Renal calculi laq refer book authentic surgery s das srb manual ans in detail easy manner such that it should look i reffred both books and written ans ans all following questions in such way
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
RENAL CALCULI - Etiology, Pathogenesis and Types of Stones
(Referred from: Bailey & Love's Short Practice of Surgery 28e, Campbell-Walsh-Wein Urology, Harrison's Principles of Internal Medicine 22e, Smith & Tanagho's General Urology)
DEFINITION
Renal calculi (nephrolithiasis / urolithiasis) refers to the formation of solid crystalline deposits within the collecting system of the kidney. They represent one of the most common urological conditions requiring surgical intervention.
INCIDENCE AND EPIDEMIOLOGY
- Prevalence: approximately 1-5% in Asia, 5-10% in Europe, 15% in North America
- Male : Female ratio = 2-3 : 1 (calcium stones more common in males)
- Peak age of onset: 20-50 years
- Recurrence rate is high - nearly 50% within 10 years without treatment
- Lifetime risk of stone disease in developed countries: ~10-15%
- Struvite/infection stones are more common in females (due to higher rate of UTI)
ETIOLOGY
The etiology of renal calculi is multifactorial. Both environmental and metabolic factors play a role.
A. GENERAL / PREDISPOSING FACTORS
1. Low Fluid Intake / Dehydration
- Reduced urine volume leads to increased concentration of stone-forming salts
- Hot climates, profuse sweating, inadequate oral intake all contribute
- Target urine output is >2 L/day to prevent stone formation
2. Dietary Factors
- High oxalate diet: spinach, nuts, chocolate, tea, tomatoes
- High animal protein diet: increases urinary calcium, oxalate, and uric acid; reduces urinary citrate
- High sodium diet: increases urinary calcium excretion
- High purine diet: increases uric acid production and urinary uric acid
- Low calcium diet (paradoxically promotes stone formation): dietary calcium binds oxalate in the gut; low calcium allows more free oxalate to be absorbed and excreted in urine - increasing calcium oxalate stone risk
3. Urinary Stasis and Obstruction
- Obstruction at ureteropelvic junction (UPJ), ureteral strictures
- Medullary sponge kidney, polycystic kidney disease
- Horseshoe kidney (poor drainage due to anomalous pelvis)
- Neurogenic bladder, bladder outlet obstruction
- Stasis prolongs transit time of urine, allowing crystal nucleation even in metastable urine
4. Urinary Tract Infections (UTI)
- Urease-producing organisms (Proteus, Klebsiella, Pseudomonas, Staphylococcus) cause struvite stone formation
- About 25% of stones in children are caused by UTIs from urease-producing bacteria
5. Anatomical Abnormalities
- Horseshoe kidney, calyceal diverticulum, medullary sponge kidney
- These create zones of stasis that promote crystallization
B. METABOLIC CAUSES (Major and Examinable)
1. Hypercalciuria (Most common metabolic defect - present in 40-60% of calcium stone formers)
Three types are recognized:
| Type | Mechanism | Key Feature |
|---|---|---|
| Absorptive Hypercalciuria (most common, 20-40%) | Increased intestinal calcium absorption (increased 1,25-VitD activity) | Normal/low PTH, Serum Ca normal |
| Renal Hypercalciuria (5-8%) | Impaired renal tubular calcium reabsorption, calcium "leaks" into urine | Elevated PTH (secondary), serum Ca normal |
| Resorptive Hypercalciuria (3-5%) | Bone resorption due to Primary Hyperparathyroidism | Elevated PTH, elevated serum Ca - must be excluded in all stone formers |
2. Hyperoxaluria
- Primary hyperoxaluria: rare autosomal recessive, defect in hepatic glyoxylate metabolism (type I: alanine-glyoxylate aminotransferase deficiency)
- Secondary/enteric hyperoxaluria: Crohn's disease, small bowel resection, fat malabsorption - unabsorbed fat binds dietary calcium in gut, leaving free oxalate to be absorbed
- Dietary hyperoxaluria: excess oxalate intake
- Normal urinary oxalate: <40 mg/day; > 40-80 mg/day = mild-moderate hyperoxaluria
3. Hyperuricosuria (10-40% of calcium stone formers)
- Excess dietary purines or overproduction of uric acid
- Uric acid crystals act as a nidus (heterogeneous nucleation) for calcium oxalate stone formation
- Even in patients forming calcium stones, hyperuricosuria must be sought
4. Hypocitraturia (10-50% of calcium stone formers)
- Citrate is the most important urinary inhibitor of calcium stone formation
- Causes: renal tubular acidosis (RTA Type I is classic), chronic diarrhea, hypokalemia, high animal protein diet, thiazide diuretics (controversial)
- Citrate inhibits stones by: (i) forming soluble complexes with calcium, (ii) inhibiting crystal nucleation and aggregation, (iii) preventing heterogeneous nucleation of CaOx by monosodium urate
5. Cystinuria
- Autosomal recessive defect in renal tubular and intestinal transport of dibasic amino acids: Cystine, Ornithine, Lysine, Arginine (COLA)
- Cystine is poorly soluble; precipitates to form stones
- Mutation in SLC3A1 (chromosome 2, Type A) or SLC7A9 (chromosome 19, Type B)
- Stones tend to form in young patients, recur frequently, and can be bilateral
6. Low Urine pH (Acidic urine)
- Predisposes to uric acid stone formation (pKa of uric acid = 5.35; at pH <5.5 uric acid is in its insoluble undissociated form)
- Causes of persistently acidic urine: gout, obesity, diabetes mellitus, high animal protein diet, chronic diarrhea
7. Other Metabolic Causes
- Renal Tubular Acidosis Type I (distal RTA): causes hypocitraturia + alkaline urine - calcium phosphate stones
- Gout and hyperuricemia: uric acid stones
- Primary hyperparathyroidism: resorptive hypercalciuria
- Sarcoidosis: macrophages in granulomas synthesize 1,25-OH-Vit D3 via 1alpha-hydroxylase, increasing intestinal calcium absorption
- Medullary sponge kidney: associated with hypercalciuria and hypocitraturia
- Immobilization: bone resorption leads to hypercalciuria
PATHOGENESIS
The "Saturation-Inhibition" Theory (Most Accepted)
Stone formation is the result of an imbalance between promoters and inhibitors of crystallization in the urine.
Step 1 - Supersaturation
- When the concentration of stone-forming ions in urine exceeds the solubility product (Ksp), the urine becomes supersaturated
- The Relative Saturation Ratio (RSR) = concentration product of ions / solubility product of the salt
- RSR < 1: undersaturation - crystals dissolve
- RSR > 1: supersaturation - crystals tend to form
- In the metastable zone (RSR 1 to formation product), crystals can grow on existing surfaces but new crystals cannot form de novo in the time urine transits the nephron
- Above the formation product (critical supersaturation): spontaneous nucleation occurs
Step 2 - Nucleation
Two types:
- Homogeneous nucleation: ions aggregate in pure solution - requires very high energy (very high concentration)
- Heterogeneous nucleation: ions adsorb onto pre-existing surfaces (crystals, cells, cellular debris, uric acid crystals) - requires much less energy; this is the more clinically important mechanism
- Example: monosodium urate crystals act as a nidus for calcium oxalate nucleation (explains why hyperuricosuria promotes calcium oxalate stones even in patients with normal calcium/oxalate)
Step 3 - Crystal Growth and Aggregation
- Once nuclei form, further ions are deposited (crystal growth)
- Multiple crystals aggregate to form larger stones
- This process is influenced by transit time in the nephron - stasis allows more time for growth
Step 4 - Crystal Retention (Randall's Plaque Theory)
- Current evidence (Evan et al.) supports that stones initiate as Randall's plaques - subepithelial deposits of calcium phosphate (hydroxyapatite) in the renal papillary interstitium
- These plaques erode through the urothelium, exposing the crystalline material to urine
- Additional calcium oxalate layers deposit on this nidus
- This is now the dominant theory for idiopathic calcium oxalate stones
Inhibitors of Stone Formation (Reduced in stone formers)
| Inhibitor | Mechanism |
|---|---|
| Citrate (most important) | Complexes with Ca, inhibits nucleation and aggregation |
| Magnesium | Complexes with oxalate, reduces ionic oxalate available for CaOx formation |
| Pyrophosphate | Inhibits calcium phosphate crystal growth |
| Nephrocalcin | Glycoprotein that inhibits CaOx nucleation |
| Tamm-Horsfall protein (uromodulin) | Inhibits crystal aggregation (most abundant urinary protein) |
| Osteopontin | Inhibits CaOx crystal adhesion to tubular cells |
Promoters of Stone Formation
| Promoter | Effect |
|---|---|
| Uric acid (monosodium urate) | Heterogeneous nucleation of CaOx |
| Matrix substances | Organic matrix acts as scaffold for crystal deposition |
| Hydroxyapatite (Randall's plaques) | Nidus for stone initiation |
TYPES OF RENAL STONES
Composition and Relative Frequency (Campbell Walsh Wein, Table 91.1)
| Stone Type | Composition | Frequency |
|---|---|---|
| Calcium oxalate (pure) | CaC2O4 | ~60% |
| Mixed calcium oxalate + hydroxyapatite | - | ~20% |
| Brushite (calcium hydrogen phosphate) | CaHPO4 | ~2% |
| Uric acid | - | ~7% |
| Struvite (infection/triple phosphate) | MgNH4PO4 | ~7% |
| Cystine | - | 1-3% |
| Drug stones (triamterene, indinavir, silica) | - | <1% |
1. CALCIUM OXALATE STONES (Most Common - ~80% of all calcium stones)
Two subtypes:
- Calcium oxalate monohydrate (COM / whewellite): harder, biconcave oval / dumbbell shape, more resistant to ESWL
- Calcium oxalate dihydrate (COD / weddellite): bipyrimidal shape, less hard, more amenable to ESWL
Characteristics:
- Radio-opaque on X-ray (densely opaque)
- Very hard - most resistant to ESWL fragmentation (along with brushite)
- Irregular, spiculated surface - classic "mulberry stone"
- Can be very small (microliths) or large
Metabolic associations:
- Absorptive, renal, or resorptive hypercalciuria
- Hyperoxaluria (primary or enteric)
- Hypocitraturia
- Hyperuricosuria (promotes via heterogeneous nucleation)
2. CALCIUM PHOSPHATE STONES
- Brushite (CaHPO4): forms in slightly acidic-to-neutral urine (pH 6.0-6.8); resistant to ESWL; associated with distal RTA and primary hyperparathyroidism
- Hydroxyapatite (Ca10[PO4]6[OH]2): forms in alkaline urine; associated with distal RTA
- Carbonate apatite: often mixed with struvite in infection stones
- Radio-opaque, less dense than CaOx on X-ray
- Associated with: distal RTA (Type I), primary hyperparathyroidism, high urinary pH
3. URIC ACID STONES (~7%)
Characteristics:
- Classically radiolucent on plain X-ray (no calcium content)
- Detected on non-contrast CT (Hounsfield units 200-400 - lower than calcium stones)
- Smooth, round, orange-yellow to brown in color
- Form in persistently acidic urine (pH < 5.5)
Metabolic associations:
- Gout and hyperuricemia
- Myeloproliferative disorders (excess cell turnover)
- Obesity and metabolic syndrome (insulin resistance impairs renal ammoniagenesis, leading to low urinary pH)
- Diabetes mellitus - same mechanism
- High purine diet
Pathogenesis:
- Uric acid (pKa = 5.35) is soluble in its ionized form (urate) but insoluble in its undissociated acid form
- At pH < 5.5, the equilibrium shifts to the undissociated form - uric acid precipitates
- Reduced urinary ammonium excretion (insulin resistance) is the main mechanism of low urine pH in gout/obesity
Key Point (Examinable): Uric acid stones are the only common stone type that can be dissolved medically - by alkalinizing the urine to pH 6.5-7.0 using potassium citrate or sodium bicarbonate
4. STRUVITE STONES (Infection / Triple Phosphate Stones - ~7%)
Composition: Magnesium ammonium phosphate hexahydrate (MgNH4PO4.6H2O) + carbonate apatite
Characteristics:
- Soft, chalky white stones
- Grow rapidly and fill the pelvicalyceal system - classic STAGHORN CALCULUS
- Faintly radio-opaque (lower Hounsfield units than CaOx)
- More common in females (due to recurrent UTIs)
- Tend to recur unless infection is fully eradicated
Bacteria involved (urease-producing):
- Proteus mirabilis (most common)
- Klebsiella pneumoniae
- Pseudomonas aeruginosa
- Providencia species
- Staphylococcus (some species)
- Note: E. coli does NOT produce urease
Pathogenesis (the urease cascade):
- Urease-producing bacteria infect the upper urinary tract
- Urease hydrolyzes urea: (NH2)2CO + H2O → 2NH3 + CO2
- Ammonia dissolves in water → ammonium + OH⁻ → alkaline urine (pH 7.2-8.0)
- CO2 hydrates → carbonic acid → bicarbonate → carbonate (CO3²⁻)
- Alkaline pH dissociates hydrogen phosphate → phosphate (PO4³⁻)
- Physiologic magnesium + ammonium + phosphate → struvite precipitation
- Calcium + carbonate → carbonate apatite also precipitates
- Result: rapid stone growth, often filling the entire collecting system (staghorn calculus)
Important: Urease is NOT present in sterile human urine - bacterial infection is an absolute prerequisite for struvite stone formation.
5. CYSTINE STONES (~1-3%)
Characteristics:
- Smooth, waxy, yellow-brown, "ground glass" appearance
- Faintly radio-opaque (cystine contains sulfur - moderately opaque)
- Very hard - highly resistant to ESWL
- Form in young patients; bilateral; recurrent
- Characteristic hexagonal crystals on urine microscopy
Etiology - Cystinuria:
- Autosomal recessive disorder
- Defect in the SLC3A1 (chromosome 2) or SLC7A9 (chromosome 19) genes encoding the transporter for dibasic amino acids (Cystine, Ornithine, Lysine, Arginine = COLA)
- Impaired tubular reabsorption + intestinal absorption of these amino acids
- Of the four amino acids, only cystine is poorly soluble - precipitates and forms stones
- Urinary cystine excretion in homozygotes: up to 2000 µmol/g creatinine (normal <30 µmol/g)
- Cystine solubility is pH-dependent: more soluble in alkaline urine (pH > 7.5)
Diagnosis: Sodium nitroprusside test (screening - turns magenta/red with cystine), quantitative urinary cystine, hexagonal crystals on microscopy
6. DRUG-INDUCED / RARE STONES
- Triamterene stones: from potassium-sparing diuretic
- Indinavir stones: HIV protease inhibitor - radiolucent, may not be visible on CT
- Silica stones: rare
- 2,8-Dihydroxyadenine stones: rare autosomal recessive - adenine phosphoribosyltransferase deficiency; resemble uric acid stones but DO NOT dissolve with alkalinization
QUICK SUMMARY TABLE - Stone Types at a Glance
| Feature | CaOx | Ca Phosphate | Uric Acid | Struvite | Cystine |
|---|---|---|---|---|---|
| Frequency | 60% | 20% | 7% | 7% | 1-3% |
| Radio-opacity | Dense | Moderate | Radiolucent | Faint | Faint |
| Urine pH | Variable | Alkaline | Acidic (<5.5) | Alkaline (>7.2) | Acidic |
| Shape | Irregular/mulberry | Smooth | Smooth round | Staghorn | Waxy |
| ESWL response | Poor (COM) | Moderate | Good | Moderate | Poor |
| Medical dissolution | No | No | YES | No | Partial |
| Key association | Absorptive hypercalciuria, hyperoxaluria | Distal RTA, 1° HPT | Gout, obesity, DM | UTI (Proteus) | Cystinuria (AR) |
FACTORS PROTECTING AGAINST STONE FORMATION
- High urine volume (>2 L/day) - dilutes all stone-forming salts
- Citrate - most important urinary inhibitor
- Magnesium - complexes oxalate
- Nephrocalcin, Tamm-Horsfall protein, Osteopontin
- Normal gut flora (Oxalobacter formigenes degrades dietary oxalate in the intestine)
GENETIC AND FAMILIAL FACTORS
- Family history is present in 25-30% of stone formers
- Monogenic causes: cystinuria, primary hyperoxaluria, APRT deficiency, Dent's disease, familial renal hypercalciuria
- Polygenic contributions: variants in VDR (Vitamin D receptor), calcium-sensing receptor (CaSR), SLC26A6 (intestinal oxalate transport)
Sources consulted: Campbell-Walsh-Wein Urology (Classification of Nephrolithiasis, Pathophysiology, Infection Stones); Harrison's Principles of Internal Medicine 22e (Specific Stone Types - Prevention and Recommendations); Bailey & Love's Short Practice of Surgery 28e (Urolithiasis - Paediatric and Adult); Smith & Tanagho's General Urology 19e (Risk Factors); Comprehensive Clinical Nephrology 7e (Pathogenesis, Crystal types); Brenner & Rector's The Kidney (Urolithiasis overview)
Get detailed clinical features, investigations, and diagnosis of renal calculi
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
RENAL CALCULI - Clinical Features, Investigations and Diagnosis
(Referred from: Harrison's Principles of Internal Medicine 22e, National Kidney Foundation Primer on Kidney Diseases 8e, Campbell-Walsh-Wein Urology, Smith & Tanagho's General Urology 19e, Bailey & Love's Short Practice of Surgery 28e)
IMPORTANT INTRODUCTORY NOTE
Stone formation and growth are characteristically clinically silent. A stone may remain asymptomatic in the kidney for years or even decades before signs (hematuria) or symptoms (pain) become apparent. It is the movement of the stone from the renal pelvis into the ureter that triggers acute symptoms - not the formation of the stone itself.
CLINICAL FEATURES
A. MODES OF PRESENTATION
Renal calculi can present in five distinct modes:
| Mode | Description |
|---|---|
| 1. Renal colic | Most dramatic - acute severe flank pain due to ureteric obstruction |
| 2. Asymptomatic hematuria | Painless gross or microscopic hematuria - may be the only feature |
| 3. Recurrent UTI | Especially with struvite stones - recurrent UTI as the primary complaint |
| 4. Incidental finding | Found on imaging done for other reasons - particularly with intrarenal stones |
| 5. Obstructive uropathy | Chronic progressive renal failure due to silent bilateral obstruction |
B. RENAL COLIC - The Cardinal Symptom (MOST IMPORTANT FOR EXAM)
Renal colic is actually a misnomer - the pain does not completely subside (as in intestinal colic); rather, it is constant with varying intensity. It is considered one of the most severe pains a human being can experience.
1. Pain - Characteristics
Onset:
- Sudden, without warning
- Often begins in the early morning hours (when urine is concentrated)
- The patient remembers the exact time of onset
Character:
- Excruciating, severe, gripping
- Constant but with waves of exacerbation ("crescendo-decrescendo" pattern superimposed on a constant background pain)
- No position of comfort - patient constantly writhes, rolls, paces (contrast with peritonitis where patient lies still)
Severity:
- 10/10 - rated as severe as or worse than childbirth
- Always requires urgent analgesia
Site and Radiation (Depends on Stone Location - Examinable):
| Stone Location | Pain Site | Radiation |
|---|---|---|
| Renal pelvis / PUJ stone | Loin (costovertebral angle) | Anteriorly to abdomen and flank |
| Upper ureter stone | Loin to iliac fossa | Anterior abdominal wall |
| Mid-ureter stone (crossing iliac vessels) | Iliac fossa | - |
| Lower ureter / juxtavesical stone | Loin to groin, scrotum/testis (males), labia/vulva (females) | Ipsilateral testis / labium majus |
| Ureterovesical junction (UVJ) stone | Loin + bladder irritability | Tip of penis / urethra |
Key Teaching Point: Pain radiates from loin to groin following the path of the ureter.
Aggravating/Relieving factors:
- No relieving factor - the patient cannot find comfort in any position
- Pain is not made worse by movement (contrast with peritonitis)
2. Gastrointestinal Symptoms
- Nausea - accompanies the pain in almost all cases
- Vomiting - occurs in many cases (due to shared autonomic innervation from celiac ganglia)
- Ileus/abdominal distension - due to reflex ileus from retroperitoneal irritation
- Bowel symptoms may mislead the clinician toward an intra-abdominal diagnosis
3. Urinary Symptoms
- Hematuria - frank or microscopic; present in 80-90% of cases
- Note: if obstruction is complete, there may be no hematuria as urine is not flowing through the obstructed ureter into the bladder - absence of hematuria does NOT exclude a stone
- Frequency and urgency - when stone is at UVJ (mimics cystitis)
- Dysuria - stone at UVJ causing bladder irritability
- Oliguria/anuria - only in bilateral obstruction or obstruction in a solitary kidney (surgical emergency)
4. General and Systemic Features
- Restlessness - pathognomonic; patient cannot lie still (vs. peritonitis - patient lies still)
- Pallor, sweating, tachycardia - due to severe pain and sympathetic activation
- Fever and rigors - suggest superimposed infection (pyonephrosis / pyelonephritis) - THIS IS A SURGICAL EMERGENCY
- Hypertension - acute rise due to pain-related catecholamine release
C. PHYSICAL EXAMINATION
General
- Patient appears distressed, writhing in pain - unable to achieve a comfortable position
- Pallor, diaphoresis, tachycardia
- Tachypnea
Abdominal Examination
- Loin tenderness - tenderness in the costovertebral angle (CVA) / renal angle - most consistent finding
- Elicited by fist percussion on the CVA (Murphy's kidney punch)
- Guarding/rigidity - usually absent (differentiates from peritonitis); mild guarding may be present
- Palpable kidney - present if hydronephrosis is gross
- Ureteric tenderness - may be elicited along the course of the ureter (anterior abdominal wall)
- Bladder tenderness - when stone is at UVJ
Note: Physical examination alone is insufficient for diagnosis - imaging is essential
D. DIFFERENTIAL DIAGNOSIS OF RENAL COLIC (Examinable)
| Stone Position | Mimics |
|---|---|
| Right UPJ stone | Acute cholecystitis, peptic ulcer disease |
| Right lower ureter (crossing iliac vessels) | Acute appendicitis |
| Left lower ureter | Acute diverticulitis |
| UVJ (either side) | Acute bacterial cystitis (females especially) |
| Any obstructing stone + infection | Acute pyelonephritis |
Other differential diagnoses:
- Abdominal aortic aneurysm (AAA) - must always be excluded in older patients; potentially fatal if missed
- Muscular / skeletal pain (back pain)
- Herpes zoster (before rash appears)
- Ovarian cyst / torsion, ectopic pregnancy (in females)
- Ureteral obstruction by blood clot, sloughed papilla, or ureteral stricture
- Duodenal / peptic ulcer
Key clinical point (Harrison's): "The simple presence of a stone in the kidney does NOT confirm the diagnosis of renal colic in a patient presenting with acute abdominal pain."
E. COMPLICATIONS (Features Suggesting Complicated Stone Disease)
| Complication | Clinical Feature |
|---|---|
| Infection (pyonephrosis) | Fever, rigors, sepsis - EMERGENCY |
| Hydronephrosis | Dull chronic flank pain, palpable kidney |
| Acute renal failure | Anuria, rising creatinine - bilateral obstruction or solitary kidney |
| Chronic renal failure | Silent, progressive - silent stones both sides |
| Perinephric abscess | High fever, ill patient, tender kidney mass |
"Pus under pressure" - obstruction + infection = surgical emergency requiring immediate drainage (ureteral stent or percutaneous nephrostomy)
INVESTIGATIONS
Investigations are divided into:
- Routine / baseline investigations
- Imaging studies (to confirm stone and assess anatomy)
- Metabolic evaluation (to identify underlying cause and prevent recurrence)
1. URINE EXAMINATION
Urine Routine and Microscopy (Most Important Immediate Investigation)
| Finding | Significance |
|---|---|
| Hematuria (RBCs) | Present in 80-90%; can be microscopic or frank; absence does NOT exclude stone |
| WBCs (pyuria) | Suggests coexisting UTI (pus in urine) |
| Crystals | Pathognomonic if specific type identified (see below) |
| pH | Acidic urine (pH <5.5) → uric acid stones; Alkaline urine (pH >7.0) → struvite/apatite |
| Protein | Usually absent or minimal |
| Casts | Tubular/granular if renal parenchymal damage |
Urinary Crystals - Characteristic Types (Highly Examinable with Images):
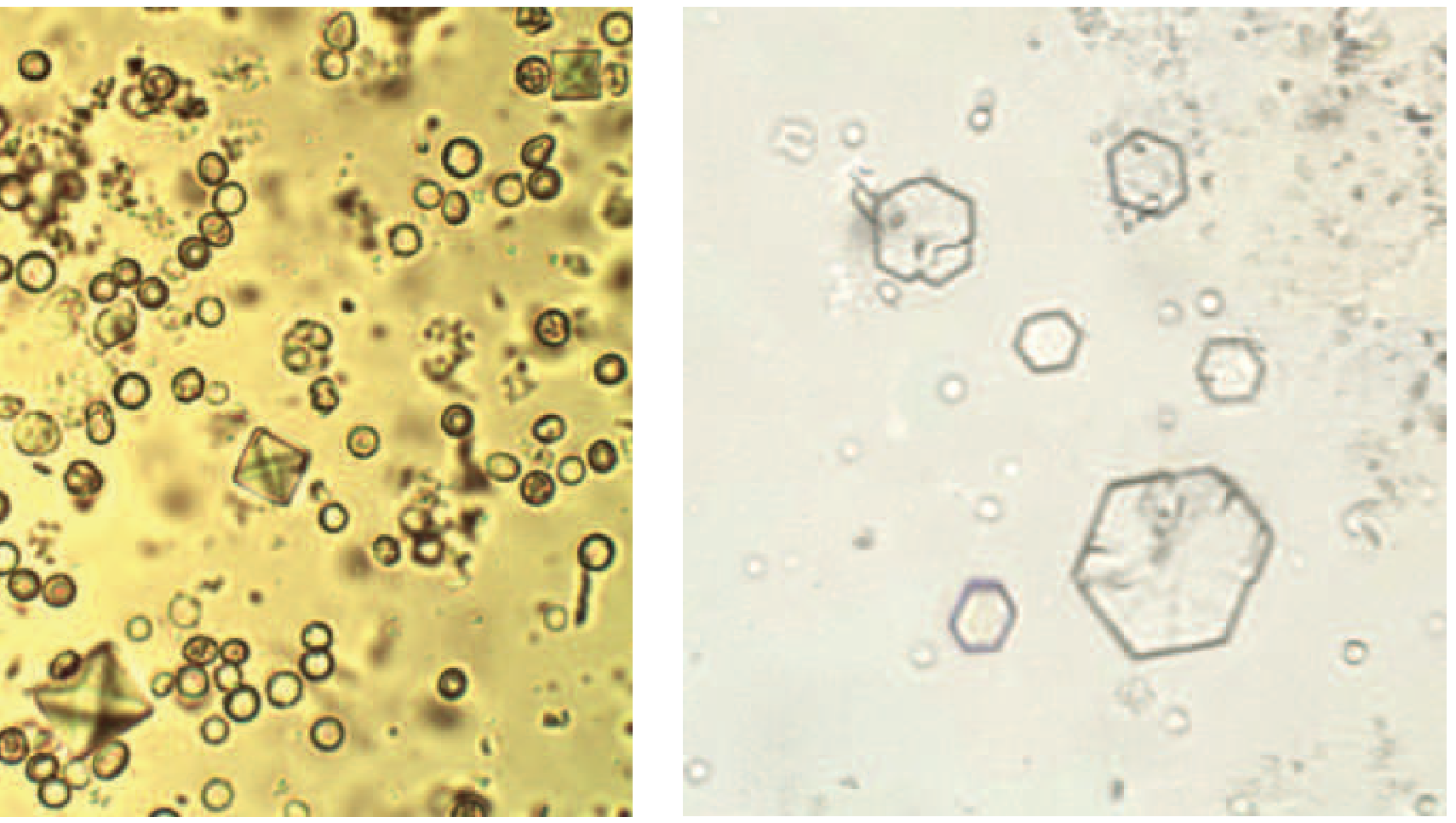
| Crystal Type | Morphology | Urine pH |
|---|---|---|
| Calcium oxalate dihydrate | Bipyramidal "envelope" / dumbbell shape (see image, LEFT) | Acidic/neutral |
| Calcium oxalate monohydrate | Small biconcave ovals, dumbbell-shaped | Acidic/neutral |
| Cystine | Hexagonal - pathognomonic (see image, RIGHT) | Acidic |
| Uric acid | Amorphous golden-brown powder / rhomboid | Acidic |
| Struvite (triple phosphate) | Coffin-lid shaped prisms | Alkaline |
| Calcium phosphate | Blunt needles, rosettes | Alkaline |
Urine Culture and Sensitivity
- Mandatory in ALL stone cases
- Identifies infecting organism (especially Proteus in struvite stones)
- Guides antibiotic therapy pre-operatively
24-Hour Urine Collection (Metabolic Evaluation)
- Collected on at least two separate days (there is substantial day-to-day variability)
- Parameters measured:
| Parameter | Normal Value | Significance if Abnormal |
|---|---|---|
| Total volume | >2 L/day | Low volume = major risk factor |
| Calcium | <250 mg/day (F), <300 mg/day (M) | Hypercalciuria |
| Oxalate | <40 mg/day | Hyperoxaluria |
| Citrate | >320 mg/day (F), >450 mg/day (M) | Hypocitraturia = major risk |
| Uric acid | <700 mg/day (F), <800 mg/day (M) | Hyperuricosuria |
| Sodium | - | High Na → high urine Ca |
| Phosphorus | - | Hyperphosphaturia |
| Magnesium | - | Low Mg = risk factor |
| pH | - | Persistently low → uric acid risk |
| Creatinine | - | Confirms adequacy of collection |
2. BLOOD INVESTIGATIONS
Routine Blood Tests
| Test | Finding | Significance |
|---|---|---|
| Serum creatinine/BUN | Elevated | Obstructive uropathy / renal failure |
| Serum calcium | Elevated | Primary hyperparathyroidism (must exclude) |
| Serum phosphate | Low (in 1° HPT) | Hyperparathyroidism |
| Serum uric acid | Elevated | Gout / hyperuricemia → uric acid stones |
| Serum electrolytes | Hypokalemia | May indicate RTA |
| PTH (intact) | Elevated | Primary hyperparathyroidism |
| 25-OH Vitamin D | Measured with PTH | Vitamin D excess / sarcoidosis |
| CBC | Leukocytosis | Infection / stress response |
| Blood glucose | Elevated | DM → uric acid stones |
| Alkaline phosphatase | Elevated | Bone disease, hyperparathyroidism |
Note: In uncomplicated renal colic, blood tests are usually normal. GFR may be reduced only in volume depletion, bilateral obstruction, or solitary kidney obstruction.
3. IMAGING INVESTIGATIONS
A. Plain X-ray (KUB) - Kidney, Ureter, Bladder
Role: First-line investigation; part of initial assessment; used for follow-up of known radio-opaque stones.
Radio-opacity of stones:
| Stone Type | KUB Appearance |
|---|---|
| Calcium oxalate | Dense opaque (most opaque) |
| Calcium phosphate | Opaque (less dense) |
| Struvite | Faintly opaque (may be staghorn) |
| Cystine | Faintly opaque (ground glass) |
| Uric acid | Radiolucent - NOT visible |
| Indinavir stones | Radiolucent |
Limitations of KUB:
- Cannot detect radiolucent stones (uric acid, indinavir)
- Small stones (<5 mm) and stones overlying bones may be missed
- Cannot assess obstruction or hydronephrosis
- Low sensitivity - limited utility in acute setting
- Useful mainly for monitoring known opaque stones
B. Ultrasound (USG)
Advantages:
- No radiation - first-line investigation in pregnant women
- Easily available, portable, inexpensive
- Can detect hydronephrosis/hydroureter reliably
- Can detect stones in renal pelvis and calyces
- Detects perinephric collection, abscess
Findings:
- Echogenic foci with posterior acoustic shadowing = calculus
- Hydronephrosis/hydroureter = obstruction
- Loss of ureteric jet on colour Doppler from contralateral side suggests complete obstruction
Limitations:
- Sensitivity ~29-69% for stones (significantly lower than CT)
- Cannot image the mid and distal ureter reliably
- Misses small stones (<5 mm) and ureteral stones
- Operator-dependent
When preferred: Pregnant patients, children, follow-up of known stones, emergency department first-line (can be used as initial imaging)
C. Non-Contrast CT (NCCT) KUB - GOLD STANDARD
Non-contrast helical (spiral) CT is the gold standard for diagnosis of renal calculi and suspected renal colic.
Advantages:
- Detects stones as small as 1 mm
- Detects ALL stone types including uric acid stones (traditionally "radiolucent" but visible on CT)
- Provides information on stone size, number, location, composition (Hounsfield Units)
- Shows hydronephrosis, hydroureter, perinephric stranding (evidence of recent passage)
- Can diagnose alternative pathology causing the pain (AAA, appendicitis, ovarian torsion, etc.)
- Does NOT require contrast (which could be nephrotoxic in obstruction)
- Quick to perform
CT Findings in Renal Calculi:
- Hyperdense calculus in collecting system / ureter
- Secondary signs: hydronephrosis, hydroureter, perinephric fat stranding (key sign of active obstruction)
- Tissue rim sign: soft tissue density rim around calculus at ureterovesical junction (distinguishes ureteral stone from phlebolith)
Hounsfield Units (HU) - Stone composition estimation:
| Stone Type | HU Range |
|---|---|
| Calcium oxalate monohydrate | >1000 HU (very dense) |
| Calcium oxalate dihydrate | ~800-1000 HU |
| Brushite | ~800-1000 HU |
| Struvite | ~600-900 HU |
| Uric acid | 200-450 HU (low density) |
| Cystine | ~600-700 HU |
Low-dose CT: Many centres now use low-dose CT protocols (<3 mSv vs 14 mSv for standard CT) with comparable stone detection sensitivity - reduces radiation exposure.
This is the actual CT image from Harrison's showing an obstructing left ureteral calculus:
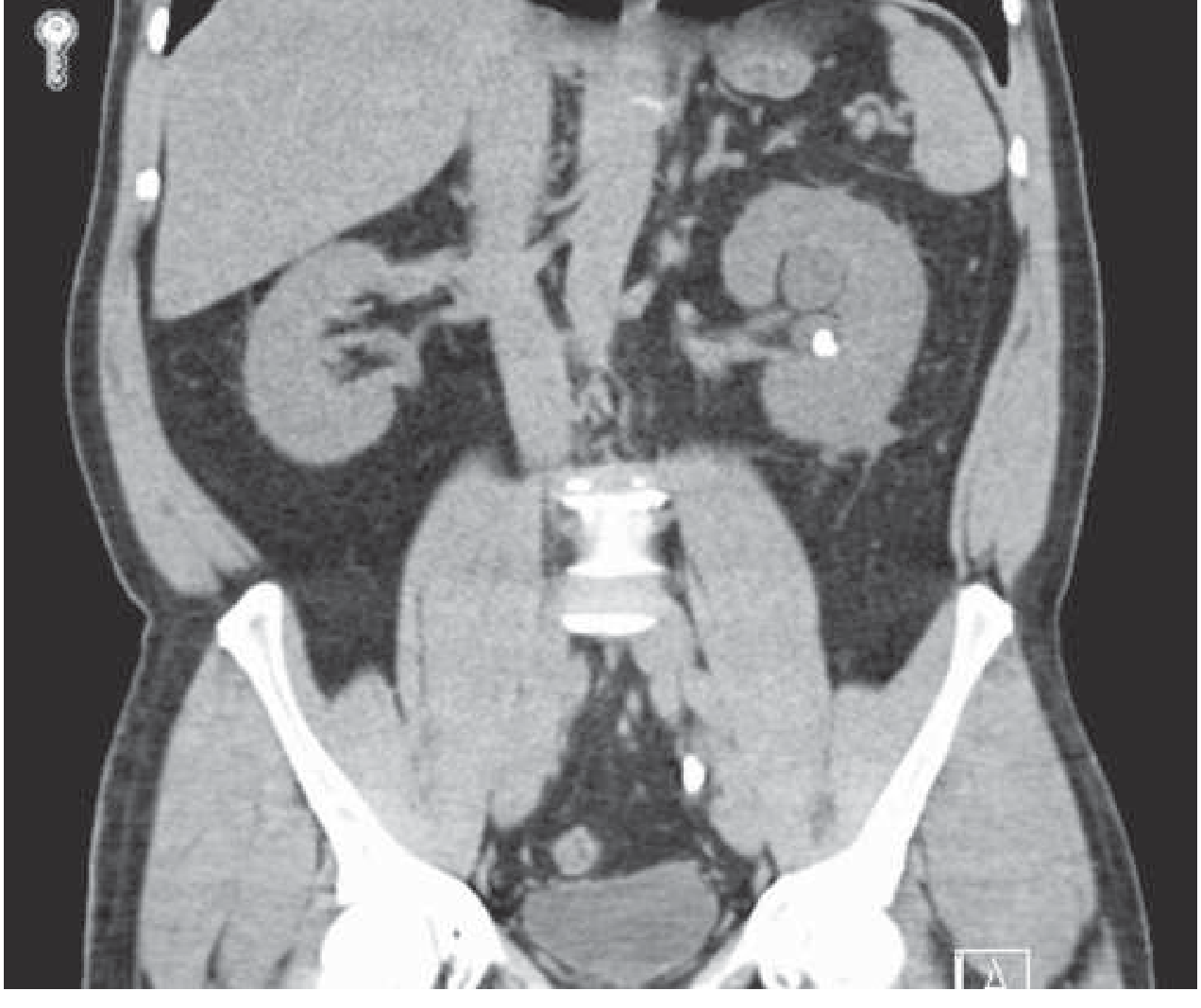
CT shows: 10 mm calculus in distal left ureter at S1 level, severe left hydroureteronephrosis, perinephric fat stranding, and a non-obstructing 6 mm left renal calculus in the interpolar region.
D. Intravenous Pyelogram / Urogram (IVP / IVU)
Previously the gold standard - now largely replaced by NCCT.
Findings on IVP:
- Delayed nephrogram on obstructed side
- Filling defect at site of obstruction
- Hydronephrosis / hydroureter above obstruction
- Non-functioning kidney (dense persistent nephrogram with no calyceal filling)
- Radiolucent stones appear as filling defects in contrast-filled collecting system
Still used:
- When anatomic detail of collecting system required prior to surgery
- Limited IVU preferred in pregnancy if ultrasound inconclusive (93% diagnostic accuracy)
- Some centres still prefer it for comprehensive urographic anatomy
Contraindications to IVP:
- Renal failure (nephrotoxicity of contrast)
- Contrast allergy
- Pregnancy (radiation + contrast)
- Myeloma (Bence Jones proteins + contrast → tubular precipitation)
E. MRI Urography
- No radiation - useful in pregnant patients when ultrasound is inconclusive
- MRI findings: signal void at stone site, perinephric/periureteral edema, abrupt ending of ureter at obstruction
- Sensitivity for stones higher than ultrasound but less than CT
- Limitations: expensive, time-consuming, poor at detecting small stones
- Not routinely used
F. Retrograde Pyelogram (RGP)
- Performed at cystoscopy
- Shows site of obstruction from below
- Used when NCCT is unavailable or for definitive anatomic mapping before endoscopic surgery
- Gold standard for ureteral anatomy before ureteroscopy
4. STONE ANALYSIS
When a stone is passed or retrieved surgically, it must be sent for analysis.
- Method: Infrared spectroscopy or X-ray crystallography (most accurate)
- Chemical analysis (older method)
- Identifies exact stone composition → guides targeted prevention
Patients should be instructed to strain their urine through a filter/gauze to capture passed stones for analysis.
5. SPECIAL/ADDITIONAL INVESTIGATIONS FOR METABOLIC WORKUP
Who needs a complete metabolic evaluation?
- All recurrent stone formers
- Patients with bilateral stones or multiple stones
- Strong family history
- Stones in children
- Struvite (infection) stones
- Cystinuria
- After first stone if the patient is motivated (recurrence is common and preventable)
Serum Tests
- Intact PTH + serum calcium → primary hyperparathyroidism
- 25-OH Vitamin D → hypervitaminosis D, sarcoidosis
- Serum ACE level → sarcoidosis
- Bicarbonate / anion gap → RTA
Specific Urine Tests
| Test | Stone Type Screened |
|---|---|
| Sodium nitroprusside test (urine) | Cystinuria (turns magenta/red) |
| Urine oxalate | Hyperoxaluria |
| Urine cystine quantification | Cystinuria |
| Urine uric acid | Hyperuricosuria |
| Urine culture | Struvite / UTI |
| Urine pH | Uric acid (persistent acidic), RTA (persistently alkaline) |
| Urine calcium/creatinine ratio | Hypercalciuria screening |
DIAGNOSIS - APPROACH AND CRITERIA
Diagnostic Approach to Suspected Renal Colic
Step 1 - History: Sudden loin-to-groin pain, hematuria, nausea/vomiting, previous stone episodes, relevant family/dietary/drug history
Step 2 - Physical Examination: CVA tenderness, patient writhing in pain, absence of peritoneal signs
Step 3 - Urine analysis: Hematuria ± pyuria ± crystals; pH
Step 4 - Imaging: NCCT KUB (gold standard) confirming stone, location, size, obstruction
The diagnosis is often made clinically from history + examination + urinalysis BEFORE imaging. It is not necessary to wait for radiographic confirmation before treating pain (Harrison's).
Diagnostic Summary Table - Imaging Comparison
| Feature | KUB | Ultrasound | NCCT | IVP |
|---|---|---|---|---|
| Stone detection | 60-70% | 29-69% | 95-98% | 70-80% |
| Radiolucent stones | No | No | Yes | Filling defect only |
| Obstruction | No | Yes | Yes | Yes |
| Ureter visualization | Poor | Poor (distal) | Excellent | Good |
| Radiation | Low | None | Moderate | Moderate + contrast |
| Time | Quick | Quick | Quick | Slow |
| Cost | Low | Low | Moderate | Moderate |
| In pregnancy | Avoid | Preferred | Avoid (last resort) | Avoid |
| Recommended for | Monitoring | First-line/pregnant | Acute diagnosis | Pre-op anatomy |
When to Suspect Complicated Stone Disease
The following features mandate urgent urological intervention:
- Fever + obstructing stone = pus under pressure = urological emergency
- Anuria = bilateral obstruction or solitary kidney
- Rising creatinine = obstructive nephropathy
- Uncontrollable pain = stone unlikely to pass spontaneously
- Stone >6 mm = low spontaneous passage rate
- Solitary kidney with obstruction
Sources consulted: Harrison's Principles of Internal Medicine 22e (Clinical Presentation, Diagnosis, Evaluation); National Kidney Foundation Primer on Kidney Diseases 8e (Acute Renal Colic, Imaging); Campbell-Walsh-Wein Urology (Natural History, Surgical Planning); Barash Clinical Anesthesia 9e (Imaging modalities); Smith & Tanagho's General Urology 19e (Risk Factors, Crystal morphology); Bailey & Love's Short Practice of Surgery 28e (Urolithiasis)
Hydronephrosis defination causes pathology clinical features management and acc to above way
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
HYDRONEPHROSIS
(Referred from: S Das - A Manual on Clinical Surgery 13th Edition, Robbins & Kumar Basic Pathology, Comprehensive Clinical Nephrology 7th Edition, Smith & Tanagho's General Urology 19th Edition, Campbell-Walsh-Wein Urology)
DEFINITION
Hydronephrosis is the dilatation of the renal pelvis and calyces, with accompanying atrophy of the renal parenchyma, caused by obstruction to the outflow of urine.
(Robbins & Kumar Basic Pathology)
- The obstruction may be sudden or insidious
- It may occur at any level of the urinary tract - from the urethra to the renal pelvis
- The degree of parenchymal damage depends on the degree, duration, and completeness of obstruction
- When obstruction is below the level of the ureters → bilateral hydronephrosis
- When obstruction is at or above the ureters → unilateral hydronephrosis
CAUSES
Causes are best classified as:
- By level of obstruction (most practical for surgical exams)
- By type (congenital / acquired)
- By side (unilateral / bilateral)
A. CAUSES BY LEVEL OF OBSTRUCTION
I. Renal Pelvis / Pelviureteric Junction (PUJ) Obstruction (Unilateral)
(S Das, A Manual on Clinical Surgery)
| Cause | Details |
|---|---|
| (i) Idiopathic PUJ stenosis | Most common cause of unilateral hydronephrosis; congenital narrowing or aperistaltic segment |
| (ii) Calculus (stone) | Stone impacted at PUJ - most common acquired cause |
| (iii) Tumour of renal pelvis | Transitional cell carcinoma causing obstruction |
| (iv) Aberrant / crossing renal artery | Compresses lower pole of PUJ from outside |
II. Ureteric Obstruction (Usually unilateral)
(S Das)
| Cause | Details |
|---|---|
| (i) Calculus | Most common ureteric cause; stone at any level of ureter |
| (ii) Tumour of ureter | Transitional cell carcinoma of ureter |
| (iii) Tumour infiltrating from adjacent organs | Ca cervix, Ca bladder, Ca colon/rectum invading ureter |
| (iv) Ureterocele | Cystic dilatation of distal ureter prolapsing into bladder |
| (v) Schistosomiasis | Fibrosis and stricture of ureter (endemic areas) |
| (vi) Bladder tumour | Involving ureteric orifice |
| (vii) Retroperitoneal fibrosis | Idiopathic or drug-induced; bilateral ureteric involvement |
| (viii) Pregnancy | Physiological compression of ureter by gravid uterus (usually right side) |
| (ix) Ureteral stricture | Post-inflammatory, post-surgical, post-radiation |
| (x) Sloughed papilla | Diabetic papillary necrosis, analgesic nephropathy |
| (xi) Blood clot | Impacted clot causing temporary obstruction |
III. Bladder Outlet / Infravesical Obstruction (Bilateral hydronephrosis)
(S Das)
| Cause | Details |
|---|---|
| (i) Prostatic enlargement | BPH - most common cause of bilateral hydronephrosis in elderly males |
| (ii) Carcinoma of prostate | Direct invasion of bladder outlet |
| (iii) Carcinoma of bladder | Involving trigone and both ureteric orifices |
| (iv) Urethral stricture | Post-inflammatory (gonorrhoea) or post-traumatic |
| (v) Posterior urethral valves | Congenital; in boys - common cause in children |
| (vi) Phimosis | Severe; obstructs urinary outflow |
| (vii) Neurogenic bladder | Paralysis of bladder after spinal cord damage; functional obstruction |
| (viii) Schistosomiasis | Bladder involvement |
B. CAUSES BY TYPE
| Congenital | Acquired |
|---|---|
| Atresia/stenosis of urethra | Calculi (stones) - most common acquired |
| Posterior urethral valves | BPH |
| Ureterocele | Carcinoma (bladder, prostate, cervix) |
| Aberrant renal artery compressing ureter | Retroperitoneal fibrosis |
| Malrotation/kinking of ureter | Urethral stricture |
| Horseshoe kidney (abnormal position) | Sloughed papilla, blood clot |
| - | Pregnancy |
| - | Neurogenic bladder |
PATHOLOGY (PATHOGENESIS AND MORPHOLOGY)
Pathogenesis (Robbins & Kumar Basic Pathology)
Step 1 - Continued glomerular filtration despite obstruction:
Even with complete obstruction, glomerular filtration persists for some time, and the filtrate subsequently diffuses back into the renal interstitium and perirenal spaces and ultimately returns to the lymphatic and venous systems.
Step 2 - Pressure build-up:
Because of continued filtration, the affected calyces and pelvis become progressively dilated - often markedly. This generates unusually high back pressure in the renal pelvis, which is transmitted back through the collecting ducts and compresses the renal vasculature.
Step 3 - Vascular compromise:
Back pressure → arterial insufficiency + venous stasis → ischemia of renal parenchyma. The most severe effects are in the papillae, which are subjected to the greatest increases in pressure.
Step 4 - Tubular dysfunction first:
The initial functional disturbances are largely tubular - manifested primarily by impaired concentrating ability. Glomerular filtration only diminishes later.
Step 5 - Fibrosis:
Obstruction triggers an interstitial inflammatory reaction → eventually leads to interstitial fibrosis.
Gross Morphology (Robbins Basic Pathology)

Gross specimen of hydronephrotic kidney showing massively distended pelvicalyceal system with dramatic thinning of renal parenchyma. The kidney has become a thin shell surrounding a large cystic cavity.
With subtotal or intermittent obstruction:
- Kidney may be massively enlarged (up to 20 cm in length)
- Organ may consist almost entirely of greatly distended pelvicalyceal system
- Renal parenchyma is compressed and atrophied
- Obliteration of the papillae and flattening of the pyramids
- Ureter may also be dilated (hydroureter) depending on level of obstruction
With sudden and complete obstruction:
- Glomerular filtration is compromised relatively early
- Renal function may cease while dilation is comparatively mild
Microscopic Morphology
Early changes:
- Tubular dilation and atrophy
- Tubular epithelium flattens and eventually disappears
- Loss of loops of Henle and collecting tubules
Late changes:
- Loss of glomeruli
- Replacement of renal parenchyma by fibrous tissue (interstitial fibrosis)
- Inflammatory reaction (usually minimal in uncomplicated cases)
- Superimposed pyelonephritis is common - an important complication
Grading of Hydronephrosis (Ultrasound / Society for Fetal Urology)
| Grade | Description |
|---|---|
| Grade 0 | No hydronephrosis |
| Grade 1 | Mild - only renal pelvis dilated; calyces normal; parenchyma normal |
| Grade 2 | Moderate - pelvis + calyces dilated; parenchyma normal thickness |
| Grade 3 | Moderate-severe - pelvis + calyces dilated; parenchyma slightly thinned; medullary pyramids starting to flatten |
| Grade 4 | Severe - massively dilated pelvicalyceal system; parenchyma markedly thinned; corticomedullary differentiation lost |
(Comprehensive Clinical Nephrology - ultrasound grading: mild/moderate/severe)
CLINICAL FEATURES
A. UNILATERAL HYDRONEPHROSIS
(S Das - A Manual on Clinical Surgery)
Affected population:
- Females more often affected than males
- Occurs at practically all ages
- Onset is typically insidious
Symptoms
1. Pain
- The cardinal symptom
- Typically dull ache or a sense of heaviness / weight in the loin
- Sometimes patients may ignore it as mild backache
- If hydronephrosis develops quickly (acute obstruction) → pain may be severe and colicky - ureteric colic
- Pain may be exacerbated by:
- Drinking excessive amounts of water or alcohol
- Taking diuretics
- Pain may be referred to the epigastrium - can be mistaken for duodenal ulcer
- "Dietl's Crisis" (see below)
Dietl's Crisis (Classic S Das point): Episodic severe pain in the loin, followed (after a few hours) by passing of a large quantity of urine and significant reduction in the size of the loin swelling. This occurs due to intermittent obstruction at the PUJ that temporarily "blows open" - urine drains out rapidly, relieving the distension and pain. Pathognomonic of intermittent hydronephrosis.
2. Swelling in the Loin / Abdomen
- Gradually enlarging, painless swelling in the loin or hypochondrium
- Often the patient's presenting complaint when hydronephrosis is large
3. Haematuria
- May be present when the cause is a stone, tumour, or infection
- Frank haematuria suggests tumour or stone
4. Symptoms of Renal Failure (if bilateral or if contralateral kidney is damaged)
- Oliguria / anuria
- Oedema
- Uraemia - nausea, vomiting, drowsiness, hiccoughs
5. Symptoms of UTI / Pyonephrosis
- Fever with rigors
- Cloudy, foul-smelling urine
- Frequency, dysuria
6. Symptoms of Underlying Cause
- Lower urinary tract symptoms (BPH, urethral stricture)
- Loss of weight / bleeding per rectum (retroperitoneal malignancy)
- Cervical discharge (carcinoma cervix)
Signs on Examination
General:
- Usually looks well (chronic, insidious course)
- Oedema, pallor (if renal failure)
- Signs of uraemia in advanced cases
Abdominal Examination:
- Loin fullness / visible swelling - in large hydronephrosis
- Palpable renal swelling - the most important sign:
- Cystic, tense, non-tender (unless infected)
- Ballottable - can be felt bimanually
- Moves with respiration
- Occupies the flank and moves downward on inspiration
- Bimanual palpation - one hand in loin, other on anterior abdomen; feels like a cystic swelling that is "ballottable" (can be bounced between two hands)
- Resonant on percussion if gas-filled bowel is anterior; dull if large
- Tenderness - present if infection supervenes (pyonephrosis)
- Transillumination - may be positive in very large thin-walled hydronephrosis (thin parenchyma = translucent cyst); not reliable
Key physical sign: "A cystic large renal swelling felt on bimanual palpation that is ballottable" - S Das
B. BILATERAL HYDRONEPHROSIS
(S Das - Bilateral Hydronephrosis section)
Symptoms are mainly those of the underlying cause plus features of:
- Uraemia / Chronic Renal Failure: oliguria, anuria, uraemic symptoms (nausea, vomiting, hiccough, confusion, uraemic frost)
- Bladder distension: lower urinary tract symptoms, overflow incontinence
- Paradoxical polyuria: incomplete bilateral obstruction causes polyuria (not oliguria!) due to defects in tubular concentrating ability - this may OBSCURE the true diagnosis
- Bilateral flank discomfort
- Signs of the primary cause: enlarged prostate on PR examination, palpable bladder, urethral stricture
Important (Robbins): "Paradoxically, incomplete bilateral obstruction causes polyuria rather than oliguria as a result of defects in tubular concentrating mechanisms, and this may obscure the true nature of the lesion."
INVESTIGATIONS
1. Urine Examination
- Routine and microscopy: RBCs, WBCs, casts, protein
- Culture and sensitivity: to identify infection / causative organism
- 24-hour urine: for creatinine clearance (renal function assessment)
2. Blood Investigations
| Test | Significance |
|---|---|
| Serum creatinine / BUN | Raised in bilateral hydronephrosis / renal failure |
| Serum electrolytes | Hyperkalaemia, metabolic acidosis in obstruction |
| CBC | Anaemia (chronic renal failure); leukocytosis (infection) |
| PSA | Elevated in carcinoma prostate |
| Serum calcium / PTH | If stone disease suspected |
3. Imaging Investigations
A. Plain X-ray (KUB)
- May show calculus (radio-opaque stones)
- Obliterated psoas shadow suggests perinephric collection
- Large soft tissue shadow of hydronephrotic kidney may be visible
- Prostatic calcification may be seen
B. Ultrasound - First-line and Most Important Bedside Investigation
Ultrasound grading of hydronephrosis (Comprehensive Clinical Nephrology):
- Mild: Dilation of renal pelvis and calyces, parenchymal architecture retained
- Moderate: Medullary pyramids start to flatten; increasing pelvicalyceal dilation
- Severe: Ballooned pelvis and calyces occupying most of kidney; thin parenchyma; loss of corticomedullary differentiation; parenchyma appears as a thin rim
What ultrasound shows:
- Anechoic (dark) fluid-filled branching pelvicalyceal system
- Degree and grade of hydronephrosis
- Thickness of remaining parenchyma (predicts functional recovery)
- Associated hydroureter
- Presence of stone (echogenic focus with posterior acoustic shadowing)
- Absent ureteric jets on Colour Doppler from affected side = complete obstruction
Pyonephrosis: if hydronephrotic area demonstrates internal echoes = pus in collecting system → emergency drainage required
S Das: "Ultrasound scanning is also quite confirmatory, moreover it is the least invasive. It may be used to detect this case due to pelviureteric junction obstruction in utero."
C. Intravenous Pyelogram / Urogram (IVP / IVU)
(S Das - "Urography is confirmatory")
Findings on IVP:
- Earliest changes: depending on whether pelvis is extra- or intrarenal:
- Extrarenal pelvis (majority): earliest changes in renal pelvis itself
- Intrarenal pelvis: decreasing concavity then flattening of minor calyces is the first change
- Progressive dilatation of major calyces
- Clubbing/convexity of minor calyces (blunting of fornices - calyces become rounded rather than cupped)
- The pelvis becomes so distended that its convex lower margin forms an acute angle with the ureter (in late stages)
- Delayed nephrogram - obstructed kidney shows persistent dense nephrogram with no calyceal filling (absent / delayed excretion)
- Dense persistent nephrogram with good function but no drainage = obstruction
- Non-functioning kidney shows no nephrogram
S Das: "Conventional earlier films may fail to visualize the pelvis and calyces. Better delineation may be seen after 6 hours of injection. If pelvis and calyces are not seen properly, retrograde urography should be called for."
D. Non-Contrast CT (NCCT) KUB - Gold Standard for Acute Obstruction
- Detects underlying cause (stone, tumour mass, retroperitoneal disease)
- Shows degree of hydronephrosis
- Perinephric fat stranding = active obstruction
- Characterizes stone (size, HU, location)
- CT urogram (with contrast) gives anatomical detail
E. Retrograde Pyelogram (RGP)
(S Das: "Retrograde urography should be called for when IVP fails")
- Gold standard for anatomical detail of obstructed ureter
- Shows site and level of obstruction from below
- Used pre-operatively before definitive repair
- Risk: introducing infection above obstruction
F. Isotope Renography (Radionuclide Scan / MAG-3 Scan)
(S Das: "Isotope renography may be used to detect dilatation of the renal collecting system due to obstruction")
- MAG-3 diuresis renogram (Lasix renogram): differentiates obstructive from non-obstructive dilatation
- Tc-DTPA or MAG-3 scan with frusemide washout:
- Obstructed kidney: prolonged t½ (>20 minutes) after frusemide
- Non-obstructed dilation: rapid washout after frusemide
- Measures differential renal function (GFR contribution of each kidney)
- Essential before surgery to ensure the kidney has recoverable function
- If one kidney contributes <10-15% of total GFR → nephrectomy may be preferred over reconstruction
G. Whitaker Test (Pressure-Flow Studies)
(S Das: "Whitaker test is sometimes used in specialised unit to monitor intrapelvic pressure by percutaneous puncture of the kidney")
- Percutaneous puncture of the renal pelvis under ultrasound guidance
- Fluid infused at a standard rate (10 mL/min)
- Intrapelvic pressure measured simultaneously
- Normal: intrapelvic pressure < 15 cm H2O
- Obstruction: pressure > 22 cm H2O
- Used when isotope renogram is equivocal
- Invasive - used in specialized units only
H. MRI Urography
- No radiation - useful in pregnancy
- Shows anatomical detail of obstruction
- Excellent soft tissue contrast - useful for retroperitoneal fibrosis, tumour
- Not first-line but used when CT contraindicated
I. Cystoscopy
- Essential to examine bladder and ureteric orifices
- Can identify bladder tumour, ureteric orifice obstruction, ureterocele
- Allows retrograde stenting / pyelogram under direct vision
- PR examination (per rectum) - enlarged prostate palpable in BPH/Ca prostate
MANAGEMENT
Management depends on:
- Level and cause of obstruction
- Unilateral vs bilateral
- Degree of renal function preserved (critical decision point)
- Presence of infection (pyonephrosis = emergency)
- Acute vs chronic obstruction
GENERAL PRINCIPLES OF MANAGEMENT
(Comprehensive Clinical Nephrology)
"Treatment is dictated by the location of the obstruction, the underlying cause, and the degree of any kidney impairment. Complete bilateral ureteral obstruction manifesting as AKI is a medical emergency requiring rapid intervention to salvage kidney function."
A. EMERGENCY / IMMEDIATE MANAGEMENT (Drainage)
Indication for emergency drainage:
- Bilateral obstruction with acute renal failure (AKI)
- Obstruction of a solitary functioning kidney
- Infected obstructed kidney (pyonephrosis = "pus under pressure")
- Rising serum creatinine despite adequate hydration
Methods of emergency drainage:
| Level of Obstruction | Method |
|---|---|
| Bladder outlet / infravesical | Urethral catheter (first choice) |
| Urethral catheter fails (stricture, prostatic block) | Suprapubic cystostomy (SPC) |
| Upper tract obstruction / ureteral | Percutaneous Nephrostomy (PCN) under ultrasound guidance |
| Upper tract (alternative) | Retrograde ureteral stenting (JJ stent) via cystoscopy |
Percutaneous Nephrostomy (PCN) is the preferred emergency treatment for upper urinary tract obstruction, especially with AKI:
- Performed under local anaesthetic (can avoid GA)
- Allows rapid drainage and recovery of function in >70% of cases
- After PCN, antegrade contrast can be injected to map exact site of obstruction (antegrade nephrostogram) before planning definitive surgery
- Major complications (abscess, infection, haematoma) <5%
- If both kidneys obstructed: nephrostomy placed in kidney with most preserved parenchyma first; bilateral nephrostomies may be required
B. DEFINITIVE MANAGEMENT (Based on Cause)
1. Pelviureteric Junction (PUJ) Obstruction
Conservative management (watchful waiting):
- Asymptomatic hydronephrosis with good function and no deterioration
- Monitored with serial ultrasound and MAG-3 scans
Surgical management - Anderson-Hynes Dismembered Pyeloplasty (Operation of choice):
- The gold standard for PUJ obstruction
- The obstructed PUJ segment is excised and the renal pelvis is trimmed and re-anastomosed to the ureter in a funnel-shaped, dependent manner
- Advantages: excises the abnormal segment; reduces pelvis size; creates a wide, dependent anastomosis; crosses aberrant vessels
- Success rate >90%
- Can be performed:
- Open (loin incision)
- Laparoscopic (transperitoneal or retroperitoneal)
- Robot-assisted laparoscopic (increasingly preferred)
Alternatives to pyeloplasty:
- Endopyelotomy (endoscopic incision of PUJ): percutaneous or ureteroscopic; lower success rates than open pyeloplasty; used for secondary/recurrent cases
- Balloon dilatation of PUJ: poor long-term results
2. Ureteric Calculus Causing Obstruction
- Conservative (analgesia, fluids, alpha-blockers) for stones <6 mm
- ESWL for stones 6-20 mm
- Ureteroscopy + laser lithotripsy for ureteric stones
- PCNL for large renal calculi with associated obstruction
- JJ stent placement if obstruction with infection
3. BPH / Prostatic Obstruction (Bilateral Hydronephrosis)
- Initial drainage with urethral catheter
- Medical therapy: alpha-blockers (tamsulosin), 5-alpha-reductase inhibitors (finasteride)
- TURP (Transurethral Resection of Prostate) - gold standard surgical treatment for BPH
- Open prostatectomy for very large glands
4. Urethral Stricture
- Urethral dilatation (bougies)
- Optical urethrotomy (endoscopic incision of stricture)
- Urethroplasty (open reconstruction) for long/recurrent strictures
5. Retroperitoneal Fibrosis
- Steroids (prednisolone) - first-line medical therapy
- Ureterolysis + omental wrap (surgical)
- JJ stenting as temporary measure
6. Carcinoma (Cervix, Bladder, Prostate) Causing Obstruction
- Treat underlying malignancy (chemotherapy, radiotherapy, surgery)
- Palliative nephrostomy or JJ stent for obstruction not amenable to curative treatment
7. Neurogenic Bladder
- Intermittent self-catheterisation (ISC)
- Anticholinergic medications
- Urinary diversion (ileal conduit) in severe refractory cases
C. NEPHRECTOMY (Removal of Hydronephrotic Kidney)
Indications for nephrectomy instead of reconstruction:
- Kidney with <10-15% split function on MAG-3 scan (non-recoverable)
- Grossly infected hydronephrosis (pyonephrosis) where reconstruction not feasible
- Associated malignancy of the kidney
- Stone-laden non-functioning kidney
Key principle: Before nephrectomy, always confirm the contralateral kidney is functioning adequately.
D. POST-RELIEF COMPLICATIONS - POSTOBSTRUCTIVE DIURESIS
After relief of bilateral obstruction (or single functioning kidney obstruction), a significant postobstructive diuresis may occur:
- Large volumes of urine (up to 5-10 L/day)
- Due to:
- Accumulated solutes (urea, sodium) acting as osmotic diuretic
- Tubular dysfunction with impaired reabsorption
- Volume expansion during obstruction
- Management: careful IV fluid replacement to match output (avoid dehydration and electrolyte imbalance)
- Monitor electrolytes closely (Na, K, bicarbonate)
- Usually self-limiting over 24-72 hours as tubular function recovers
PROGNOSIS AND RECOVERY OF RENAL FUNCTION
- Acute obstruction (<1-2 weeks): excellent recovery of function after relief
- Chronic obstruction (months to years): variable; permanent damage may occur
- Histological studies show: thinned cortex, few atrophic tubules, dense fibrous interstitium, no glomeruli in chronically obstructed kidneys → no prospect of significant functional recovery even after relief
- Removal of obstruction usually permits full return of function within a few weeks with short-duration obstruction; with longstanding obstruction the changes become irreversible (Robbins)
- MAG-3 scan differential function of <15% → nephrectomy preferred over salvage surgery
COMPLICATIONS OF UNTREATED HYDRONEPHROSIS
| Complication | Mechanism |
|---|---|
| Pyonephrosis | Superimposed infection of obstructed kidney - pus fills the collecting system |
| Perinephric abscess | Extension of infection through renal capsule |
| Chronic pyelonephritis | Recurrent infection → scarring |
| Chronic renal failure | Progressive parenchymal atrophy |
| Hypertension | Renal ischaemia → renin-angiotensin activation |
| Uraemia | Bilateral obstruction → end-stage renal disease |
| Spontaneous rupture | Rare; urinoma formation |
SUMMARY TABLE - UNILATERAL VS BILATERAL HYDRONEPHROSIS
| Feature | Unilateral | Bilateral |
|---|---|---|
| Level of obstruction | Renal pelvis / ureter | Below ureteric junction (bladder outlet / urethra) |
| Common causes | PUJ obstruction, calculus, ureteric tumour | BPH, carcinoma bladder, urethral stricture |
| Renal failure | No (other kidney compensates) | Yes (both kidneys affected) |
| Presenting complaint | Loin pain, flank mass, Dietl's crisis | LUTS, uraemia, overflow incontinence |
| Paradoxical polyuria | No | Yes (incomplete obstruction) |
| Emergency drainage | PCN / JJ stent (upper tract) | Urethral catheter / SPC |
| Definitive surgery | Pyeloplasty / stone removal | Treat underlying cause (TURP etc.) |
Sources consulted: S Das - A Manual on Clinical Surgery 13th Edition (Unilateral and Bilateral Hydronephrosis, Causes, Clinical features, Investigations - Urography, Ultrasound, Isotope Renogram, Whitaker Test); Robbins & Kumar Basic Pathology (Definition, Pathogenesis, Gross and Microscopic Morphology, Clinical Features); Comprehensive Clinical Nephrology 7th Edition (Ultrasound grading, Treatment - PCN, Drainage principles, Postobstructive diuresis); Smith & Tanagho's General Urology 19e (Pyeloplasty); Campbell-Walsh-Wein Urology (Transplant hydronephrosis management)
Create a Word document summarizing renal calculi, clinical features, and hydronephrosis for easy reference
Reading File
Running Command
mkdir -p /home/daytona/workspace/renal-notes && ls /home/daytona/workspace/renal…
This is a shared conversation. Sign in to Orris to start your own chat.