All reasons for low HB
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from Harrison's, Frameworks for Internal Medicine, and Creasy & Resnik's Maternal-Fetal Medicine. Here is the complete answer:
All Causes of Low Hemoglobin (Anemia)
Anemia is defined as hemoglobin below normal for a given population. There are two major classification frameworks: by red cell size (MCV) and by mechanism (production vs. destruction/loss).
Classification by MCV (Red Cell Size)
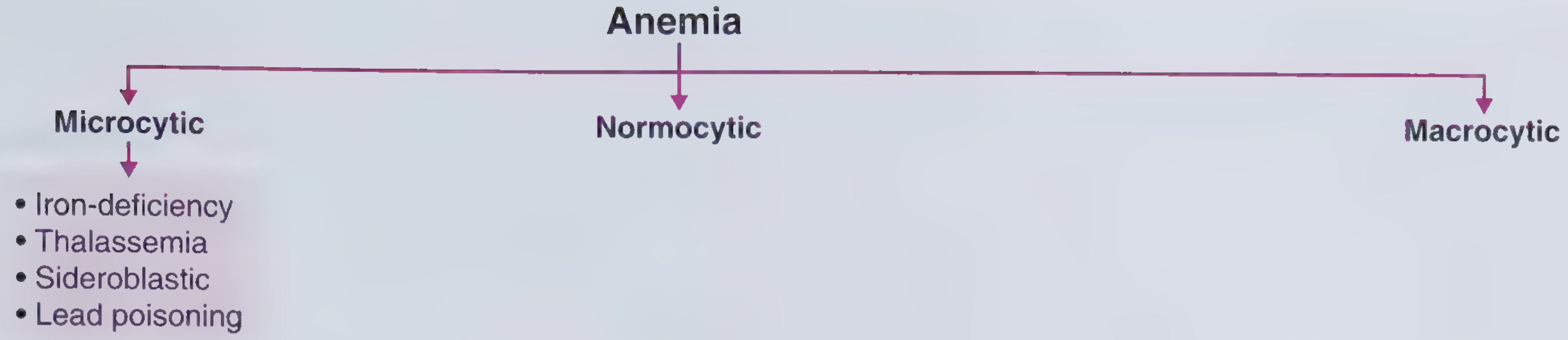
Microcytic (low MCV) - due to impaired hemoglobin synthesis
| Cause | Mechanism |
|---|---|
| Iron deficiency | Most common worldwide; poor intake, malabsorption (celiac), chronic blood loss, increased demand (pregnancy) |
| Thalassemia | Inherited defect in alpha or beta globin chain synthesis |
| Anemia of chronic disease/inflammation | Cytokine-mediated inhibition of iron reutilization |
| Sideroblastic anemia | Defect in heme synthesis; ringed sideroblasts in marrow |
| Lead poisoning | Inhibits heme synthesis enzymes |
Macrocytic (high MCV)
Megaloblastic (oval macrocytes - defective DNA synthesis):
- Vitamin B12 deficiency (pernicious anemia, strict veganism, gastric surgery, malabsorption)
- Folate deficiency (poor intake, malabsorption, increased demand)
- Copper deficiency
- Nitrous oxide inhalation (inactivates B12)
- Medications: chemotherapy agents, some antiseizure drugs, methotrexate, hydroxyurea
- Myelodysplastic syndrome
Non-megaloblastic (round macrocytes - membrane defects):
- Alcohol use
- Liver disease
- Hypothyroidism
- Dysproteinemia
- Hypoxia
- Smoking
- Reticulocytosis (from hemolysis or bleeding)
Normocytic (normal MCV)
- Aplastic anemia
- Pure red cell aplasia
- Renal disease (decreased EPO)
- Endocrinopathies (hypothyroidism, adrenal insufficiency, hypogonadism)
- Marrow invasion (myeloma, metastatic cancer, lymphoma)
- Early iron deficiency or mixed deficiencies
Classification by Mechanism
I. Dilutional (plasma volume expansion)
- Pregnancy (physiological)
- Hyperglobulinemia
- Massive splenomegaly
II. Decreased RBC Production (Underproduction)
At least 75% of anemias are hypoproliferative. Reticulocyte count is low/inappropriately normal.
A. Nutritional deficiencies
- Iron - most common cause of anemia worldwide
- Vitamin B12
- Folate
- Copper
- Vitamin C (impairs iron absorption)
- Protein deficiency
B. Reduced/absent EPO stimulation
- Chronic kidney disease - leading cause of EPO deficiency
- Anemia of inflammation/chronic disease - cancer, chronic infection, autoimmune disease (cytokines suppress EPO and iron utilization)
- Anemia of aging - reduced EPO responsiveness
- Endocrine failure - hypothyroidism, hypopituitarism, Addison's disease, hypogonadism
C. Bone marrow failure / absence of precursors
- Aplastic anemia - autoimmune, drugs (chloramphenicol, NSAIDs), radiation, toxins, infections (EBV, CMV, hepatitis), idiopathic
- Pure red cell aplasia - autoimmune targeting erythroid precursors, parvovirus B19, thymoma
D. Marrow replacement (myelophthisic anemia)
- Tumor infiltration (metastatic cancer, lymphoma)
- Granulomatous disease (TB, sarcoidosis)
- Fibrosis (myelofibrosis)
- Infection
E. Stem cell / clonal defects
- Myelodysplastic syndrome (MDS) - clonal stem cell disorder with ineffective erythropoiesis
- Acute leukemia (AML, ALL)
- Chronic leukemia (CML, CLL)
F. Ineffective erythropoiesis (cells made but die in marrow)
- Megaloblastic anemias (B12/folate deficiency)
- Thalassemia major
- Refractory anemia / MDS
III. Increased RBC Loss (Hyperproduction state - reticulocyte count high)
A. Hemorrhage (blood loss)
- Acute hemorrhage (trauma, surgery, GI bleed, ruptured ectopic pregnancy)
- Chronic blood loss (GI bleeding from ulcer/cancer/IBD, heavy menstruation, hookworm infection, frequent phlebotomy)
B. Hemolysis
1. Intrinsic RBC disorders (intracorpuscular - mostly inherited):
| Category | Examples |
|---|---|
| Hemoglobinopathies | Sickle cell disease, HbC disease, unstable hemoglobins |
| RBC enzyme deficiencies | G6PD deficiency, pyruvate kinase deficiency |
| Membrane defects | Hereditary spherocytosis (spectrin/ankyrin defects), hereditary elliptocytosis |
| Porphyrias | Defects in heme biosynthesis pathway |
Acquired intrinsic:
- Paroxysmal nocturnal hemoglobinuria (PNH) - clonal disorder, GPI-anchor defect
- Lead poisoning
2. Extrinsic RBC disorders (extracorpuscular):
| Category | Examples |
|---|---|
| Immune | Autoimmune hemolytic anemia (warm IgG or cold IgM), drug-induced hemolysis, transfusion reactions, hemolytic disease of the newborn |
| Mechanical / microangiopathic | TTP, HUS, DIC, HELLP syndrome, prosthetic heart valves, march hemoglobinuria |
| Infections | Malaria (most common worldwide cause of hemolytic anemia), Clostridium, Babesia, Bartonella |
| Chemical/toxic agents | Arsine gas, dapsone, oxidant drugs in G6PD-deficient patients, snake venoms |
| Hypersplenism | Sequestration and destruction of RBCs in enlarged spleen (portal hypertension, lymphoma, storage diseases) |
| Liver disease | Spur cell anemia (acanthocytes) |
Quick Reference Summary
| Mechanism | Key Examples |
|---|---|
| Iron deficiency | Poor diet, blood loss, malabsorption |
| B12/folate deficiency | Pernicious anemia, veganism, malnutrition |
| Chronic disease/inflammation | Cancer, infection, autoimmune |
| Renal failure | Low EPO |
| Aplastic anemia | Autoimmune, drugs, radiation |
| Thalassemia | Inherited globin chain defect |
| Hemolytic (intrinsic) | Sickle cell, G6PD, spherocytosis, PNH |
| Hemolytic (extrinsic) | AIHA, TTP/HUS, malaria, hypersplenism |
| Blood loss | GI bleed, menorrhagia, trauma |
| Marrow infiltration | Leukemia, MDS, metastases |
| Dilutional | Pregnancy, splenomegaly |
Sources: Harrison's Principles of Internal Medicine 22E, pp. 492-495; Frameworks for Internal Medicine, pp. 331-340; Creasy & Resnik's Maternal-Fetal Medicine, p. 1011
This is a shared conversation. Sign in to Orris to start your own chat.