ctec for tuberculosiar meningitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"tuberculous meningitis" treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
I now have all the information needed to compose a thorough CTEC answer. Let me compile it now.
Tuberculous Meningitis - CTEC
CTEC = Clinical features | Treatment | Etiology/Epidemiology | Complications
C - Clinical Features
Presentation
TB meningitis is classically subacute, evolving over 1-2 weeks (contrast with bacterial meningitis which is acute). The hallmark triad:
| Feature | Detail |
|---|---|
| Fever | Low-grade, persistent |
| Headache | >50% of cases; persistent and progressive |
| Neck stiffness | ~75% of cases; Kernig's and Brudzinski's signs |
Additional features:
- Lethargy, confusion, malaise (early)
- Cranial nerve palsies in ~20% - most commonly III, IV, VI (ocular palsies); less often VII (facial), VIII (deafness)
- Papilledema - due to raised ICP
- Seizures - especially in children; may be the presenting feature in infants
- Focal neurologic deficits - from vasculitis causing hemorrhagic infarction (Circle of Willis or primary branches)
- Hypothermia and hyponatremia - documented additional features
In young children/infants: apathy, hyperirritability, vomiting, seizures; stiff neck may be absent.
In HIV patients: course may be accelerated, with more frequent involvement of other organs.
CSF Findings
| Parameter | Finding |
|---|---|
| Appearance | Clear/xanthochromic |
| Pressure | Elevated |
| Cells | Lymphocytic pleocytosis (mononuclear) |
| Protein | Elevated |
| Glucose | Low (CSF:serum glucose ratio <0.5) |
| AFB smear | Sensitivity 10-50% (highly variable); large volumes + concentration techniques improve yield |
Diagnosis
- AFB smear: sensitivity 10-50%; multiple large-volume LPs improve yield
- Culture: gold standard but slow (weeks); rapid culture techniques available (< 1 week)
- PCR (NAAT): sensitivity ~80%, 10% false-positive rate; multiplex PCR is significantly more sensitive
- Adenosine deaminase (ADA): significantly elevated in TBM vs. other types
- Dot-ELISA (antigen/antibody in CSF): positive in ~86% of suspected TBM cases
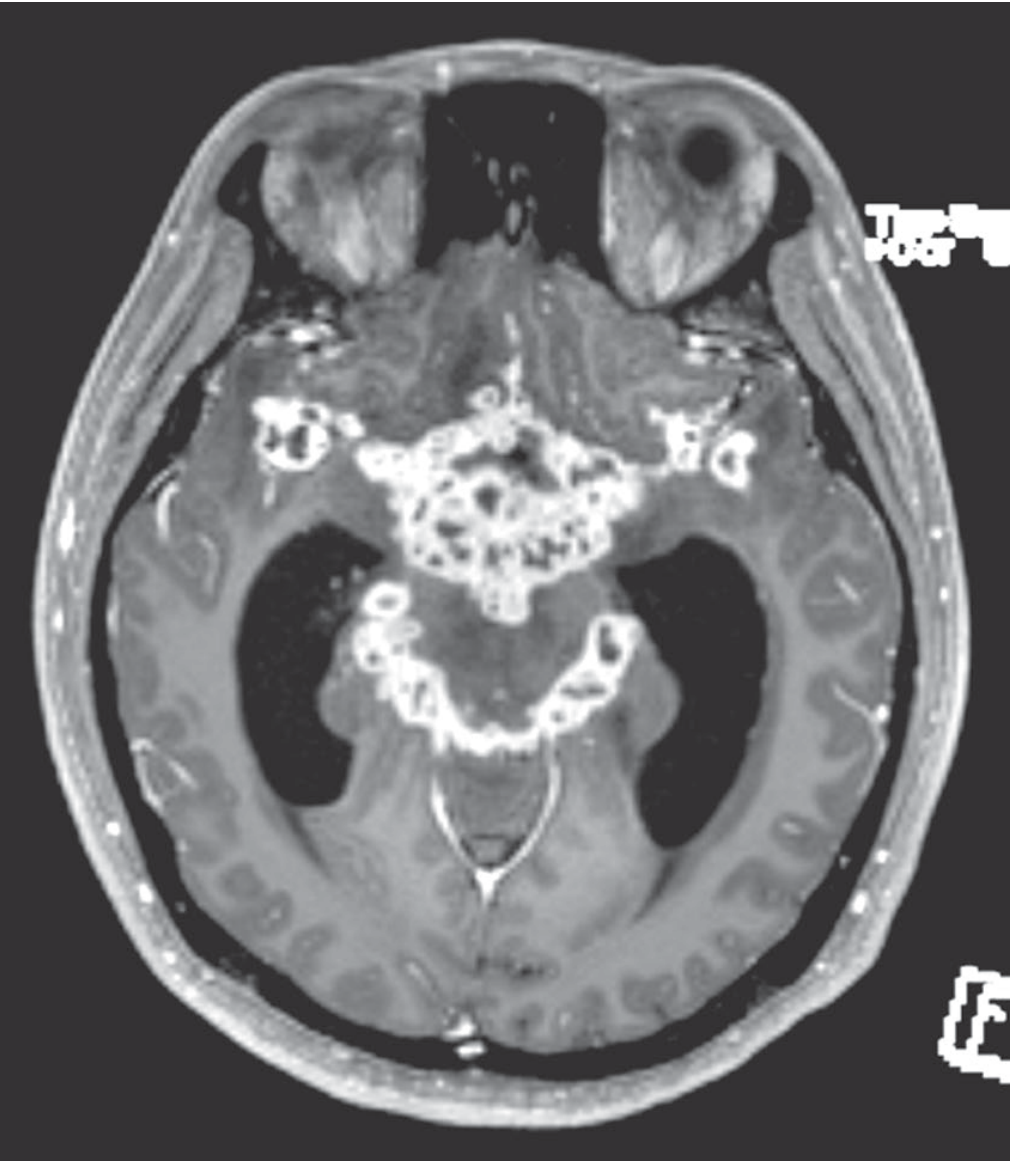
- Imaging (CT/MRI):
- Basal meningeal enhancement (gadolinium)
- Hydrocephalus
- Cerebral infarcts (deep, from Circle of Willis involvement)
- Tuberculomas (2-12 mm, ring-enhancing)
- CT may be normal in 30% of mild disease
CT normal in 30% of mild cases - do not rely on imaging to exclude TBM
T - Treatment
Antituberculosis Drugs (4-drug intensive phase)
The standard regimen is RIPE (4 drugs for the first 2 months, then INH + RMP for a prolonged continuation phase):
| Drug | Adult Dose | Key Toxicities |
|---|---|---|
| Isoniazid (INH) | 5 mg/kg/day (max 300 mg) | Peripheral neuropathy (mitigated by pyridoxine 50 mg/day), hepatitis |
| Rifampin (RMP) | 10 mg/kg/day adults; 15 mg/kg children (max 600 mg) | Hepatotoxicity, drug interactions, orange discoloration of secretions |
| Pyrazinamide (PZA) | 20-35 mg/kg once daily | Rash, GI disturbances, hepatitis |
| Ethambutol (EMB) | 15 mg/kg once daily | Optic neuropathy (check visual acuity and red-green color discrimination regularly) |
- Total duration: 9-12 months (if first-line drugs used; not all 4 drugs needed for the entire period)
- An alternative regimen: INH + PZA + high-dose RMP + moxifloxacin
Blood-brain barrier penetration ranking: INH > PZA > RMP > EMB
Drug-Resistant TBM
- In multi-drug resistance (MDR-TB), add ethionamide (ETA) as a 5th drug (15-25 mg/kg/day in divided doses; causes gastric irritation)
- High-dose rifampicin + levofloxacin in INH-resistant isolates
Adjunctive Corticosteroids (MANDATORY)
- Dexamethasone IV: 0.4 mg/kg/day for 1 week, then taper over 3-6 weeks
- Or initial dose: 0.15 mg/kg IV (Rosen's recommendation)
- Evidence: RCT in Vietnam showed IV dexamethasone reduced mortality from 41% to 32%
- Indicated for: raised ICP, subarachnoid block, severe disease
- Given only in conjunction with antituberculosis drugs - never alone
Empiric Treatment
- If TBM is clinically suspected and cryptococcal/other fungal infections + meningeal neoplasia are reasonably excluded - start treatment without waiting for culture results
Neurosurgical Intervention
- Ventriculoperitoneal shunting required in 25% of patients for hydrocephalus
- Consider in obstructive hydrocephalus or mass lesions
E - Etiology / Epidemiology
Etiology
- Primary organism: Mycobacterium tuberculosis (acid-fast bacillus)
- Rarely: M. bovis, M. avium, M. kansasii, M. fortuitum (post-neurosurgery or cranial trauma)
- HIV leads to increased cases from both typical AND atypical mycobacteria
Pathogenesis (Rich's concept)
Two-stage process:
- Hematogenous seeding of meninges/subpial brain regions → formation of tubercles (subependymal or meningeal)
- Rupture of one or more tubercles → discharge of bacteria into subarachnoid space → intense meningeal inflammation
Epidemiology
- More common in developing countries (sub-Saharan Africa: ~25x higher than the US)
- In the US: historically declining, but increased ~16%/year from ~1985 due to HIV epidemic
- With HIV under control, incidence trend reversed in many regions
- Risk populations: HIV/AIDS (incidence ~500x general population), alcoholics, immigrants from high-burden regions (Asia, Africa, India, former Soviet Union), malnourished, immunocompromised
- In 2/3 of patients: evidence of active TB elsewhere (usually lungs; also small bowel, bone, kidney, ear)
Pathology
- Brunt of disease at base of brain (basal meninges): thick gelatinous exudate in pontine and interpeduncular cisterns, optic chiasm, undersurfaces of temporal lobes
- Microscopically: central caseation + epithelioid/giant cells + lymphocytes + plasma cells
- Not confined to subarachnoid space - penetrates pia and ependyma → true meningoencephalitis
- Ependymia and choroid plexus studded with minute glistening tubercles
- Cranial nerves frequently involved (far more so than bacterial meningitis)
C - Complications
| Complication | Detail |
|---|---|
| Hydrocephalus | Obstructive (aqueduct/4th ventricle) or communicating (basal cistern blockage); 25% need VP shunting |
| Cerebral infarction | Vasculitis of Circle of Willis or primary branches → hemorrhagic infarction; deep infarcts |
| Cranial nerve palsies | CN III, IV, VI (ocular palsies most common), CN VII, CN VIII (deafness) |
| Seizures | Especially in children; recurrent seizures as residual |
| Arachnoid fibrosis | At brain base → impairs CSF resorption → chronic hydrocephalus |
| Residual neurological deficits | 20-30% of survivors: diminished intellect, psychiatric disturbances, visual/oculomotor disorders, deafness, hemiparesis |
| Tuberculoma | Space-occupying lesions; 5-30% of intracranial masses in developing countries |
| Spinal cord involvement | Myeloradiculitis; cord compression (Pott's disease - spinal TB/osteomyelitis) |
| Death | Overall mortality ~10%; ~50% if coma has supervened; ~21% in HIV-infected patients |
| SIADH/Hyponatremia | Documented additional feature |
Prognosis
- Overall mortality: ~10%
- Late diagnosis (coma): mortality approaches 50%
- HIV co-infection: mortality ~21% (delays in diagnosis + drug resistance)
- Residual deficits: 20-30% of survivors
- Early diagnosis and treatment = best outcome determinant
Recent Evidence Update
A 2026 Lancet Infectious Diseases practice guideline (PMID: 40840485) was published specifically for TB meningitis management - the most current guidance available. A 2024 systematic review in JAMA Network Open (PMID: 39093565) analyzed global bacterial meningitis case fatality over 80 years.
Sources: Adams & Victor's Principles of Neurology 12e | Rosen's Emergency Medicine | Tintinalli's Emergency Medicine | Henry's Clinical Diagnosis and Management by Laboratory Methods | Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.