Principles of split thickness skin graft. [5]
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete answer on the Principles of Split Thickness Skin Graft (STSG):
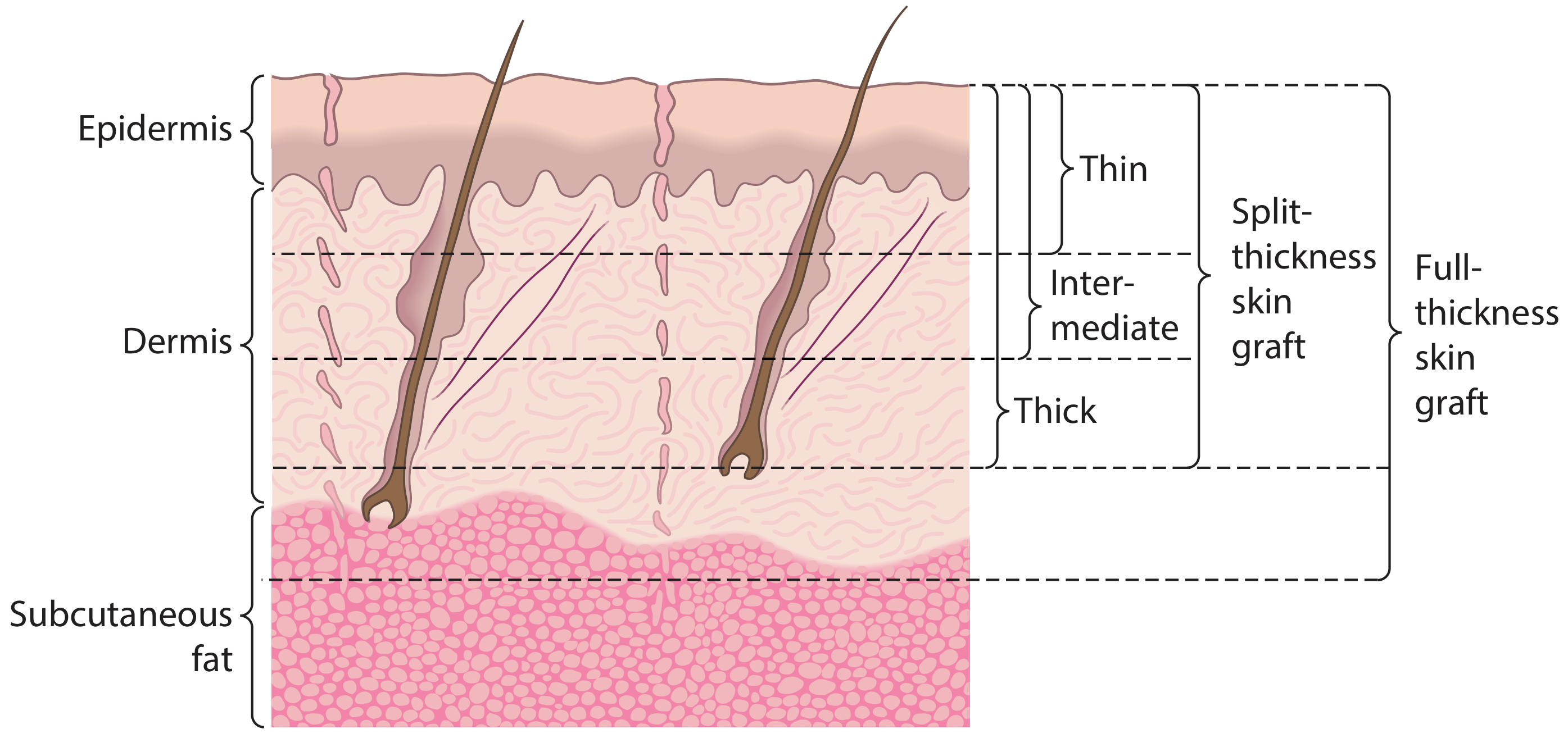
Split Thickness Skin Graft (STSG) - Principles
1. Definition and Composition
A split thickness skin graft consists of the entire epidermis plus a variable portion of the dermis (but not the full dermis). It does NOT include subcutaneous fat. Depending on how much dermis is included, STSGs are classified as:
- Thin (0.15-0.3 mm)
- Intermediate/medium (0.3-0.45 mm)
- Thick (0.45-0.6 mm)
Usual harvesting thickness ranges from 0.012 to 0.016 inches (approximately 0.3-0.4 mm).
2. Harvesting
- Donor sites: Thigh and buttocks are most commonly used; scalp is another option.
- Instrument: Harvested with a dermatome (electric, air-powered, or manual/Humby knife) set to the desired depth.
- Because only part of the dermis is taken, adnexal structures (hair follicles, sweat glands) remain in the donor site, allowing spontaneous re-epithelialization of the donor wound.
- Donor site wound care should promote re-epithelialization by keeping the wound moist (occlusive semi-permeable dressings).
3. Graft Take - The Biological Process
"Take" is the process by which a graft becomes permanently integrated. It occurs in four stages:
| Stage | Time | Mechanism |
|---|---|---|
| Graft adherence | Immediate | Graft adheres to recipient bed via a fibrin layer |
| Serum (plasmatic) imbibition | 0-48 hours | Graft survives by absorbing nutrients diffusing from plasma leaking from capillaries in the recipient bed; graft gains weight and swells |
| Revascularization | 48 hours - 3 weeks | Re-establishment of blood supply via three mechanisms (see below) |
| Remodelling | 3 weeks - 1 year | Maturation with collagen reorganization and increasing tensile strength |
Mechanisms of Revascularization:
- Inosculation: Joining of cut vessel ends in the graft with those in the recipient bed - the most critical phase; disruption here causes graft failure.
- Revascularization: Ingrowth of new vessels from the recipient bed producing new vascular channels within the graft.
- Neovascularization: Degeneration of old vessel endothelium leaving behind basement membranes, which act as conduits for new capillary bud growth.
4. Principles of Successful Take
For a graft to "take," three conditions must be met:
a) Adequate Recipient Bed
- Healthy granulation tissue, muscle, fascia, and periosteum-covered bone are good recipient beds.
- Exposed bone (without periosteum), bare tendon, and cartilage will not support a graft.
- If bone is exposed, it can be burred to create pinpoint bleeding ("pinpoint bleeding diploic bone") to facilitate take.
b) Immobilization and Contact
- The graft must maintain direct, uninterrupted contact with the recipient bed.
- Shear forces must be avoided - tie-over bolster dressings, foam, VAC (negative pressure wound) dressings are used.
- Haematoma and seroma are the most common causes of graft loss - they lift the graft off the bed and prevent vascular ingrowth. Prevention: meticulous haemostasis + meshing/fenestrating the graft.
c) Freedom from Infection
- Wounds with >10^5 organisms/gram of tissue will not support a graft.
- Key pathogens that destroy fibrin and prevent adherence: Streptococcus pyogenes, Pseudomonas aeruginosa, MRSA.
5. Contraction
- Primary contraction: Occurs immediately after harvesting due to elastic recoil of dermis. STSGs contract less primarily than FTSGs (less dermis = less elastin).
- Secondary contraction: Occurs after revascularization, driven by myofibroblast activity in the wound bed. STSGs undergo more secondary contraction than FTSGs (less dermis = less resistance to myofibroblast pull).
- Thinner STSGs contract more; thicker STSGs contract less but have lower reliability of take.
6. Characteristics and Limitations of STSG
| Feature | STSG |
|---|---|
| Chance of successful take | Higher (less metabolic demand) |
| Contraction | More secondary contraction |
| Colour match | Abnormal pigmentation |
| Trauma resistance | Poor |
| Sensory recovery | Poor (fewer neurilemmal sheaths) |
| Hair growth | None (hair follicles absent) |
| Donor site healing | Spontaneous re-epithelialization |
| Coverage area | Large areas possible; can be meshed |
7. Meshing
- STSGs can be meshed (cut in a lattice pattern) to expand the graft area (e.g., 1:1.5, 1:3, 1:6 expansion ratios).
- Meshing allows fluid drainage (preventing haematoma/seroma), increases coverage area, and improves graft conformation to irregular surfaces.
- Interstices fill by re-epithelialization but leave a characteristic "mesh" appearance.
8. Applications
- Burns (large surface area coverage)
- Small defects of the oral cavity
- Maxillectomy defects (internal lining)
- Coverage of free flap donor sites
- Large scalp defects (where galea or periosteum is intact)
- Auricular defects (applied to intact perichondrium)
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 91
- Schwartz's Principles of Surgery, 11th Ed.
- K.J. Lee's Essential Otolaryngology, 11th Ed.
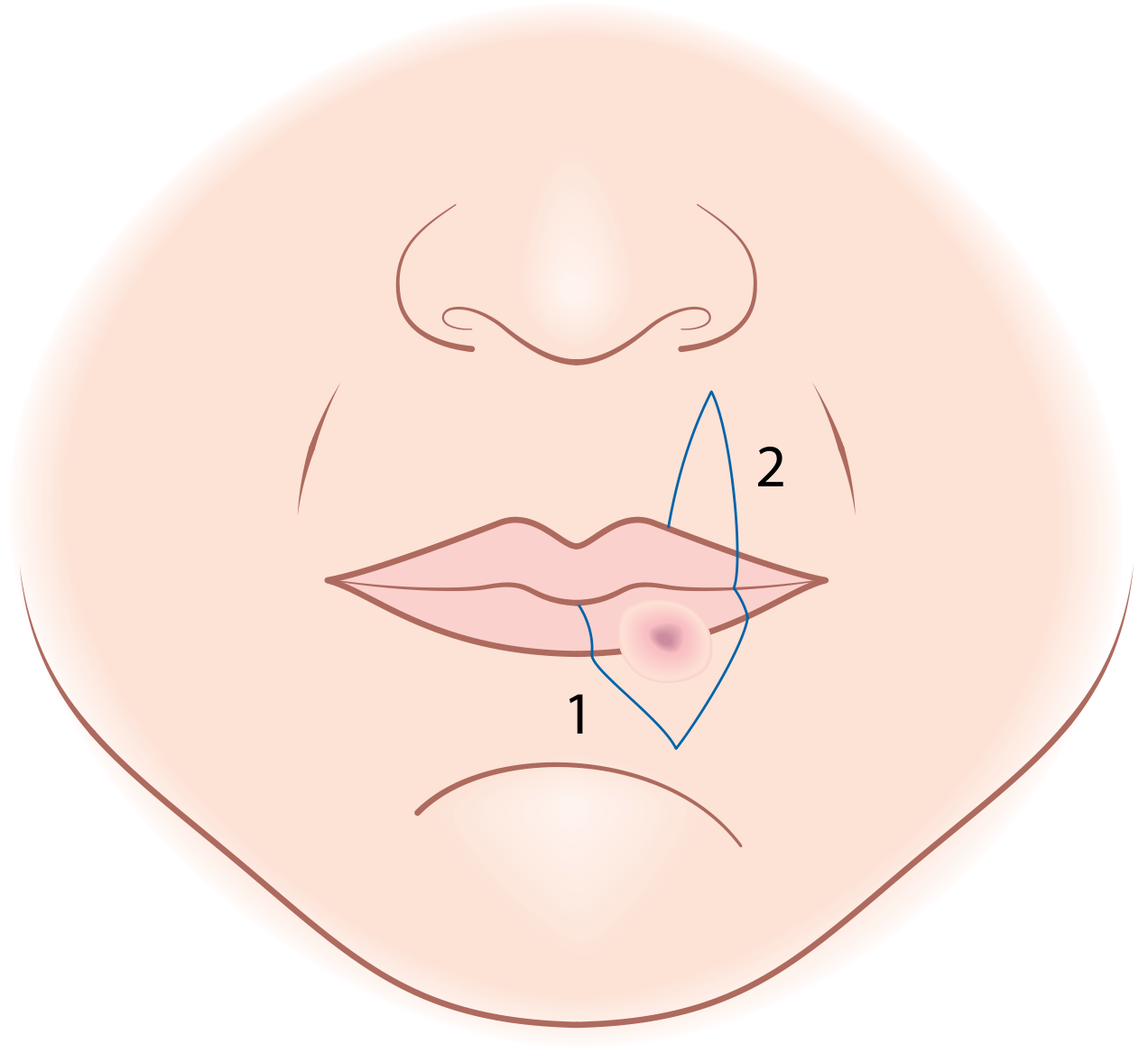
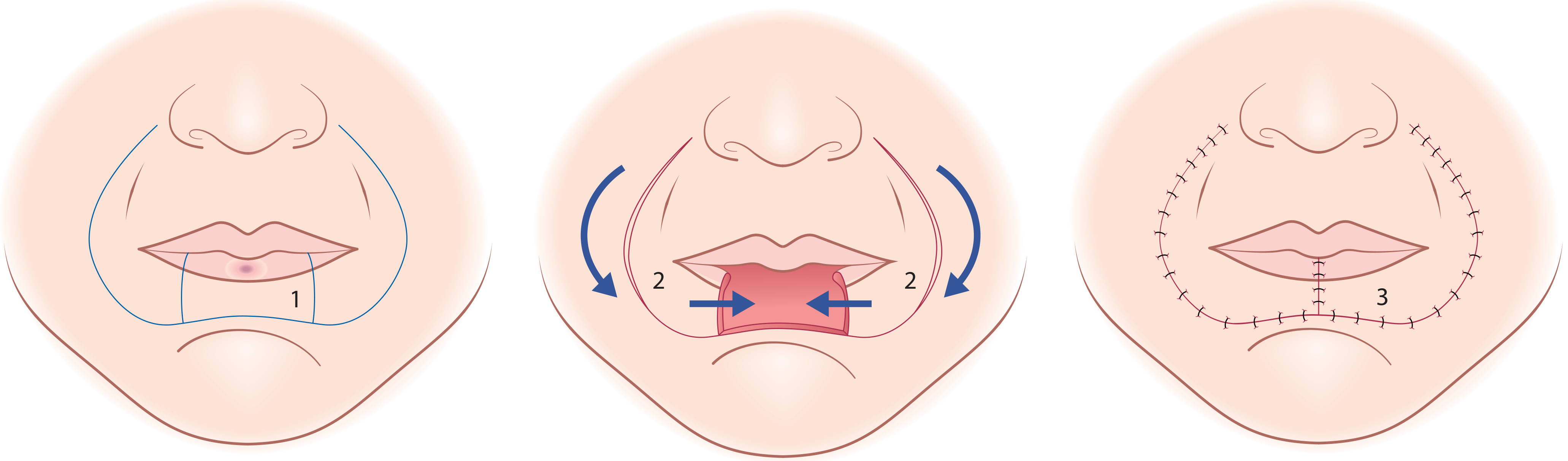
Local flaps for reconstruction of lip
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete and organized answer on Local Flaps for Reconstruction of the Lip:
Local Flaps for Lip Reconstruction
General Principles
The typical lip length is 6-8 cm. Reconstructive choice is guided primarily by the proportion of lip resected:
| Defect Size | Reconstruction |
|---|---|
| Up to 1/3 (< 30%) of lip | Wedge excision + primary closure |
| 1/3 to 2/3 (30-60%) | Lip switch flaps (Abbe, Estlander) |
| > 2/3 (> 60%) to total | Karapandzic, Bernard-Burow, Gilles fan flap |
Key goals: oral competence, dynamic function (orbicularis continuity), acceptable cosmesis, preservation of commissures where possible.
1. Abbe Flap (Abbe-Sabattini Flap) - Lip Switch
Indication: Defects of 1/3 to 2/3 of the lower or upper lip NOT involving the commissure.
Design:
- A full-thickness flap from the opposite lip (lower lip defect -> upper lip donor, or vice versa).
- Flap width = half the width of the defect (to distribute loss equally between both lips).
- Pedicle is based on the labial artery (kept on one lateral edge of the flap).
Technique:
- A full-thickness wedge or rectangular flap is raised from the donor lip with a medial or lateral arterial pedicle intact.
- The flap is rotated 180° and inset into the recipient defect.
- The pedicle is divided at a second stage after 7-14 days once the flap has established its blood supply.
Advantages:
- Brings like-for-like tissue (vermilion, muscle, mucosa).
- Preserves both commissures - no blunting.
Disadvantages:
- Two-stage procedure.
- Creates an insensate, adynamic segment (some reinnervation occurs over time).
- Better suited for upper lip reconstruction.
2. Estlander Flap
Indication: Defects of the lateral lip involving or close to the oral commissure (lateral 1/3).
Design: Similar to the Abbe flap but the pedicle crosses at the commissure, making it a single-stage procedure.
Technique:
- Full-thickness flap from the opposite lip, rotated around the commissure to fill the lateral defect.
- No pedicle division required - the commissure provides the pivot point.
Key difference from Abbe: Single-stage, but the reconstructed commissure is blunted and may require secondary commissuroplasty.
Disadvantage: Blunting of the oral commissure (rounded, less defined angle).
3. Karapandzic Flap
Indication: Defects of > 1/3 to total lower lip (can reconstruct up to total lip loss). Best for central lower lip defects when tissue laxity allows.
Design:
- Paired full-thickness mucomusculocutaneous circumoral advancement-rotation flaps on both sides.
- Flaps are based on branches of the facial artery.
- Incisions are made equidistant from the free lip margin around the commissure - the distance from lip margin must equal the height of the lip defect to restore normal lip height.
- Superior incisions are placed lateral to the nasolabial creases.
- Mucosal incisions are parallel but much shorter (~2 cm on each side).
Technique:
- For central defects: lip depressor muscles divided bilaterally to allow medial advancement.
- For large defects: superior incisions deepened through skin, fat, and superficial facial muscles. Buccinator and orbicularis oris are preserved.
- Neurovascular bundles (sensory and motor nerves, labial vessels) are carefully preserved radially - nerves enter the flaps radially.
- After rotation, superficial muscle layer is reattached to the orbicularis.
- Wounds closed in layers (mucosa -> muscle -> skin).
Advantages:
- Preserves neurovascular supply - results in a sensate, functional lip.
- Best functional outcomes of all lip reconstruction techniques.
- Single stage.
Disadvantage:
- Microstomia is inevitable with large defects - secondary revision may be required.
- Not suitable when tissue laxity is poor.
4. Johanson's Step Technique
Indication: Central lower lip defects only.
Technique:
- Lesion removed as a rectangle; remaining lateral lower lip segments are advanced medially.
- Square/rectangular segments of skin and subcutaneous tissue lateral to the defect are excised in a descending stepwise fashion along the labiomental crease.
- Each step excised is approximately half the width of the defect.
- Final caudal segment is triangular.
- Flaps advance medially as steps are closed.
- Orbicularis is carefully reconstructed.
Functional results: Comparable to Karapandzic, but scarring can appear unnatural. Large defects lead to microstomia.
5. Bernard-von Burow Procedure (and Freeman Modification)
Indication: Large defects up to total lower lip reconstruction when Karapandzic is insufficient or tissue laxity is poor.
Principle: Reconstructs the lower lip by medially advancing both cheeks.
Technique:
- Full-thickness triangular Burow's triangles of cheek tissue are excised above and below the defect at the nasolabial fold.
- Width of each triangle = half the width of the lip defect.
- This releases tension and allows bilateral medial cheek advancement.
- Vermillion is reconstructed by tongue flaps (or cheek mucosa in Webster's modification).
Freeman Modification (preferred current technique):
- Converts the lower incision from horizontal to curved, following the natural lip-chin junction.
- Only skin and fat are excised in the triangular areas (not full thickness medially).
- A unilateral version can also be used for lateral defects combined with a contralateral Karapandzic flap for subtotal defects.
Disadvantage: Cheek skin differs in texture/colour from lip; function is always suboptimal as orbicularis continuity is not restored.
6. Gilles Fan Flap (Webster modification)
Indication: Large/total lower lip defects, particularly when Karapandzic is not feasible.
Principle: Bilateral full-thickness cheek flaps are rotated around the commissures as "fans" to reconstruct the lower lip.
Disadvantage: Does not restore neuromuscular function; results in an oral incompetence and poor cosmesis in many cases.
Summary Table
| Flap | Defect Size | Commissure | Stage | Key Feature |
|---|---|---|---|---|
| Wedge + primary closure | < 1/3 | Preserved | Single | Simplest |
| Abbe | 1/3 - 2/3, central | Preserved | Two-stage | Like-for-like tissue |
| Estlander | 1/3 - 2/3, lateral | Resected | Single | Commissure blunting |
| Karapandzic | > 1/3 to total | Preserved | Single | Sensate; neurovascular sparing |
| Johanson step | Medium-large, central | Preserved | Single | Step advancement |
| Bernard-Burow | Large to total | Resected | Single | Cheek advancement |
| Gilles fan | > 2/3 to total | Resected | Single | Fan rotation |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 12
- Cummings Otolaryngology Head and Neck Surgery, Chapter 91
- K.J. Lee's Essential Otolaryngology, 11th Ed.
- Schwartz's Principles of Surgery, 11th Ed.
Enumerate principle of management of cleft lip and palate
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive material from multiple authoritative textbooks. Here is the complete answer:
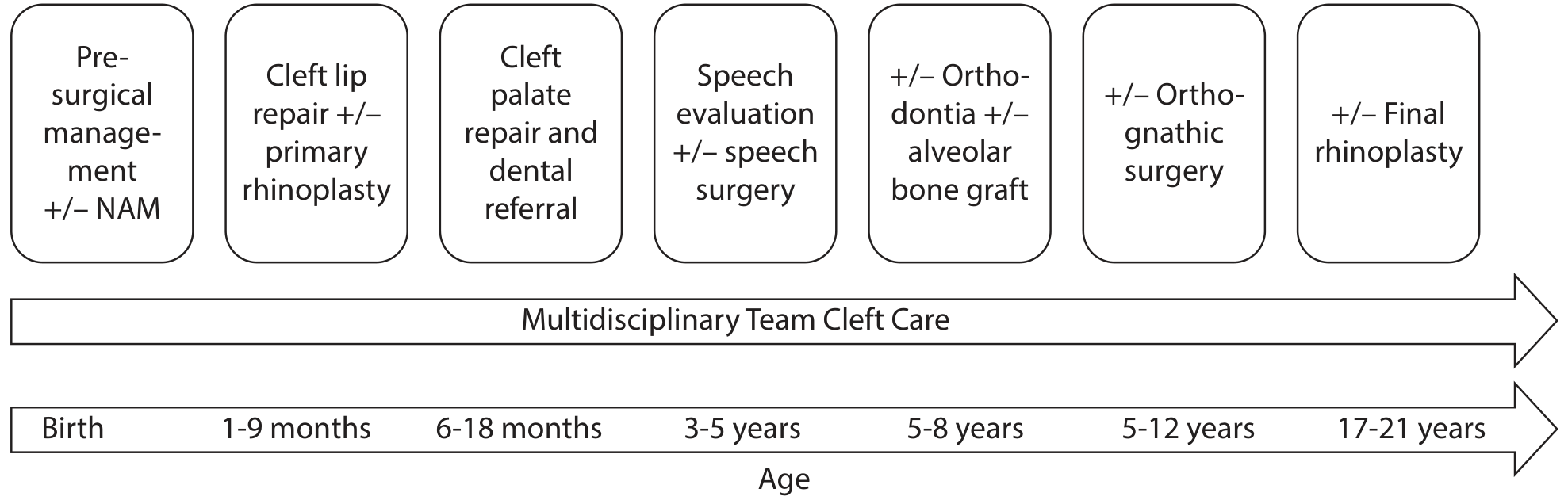
Principles of Management of Cleft Lip and Palate
I. Overarching Principles
-
Multidisciplinary team approach - Management requires coordinated input from: surgeon (plastic/craniofacial/ENT), pediatrician, geneticist, feeding specialist, speech and language pathologist, orthodontist, oral and maxillofacial surgeon, audiologist, psychologist, and social worker.
-
Staged, lifelong management - Treatment is not a single operation but a series of planned interventions from birth through early adulthood.
-
Goals of management:
- Normal lip closure and symmetry
- Patent nasal airway
- Age-appropriate speech (avoid velopharyngeal insufficiency)
- Normal eustachian tube function and hearing
- Normal dental occlusion
- Optimal symmetry of lip, nose, and midface
- Psychosocial well-being
II. Prenatal Management
- Diagnosis possible on routine ultrasonography from ~18 weeks (2D + 3D improves accuracy; cleft lip more reliably diagnosed than cleft palate).
- Parents are referred to the cleft team for antenatal counseling - most families find this helpful in planning care.
- Screen for associated anomalies: >15% of fetuses will have other abnormalities; >500 syndromes have facial clefts as associations.
- Genetic evaluation is recommended - consider van der Woude syndrome (most common syndromic cause of cleft lip), Pierre Robin sequence, 22q11.2 deletion, Stickler syndrome.
III. Neonatal / Early Management (Birth)
-
Feeding:
- Breastfeeding is generally not possible with cleft palate.
- Specialized feeding bottles with modified nipples (Haberman feeder, pigeon-type nipple) that control flow rate are used.
- Monitor for adequate weight gain.
-
Airway:
- Especially important in Pierre Robin sequence (micrognathia + glossoptosis + U-shaped cleft palate).
- Positioning (prone), nasal trumpet, or mandibular distraction may be required.
-
Hearing assessment: Screen for congenital sensorineural and conductive hearing loss. Eustachian tube dysfunction is associated with cleft palate in 95-100% of patients.
-
Presurgical orthopaedics (started within first 1-2 weeks of life):
- Lip taping: Application of tape across the cleft to narrow the gap width, reduce tension on closure, and improve surgical outcomes. Useful in wide unilateral or bilateral complete cleft lip.
- Nasoalveolar molding (NAM): A palatal appliance fabricated by a trained orthodontist, adjusted weekly over 2-3 months.
- Gradually narrows the palatal cleft width.
- Nasal posts added later to guide nasal tip and alar cartilage repositioning (improves symmetry in unilateral cleft; elongates short columella in bilateral cleft).
- Definitive surgical repair follows NAM treatment.
IV. Cleft Lip Repair (1-9 Months)
Timing: Based on the Rule of Tens:
- Age > 10 weeks
- Weight > 10 pounds (4.5 kg)
- Haemoglobin > 10 g/dL
Surgical goals:
- Restore function of the orbicularis oris muscle (functional sphincter)
- Alignment and recreation of the philtral ridges, Cupid's bow, white roll, and mucocutaneous ridge
- Reconstruction of the nasal floor
- Symmetric alar base
Technique - Millard Rotation-Advancement (most widely used for unilateral cleft):
- Downward rotation of the medial lip segment + medial advancement of the lateral segment into the defect.
- Orbicularis oris released from abnormal attachments (alar base and columella) and approximated to form a functional sphincter.
- Alar base on cleft side released and realigned.
- Meticulous mucocutaneous border alignment.
- Primary rhinoplasty may be performed simultaneously to improve nasal symmetry.
Bilateral cleft lip repair - additional goals:
- Reconstruction of a functional muscular sphincter
- Symmetric alar base narrowing
- Creation of a philtral column with adequate columella length
- One-stage or two-stage repair (lip adhesion early, definitive repair later)
V. Cleft Palate Repair and Dental Referral (6-18 Months)
Timing:
- Repaired before 18 months of age (standard in most centres; typically 6-16 months).
- Balance between: late repair (impairs speech development) vs. early repair (may impair maxillary growth).
Surgical goals:
- Restore normal palatal anatomy
- Reconstruct the levator veli palatini muscle sling (intravelar veloplasty) - key to eustachian tube function and speech
- Achieve a watertight, tension-free 3-layer closure (nasal mucosa, muscle, oral mucosa)
Common techniques:
| Technique | Description |
|---|---|
| Von Langenbeck palatoplasty | Bilateral bipedicled mucoperiosteal flaps advanced medially; preserves greater palatine vessels |
| Two-flap palatoplasty (Bardach) | Two large mucoperiosteal flaps pedicled on greater palatine vessels; good hard palate closure |
| Furlow double-opposing Z-plasty | Two opposing Z-plasties in soft palate; lengthens the palate and reconstructs the muscle sling; better VPI outcomes |
| Veau-Wardill-Kilner (V-Y pushback) | Pushes palate posteriorly to increase length; greater risk of fistula |
Complications:
- Oronasal fistula: up to 10%
- Velopharyngeal insufficiency (VPI): up to 25% (hypernasal speech, nasal emission, nasal regurgitation during phonation)
VI. Otological Management (Ongoing)
- Chronic otitis media with effusion (COME) affects 95-100% of cleft palate patients.
- Mechanism: abnormal tensor veli palatini and levator veli palatini -> poor eustachian tube function.
- Pressure equalization (PE/grommet) tubes are placed, often at the time of lip repair.
- Middle ear disease frequently improves after palate repair and with age.
- Regular audiological monitoring throughout childhood.
VII. Speech and Language Evaluation (3-5 Years)
- Speech issues occur in ~25% of cleft palate patients.
- All patients need aggressive speech and language pathology evaluation from early infancy.
- VPI management:
- Speech therapy for compensatory articulation errors.
- If VPI persists despite palatoplasty: pharyngoplasty (sphincter pharyngoplasty or posterior pharyngeal wall augmentation) or palate re-repair.
VIII. Orthodontic Management and Alveolar Bone Grafting (5-12 Years)
- Alveolar bone grafting performed at age 5-8 years (before eruption of permanent canine teeth - mixed dentition phase).
- Autologous cancellous bone (iliac crest) grafted into the alveolar cleft.
- Provides bony support for eruption of permanent teeth and nasal alar base.
- Palatal expansion and dental alignment with orthodontic appliances.
- Timing coordinated with dental development.
IX. Orthognathic Surgery (12-17 Years)
- For midface (maxillary) hypoplasia and malocclusion - a common consequence of early palate repair.
- Le Fort I osteotomy with advancement to correct midface retrusion.
- Performed after completion of facial growth (girls ~15-16 years, boys ~17-18 years).
X. Final Rhinoplasty (17-21 Years)
- Definitive cosmetic and functional rhinoplasty after skeletal growth is complete.
- Addresses residual nasal asymmetry, alar base asymmetry, and tip deformity from the original cleft nasal anatomy.
Summary Timeline
| Age | Intervention |
|---|---|
| Prenatal | Diagnosis, counseling, genetic evaluation |
| Birth | Feeding support, airway, hearing screen |
| 0-2 weeks | Lip taping, NAM |
| 1-9 months | Cleft lip repair +/- primary rhinoplasty |
| 6-18 months | Cleft palate repair + dental referral |
| 3-5 years | Speech evaluation +/- VPI surgery |
| 5-8 years | Orthodontia +/- alveolar bone graft |
| 5-12 years | Orthodontic treatment, palate expansion |
| 12-17 years | +/- Orthognathic surgery |
| 17-21 years | +/- Final definitive rhinoplasty |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 188
- K.J. Lee's Essential Otolaryngology, Chapter 52
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
- Schwartz's Principles of Surgery, 11th Ed.
Musculocutaneous flap
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive answer on Musculocutaneous Flaps:
Musculocutaneous (Myocutaneous) Flap
1. Definition
A musculocutaneous flap (also called a myocutaneous flap) is a composite unit of skin, subcutaneous tissue, and the underlying muscle, all elevated and transferred together on the muscle's dominant vascular pedicle. The skin survives because musculocutaneous perforator vessels pass from the muscle through the overlying subcutaneous fat to supply the skin island.
The correct terminology is:
- The muscle is the actual flap (the vascular carrier).
- The skin is referred to as the skin island or paddle - it is a "passenger" on the muscle.
2. Vascular Anatomy
The key feature distinguishing musculocutaneous from other flaps is the route of blood supply to the skin:
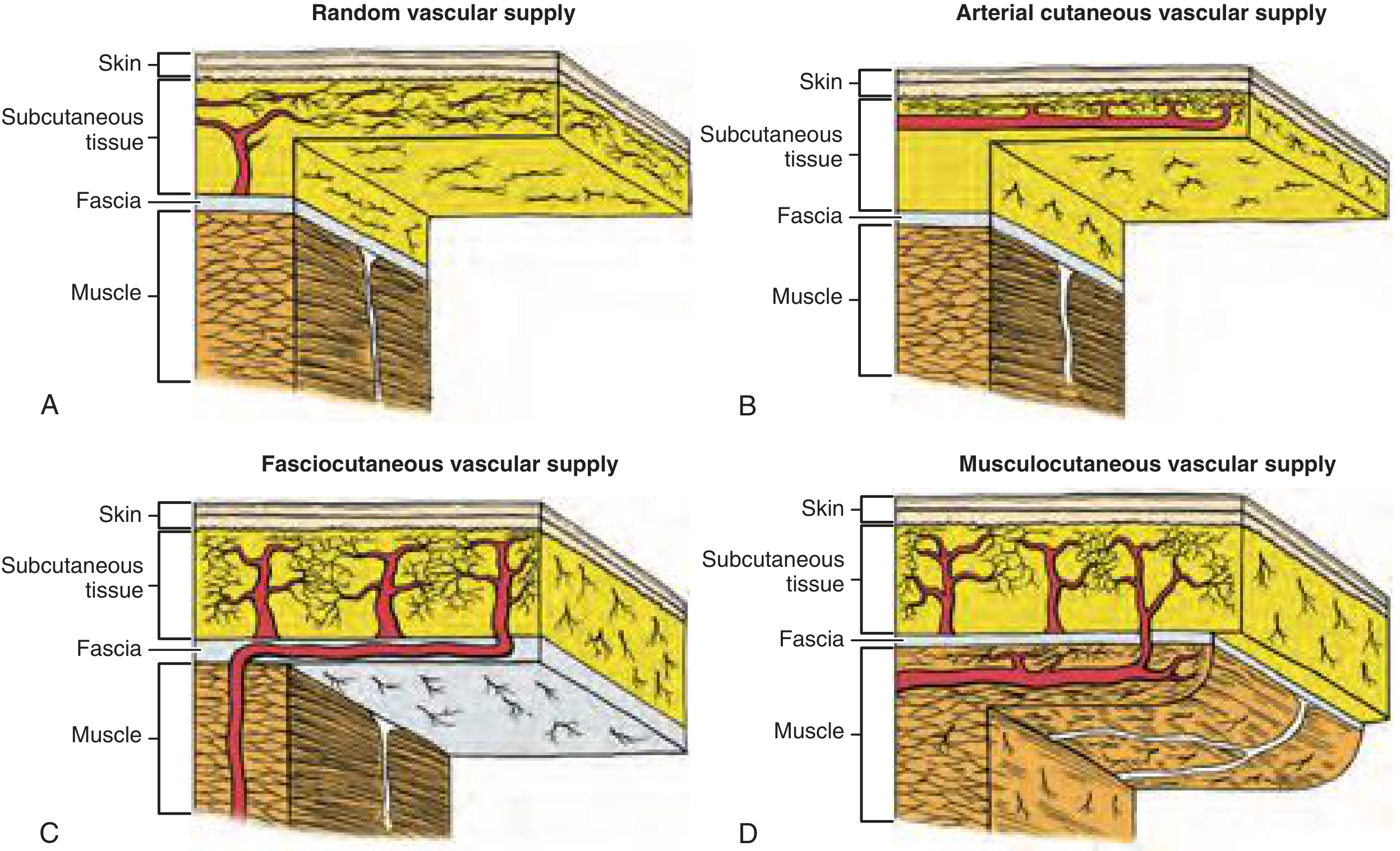
| Flap Type | Blood Supply Route |
|---|---|
| Random cutaneous | Subdermal plexus from unnamed perforators at base |
| Axial (arterial cutaneous) | Named septocutaneous artery in subcutaneous fat |
| Fasciocutaneous | Deep fascia plexus -> subdermal plexus |
| Musculocutaneous | Dominant muscle pedicle -> musculocutaneous perforators -> through muscle -> subdermal plexus |
The greater blood flow and higher tissue oxygen tensions in musculocutaneous flaps make them superior to random-pattern flaps, especially in contaminated or infected wounds, due to improved phagocytic and bactericidal leukocyte activity.
3. Mathes and Nahai Classification of Muscle Blood Supply
Muscles are classified by Mathes and Nahai (1981) into 5 types based on their vascular anatomy. This determines arc of rotation, reliability, and whether the muscle can be used as a flap:
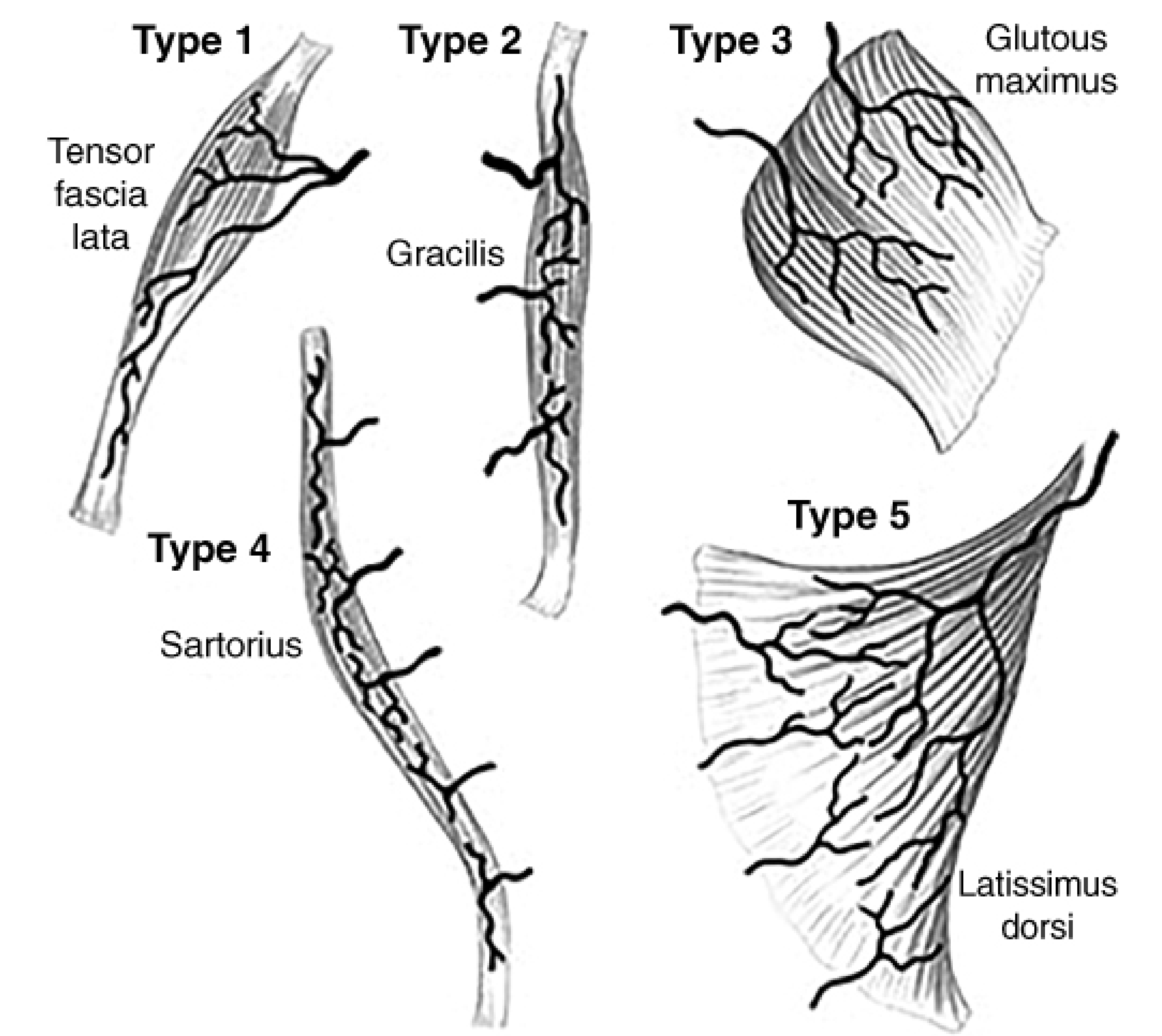
| Type | Vascular Supply | Example Muscles |
|---|---|---|
| I | One (single) dominant pedicle | Gastrocnemius, Tensor fascia lata |
| II | One dominant + minor pedicle(s) | Gracilis, Soleus, Platysma |
| III | Two dominant pedicles | Rectus abdominis, Gluteus maximus, Serratus anterior |
| IV | Multiple segmental pedicles (no dominant) | Sartorius, Tibialis anterior |
| V | One dominant + secondary segmental pedicles | Latissimus dorsi, Pectoralis major |
- Types I, II, and V are most suitable for musculocutaneous flaps, as they have a reliable dominant pedicle that can support the entire muscle and overlying skin.
- Type IV muscles are generally not suitable as pedicled flaps - the segmental supply means division of any pedicle devascularizes part of the muscle.
4. Advantages of Musculocutaneous Flaps
- Reliable, well-vascularized tissue - high oxygen delivery to the flap.
- Resistant to infection - improved leukocyte function; can be placed in contaminated/infected beds.
- Bulk - provides volume to fill dead space (e.g., after radical neck dissection, sternal wounds).
- Can reach distant defects when rotated on pedicle.
- Single-stage transfer for pedicled flaps.
- Can carry bone (osteomyocutaneous flap) if periosteum included.
- Can be sensate if the sensory nerve is included.
- Can be used as pedicled or free flap (microvascular transfer).
5. Disadvantages
- Donor site morbidity - functional loss of the harvested muscle.
- Bulky - may be too thick for some defects (e.g., intraoral reconstructions in obese patients).
- Limited arc of rotation for pedicled flaps.
- Skin paddle necrosis can occur even when the muscle survives (the skin is the most vulnerable part of the flap).
- Poor colour/texture match with the recipient site skin.
- Muscle atrophy over time (especially after denervation), leading to volume loss.
6. Common Musculocutaneous Flaps
A. Pectoralis Major Myocutaneous Flap (PMMC)
- Vascular supply: Pectoral branch of the thoracoacromial artery (Type V muscle - dominant) + lateral thoracic artery.
- Skin paddle: Designed medial to the nipple, at the level of the 6th rib; infra-mammary placement preferred in females.
- Uses in head and neck: Oral cavity, oropharynx, pharyngeal defects, neck coverage, salvage after free flap failure.
- Advantages: Reliable, large skin paddle, long pedicle, easy harvest.
- Disadvantages: Bulky in females; creates chest deformity; limited reach in upper neck.
B. Latissimus Dorsi Myocutaneous Flap
- First myocutaneous flap described in the medical literature (Tanzini, repopularized by Olivari 1976).
- Vascular supply: Thoracodorsal artery (branch of subscapular artery from axillary artery) - Type V.
- Thoracodorsal artery divides into superior and lateral branches within the muscle - allowing the muscle to be split into two independent units.
- Skin paddle: Up to 40 x 20 cm (though defects >10 x 8 cm require skin grafting of donor site).
- Uses: Shoulder/chest wall defects, breast reconstruction (+ implant), head and neck (up to zygomatic arch level), axilla coverage.
- Can be used as pedicled or free flap - pedicle length >10 cm; subscapular artery diameter ~3 mm.
C. Rectus Abdominis Myocutaneous Flap (RAM/TRAM/VRAM)
- Vascular supply: Type III - dual dominant supply:
- Superior epigastric artery (continuation of internal mammary)
- Deep inferior epigastric artery (DIEA - dominant for free flap)
- TRAM flap (Transverse Rectus Abdominis Myocutaneous) - skin paddle oriented transversely; used for breast reconstruction.
- VRAM flap (Vertical RAM) - skin paddle oriented vertically; used for chest wall, perineal, and pelvic defects.
- Can be converted to a DIEP flap (deep inferior epigastric perforator) - muscle-sparing variant.
D. Gastrocnemius Myocutaneous Flap
- Vascular supply: Type I - single dominant pedicle (sural branches of popliteal artery).
- Medial head: Larger, more commonly used.
- Uses: Coverage of proximal third of tibia, knee joint, exposed prosthesis.
- Skin paddle placed over the muscle belly.
E. Trapezius Myocutaneous Flap
- Based on the transverse cervical artery (upper flap) or dorsal scapular artery (lower flap).
- Used in head and neck reconstruction, especially posterior scalp defects.
F. Gracilis Myocutaneous Flap
- Vascular supply: Type II - dominant medial circumflex femoral artery + minor pedicles from superficial femoral.
- Used for perineal, vaginal, and limb reconstruction; also as functional free muscle transfer.
7. Indications for Musculocutaneous Flaps
- Coverage of large soft tissue defects after tumor resection (oral cavity, pharynx, neck)
- Infected or contaminated wounds (osteomyelitis, sternal dehiscence)
- Radiation-damaged tissue beds
- Pressure sore coverage (gluteus maximus, tensor fascia lata)
- Breast reconstruction (latissimus dorsi, TRAM)
- Limb salvage (gastrocnemius, soleus)
- Perineal reconstruction (gracilis, VRAM, gluteus)
- Chest wall reconstruction (pectoralis, latissimus, rectus)
8. Causes of Flap Failure
- Pedicle compression/kinking
- Hematoma beneath the flap
- Infection
- Excessive tension
- Venous congestion (more common than arterial insufficiency)
- Random extension of the skin paddle beyond the vascular territory
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 77
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 92
- Fischer's Mastery of Surgery, 8th Ed., Chapter 74
- Rockwood and Green's Fractures in Adults, 10th Ed.
- Hinman's Atlas of Urologic Surgery
Principle of reconstruction in head and neck surgery
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive, authoritative material from multiple textbooks. Here is the complete answer:
Principles of Reconstruction in Head and Neck Surgery
I. Overview and Goals
Head and neck cancer resection, trauma, and infection create defects that can severely affect a patient's quality of life - impacting speech, swallowing, respiration, facial expression, and cosmesis. The ideal reconstruction replaces resected tissue with tissue that matches the quality and function of what was lost ("like with like").
Overarching goals:
- Reliable wound coverage - prevent exposure of vital structures (carotid artery, brain, orbit)
- Restore function - airway patency, oral competence, swallowing, speech, eustachian tube function
- Acceptable cosmesis - respect facial cosmetic subunits, relaxed skin tension lines
- Minimize donor site morbidity
- Allow adjuvant treatment (radiotherapy) to proceed without delay
- Preserve patient quality of life and social re-integration
II. The Reconstructive Ladder
The reconstructive ladder organizes options from simplest to most complex. The surgeon begins at the lowest rung that adequately addresses the defect.
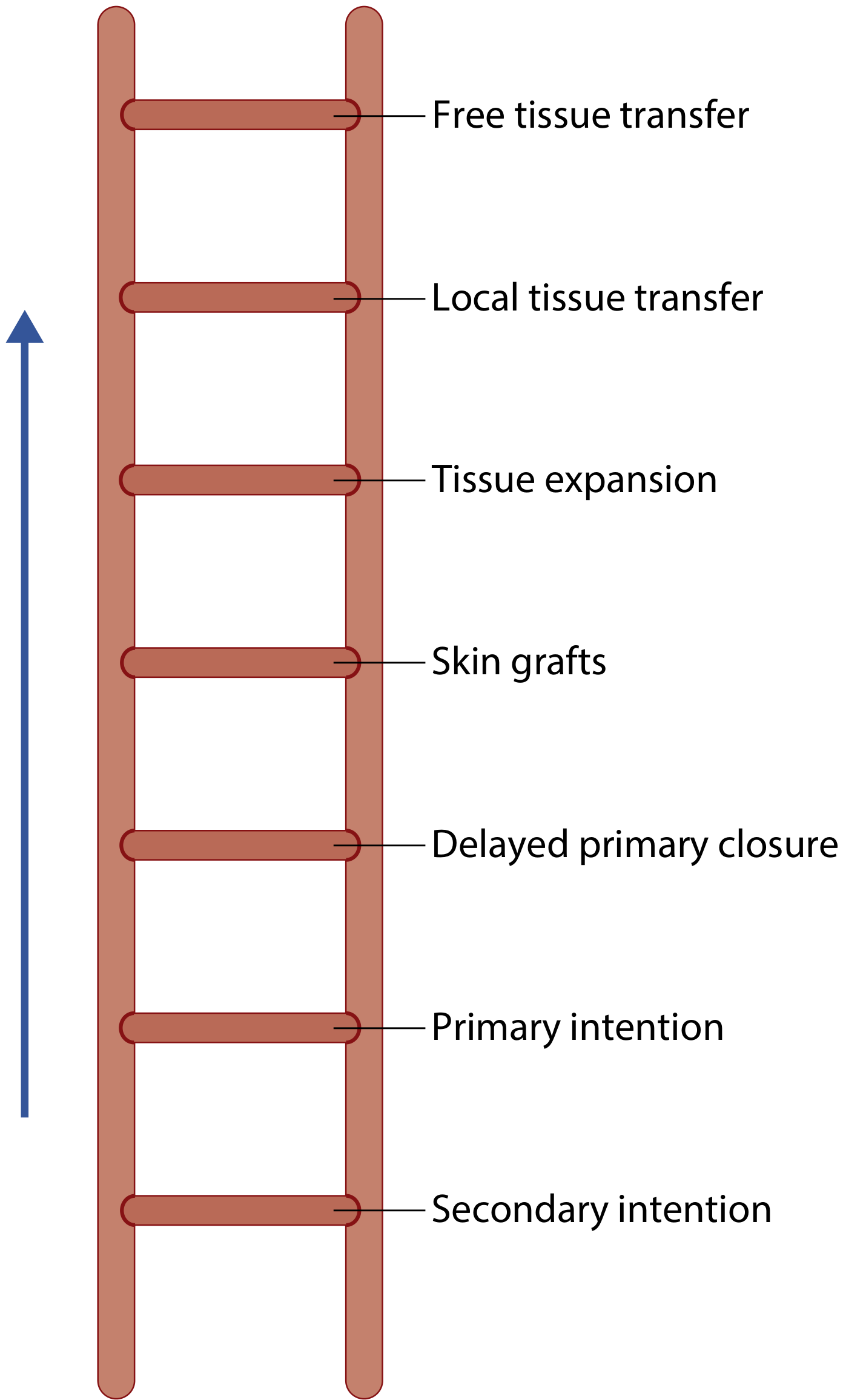
| Rung (Simple → Complex) |
|---|
| Secondary intention healing |
| Primary intention (direct closure) |
| Delayed primary closure |
| Skin grafts (STSG / FTSG) |
| Tissue expansion |
| Local flaps |
| Regional (pedicled) flaps |
| Free microneurovascular tissue transfer |
The "Reconstructive Elevator": In some situations, rungs should be skipped. For example, a neck defect with exposed carotid vessels after tumour excision warrants a pedicled or free flap directly - not a skin graft - even though the graft would technically "take." The modern approach does not climb the ladder rung by rung but selects the best option for the individual patient and defect.
III. Defect Analysis (Pre-operative Assessment)
Before choosing a reconstructive strategy, a thorough defect analysis is mandatory:
A. Tissue components missing:
- Skin / mucosa
- Muscle
- Bone / cartilage
- Nerve(s)
- Composite combinations
B. Structural and functional requirements of the recipient site:
- Bone stock for skeletal framework and osseointegration (dental implants)
- Soft tissue coverage of vital structures (carotid, dura, orbit)
- Muscle continuity (e.g., orbicularis oris for oral competence)
- Pliability of tissues (tongue, soft palate need mobile, flexible tissue)
- Volume restoration (e.g., total glossectomy, orbital exenteration)
- Secretory mucosal surface (salivary function)
- Potential for sensate reconstruction
- Vascularized tissue to treat fistulae, osteomyelitis, osteoradionecrosis
C. Special conditions at the wound site:
- Previous irradiation (impairs wound healing; demands vascularized flap)
- Infection or fistulae
- Prior surgery / scarring (limits local tissue availability)
D. Patient factors:
- Comorbidities (diabetes, peripheral vascular disease, immunosuppression, smoking)
- Nutritional status (hypoalbuminaemia impairs healing)
- Age and performance status
- Donor site suitability (prior abdominal surgery, peripheral vascular disease of limb)
- Mental status and patient wishes
IV. Principles of Wound Closure
1. Relaxed Skin Tension Lines (RSTLs)
- Incisions placed parallel to natural wrinkle lines (perpendicular to underlying muscle fibres) minimize scar tension and give the best cosmetic result.
- Scars crossing areas of mobility (e.g., oral commissure, lower eyelid) risk contracture.
2. Cosmetic Subunits of the Face
- The face is divided into cosmetic subunits (forehead, nose, eyelids, cheek, lip, chin, ear).
- Reconstruct each subunit separately where possible; scars should not cross subunit boundaries.
- If >50% of a cosmetic subunit is involved, it may be preferable to excise the entire subunit and reconstruct it completely for a superior result.
3. Wedge Excision Principle
- Lesions at the free edge of composite tissues (lip, eyelid, helix) can be excised as wedges.
- Each tissue layer (mucosa, muscle, skin in lip; conjunctiva, tarsal plate, skin in eyelid) must be repaired individually in layers to restore both function and appearance.
4. "Like for Like" Replacement
- Intraoral mucosa should ideally be replaced with moist, pliable tissue.
- Bone should ideally be replaced with vascularized bone.
- Hair-bearing skin should not be used for intraoral reconstruction.
V. Reconstructive Options in Detail
1. Healing by Secondary Intention
- Relies on granulation, wound contraction (myofibroblasts), and epithelialization.
- Only possible when a viable base exists (granulating tissue, muscle, fat) - not over bare bone or tendon.
- Suitable sites (concavities, where contraction gives acceptable result):
- Medial canthal area
- Temple / lateral forehead
- Glabella
- Perinasal melolabial fold
- Concave areas of ear
- Not suitable for: free edges (lip, nasal ala, eyelid) - contraction causes distortion.
2. Primary Closure
- When sufficient tissue redundancy exists.
- Place incision parallel to RSTLs; avoid straight-line closures over mobile areas.
- Avoid excess tension - undermining improves mobility but reduces blood supply.
- Use multi-layer closure: deep layer carries load (50% final strength at 6 weeks); early removal of superficial sutures avoids suture tracks.
3. Skin Grafts
- Survive by plasmatic imbibition then inosculation and revascularization from recipient bed.
- Contraindicated in irradiated and infected wound beds.
- Suitable receptor beds: fat, muscle, fascia, periosteum, perichondrium.
- Conditions for take: immobilization (bolsters/VAC), haematoma prevention (meshing/pie holes), freedom from infection.
- STSG - more secondary contraction; suitable for oral cavity, maxillectomy defects, large surface coverage.
- FTSG - better colour match, less contraction; better for visible facial defects.
4. Local Flaps
- Tissue adjacent to the defect; classified by vascular supply (random/axial) and movement (advancement, rotation, transposition, interpolated).
- Respect relaxed skin tension lines for donor site closure.
- Examples: nasolabial flap, forehead flap, paramedian forehead flap (nasal reconstruction), bilobed flap, cheek advancement.
- Cannot usually provide enough tissue for reconstruction after open major resections; increasingly used for transoral resections.
5. Regional (Pedicled) Flaps
- Tissue from adjacent areas carried on a named vascular pedicle.
- Allow single-stage coverage of large defects with well-vascularized tissue.
- Particularly useful for: contaminated/infected wounds, coverage of exposed vessels, salvage after free flap failure.
- Key flaps: pectoralis major myocutaneous (workhorse for H&N), latissimus dorsi, trapezius, deltopectoral fasciocutaneous flap.
6. Microvascular Free Tissue Transfer
- Gold standard for many complex head and neck defects.
- Allows transfer of tailored composite tissue (skin + bone + muscle + nerve) from distant donor site.
- Vascularity maintained by microvascular anastomosis to recipient vessels in the neck (commonly facial, lingual, superior thyroid, or transverse cervical arteries).
- Advantages over pedicled flaps: not limited by arc of rotation; allows precise tissue selection; less bulk distortion; can carry bone, nerve, and sensory components.
- Common free flaps:
- Radial forearm - thin, pliable; oral cavity, oropharynx, pharynx
- Anterolateral thigh (ALT) - versatile, large; oral cavity, pharynx, scalp, wide-area coverage
- Fibula - vascularized bone; mandibular and maxillary reconstruction
- Rectus abdominis (VRAM/TRAM) - large soft tissue bulk; total glossectomy, skull base
- Scapular / parascapular - reliable; composite reconstruction with bone
- Lateral arm - moderately thin; good colour match
- Free flaps have become standard of care for most major H&N defects over the past 30 years.
VI. Special Reconstructive Considerations in Head and Neck Surgery
Airway Management
- Bulky flaps and oedema after oral cavity/oropharyngeal reconstruction can compromise the upper airway in the immediate postoperative period.
- Elective tracheostomy is classically advocated as the safest option, though some centres use delayed extubation.
- Provides secure airway, allows early discontinuation of mechanical ventilation, and enables urgent reaccess if there is flap compromise.
Fistula Prevention and Management
- Pharyngocutaneous fistula is a major complication, especially after total laryngectomy with prior radiation.
- Risk factors: previous irradiation, malnutrition, hypothyroidism.
- Use of vascularized tissue to reinforce pharyngeal closure significantly reduces fistula risk.
- Established fistulas: conservative management first (wound care, enteral nutrition, nothing by mouth); operative intervention for large or infected fistulas - pectoralis major muscle flap is the gold standard for fistula closure.
Bony Defects
- Mandibular and maxillary defects compromise 3D skeletal structure, dental occlusion, and speech/swallowing.
- Require vascularized bone replacement (fibula free flap is most widely used; also scapula, iliac crest) for optimal function.
- Non-vascularized bone grafts fail in irradiated or infected beds.
Radiation Effects
- Prior radiotherapy impairs wound healing via: obliterative endarteritis, fibrosis, reduced tissue oxygenation.
- Irradiated beds require vascularized flap reconstruction - skin grafts and primary closure are unreliable.
- Osteoradionecrosis requires debridement + vascularized tissue transfer to restore blood supply.
Nutrition
- Optimisation of nutritional status is fundamental; hypoalbuminaemia impairs healing and increases fistula risk.
- Enteral feeding via nasogastric or gastrostomy tube is used perioperatively.
- Monitor and correct hypothyroidism (associated with fistula risk after laryngectomy).
VII. Summary Framework for Reconstructive Decision-Making
Defect Analysis
↓
Identify: tissue components missing + functional requirements + wound site conditions + patient factors
↓
Apply Reconstructive Ladder (or "Elevator" when appropriate)
↓
Choose simplest option that adequately:
- Provides reliable wound coverage
- Restores function
- Achieves acceptable cosmesis
- Minimises donor site morbidity
- Allows adjuvant treatment
↓
Plan contingency if primary reconstruction fails
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 91
- Cummings Otolaryngology Head and Neck Surgery, Chapters 77, 98
- K.J. Lee's Essential Otolaryngology, Chapter 55
- Sabiston Textbook of Surgery, Chapter 69
- Fischer's Mastery of Surgery, 8th Ed., Chapter 74
How will you provide cover after resection of hemi-mandible and overlying skin and mucosa for gingival sulcus tumour?
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material. Here is the complete structured answer:
Reconstruction After Hemi-mandibulectomy with Overlying Skin and Mucosa for Gingival Sulcus Tumour
Nature of the Defect
Resection of a gingival sulcus (lower alveolar) tumour invading the mandible creates a composite (three-layer) defect comprising:
- External skin of the lower face/cheek
- Mandibular bone (hemi-mandible = condyle to midline, or body + ramus)
- Intraoral mucosa (gingival sulcus, floor of mouth, buccal mucosa)
This is a high-complexity composite defect. All three layers must be addressed simultaneously. The failure to restore the bony mandible results in:
- Mandibular deviation toward the deficient side
- Malocclusion / loss of occlusal function
- Facial contour deformity
- Impaired speech and swallowing
Reconstructive Goals
- Restore mandibular continuity and facial contour
- Provide intraoral lining (watertight mucosal cover to prevent orocutaneous fistula and salivary contamination of neck)
- Provide external skin cover of the cheek/lower face
- Obliterate dead space in the neck (especially after neck dissection)
- Protect the carotid artery from exposure
- Restore mastication, speech, and swallowing function
- Allow future dental rehabilitation (osseointegrated implants)
The Gold Standard: Fibula Osteocutaneous Free Flap
The free fibula osteocutaneous flap (peroneal artery flap) is the current gold standard for composite hemi-mandibular reconstruction.
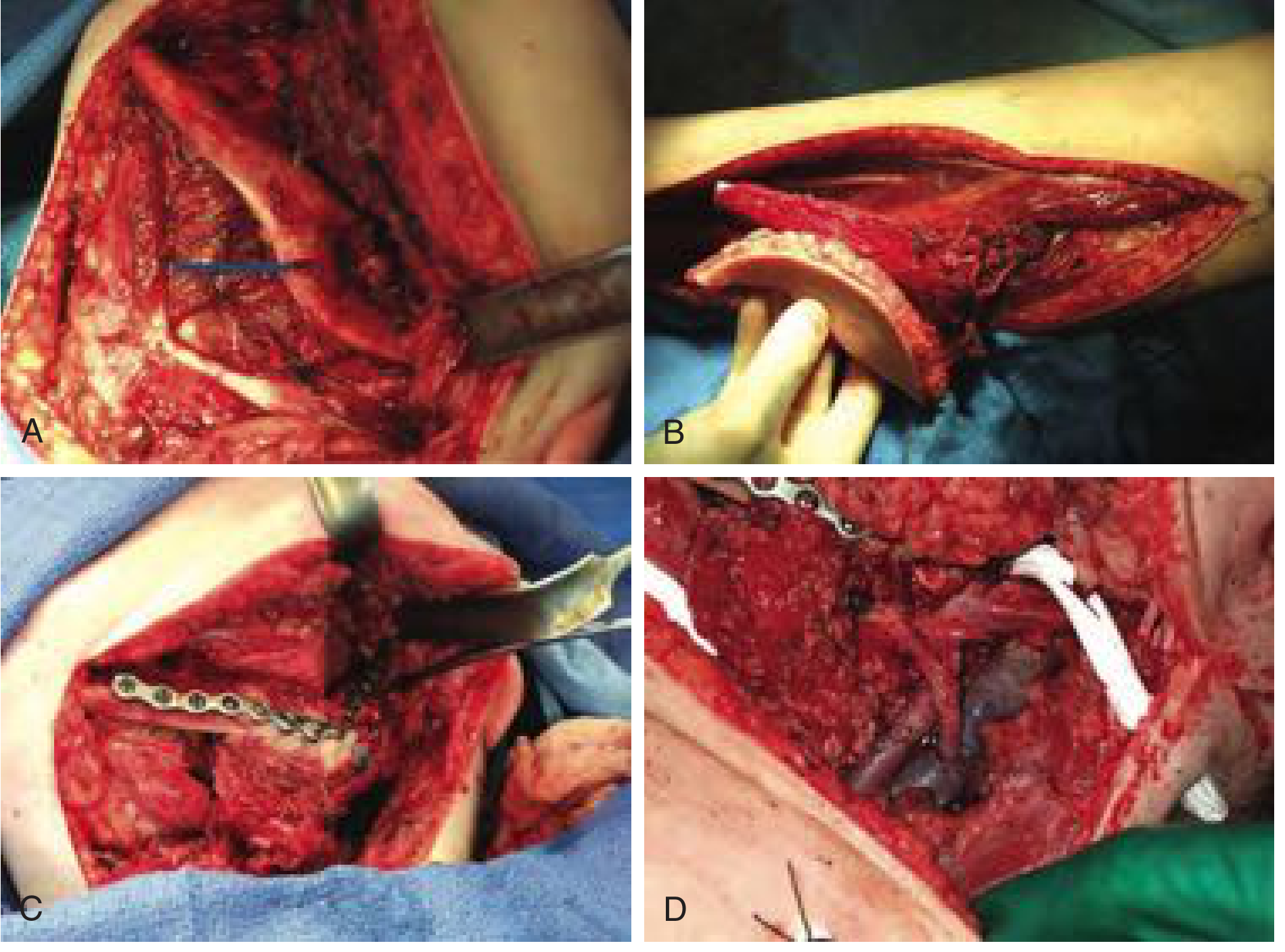
Anatomy:
- Vascular pedicle: peroneal artery and venae comitantes
- Bone: up to 25 cm of straight, cortical fibula - provides length for full hemi-mandible replacement
- Skin paddle: lateral leg skin - thin and pliable, supplied by musculocutaneous/septocutaneous perforators from the peroneal artery
How it reconstructs the three-layer defect:
- Bone (fibula): The fibula is osteotomized at multiple points to reproduce the curved shape of the mandible (body + angle + ramus), secured to a titanium reconstruction plate pre-bent to the patient's mandibular contour. It replaces the bone defect precisely.
- Intraoral lining (skin paddle 1): One skin paddle - folded inward - provides the intraoral mucosal lining (floor of mouth, gingival sulcus).
- External skin (skin paddle 2 or separate flap): With a double-island skin paddle or the use of a second flap, the external cheek skin defect is covered.
Pre-operative prerequisite:
- Confirm three-vessel run-off to the foot (CT angiography or Doppler) - peroneal artery sacrifice must not compromise foot perfusion.
- Confirm 5 cm of distal fibula preserved to protect the ankle joint.
Advantages of fibula flap:
- Longest available vascularized bone (up to 25 cm) - sufficient for full hemi-mandible
- Bicortical bone - strong enough to support osseointegrated dental implants
- Reliable skin paddle - allows single-flap reconstruction of bone + mucosa
- Reliable pedicle (peroneal artery, 3-4 mm caliber, pedicle length 6-10 cm)
- Allows simultaneous resection and reconstruction (two-team approach)
- Can be harvested in supine position alongside the head and neck procedure
- Long-term allows osseointegrated implants for dental rehabilitation
Limitations:
- Skin paddle can be unreliable for large three-layer defects - may need a second flap for external skin
- Perforator location in the lower leg is variable - unreliability minimized by including a soleus muscle cuff (musculocutaneous perforators)
- Results in a broad, rounded neomandible without dental implants (difficult to fit a prosthesis)
- Some donor site morbidity (prolonged pain on ambulation in some patients)
Step-by-Step Reconstructive Plan for Hemi-mandibulectomy
Step 1 - Virtual Surgical Planning (VSP)
- Pre-operative CT scanning of the head/neck and lower leg.
- Computer-assisted design of the osteotomy cuts, plate bending, and implant positions.
- Stereolithographic models and cutting guides manufactured for intra-operative use.
- This maximises accuracy of mandibular reconstruction and facilitates later dental rehabilitation.
Step 2 - Hemi-mandibulectomy (Ablative Phase)
- The condyle may or may not be preserved depending on oncological involvement.
- A reconstruction plate is pre-bent to the mandibular contour before resection (or custom CAD/CAM plate used).
- Ensure clear oncological margins throughout.
Step 3 - Fibula Harvest (Simultaneous two-team approach)
- Mark perforators with Doppler.
- Harvest fibula with overlying skin paddle(s) - single or double paddle depending on defect.
- Perform multiple osteotomies to match the reconstructed mandibular contour.
- Fix fibula segments to the reconstruction plate.
Step 4 - Microvascular Anastomosis
- Recipient vessels in the neck (from the neck dissection field): facial artery, superior thyroid artery, lingual artery (arterial); internal/external jugular vein or facial vein (venous).
- End-to-end or end-to-side anastomoses performed under microscope.
Step 5 - Soft Tissue Inset
- First skin paddle folded inward to reconstruct the intraoral lining (gingival sulcus + floor of mouth).
- Second skin paddle (or separate soft tissue flap) used to reconstruct the external cheek skin defect.
- If the fibula skin paddle is insufficient for both layers, a second free flap (e.g., radial forearm, ALT) or pedicled flap (e.g., pectoralis major) can cover the external defect.
Step 6 - TMJ Reconstruction (if condyle resected)
- Simplest: blunt end of fibula placed against condylar fossa - scars into place, provides adequate mouth opening.
- Alternatively: preserved condyle plated as free graft to fibula end; rib cartilage graft; or mechanical prosthetic TMJ replacement.
Alternative Options (When Fibula is Not Available)
| Situation | Alternative |
|---|---|
| Bilateral lower limb vascular disease | Iliac crest (DCIA) flap - robust bone; short pedicle, limited length, thick soft tissue |
| Short lateral/posterior defect (<5 cm), edentulous patient | Reconstruction plate + pedicled soft tissue flap (pectoralis major) |
| Thin bone needed, limited defect | Osteocutaneous radial forearm (OCRFFF) - limited bone (max 10-12 cm, 40% radius circumference) |
| Large defect + multiple soft tissue islands needed | Subscapular system (scapula + LD + parascapular) - composite, chimeric flap |
| Poor surgical risk, palliation | Reconstruction plate alone + soft tissue coverage (pectoralis major myocutaneous flap) |
| Non-vascularized bed (benign disease, no radiation) | Titanium mesh + bone graft + pectoralis major |
Pectoralis Major Myocutaneous Flap - Adjunct or Salvage
When free flap reconstruction is not feasible or fails, the pectoralis major myocutaneous flap (PMMC) provides:
- Reliable soft tissue bulk to cover a reconstruction plate
- Intraoral lining via skin paddle
- Coverage of exposed vessels in the neck
- Obliteration of dead space after neck dissection
It does not restore bone, so mandibular deviation and malocclusion persist with this option. Best for: lateral/posterior defects, edentulous patients, patients with poor surgical fitness, or salvage after failed free flap.
Dental Rehabilitation (Final Phase)
- After bone healing and completion of adjuvant radiotherapy, osseointegrated implants are placed into the fibula bone.
- Implant-supported prostheses restore masticatory function and complete the rehabilitative process.
- This is the ultimate goal of bony mandibular reconstruction and significantly improves quality of life.
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapters 78, 92
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 93
- Sabiston Textbook of Surgery, Chapter 69
Describe the management of 2 cm nodule in the prostate detected in a 60-year-old patient with PSA (Prostate Specific Antigen) of 24 ng/ml. [10]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material. Here is the complete, structured answer for this 10-mark question:
Management of a 2 cm Prostate Nodule with PSA of 24 ng/ml in a 60-year-old Man
Initial Assessment
This clinical scenario raises strong suspicion of prostate cancer:
- A palpable 2 cm nodule on DRE = cT2 disease at minimum (palpable, confined to one lobe) or cT3 (if extending beyond the capsule)
- PSA of 24 ng/ml is markedly elevated; the risk interpretation is:
- PSA 4-10 ng/ml: ~20-30% risk of cancer
- PSA 10-20 ng/ml: ~50% risk of cancer
- PSA >20 ng/ml: organ-confined disease in <50% of cases; 20% have pelvic lymph node involvement
- The combination of a palpable nodule + PSA 24 ng/ml = high probability of clinically significant prostate cancer, almost certainly at least intermediate risk and likely high risk
Step 1: History and Examination
History:
- Lower urinary tract symptoms (LUTS): hesitancy, frequency, urgency, poor stream, nocturia
- Haematuria, haematospermia
- Bone pain (pelvis, spine) - suggesting possible metastases
- Weight loss, constitutional symptoms
- Family history of prostate cancer, BRCA1/2 mutations (Lynch syndrome)
- Comorbidities, performance status, life expectancy
- Previous PSA trend (velocity) if available
Examination:
- Digital Rectal Examination (DRE): Characterise the nodule - size, consistency (hard, firm), fixation, extension to seminal vesicles, bilateral or unilateral involvement, fixation to pelvic sidewall
- General examination: lymphadenopathy, bone tenderness, hepatomegaly
Step 2: Investigations for Diagnosis and Staging
A. Tissue Diagnosis - Prostate Biopsy
Indication: Palpable nodule + elevated PSA = definitive indication for biopsy.
Pre-biopsy MRI (multiparametric MRI - mpMRI) - preferred:
- Performed before biopsy to characterize the lesion (PI-RADS score 1-5)
- Identifies the index lesion, extracapsular extension, seminal vesicle involvement
- Guides targeted (MRI-fusion) biopsy + systematic cores
Biopsy technique:
- Transrectal ultrasound (TRUS)-guided biopsy (traditional) OR
- MRI-targeted fusion biopsy (preferred when mpMRI available) - higher detection rate of clinically significant cancer
- Transperineal biopsy - lower infection risk, increasingly preferred
- Standard: 12-core systematic biopsy + targeted cores from the index lesion
- Biopsy provides: Gleason score / Grade Group, number of positive cores, percentage of cores involved, perineural invasion, extraprostatic extension
Gleason Grading / Grade Groups:
| Grade Group | Gleason Score | Prognosis |
|---|---|---|
| 1 | ≤6 | Favourable |
| 2 | 3+4=7 | Intermediate-favourable |
| 3 | 4+3=7 | Intermediate-unfavourable |
| 4 | 4+4=8 | High |
| 5 | 9-10 | Very high |
B. Staging Investigations
1. Bone scan (radionuclide scintigraphy):
- Indicated with PSA >20 ng/ml (clinical stage T1) - this patient qualifies
- Also indicated: Gleason 8-10, clinical T3/T4, bone symptoms
- Detects skeletal metastases (most common site of prostate cancer spread)
2. CT Scan - Pelvis and Abdomen:
- Recommended for high-risk patients (>10% nomogram probability of lymph node involvement)
- Evaluates pelvic lymph nodes, seminal vesicles, extracapsular extension
- PSA 24 ng/ml with palpable nodule = high risk → CT indicated
3. MRI of Pelvis (mpMRI):
- Most sensitive for local staging: extracapsular extension (ECE), seminal vesicle invasion (SVI), neurovascular bundle involvement
- T2-weighted + diffusion-weighted + dynamic contrast-enhanced sequences
- Preferred over TRUS alone for local staging
4. PSMA PET-CT (Prostate-Specific Membrane Antigen):
- Increasingly replacing conventional bone scan + CT
- High sensitivity and specificity for nodal and distant metastases
- Now considered first-line staging in high-risk prostate cancer in many guidelines
Step 3: Risk Stratification
Using PSA, DRE (clinical T stage), and Gleason score, this patient is classified using the D'Amico / NCCN risk stratification:
| Risk | PSA | T stage | Gleason |
|---|---|---|---|
| Low | <10 | T1-T2a | ≤6 |
| Intermediate | 10-20 | T2b-T2c | 7 |
| High | >20 | T3a | 8-10 |
| Very High | - | T3b-T4 | - |
This patient with PSA 24 ng/ml = HIGH RISK at minimum, regardless of Gleason score.
Nomograms (Partin tables, Memorial Sloan Kettering) can integrate PSA + clinical T stage + Gleason to predict pathologic stage and guide treatment intensity.
Step 4: Treatment - Management Options
Once biopsy confirms cancer and staging is complete, management is guided by:
- Risk group (high risk in this case)
- Extent of disease (organ-confined vs locally advanced vs metastatic)
- Patient age (60 years - good life expectancy, fit for radical treatment)
- Patient preference and comorbidities
A. Localised High-Risk Disease (No Metastases)
The AUA/ASTRO/NCCN guidelines recommend radical intent treatment for high-risk localised prostate cancer. Active surveillance is not appropriate for high-risk disease.
Option 1: Radical Prostatectomy (RP)
- Gold standard surgical treatment: Robotic-assisted laparoscopic radical prostatectomy (RALRP) or open retropubic radical prostatectomy
- Removes entire prostate, seminal vesicles, and pelvic lymph nodes (pelvic lymph node dissection - PLND is mandatory for high-risk disease)
- Nerve-sparing may not be possible if cancer is adjacent to neurovascular bundles
- Benefits: definitive pathological staging, single treatment, allows adjuvant radiotherapy if needed
- Complications: incontinence (urinary - early, usually resolves), erectile dysfunction, anastomotic stricture, haemorrhage
Option 2: External Beam Radiotherapy (EBRT) + Androgen Deprivation Therapy (ADT)
- EBRT using intensity-modulated radiotherapy (IMRT) / image-guided radiotherapy (IGRT)
- Long-term ADT (2-3 years) combined with EBRT is standard for high-risk disease - significantly improves survival (Level 1 evidence)
- Can be combined with brachytherapy boost (HDR or LDR)
- Benefits: avoids surgical morbidity, better short-term urinary/sexual function
- Risks: long-term progressive urinary and sexual dysfunction, rectal toxicity, secondary malignancy (bladder, rectum) at 15-20 years; ADT side effects (hot flushes, loss of libido, metabolic syndrome, osteoporosis)
Option 3: Surgery followed by Adjuvant Radiotherapy
- For post-operative adverse features: positive surgical margins, pT3 disease, PSA persistence
- Adjuvant EBRT reduces biochemical recurrence
B. Locally Advanced Disease (cT3/T4 - extracapsular extension on MRI)
- EBRT + long-term ADT (2-3 years) is the standard treatment
- Radical prostatectomy may still be performed by experienced surgeons in selected cT3 cases (extended nerve-sparing not performed; PLND essential)
C. Metastatic Disease (if bone scan / PSMA PET positive)
- Androgen Deprivation Therapy (ADT) is the backbone:
- Surgical castration (bilateral orchidectomy) - simple, permanent, inexpensive
- Medical castration: LHRH agonists (goserelin, leuprolide) or LHRH antagonists (degarelix, relugolix) - reversible
- Initial response in ~80%; castration-resistant prostate cancer (CRPC) develops in ~2-3 years
- Combination therapy (doublet/triplet) for metastatic hormone-sensitive prostate cancer (mHSPC):
- ADT + docetaxel (CHAARTED/STAMPEDE trials)
- ADT + abiraterone (LATITUDE trial)
- ADT + enzalutamide, apalutamide, or darolutamide (ARCHES, TITAN, ARASENS trials)
- Local therapy to the prostate (radical RT) in low metastatic burden improves survival (STAMPEDE trial)
- Bone-targeted agents: zoledronic acid (bone-related events prevention), radium-223 (symptomatic bone metastases)
Step 5: Follow-up After Treatment
After radical prostatectomy:
- PSA should fall to undetectable (<0.1 ng/ml) by 4-6 weeks post-op
- PSA checked every 3-6 months for 5 years, then annually
- Biochemical recurrence (BCR) = PSA ≥0.2 ng/ml on two consecutive readings → consider salvage radiotherapy ± ADT
After radiotherapy:
- PSA monitored every 3-6 months
- Nadir + 2 ng/ml = Phoenix definition of BCR after radiotherapy
- BCR after RT → salvage EBRT if prior RT, salvage prostatectomy, or ADT
Step 6: Supportive and Multidisciplinary Care
- Multidisciplinary team (MDT) input: urologist, radiation oncologist, medical oncologist, pathologist, radiologist
- Nutritional support and management of ADT side effects (bone mineral density, metabolic syndrome)
- Psychosocial support and quality of life assessment
- Bone protection: calcium + vitamin D, DEXA scan, bisphosphonates if on ADT >6 months
Summary Algorithm for This Patient
60-year-old man, 2 cm prostate nodule, PSA 24 ng/ml
↓
Detailed history + DRE (characterize nodule)
↓
mpMRI prostate (local staging) + PSMA PET-CT or Bone scan + CT abdomen/pelvis
↓
Transperineal MRI-targeted + systematic biopsy → Gleason / Grade group
↓
Risk stratification → HIGH RISK (PSA >20 ng/ml)
↓
┌───────────────────────────────────────┐
│ MDT Discussion │
└───────────────────────────────────────┘
↓
No metastases: Metastases:
Radical prostatectomy ADT + docetaxel/abiraterone/
+ PLND ± adj RT enzalutamide (doublet therapy)
OR ± local RT to prostate
EBRT + ADT (2-3 years)
↓
PSA monitoring + manage treatment side effects
Sources:
- Campbell-Walsh-Wein Urology, Chapters 152, 153
- AUA/ASTRO/SUO Guidelines: Clinically Localized Prostate Cancer
- NCCN Guidelines: Prostate Cancer
This is a shared conversation. Sign in to Orris to start your own chat.