strategy
MIBE (Measles Inclusion Body Encephalitis)
A separate, distinct CNS complication of measles:
| Feature | SSPE | MIBE |
|---|---|---|
| Host | Immunocompetent | Immunodeficient (T-cell defect) |
| Latency | 2-12 years | 1-9 months |
| Course | Slow (years) | Rapidly progressive (weeks-months) |
| Fever | Absent | Absent |
| Seizures | Myoclonic | Refractory focal/generalized |
| CSF | High measles Ab | Normal (no Ab response) |
| Diagnosis | Serology + EEG | PCR in brain/CSF |
| Vaccine strain | No | Yes (can occur post-MMR in immunodeficient) |
| Treatment | IFN-alfa + isoprinosine | Supportive + reduce immunosuppression + passive Ig |
MIBE = direct viral attack on brain cells due to failed cell-mediated immunity. No inflammatory CSF because the immune system cannot mount a response. Fatal within weeks to months.
This is a shared conversation. Sign in to Orris to start your own chat.