Here is your complete comprehensive guide to Harrison's Chapters 131-146 - Community Acquired Infections. This is drawn directly from Harrison's Principles of Internal Medicine 22nd Edition (2025).
🏥 HARRISON'S CHAPTERS 131-146: Community Acquired Infections
Complete Study Guide for Future Doctors
CHAPTER 131 - PNEUMONIA
Authors: Lionel A. Mandell, Michael S. Niederman
Definition
Pneumonia is infection of the pulmonary parenchyma. It is classified as:
- Community-acquired (CAP) - acquired outside hospital
- Hospital-acquired (HAP) - acquired ≥48h after admission
- Ventilator-associated (VAP) - acquired ≥48h after intubation
Healthcare-associated pneumonia (HCAP) - this category has been discontinued because it did not reliably predict MDR organisms
Aspiration pneumonia accounts for 5-15% of CAP cases. It is a continuum with CAP and HAP, not a separate category.
Pathophysiology
The lungs are not sterile - they have a lung microbiota. Pneumonia is an emergent phenomenon involving:
- Inflammatory trigger (often viral + microaspiration)
- Cytokine/chemokine release → selective bacterial growth (e.g., S. pneumoniae, P. aeruginosa)
- Positive feedback loop - inflammation → more bacterial growth → more inflammation
Routes of organism entry:
- Microaspiration of oropharyngeal flora (most common)
- Inhalation
- Hematogenous spread
- Direct mucosal dispersion
Host defenses overcome by pathogens:
- Nasal hairs/turbinates
- Branching airway anatomy
- Mucociliary clearance
- Gag/cough reflex
- Alveolar macrophages
- Neutrophil recruitment
Etiology of CAP
| Setting | Key Organisms |
|---|
| Outpatient, no comorbidities | S. pneumoniae, M. pneumoniae, H. influenzae, respiratory viruses |
| Outpatient, comorbidities | S. pneumoniae, H. influenzae, enteric gram-negatives |
| ICU | S. pneumoniae, S. aureus (MRSA), Legionella, gram-negatives |
| Aspiration risk | Anaerobes, S. pneumoniae, enteric gram-negatives |
Atypical organisms (cause "atypical pneumonia"):
- Mycoplasma pneumoniae
- Chlamydia pneumoniae
- Legionella pneumophila
Antimicrobial Resistance - Key Facts
- Penicillin-resistant S. pneumoniae - very common; mechanism = altered penicillin-binding proteins
- Macrolide-resistant M. pneumoniae - Japan 30%, China 95%, US/France 5-13% (mutation in 23S rRNA domain V)
- ESBL-producing gram-negatives - treat with carbapenems
- Fluoroquinolone-resistant E. coli - increasing in community
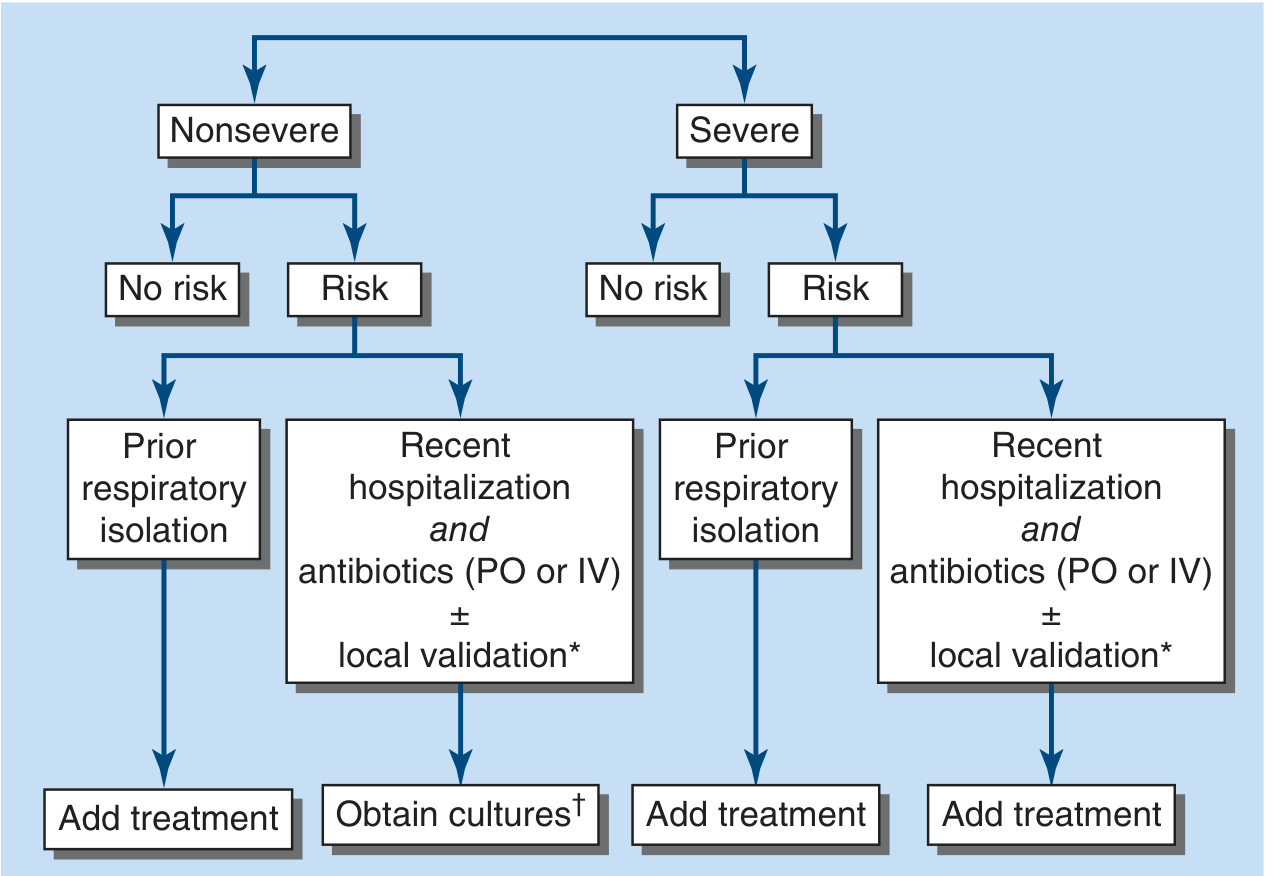
CAP Treatment Algorithm
FIGURE 131-1: Algorithm for assessing inpatient risk of MRSA or Pseudomonas aeruginosa infection in CAP. "Risk" = recent hospitalization AND antibiotics (PO or IV). IV = intravenous.
Outpatient CAP Treatment
No comorbidities / No resistance risk:
- Amoxicillin 1g TID OR
- Doxycycline 100mg BD OR
- Azithromycin (in areas with low pneumococcal macrolide resistance)
With comorbidities:
- Amoxicillin-clavulanate + macrolide or doxycycline OR
- Respiratory fluoroquinolone (levofloxacin/moxifloxacin) alone
Key principle: Always cover atypical organisms (Mycoplasma, Chlamydia) in outpatients.
Inpatient CAP Treatment (Non-ICU)
- Beta-lactam + macrolide OR
- Respiratory fluoroquinolone alone
ICU-level CAP
- Beta-lactam + macrolide OR beta-lactam + fluoroquinolone
- Add vancomycin/linezolid if MRSA risk present
- Add anti-pseudomonal beta-lactam if P. aeruginosa risk present
Aspiration Pneumonia
- Routine anaerobic coverage is NOT needed unless: poor dentition, lung abscess, or necrotizing pneumonia
Severity Assessment
CURB-65 Score (1 point each):
- C - Confusion (new)
- U - Urea >7 mmol/L (BUN >20 mg/dL)
- R - Respiratory rate ≥30/min
- B - Blood pressure <90 systolic or ≤60 diastolic
- 65 - Age ≥65 years
Score 0-1: Outpatient | Score 2: Hospital admission | Score ≥3: Consider ICU
PSI/PORT Score - more complex, 5 risk classes; Class IV-V = hospitalize
HAP and VAP
- Most important pathogens: P. aeruginosa, Staphylococcus aureus, enteric gram-negatives (Klebsiella, Enterobacter, E. coli, Acinetobacter)
- Key principle: Empirical therapy must cover MDR gram-negatives and MRSA
- De-escalate based on culture results and clinical improvement
Prevention
- Pneumococcal vaccines: PCV15 or PCV20 (preferred in adults ≥65)
- Influenza vaccine: Annual, reduces secondary bacterial pneumonia
- Smoking cessation
- Elevate head of bed 30-45° to prevent VAP
- Chlorhexidine oral decontamination in ventilated patients
CHAPTER 132 - LUNG ABSCESS (Legionella Pneumonia)
Note: Chapter 132 in Harrison's covers Lung Abscess and specific organisms like Legionella.
Legionella Pneumonia
Organism: Legionella pneumophila serogroup 1 (most common)
Source: Water reservoirs (cooling towers, hospital water systems, potable water)
Transmission: Inhaled aerosolized water - NOT person-to-person
Clinical features (Pontiac Fever vs Legionnaires' Disease):
| Feature | Pontiac Fever | Legionnaires' Disease |
|---|
| Severity | Mild, flu-like | Severe pneumonia |
| Mortality | Very low | 5-30% |
| Pneumonia | No | Yes |
| Self-limiting | Yes (2-5 days) | No - needs antibiotics |
Classic Legionella clues:
- Older male, smoker, immunocompromised
- Relative bradycardia (pulse-temperature dissociation)
- Hyponatremia
- Elevated LFTs
- Diarrhea (watery)
- Confusion/encephalopathy
- Failure to respond to beta-lactams
Diagnosis:
- Urinary antigen - best for serogroup 1 (sensitivity 70-90%, rapid)
- BAL culture on BCYE agar (buffered charcoal yeast extract) - gold standard
- PCR
Treatment:
- Azithromycin (preferred) - 500mg daily x 7-10 days
- Levofloxacin 750mg daily x 5-7 days (good penetration)
- NOT beta-lactams (no cell wall; Legionella is intracellular)
CHAPTER 133 - INFECTIVE ENDOCARDITIS (IE)
Definition
IE is infection of the endocardium - usually involving heart valves, but can involve mural endocardium or septal defects. It involves a vegetation (fibrin + platelets + organisms).
Modified Duke Criteria
Major Criteria:
- Positive blood cultures with typical IE organisms (≥2 separate cultures of S. aureus, viridans streptococci, S. gallolyticus, HACEK organisms, Enterococcus faecalis without primary focus)
- Echocardiographic evidence (vegetation, abscess, new dehiscence of valve prosthesis)
- New valvular regurgitation
Minor Criteria:
- Predisposing condition (valve disease, IV drug use)
- Fever ≥38°C
- Vascular phenomena (septic emboli, Janeway lesions, intracranial hemorrhage)
- Immunologic phenomena (Osler nodes, Roth spots, RF positive, glomerulonephritis)
- Positive blood cultures not meeting major criteria
Definite IE: 2 major, OR 1 major + 3 minor, OR 5 minor
Possible IE: 1 major + 1 minor, OR 3 minor
Etiology
| Organism | % of IE | Notes |
|---|
| Staphylococcus aureus | 30-40% | Most common overall; IV drug users; acute course |
| Viridans streptococci | 20-30% | Native valve, indolent course |
| S. gallolyticus (bovis) | ~5% | Associated with colon cancer - colonoscopy needed |
| HACEK organisms | ~5% | Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella |
| Enterococcus | ~10% | GU/GI instrumentation |
| Culture-negative | 5-10% | Prior antibiotics, Coxiella, Bartonella, Brucella |
Clinical Features
Peripheral stigmata (memorize these for exams!):
| Sign | Location | Pathogenesis | Memory Tip |
|---|
| Osler nodes | Fingertips (painful) | Immune complex | "Osler = Ouch!" (painful) |
| Janeway lesions | Palms/soles (painless) | Septic emboli | "Janeway = Just painless" |
| Splinter hemorrhages | Subungual | Emboli | Under nails |
| Roth spots | Retina | Immune complex | Eye spots |
| Clubbing | Fingers | Chronic hypoxia | Subacute IE |
| Petechiae | Conjunctiva/skin | Emboli | |
Systemic features:
- Fever (90%)
- New/changing murmur (80%)
- Splenomegaly (subacute)
- Septic emboli → stroke, pulmonary emboli (right-sided IE)
Right-sided vs Left-sided IE
| Feature | Right-sided (tricuspid) | Left-sided (mitral/aortic) |
|---|
| Common in | IV drug users | Valvular disease, prosthetic valves |
| Emboli to | Lungs (septic pulmonary emboli) | Brain, kidneys, spleen |
| Organism | S. aureus | S. aureus, Streptococci |
| Prognosis | Better | Worse |
Treatment
Native valve streptococcal IE:
- Penicillin G 12-18 MU/day x 4 weeks (or ceftriaxone 2g daily x 4 weeks)
Native valve S. aureus IE:
- MSSA: Nafcillin/oxacillin 12g/day x 6 weeks
- MRSA: Vancomycin 15-20 mg/kg q8-12h x 6 weeks
- Gentamicin is NOT recommended for native valve S. aureus IE (nephrotoxic, no benefit)
Prosthetic valve IE:
- Longer courses (6 weeks)
- Often requires surgical replacement
Indications for Surgery:
- Heart failure due to valve destruction
- Paravalvular abscess
- Resistant organisms (fungal, highly resistant)
- Large vegetations with recurrent emboli
- Failure to sterilize after 7-10 days appropriate antibiotics
CHAPTER 134 - INFECTIONS OF SKIN, MUSCLE, AND SOFT TISSUES
Authors: Dennis L. Stevens, Amy E. Bryant
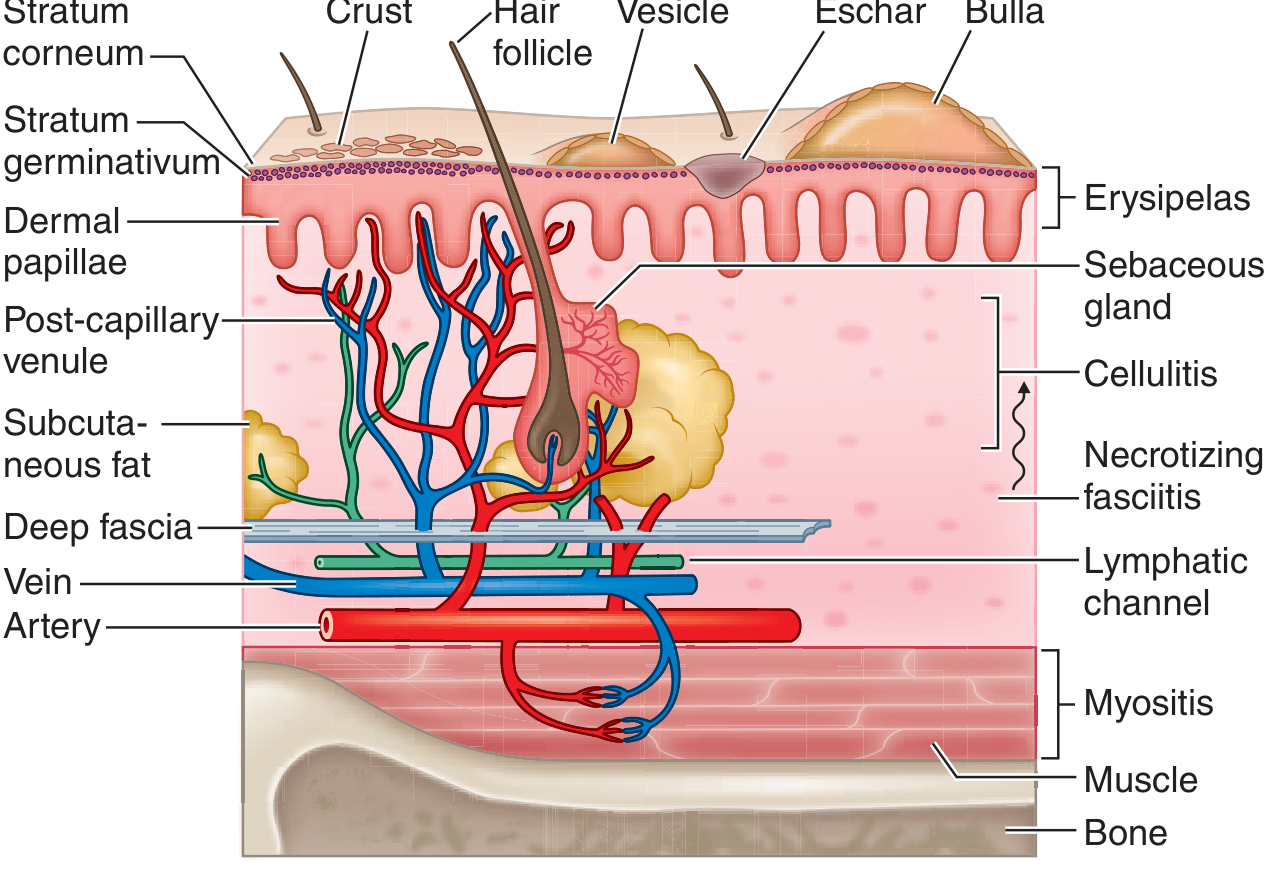
Anatomic Approach to Soft Tissue Infections
The anatomic layer determines the infection type - this is the key concept!
FIGURE 134-1: Cross-section of skin showing anatomic layers and corresponding infections. Erysipelas = superficial dermis; Cellulitis = dermis/subcutaneous fat; Necrotizing fasciitis = deep fascia; Myositis = muscle.
Key Skin Infections Summary
Impetigo
- Layer: Epidermis
- Organisms: S. aureus (bullous) and S. pyogenes (non-bullous)
- Features: Honey-colored crusted lesions (non-bullous), fragile bullae (bullous)
- Tx: Mupirocin topical (mild); oral dicloxacillin/cephalexin (extensive)
Erysipelas
- Layer: Superficial dermis and lymphatics
- Organism: Group A Streptococcus (S. pyogenes)
- Features: Sharply demarcated, raised, fiery red, painful plaque; peau d'orange skin; rapid lateral spread; often face or leg; systemic toxicity
- Tx: Penicillin V or amoxicillin (oral); IV penicillin G if severe
Cellulitis
- Layer: Deep dermis and subcutaneous fat
- Organisms: S. aureus (including MRSA), Group A/B/C Streptococci
- Features: Erythema, warmth, swelling, pain - NOT sharply demarcated (vs. erysipelas)
- Tx: Cephalexin or dicloxacillin (mild); IV cefazolin (moderate); vancomycin if MRSA suspected
Folliculitis, Furuncles, Carbuncles
- Layer: Hair follicle
- Organisms: S. aureus (most), Pseudomonas (hot-tub folliculitis in chlorinated water)
- Furuncle = deep abscess of single follicle
- Carbuncle = multiple interconnected furuncles
- Tx: I&D (drainage) is primary; add antibiotics if systemic toxicity or MRSA
Necrotizing Fasciitis (NF) - THE SURGICAL EMERGENCY
Layer: Deep fascia with sparing of muscle initially
Two types:
| Feature | Type I | Type II |
|---|
| Organisms | Polymicrobial (anaerobes + gram-negatives) | Group A Strep (S. pyogenes) alone |
| Risk factors | Diabetes, elderly, abdominal surgery | Healthy young adults, minor trauma |
| Location | Trunk/perineum | Extremities |
Clinical clues (red flags):
- Pain out of proportion to skin findings
- Bullae
- Crepitus (gas in tissues - best felt/heard on palpation)
- Skin necrosis, dusky discoloration
- Rapid progression, systemic toxicity
- CT scan shows fascial thickening and gas in planes
Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score - uses WBC, CRP, Hb, Na, creatinine, glucose
Treatment: IMMEDIATE SURGICAL DEBRIDEMENT + broad-spectrum antibiotics (piperacillin-tazobactam or meropenem + vancomycin + clindamycin to block toxin production)
Fournier's gangrene = NF of perineum/genitalia - urologic emergency
Myositis / Gas Gangrene (Clostridial Myonecrosis)
- Layer: Muscle
- Organisms: Clostridium perfringens (most important)
- Features: Severe pain, bronze/gray skin, crepitus, gas on X-ray, sweet/dishwater foul odor, rapid progression
- Treatment: Immediate surgery (amputation often needed) + high-dose penicillin G + clindamycin (blocks toxin production)
MRSA Skin Infections
Hospital admission rates for skin/soft tissue infections rose 27% between 2000-2004 due to emergence of USA300 clone of community-MRSA (CA-MRSA). This strain produces Panton-Valentine leukocidin (PVL) toxin, which causes leukocyte destruction and tissue necrosis.
CA-MRSA treatment of purulent skin infections:
- TMP-SMX DS (trimethoprim-sulfamethoxazole) - first line outpatient
- Doxycycline
- Clindamycin (check D-zone test for inducible resistance)
- Vancomycin (IV, severe)
CHAPTER 135 - INFECTIOUS ARTHRITIS
Authors: Nongnooch Poowanawittayakom, Lawrence C. Madoff
Overview
Most common bacterial causes: S. aureus, streptococci, N. gonorrhoeae
Acute bacterial infection can rapidly destroy articular cartilage - all inflamed joints must be evaluated without delay!
Pattern of Joint Involvement
| Pattern | Think |
|---|
| Acute monoarthritis | Bacterial (S. aureus, Strep) |
| Subacute/chronic monoarthritis | Mycobacterial or fungal |
| Episodic oligoarthritis | Syphilis, Lyme disease, reactive arthritis |
| Polyarthritis | Viral, disseminated gonococcal, endocarditis |
Route of Infection
- Hematogenous (most common) - bacteria escape from synovial capillaries (no limiting basement membrane) within hours
- Contiguous spread from adjacent bone/soft tissue
- Direct inoculation (surgery, injection, bite, trauma)
Synovial Fluid Analysis - CRITICAL TABLE
| Fluid Type | WBC/μL | PMNs | Appearance | Diagnosis |
|---|
| Normal | <180 | Rare | Clear | Normal |
| Non-inflammatory | <2000 | <25% | Yellow | OA, trauma |
| Inflammatory | 2000-50,000 | >50% | Cloudy | RA, crystal, reactive |
| Infectious (bacterial) | 25,000-250,000 (avg ~100,000) | >90% | Purulent | Bacterial arthritis |
| Mycobacterial/fungal | 10,000-30,000 | 50-70% | Cloudy | TB, fungal |
Gram stain: Positive in 30-50% of cases
Culture: Positive in >60% of non-gonococcal bacterial arthritis
MALDI-TOF mass spectrometry is useful when culture is negative but suspicion is high.
Gonococcal Arthritis
Most common cause of septic arthritis in young sexually active adults.
Two presentations:
- DGI (Disseminated Gonococcal Infection): Bacteremic phase - migratory polyarthralgia, tenosynovitis, skin lesions (pustules/vesicles), no joint effusion
- Purulent arthritis phase: Localized to 1-2 joints, no skin lesions
Diagnosis: NAAT (urine, cervical, rectal, pharyngeal) most sensitive; culture of joint fluid
Treatment: Ceftriaxone 1g IV/IM daily (resistance to fluoroquinolones is common now)
Prosthetic Joint Infections (PJI)
- Early (<3 months post-op): S. aureus, gram-negatives (intraoperative contamination)
- Delayed (3-24 months): Coagulase-negative staphylococci, Cutibacterium acnes
- Late (>24 months): Hematogenous seeding
Diagnosis: Sonication of explanted prosthetic joint - increases organism detection, especially if prior antibiotics within 14 days.
CHAPTER 136 - OSTEOMYELITIS
Overview
Osteomyelitis = infection of bone. Can be hematogenous, contiguous, or associated with vascular insufficiency.
Hematogenous Osteomyelitis
Adults: Vertebral osteomyelitis (most common site in adults)
- Organisms: S. aureus most common; gram-negatives (IV drug users, urinary source)
- Features: Back pain, fever, localized tenderness over spine
- Diagnosis: MRI (gold standard - shows marrow edema); bone biopsy for culture
- Complication: Epidural abscess → cord compression → EMERGENCY
Children: Long bones (metaphysis) - S. aureus, Group B Strep (neonates), Kingella kingae (toddlers)
Chronic Osteomyelitis
- Often follows hematogenous acute osteomyelitis or traumatic/surgical infection
- Sequestrum = dead bone (nidus for infection, must be removed)
- Involucrum = new periosteal bone formation around sequestrum
- Cloaca = opening from sequestrum to skin surface (draining sinus)
- Treatment: Surgical debridement + prolonged antibiotics (4-6 weeks)
Diabetic Foot Osteomyelitis
- Contiguous spread from infected foot ulcer
- Polymicrobial (S. aureus + gram-negatives + anaerobes)
- "Probe-to-bone test" - if metal probe hits bone through ulcer = high likelihood of osteomyelitis
- MRI superior to plain X-ray (changes take 10-21 days to appear on X-ray)
CHAPTER 137 - ABDOMINAL INFECTIONS AND ABSCESSES
Peritonitis
Primary (Spontaneous Bacterial Peritonitis - SBP):
- Occurs in cirrhosis with ascites
- Organism: Monomicrobial (E. coli, Klebsiella, Streptococcus pneumoniae)
- Diagnosis: Ascitic fluid PMN count ≥250/mm³
- Treatment: Cefotaxime 2g IV q8h x 5 days
- Prophylaxis: Norfloxacin/TMP-SMX (long-term in prior SBP) or ceftriaxone (acute GI bleed)
Secondary peritonitis: Perforated viscus, bowel leak
- Polymicrobial (E. coli, Bacteroides fragilis, Enterococcus, Clostridium)
- Treatment: Surgical source control + broad-spectrum antibiotics
Intraabdominal Abscesses
- Usually result from ruptured appendix, diverticulitis, Crohn's, post-surgical
- Polymicrobial (enteric gram-negatives + anaerobes)
- Treatment: Drainage (percutaneous or surgical) + antibiotics
- Drainage is essential - antibiotics alone rarely suffice
Liver Abscess
Pyogenic:
- Source: Portal vein bacteremia from bowel, biliary tract infection
- Organisms: E. coli, Klebsiella, Streptococcus milleri group, anaerobes
- CT shows hypodense lesion(s)
- Treatment: Percutaneous drainage + 4-6 weeks antibiotics
Amoebic (Entamoeba histolytica):
- Young adult male from endemic area
- "Anchovy sauce" pus (chocolate-colored)
- Right lobe, solitary
- Serology positive (>95% sensitive)
- Treatment: Metronidazole 750mg TID x 10 days (no drainage usually needed)
CHAPTER 138 - ACUTE INFECTIOUS DIARRHEAL DISEASES AND BACTERIAL FOOD POISONING
Authors: Ana A. Weil, Regina C. LaRocque
Pathogenic Mechanisms
1. Inoculum Size
Small dose causes disease:
- Shigella, E. coli O157, Giardia, Entamoeba: 10-100 organisms
- Vibrio cholerae: 10⁵-10⁸ organisms needed
This explains why Shigella/E. coli O157 spreads person-to-person while Salmonella needs to grow in food first.
2. Adherence
- V. cholerae adheres via toxin-coregulated pilus (TCP) and colonization factors
- EPEC and EHEC cause "attaching and effacing" lesions - destroy brush border microvilli
3. Toxin Production
| Toxin Type | Mechanism | Diarrhea type | Examples |
|---|
| Enterotoxin | Activates adenylyl cyclase → ↑cAMP → Cl⁻ secretion | Watery, profuse | Cholera toxin, LT of ETEC |
| Cytotoxin | Destroys mucosal cells | Bloody (dysentery) | Shiga toxin (STEC), C. difficile toxin B |
| Neurotoxin | Acts on CNS/peripheral NS | Variable | S. aureus enterotoxin, B. cereus |
4. Invasion
Pathogens invade mucosa causing inflammation:
- Shigella, Salmonella, EIEC, Yersinia invade colonic mucosa
- Campylobacter invades small bowel
Clinical Syndromes
| Syndrome | Location | Stool | Systemic Sx | Organisms |
|---|
| Watery diarrhea | Small bowel | Watery, voluminous | Dehydration | V. cholerae, ETEC, rotavirus, norovirus |
| Inflammatory diarrhea | Colon | Bloody, mucus, pus | Fever | Shigella, Salmonella, Campylobacter, EHEC |
| Enteric fever | Systemic | Variable | High fever, rose spots | Salmonella Typhi |
Bacterial Food Poisoning - Key Organisms
| Organism | Incubation | Source | Key Features |
|---|
| S. aureus enterotoxin | 1-6 hours (PREFORMED toxin) | Cream, salads, ham | Vomiting > diarrhea; no fever; self-limited |
| B. cereus emetic toxin | 1-6 hours | Fried rice | Vomiting (Chinese restaurant syndrome) |
| B. cereus diarrheal toxin | 8-16 hours | Meat, vegetables | Diarrhea |
| C. perfringens | 8-24 hours | Reheated meat | Diarrhea, cramping, no vomiting |
| C. botulinum | 18-36 hours | Canned food, honey (infants) | Descending flaccid paralysis, diplopia |
| Salmonella | 6-48 hours | Eggs, poultry | Bloody diarrhea, fever |
| E. coli O157:H7 (EHEC) | 1-8 days | Undercooked beef | HUS (hemolytic uremic syndrome) |
| Vibrio parahaemolyticus | 4-96 hours | Raw seafood | Watery diarrhea |
Memory trick for short incubation (preformed toxins): "STAPH doesn't need time" - 1-6 hours = S. aureus or B. cereus.
Treatment Approach
Most acute diarrhea: Supportive - oral rehydration solution (ORS)
ORS composition (WHO formula): Na 75 mmol/L, K 20 mmol/L, glucose 75 mmol/L, citrate 10 mmol/L
Antibiotics indicated for:
- Shigella (ciprofloxacin or azithromycin)
- Cholera (doxycycline - reduces duration)
- Typhoid (fluoroquinolone or ceftriaxone)
- Traveler's diarrhea (if severe: ciprofloxacin or azithromycin)
- C. difficile (see Ch. 139)
Avoid antibiotics for: EHEC/E. coli O157:H7 (increases HUS risk!), viral gastroenteritis, mild self-limited illness
CHAPTER 139 - CLOSTRIDIOIDES DIFFICILE INFECTION (CDI), INCLUDING PSEUDOMEMBRANOUS COLITIS
Authors: Dale N. Gerding, Stuart Johnson
Definition
CDI = colonic disease acquired most commonly with antimicrobial use and disruption of normal colonic microbiota. The most commonly diagnosed healthcare-associated diarrheal illness in the US.
Etiology and Epidemiology
- Organism: Obligately anaerobic, gram-positive, spore-forming bacillus
- Spores survive in environment for months and resist alcohol-based hand sanitizers
- Only hand-washing with soap and water removes spores effectively!
Antibiotics most associated with CDI:
- Clindamycin (historically first identified)
- Ampicillin/amoxicillin
- Second/third generation cephalosporins (cefotaxime, ceftriaxone, ceftazidime)
- Fluoroquinolones (most recent class - associated with hypervirulent NAP1/BI/027 strain)
Less risk: Penicillin/beta-lactamase inhibitor combinations (pip-tazo, ticarcillin-clavulanate)
Epidemiology:
- ~462,100 CDI cases in US in 2017
- Fecal colonization rate: Community 1-3% vs. Hospital >20% after >2 weeks
- Neonates: Frequently colonized but disease is extremely rare
Risk factors:
- Antibiotic use
- Older age
- Hospitalization / nursing home
- GI surgery
- Enteral tube feeding
- PPI use (modest risk)
- Prior CDI
Pathogenesis
Spores ingested → survive gastric acid → germinate in small bowel → (if microbiota disrupted) colonize colon → elaborate two major toxins:
| Toxin | Type | Mechanism |
|---|
| Toxin A | Enterotoxin | Intestinal fluid secretion; mucosal damage |
| Toxin B | Cytotoxin | Cell cytoskeleton destruction; more potent |
Both toxins glucosylate and inactivate Rho GTPases → cytoskeletal disruption → cell death → inflammation
NAP1/BI/027 hypervirulent strain also produces binary toxin - associated with more severe disease and increased mortality.
Pseudomembranes on colonoscopy: yellowish-white plaques (2-10mm) over inflamed mucosa - pathognomonic when present.
Clinical Spectrum
| Presentation | Features |
|---|
| Asymptomatic carriage | Common in neonates; also adults |
| Mild-moderate CDI | 3+ loose stools/day; cramping; low-grade fever |
| Severe CDI | WBC ≥15,000; creatinine >1.5x baseline; low albumin |
| Fulminant CDI (toxic megacolon) | Ileus; colonic distension >7cm; peritonitis; septic shock |
| Recurrent CDI | Return of symptoms within 8 weeks of documented cure |
Diagnosis
- NAAT (PCR): Very sensitive but does not distinguish colonization from infection - use with clinical judgment
- EIA for toxin A and B: Less sensitive but more specific for active disease
- Two-step algorithm: NAAT screen → EIA toxin confirmation (recommended in guidelines)
- Colonoscopy/sigmoidoscopy: Shows pseudomembranes; rarely needed but diagnostic
Treatment
| Severity | Treatment |
|---|
| Non-severe (1st episode) | Vancomycin oral 125mg QID x 10 days OR Fidaxomicin 200mg BD x 10 days (preferred; lower recurrence) |
| Severe | Vancomycin oral 125mg QID x 10 days |
| Fulminant | Vancomycin oral (high dose 500mg QID) + IV metronidazole 500mg TID; surgery if no improvement |
| Recurrent CDI | Vancomycin taper/pulse, or Fidaxomicin, or Bezlotoxumab + antibiotics |
Metronidazole is no longer first-line (inferior cure rates vs vancomycin). Use only in fulminant CDI as IV add-on.
Fecal Microbiota Transplantation (FMT): Highly effective (>90%) for multiply recurrent CDI.
Stop the offending antibiotic if possible.
Infection control: Contact precautions; soap-and-water handwashing; hypochlorite-based disinfectants for environment.
CHAPTER 140 - URINARY TRACT INFECTIONS: CYSTITIS, PROSTATITIS AND PYELONEPHRITIS
Pathogens
| UTI type | Most common organisms |
|---|
| Acute cystitis (women) | E. coli 75-90%, S. saprophyticus 5-15%, Klebsiella, Proteus |
| Pyelonephritis | Same as cystitis (ascending infection) |
| Catheter-associated UTI (CAUTI) | E. coli, P. aeruginosa, enterococci, S. aureus, Candida |
| Prostatitis | E. coli, other Enterobacterales; C. trachomatis (young men) |
Antimicrobial resistance concern: >20% resistance to TMP-SMX, fluoroquinolones, and nitrofurantoin in some US regions; ~9% ESBL-producing isolates.
Pathogenesis
Key factors promoting UTI:
- Flushing action of urination - primary host defense
- Obstructive uropathy - congenital anomalies, BPH, stones
- Sexual intercourse - risk increases with frequency (4.8x with 5x/week)
- Urinary instrumentation - catheters, nephrostomy tubes
- Disruption of urogenital microbiome - diaphragm/spermicide use, menopause
- Diabetes mellitus - 2-3x higher risk (impaired cytokine secretion, bladder dysfunction)
- SGLT-2 inhibitors - FDA safety warning for increased UTI risk (glucosuria)
Clinical Presentations
Acute Uncomplicated Cystitis
- Dysuria, frequency, urgency, suprapubic pain
- No fever (fever = suggests upper tract)
- Positive dipstick: leukocyte esterase and/or nitrites
- Urine culture: ≥10³ CFU/mL (significant in symptomatic women)
Treatment:
- Nitrofurantoin 100mg ER BD x 5 days (first line; not for pyelonephritis - poor renal tissue levels)
- TMP-SMX DS BD x 3 days (first line if local resistance <20%)
- Fosfomycin 3g single dose
- Fluoroquinolones - effective but reserve (high resistance, C. diff risk)
Acute Pyelonephritis
- Flank pain/tenderness (CVA tenderness)
- High fever, rigors
- Nausea/vomiting
- Bacteriuria + pyuria + casts in urine
- Blood cultures positive in ~20%
Treatment:
- Outpatient (uncomplicated): Ciprofloxacin 500mg BD x 7 days (if susceptibility known) or TMP-SMX x 14 days
- Inpatient: IV ceftriaxone or fluoroquinolone; switch to oral when improving
- Complicated / ESBL: Ertapenem or meropenem
Prostatitis
| Type | Features | Treatment |
|---|
| Acute bacterial | Fever, dysuria, tender boggy prostate; do NOT massage | Fluoroquinolone or TMP-SMX x 4 weeks |
| Chronic bacterial | Recurrent UTIs, perineal/pelvic pain | Fluoroquinolone x 6-12 weeks |
| Chronic pelvic pain syndrome (CPPS) | No bacteria on culture; most common | Alpha-blockers, NSAIDs, pelvic PT |
CHAPTER 141 - SEXUALLY TRANSMITTED INFECTIONS: OVERVIEW AND CLINICAL APPROACH
Overview
STIs affect >1 million people daily globally (WHO). Most common: chlamydia, gonorrhea, syphilis, herpes, HPV, HIV.
Major STIs Summary Table
| Organism | Disease | Key Features | Treatment |
|---|
| Chlamydia trachomatis (D-K) | Urethritis, cervicitis, PID | Asymptomatic in 70% of women; NAAT diagnosis | Doxycycline 100mg BD x 7 days (preferred) or Azithromycin 1g single dose |
| Neisseria gonorrhoeae | Gonorrhea | Urethral discharge, cervicitis; co-treat for Chlamydia | Ceftriaxone 500mg IM single dose |
| Treponema pallidum | Syphilis | See below | Benzathine penicillin G |
| HSV-2 (and HSV-1) | Genital herpes | Painful vesicles; latent in sacral ganglia; recurrent | Acyclovir/valacyclovir (suppressive or episodic) |
| HPV types 6,11 | Genital warts | Condylomata acuminata | Topical (podophyllin, imiquimod) or cryotherapy |
| HPV types 16,18 | Cervical/anal cancer | Precancerous; Pap smear/colposcopy | Vaccine prevention; surgical |
| Trichomonas vaginalis | Trichomoniasis | Frothy yellow-green discharge; strawberry cervix | Metronidazole 2g single dose |
Syphilis - Detailed
Stages:
| Stage | Features |
|---|
| Primary | Painless chancre (firm, clean, indurated ulcer) at site of inoculation; heals spontaneously in 3-6 weeks |
| Secondary | 6-8 weeks later; dissemination; maculopapular rash on PALMS AND SOLES (classic!); condylomata lata; mucous patches; lymphadenopathy; fever; alopecia |
| Latent | No symptoms; seropositive (early <1 year; late >1 year) |
| Tertiary | Years later: Cardiovascular (aortitis, aortic regurgitation), Neurosyphilis, Gummas |
Neurosyphilis:
- Early: Aseptic meningitis, cranial nerve palsies, iritis
- Late: Tabes dorsalis (posterior column degeneration), general paresis
Diagnosis:
- Screening: RPR or VDRL (non-treponemal; titers reflect disease activity; false positives common)
- Confirmation: FTA-ABS or TPHA (treponemal; remains positive lifelong)
Treatment:
- Primary/Secondary/Early latent: Benzathine penicillin G 2.4 MU IM single dose
- Late latent/unknown duration: 2.4 MU IM weekly x 3 doses
- Neurosyphilis: Aqueous penicillin G 18-24 MU/day IV x 10-14 days
- Penicillin allergy: Doxycycline 100mg BD x 14-28 days (not in pregnancy)
Pelvic Inflammatory Disease (PID)
- Ascending infection from lower genital tract
- Organisms: N. gonorrhoeae, C. trachomatis, anaerobes, M. hominis
- Clinical: Lower abdominal pain, cervical motion tenderness (Chandelier sign), adnexal tenderness, fever
- Complications: Tubo-ovarian abscess (TOA), chronic pelvic pain, ectopic pregnancy, infertility
Treatment:
- Outpatient: Ceftriaxone 500mg IM + doxycycline 100mg BD x 14 days ± metronidazole 500mg BD
- Inpatient (if severe/TOA): IV cefoxitin + doxycycline, or clindamycin + gentamicin
Chapters 142 - STIs Continued (specific organisms - see Ch 141 table)
CHAPTER 143 - ACUTE MENINGITIS
Definition
Meningitis = inflammation of the meninges (leptomeninges = pia + arachnoid). Bacterial meningitis is a medical emergency.
Common Causative Organisms by Age
| Age group | Top organisms |
|---|
| Neonates (<1 month) | Group B Streptococcus, E. coli, Listeria monocytogenes |
| Infants (1-3 months) | Group B Strep, E. coli, S. pneumoniae, N. meningitidis |
| Children/Adults | S. pneumoniae (most common), N. meningitidis |
| Elderly (>55) / Immunocompromised | S. pneumoniae, Listeria monocytogenes, gram-negatives |
| Post-neurosurgery / CSF shunt | S. aureus, coagulase-negative staphylococci, gram-negatives including P. aeruginosa |
Classic Clinical Triad (only 44% of patients have all three)
- Fever
- Neck stiffness (nuchal rigidity)
- Altered mental status
Other signs:
- Kernig's sign: Inability to extend knee when hip is flexed at 90°
- Brudzinski's sign: Passive neck flexion causes involuntary knee/hip flexion
- Photophobia, phonophobia
- Petechial/purpuric rash = meningococcal meningitis until proven otherwise!
Lumbar Puncture (LP) - CSF Analysis
| Parameter | Normal | Bacterial | Viral | Fungal/TB |
|---|
| Pressure (mmH₂O) | <200 | ↑↑ (>300) | Normal/↑ | ↑ |
| Appearance | Clear | Turbid/purulent | Clear | Clear/viscous |
| WBC | <5 | 1000-10,000 (PMN) | 10-1000 (lymph) | 25-500 (lymph) |
| Protein (mg/dL) | 15-45 | ↑↑ (100-500) | ↑ (50-200) | ↑ (100-500) |
| Glucose | 50-80 (=2/3 serum) | ↓↓ (<45, or <50% serum) | Normal | ↓ |
| Gram stain | Neg | + (60-90%) | Neg | Neg |
Contraindications to LP before CT: Papilledema, focal neurological signs, new seizures, immunocompromise, altered consciousness. If any present → CT first, then LP (but DO NOT delay antibiotics for CT!)
Empirical Treatment - The 60-Minute Goal
MEDICAL EMERGENCY: Start antibiotics within 60 minutes of patient arrival.
Do NOT delay antibiotics waiting for CT or LP results!
Standard empirical regimen (community-acquired):
- Ceftriaxone 2g IV q12h (covers S. pneumoniae, N. meningitidis, H. influenzae)
- + Vancomycin (covers cephalosporin-resistant S. pneumoniae)
- + Dexamethasone 0.15 mg/kg q6h x 4 days (give BEFORE or WITH first dose of antibiotic - reduces hearing loss and neurological sequelae in pneumococcal meningitis)
- + Acyclovir (covers HSV encephalitis in differential)
- + Doxycycline (during tick season - covers tick-borne organisms)
Add Ampicillin when Listeria is suspected:
- Age <3 months, age >55, pregnancy, immunocompromised
- Listeria is intrinsically resistant to cephalosporins!
Add Metronidazole:
- Patients with otitis, sinusitis, mastoiditis (risk of anaerobic infection)
Hospital-acquired/post-neurosurgery meningitis:
- Vancomycin + Meropenem (covers P. aeruginosa and resistant gram-negatives)
Pathogen-Specific Therapy (When Culture Known)
| Organism | Drug of Choice | Duration |
|---|
| S. pneumoniae (susceptible) | Penicillin G or amoxicillin | 10-14 days |
| S. pneumoniae (resistant) | Ceftriaxone + vancomycin | 10-14 days |
| N. meningitidis | Penicillin G | 7 days |
| Listeria | Ampicillin (± gentamicin) | 21 days |
| Gram-negative bacilli | Cefepime or meropenem | 21 days |
| P. aeruginosa | Meropenem | 21 days |
Complications
- Cerebral edema
- Cerebral herniation
- Hydrocephalus
- Vasculitis → stroke
- Subdural empyema
- Septic venous sinus thrombosis
- SIADH → hyponatremia
- Hearing loss (most common long-term complication, especially pneumococcal)
- Waterhouse-Friderichsen syndrome (meningococcal) = bilateral adrenal hemorrhage → adrenal crisis
CHAPTER 144 - CHRONIC AND RECURRENT MENINGITIS
Key Causes
| Category | Examples |
|---|
| Infectious | Tuberculous meningitis, Cryptococcal meningitis, Brucella, Lyme disease, Syphilis, HSV-2 (Mollaret's meningitis), Coccidioides |
| Malignant | Leptomeningeal carcinomatosis, lymphoma |
| Inflammatory/Autoimmune | Sarcoidosis, Behçet's disease, SLE, Sjögren's |
| Drug-induced | NSAIDs, TMP-SMX, IVIG |
| Granulomatous | Giant cell arteritis, Wegener's |
Tuberculous Meningitis (TBM) - Key Points
- Most lethal form of TB with high mortality/morbidity if untreated
- Subacute onset: weeks of headache, fever, weight loss → confusion, cranial nerve palsies
- CSF: Lymphocytic pleocytosis (100-400 cells), elevated protein, very low glucose, elevated ADA
- Diagnosis: AFB stain (low sensitivity <25%), culture (gold standard but slow), PCR (moderate sensitivity)
- Basal meningitis → basilar exudates → CN palsies (III, IV, VI especially)
- Hydrocephalus is common
Treatment: 2 months of HRZE + 7-10 months of HR (same as pulmonary TB but longer continuation phase)
Dexamethasone reduces mortality in confirmed TBM.
Cryptococcal Meningitis
- Classic in AIDS (CD4 <100 cells/μL), also organ transplant recipients
- Subacute/chronic headache, fever, minimal neck stiffness
- India ink stain of CSF - shows encapsulated yeasts (like halo around them)
- CSF cryptococcal antigen (CrAg) - highly sensitive/specific
- Elevated opening pressure - key management challenge (serial LP or lumbar drain)
Treatment:
- Induction: Liposomal amphotericin B + flucytosine x 2 weeks
- Consolidation: Fluconazole 400mg daily x 8 weeks
- Maintenance: Fluconazole 200mg daily (until immune reconstitution in HIV)
CHAPTER 145 - BRAIN ABSCESS (Encephalitis)
Note: Chapter 145 in Harrison's covers Brain Abscess.
Brain Abscess
Etiology by Source
| Source | Organisms |
|---|
| Sinusitis (frontal) | Streptococci (milleri group), anaerobes, gram-negatives |
| Dental/oral | Streptococci, Fusobacterium, Prevotella, anaerobes |
| Otitis/mastoiditis | Streptococci, Bacteroides, gram-negatives, Aspergillus |
| Hematogenous (bacteremia) | S. aureus (often multiple abscesses) |
| Post-traumatic/post-surgical | S. aureus, gram-negatives |
| HIV/Immunocompromised | Toxoplasma gondii (most common CNS lesion in AIDS), Cryptococcus, Aspergillus |
Clinical Features
- Headache (most common, >70%)
- Fever (only 50% - often absent in brain abscess!)
- Focal neurological deficits
- Seizures
- Signs of raised ICP
- Classic triad of fever, headache, focal deficit in only 20%
Diagnosis
- MRI with gadolinium - superior to CT
- Ring-enhancing lesion with surrounding edema
- Single lesion: Suspect bacterial abscess or primary tumor
- Multiple ring-enhancing lesions in AIDS: Toxoplasma vs. CNS lymphoma
Toxoplasma vs. CNS Lymphoma in AIDS:
| Feature | Toxoplasma | CNS Lymphoma |
|---|
| Lesions | Multiple | Single (often) |
| Location | Basal ganglia | Periventricular |
| Toxo serology | Usually positive | Negative |
| Response to empiric anti-Toxo therapy | Improves in 1-2 weeks | No improvement |
Treatment of Bacterial Brain Abscess
- Aspiration/drainage (surgical) - provides diagnosis AND treatment; essential if >2.5cm
- Antibiotics (6-8 weeks):
- Empirical: Ceftriaxone + metronidazole + vancomycin
- Post-neurosurgery/trauma: Vancomycin + cefepime or meropenem
- Dexamethasone - use only if severe mass effect (may impair antibiotic penetration)
- Antiepileptic drugs - for seizures
CHAPTER 146 - INFECTIOUS COMPLICATIONS OF BITES
Authors: Nongnooch Poowanawittayakom, Lawrence C. Madoff
Overview
Bites breach the skin barrier and inoculate the oral flora of the biting animal into deeper tissues. Infection risk reflects the oropharyngeal flora of the biting animal.
Dog Bites
- >4.7 million dog bites/year in US; responsible for 80% of all animal bites
- 15-20% of dog bites become infected
- Children most common victims (boys 5-9 highest risk)
- Infection manifests 8-24h after bite: cellulitis, purulent discharge, pain
Microbiology (mixed, typically):
- Pasteurella multocida
- β-hemolytic streptococci
- Staphylococcus spp. (including MRSA)
- Neisseria species
- Eikenella corrodens
- Capnocytophaga canimorsus - splenectomized/immunocompromised patients at very high risk of fatal septicemia!
- Anaerobes: Bacteroides, Fusobacterium, Prevotella
Life-threatening: Bacteremia, meningitis, brain abscess, endocarditis, especially in immunocompromised hosts.
Cat Bites
- Cat bites become infected in 30-50% (higher rate than dogs because sharper, deeper puncture wounds)
- Most important organism: Pasteurella multocida - very common in cat bite infections; rapid onset (within 12h), intense pain, erythema, swelling
- Also: streptococci, staphylococci, anaerobes, Bartonella henselae (cat-scratch disease)
Cat-Scratch Disease (Bartonella henselae):
- Cat scratch or bite (especially from kittens)
- 1-3 week incubation
- Regional lymphadenopathy (tender, may suppurate)
- Low-grade fever, malaise
- Diagnosis: Serology or PCR
- Treatment: Self-limited; azithromycin for lymphadenitis
Human Bites
- Highest infection rate of any bite (human oral flora is the most diverse and pathogenic)
- Two types:
- Occlusal/true bite - directly inflicted
- Fight bite / Clenched-fist injury (CFI) - knuckles striking teeth; highly dangerous; often involves joint space
Microbiology:
- Streptococcus spp.
- Staphylococcus aureus
- Eikenella corrodens (characteristic of human bites; not in animal bites)
- Anaerobes: Fusobacterium, Prevotella, Peptostreptococcus
Clenched-fist injury warning: Often presents late, underestimated severity. Can rapidly lead to septic arthritis, osteomyelitis, tenosynovitis - requires surgical debridement and hospitalization.
Snake Bites
- Venomous vs. non-venomous
- Local infection risk: mouth flora of snake; Gram-negatives (Morganella, Aeromonas, Providencia) + anaerobes
- Treatment of envenomation: antivenom; supportive care
- Antibiotic prophylaxis is NOT routinely recommended for all snake bites
General Bite Wound Management
"ABCDE" of bite management:
- Assess wound depth, contamination, neurovascular status
- Blood cultures if systemic signs
- Clean thoroughly - copious irrigation with saline (most important step)
- Debride devitalized tissue
- Empirical antibiotics
Prophylactic antibiotics for:
- All cat bites
- Dog bites: moderate-severe, hands/face/genitals, immunocompromised, asplenic, diabetic, edematous areas
- All human bites
Drug of choice: Amoxicillin-clavulanate (covers Pasteurella, Eikenella, anaerobes, streptococci, staphylococci)
- Penicillin allergy: Doxycycline + metronidazole, OR moxifloxacin
Wound closure:
- Generally leave open for infected or high-risk bites
- Face bites: can close primarily (good blood supply, cosmetic importance)
Rabies prophylaxis: Consider for all animal bites - assess risk based on animal species, geographic location, behavior. Unvaccinated: HRIG + rabies vaccine series.
Tetanus: Update if not vaccinated within 5 years (bites); give tetanus immunoglobulin if no prior immunization.
🧠 QUICK-RECALL MNEMONICS
CURB-65 (Pneumonia severity)
Confusion, Urea >7, Respiratory rate ≥30, BP low, 65 years
Duke Criteria for IE - MAJOR = "HERO"
Hemo-culture (typical organisms), Echocardiogram evidence, Regurgitation (new), Other: none - only 3 major criteria
C. diff Risk Antibiotics - "CAFF"
Cephalosporins, Ampicillin, Fluoroquinolones, F... clindamycin (the original)
Meningitis Organisms by Age
- Neonates: "Group B Strep, E. coli, Listeria" = "BEL (Beautiful Early Life)"
- Adults: "S. pneumo, N. meningitidis" = the two most common
Syphilis Rash Memory
"Syphilis does not spare the PALMS and SOLES" (secondary syphilis = palms + soles rash; Rocky Mountain Spotted Fever also = palms + soles!)
NF (Necrotizing Fasciitis) Red Flags
"Pain Out Of Proportion" = POOP sign = always think NF!
Bite Wound Drug
"Amox-Clav for ALL bites" (covers the spectrum)
📊 MASTER COMPARISON TABLE
| Disease | Key Bug | Key Drug | Emergency? |
|---|
| CAP | S. pneumoniae | Azithromycin / Amoxicillin | If ICU |
| HAP/VAP | P. aeruginosa, MRSA | Pip-tazo + Vancomycin | Yes |
| Legionella | L. pneumophila | Azithromycin / Levofloxacin | If severe |
| Endocarditis | S. aureus | Vancomycin (MRSA) / Nafcillin (MSSA) | Surgery if HF |
| Necrotizing Fasciitis | Group A Strep / Mixed | Pip-tazo + Vancomycin + Clindamycin | YES - Immediate surgery |
| Cellulitis | S. aureus, Strep | Cephalexin / Vancomycin | No |
| Bacterial Arthritis | S. aureus, Gonorrhea | Vancomycin / Ceftriaxone | Joint drainage |
| Osteomyelitis | S. aureus | Vancomycin → transition | Surgery if chronic |
| SBP | E. coli, Klebsiella | Cefotaxime | Yes |
| Acute Diarrhea | Norovirus, Shigella | Rehydration / Ciprofloxacin | Dehydration risk |
| C. difficile | C. difficile | Vancomycin oral / Fidaxomicin | If toxic megacolon |
| Cystitis | E. coli | Nitrofurantoin / TMP-SMX | No |
| Pyelonephritis | E. coli | Ciprofloxacin / Ceftriaxone | If sepsis |
| Gonorrhea | N. gonorrhoeae | Ceftriaxone 500mg IM | If DGI |
| Bacterial Meningitis | S. pneumoniae | Ceftriaxone + Vancomycin + Dexamethasone | YES - 60 min |
| TBM | M. tuberculosis | HRZE x 2m + HR x 7-10m | Yes |
| Cryptococcal meningitis | C. neoformans | Amphotericin B + Flucytosine | Yes |
| Brain Abscess | Strep milleri, anaerobes | Ceftriaxone + Metro + Vancomycin + Drainage | Yes |
| Dog Bite | Pasteurella, Capnocytophaga | Amoxicillin-clavulanate | If immunocompromised |
| Human Bite | Eikenella, Strep | Amoxicillin-clavulanate | CFI = surgery |
All content above is from Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill Medical) - Chapters 131-146, supplemented by your medical knowledge.
This guide covers all 16 chapters you asked about. Here is how to use it for maximum retention:
- Images help anchor the anatomy - the skin layer diagram is especially important for understanding why erysipelas vs cellulitis vs NF differ clinically.
- Tables let you rapidly compare organisms, CSF findings, and treatments.
- Mnemonics at the end help on exam day.
- Focus especially on the emergency conditions: Meningitis (60-min rule), Necrotizing Fasciitis (immediate surgery), and Bacterial Endocarditis (surgical indications).
Good luck becoming a great doctor! 🩺