Tgive me details about sternoclavicular joints
Reading File
Finding Sources
Searching the Web
sternoclavicular joint anatomy ligaments movements clinical significance
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from the textbooks. Let me compile a thorough answer.
Sternoclavicular Joint
Overview
The sternoclavicular (SC) joint is a saddle-shaped synovial joint - the only bony articulation between the upper limb and the axial skeleton. It is the primary skeletal connection linking the pectoral girdle to the trunk.
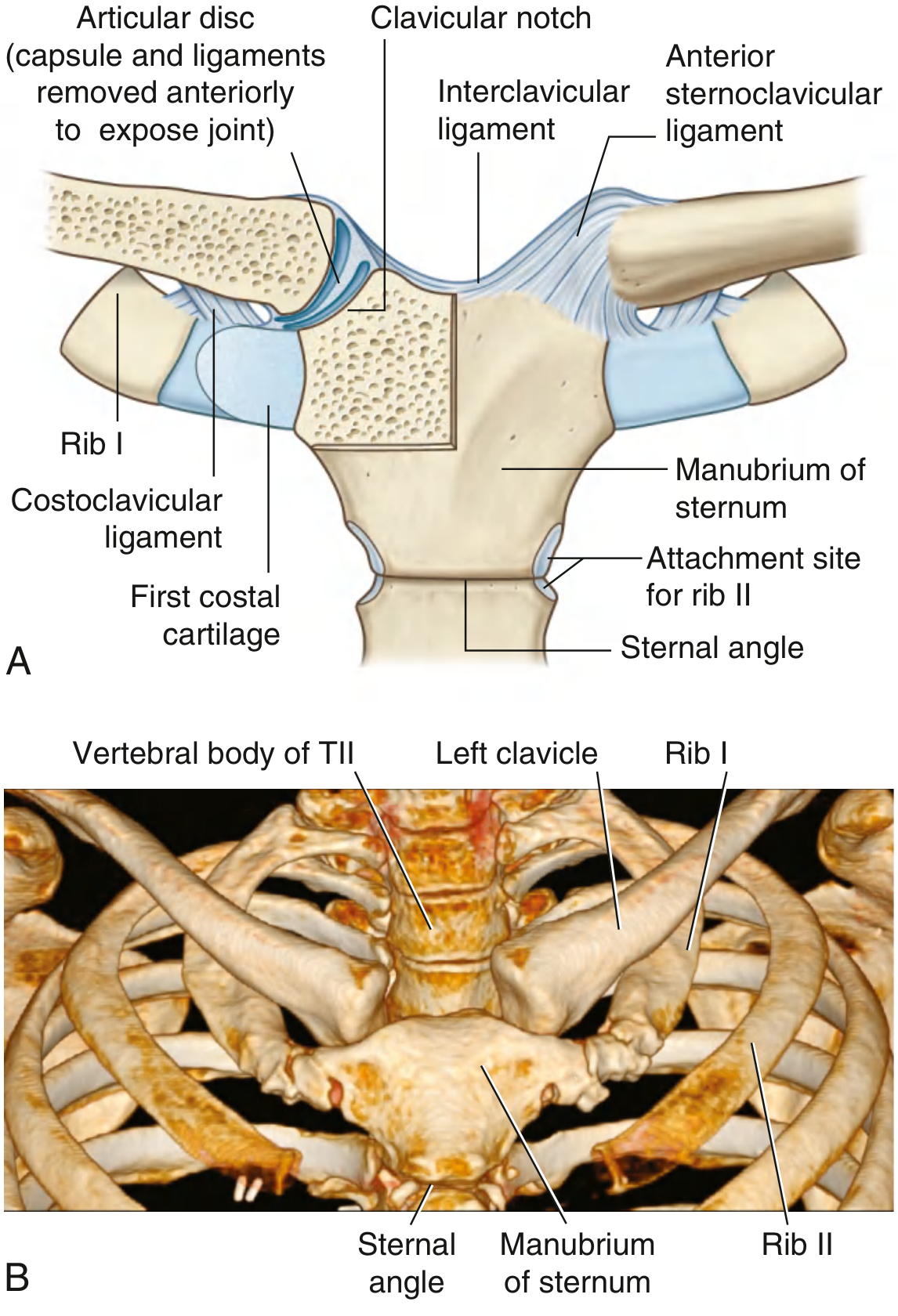
Articulating Surfaces
The joint involves three surfaces:
- Medial (sternal) end of the clavicle - larger than its counterpart, so it projects above the superior border of the manubrium
- Clavicular notch of the manubrium of the sternum
- Superior surface of the first costal cartilage
The articular surfaces are covered by fibrocartilage rather than hyaline cartilage.
- Gray's Anatomy for Students, p. 824
Articular Disc
A fibrocartilaginous intra-articular disc completely divides the joint cavity into two separate compartments (upper and lower). This disc:
- Compensates for the incongruity between the articular surfaces
- Absorbs compressive forces transmitted along the clavicle
- Acts as a pivot for clavicular movements
- Attaches superiorly to the clavicle and inferiorly to the first costal cartilage
Joint Capsule
A fibrous joint capsule surrounds the entire joint and extends to the margins of the articular surfaces. It is reinforced by four main ligaments.
Ligaments
| Ligament | Location | Function |
|---|---|---|
| Anterior sternoclavicular ligament | Anterior to the joint | Reinforces the anterior capsule; resists anterior dislocation |
| Posterior sternoclavicular ligament | Posterior to the joint | Reinforces the posterior capsule; primary restraint against posterior displacement |
| Interclavicular ligament | Superior, connects both clavicles across the jugular notch of the manubrium | Links medial ends of both clavicles; limits excessive depression of the pectoral girdle |
| Costoclavicular ligament | Lateral to the joint, between inferior surface of medial clavicle and first rib/costal cartilage | Primary restraint of the SC joint; limits elevation, protraction, and retraction of the clavicle |
The posterior capsule is considered the single most important stabilizer of the joint. The costoclavicular ligament, by anchoring the clavicle inferiorly to the first rib, is the dominant passive restraint overall.
- Gray's Anatomy for Students, p. 824; StatPearls - Anatomy, SC Joint
Movements
The SC joint has three degrees of freedom, acting like a ball-and-socket functionally despite its saddle morphology:
| Movement | Plane | Range |
|---|---|---|
| Elevation - Depression | Coronal | ~45° elevation, ~10° depression |
| Protraction - Retraction | Horizontal | ~15-30° each |
| Axial (long-axis) rotation | Along the clavicle's long axis | ~30-40° (occurs mainly during shoulder elevation above 90°) |
Almost all movements of the shoulder girdle are transmitted through this joint.
- Gray's Anatomy for Students, p. 824; Kenhub - Sternoclavicular Joint
Neurovascular Supply
- Nerve supply: Medial supraclavicular nerve (C3, C4) and a branch from the nerve to subclavius (C5, C6)
- Blood supply: Internal thoracic artery and suprascapular artery
Clinical Significance
1. Dislocation
The SC joint is inherently stable due to its strong ligamentous support - dislocation is uncommon (less than 3% of shoulder girdle injuries) but serious.
Anterior dislocation (most common):
- Results from an indirect force on the anterior shoulder with the arm abducted
- Medial end of the clavicle displaces anteriorly
- Presents with pain, swelling, and a prominent anterior deformity
- Usually managed non-operatively with closed reduction
- If irreducible, causes an unsightly prominence but minimal disability in sedentary patients
Posterior (retrosternal) dislocation (less common, more dangerous):
- The medial clavicle displaces behind the sternum into the mediastinum
- Can compress or injure: trachea, esophagus, thoracic duct, subclavian vessels, brachial plexus
- May cause: respiratory distress, venous congestion, arterial insufficiency, myocardial conduction abnormalities
- Can be a true surgical emergency
- Groh et al. found early recognition (<10 days) significantly improves likelihood of successful closed reduction
- CT scan and MRI are recommended to confirm diagnosis alongside plain radiographs
Important note: In patients under 25 years, apparent SC dislocations may actually represent physeal injuries (epiphyseal fractures), as the medial clavicular epiphysis is the last epiphysis in the body to fuse (around age 23-25).
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 7332-7377
2. Recurrent Subluxation
- Recurrent atraumatic anterior subluxation is seen typically in young women/girls during shoulder abduction and extension
- Often associated with generalized joint laxity
- Usually self-limiting; treated conservatively with upper extremity strengthening
- Surgery (tendon graft reconstruction in figure-eight configuration through drill holes in the manubrium and medial clavicle) is reserved for cases where symptoms limit daily activities
3. Arthritis
- SC joint can be affected by osteoarthritis, rheumatoid arthritis, septic arthritis, SAPHO syndrome, and gout
- Septic arthritis of the SC joint is associated with IV drug use and immunocompromised states
4. Surgical Considerations
- A thoracic surgeon must be on standby for any open surgery at the SC joint due to proximity to mediastinal structures
- Pins and wires must never be placed across the SC joint - there are well-documented cases of fatal pin migration into the heart and great vessels
Summary Table
| Feature | Detail |
|---|---|
| Joint type | Saddle-shaped synovial joint |
| Articulating bones | Medial clavicle + manubrium of sternum + 1st costal cartilage |
| Articular disc | Present - divides cavity into 2 compartments |
| Key ligaments | Anterior/posterior SC ligaments, interclavicular, costoclavicular |
| Primary stabilizer | Posterior capsule + costoclavicular ligament |
| Movements | Elevation/depression, protraction/retraction, axial rotation |
| Clinical concern | Posterior dislocation - mediastinal structure injury |
Sources: Gray's Anatomy for Students (p. 824), Campbell's Operative Orthopaedics 15th Ed 2026, Rheumatology 2-Volume Set (Elsevier 2022), NCBI StatPearls - Sternoclavicular Joint
This is a shared conversation. Sign in to Orris to start your own chat.