Cyanosis
Cyanosis
Definition
- Harrison's Principles of Internal Medicine 22E, p. 321
Pathophysiology
- Severe anemia: Even with marked arterial desaturation, cyanosis may be absent because total hemoglobin is too low to accumulate 5 g/dL of deoxygenated form.
- Polycythemia vera: Cyanosis appears at higher SaO2 levels due to the excess total hemoglobin available to become deoxygenated.
- Methemoglobin / Sulfhemoglobin: Even small quantities of these dysfunctional hemoglobin derivatives can produce cyanosis. Methemoglobin has an intense dark blue-purple color visible through the skin.
-
Skin pigmentation and thickness (may not be apparent until SaO2 drops to 75% in dark-skinned individuals)
-
State of the cutaneous capillaries
-
Quality of lighting during examination
-
Oxyhemoglobin dissociation curve
-
Guyton and Hall Textbook of Medical Physiology, p. 548
-
Harrison's Principles of Internal Medicine 22E, p. 321
Classification
Central Cyanosis
- SaO2 is reduced OR an abnormal hemoglobin derivative is present
- Both skin and mucous membranes are affected
- Best observed at the tongue and buccal mucosa (most sensitive sites)
- Not relieved by warming or massaging the extremity
| Category | Examples |
|---|---|
| Decreased atmospheric O2 | High altitude (>4000 m / 13,000 ft) |
| Alveolar hypoventilation | Sedative overdose, neuromuscular disease, COPD |
| V/Q mismatch | Pneumonia, pulmonary edema, emphysema |
| Impaired O2 diffusion | Pulmonary fibrosis, interstitial lung disease |
| Anatomic right-to-left shunts | Congenital heart disease (Fallot's tetralogy, TGA, Eisenmenger syndrome), pulmonary AV fistulas |
| Hemoglobin abnormalities | Methemoglobinemia (hereditary or acquired), sulfhemoglobinemia, hemoglobin with low O2 affinity |
- Harrison's Principles of Internal Medicine 22E, p. 322 (Table 42-1)
- Tintinalli's Emergency Medicine, p. 470
Peripheral Cyanosis
- Arterial blood is normally saturated but O2 extraction is abnormally high due to slowed blood flow
- Affects skin of extremities (nail beds, fingers, toes); mucous membranes are typically spared
- Relieved by warming or massaging the area
| Category | Examples |
|---|---|
| Reduced cardiac output | Heart failure, cardiogenic shock |
| Cold exposure | Normal vasoconstriction |
| Arterial obstruction | Embolism, Raynaud's phenomenon |
| Venous obstruction | Deep vein thrombosis, thrombophlebitis |
| Maldistribution of flow | Distributive shock (sepsis) |
- Harrison's Principles of Internal Medicine 22E, p. 322
- Tintinalli's Emergency Medicine, p. 470
Key rule: All conditions causing central cyanosis also produce peripheral cyanosis. However, peripheral cyanosis can occur without central cyanosis.
Central vs. Peripheral Cyanosis - Quick Differentiation
| Feature | Central | Peripheral |
|---|---|---|
| Mucous membranes | Involved | Spared |
| Tongue | Blue | Pink |
| SaO2 | Reduced | Normal |
| Response to warming extremity | No change | Resolves |
| ABG | Low PaO2 / SaO2 | Normal PaO2 / SaO2 |
| Associated with clubbing | Yes (chronic) | No |
Special Situations
Mixed Cyanosis
Neonatal Cyanosis
-
Peripheral cyanosis (acrocyanosis) of hands/feet is normal in the first few days of life due to vasomotor instability - benign.
-
Central cyanosis in a neonate is always pathological.
- "Comfortably blue" (cyanosis without respiratory distress) - strongly suggests congenital heart disease.
- Cyanosis that worsens with crying - cardiac origin.
- Cyanosis that improves with crying - pulmonary origin.
- Cyanosis that responds to supplemental O2 - pulmonary cause.
- Cyanosis not responding to O2 - right-to-left cardiac shunt.
-
Rosen's Emergency Medicine, p. 3202
Pseudocyanosis
-
Drugs: chlorpromazine, minocycline, amiodarone
-
Metals: gold, silver
-
Features: mucous membranes are normal color, discoloration does not blanch with pressure, more intense in sun-exposed areas.
-
Tintinalli's Emergency Medicine, p. 471
Approach to the Patient with Cyanosis
- Time of onset: Cyanosis since birth/infancy - think congenital heart disease.
- Central vs. peripheral differentiation: Examine mucous membranes; warm/massage the extremity.
- Clubbing: Cyanosis + clubbing together = chronic central cause (congenital heart disease, pulmonary AV fistula, lung abscess). Peripheral cyanosis alone does NOT cause clubbing.
- PaO2 and SaO2: Measure arterial blood gas; if mechanism is unclear, send spectroscopy for abnormal hemoglobin species.
- Harrison's Principles of Internal Medicine 22E, p. 322
Investigations
| Test | Use |
|---|---|
| Pulse oximetry | First-line; detects hypoxemia. Unreliable in hemoglobinopathies (reads 80-85% in methemoglobinemia regardless of true saturation; reads falsely high in CO poisoning) |
| ABG with co-oximetry | Gold standard - multiwavelength measurement; correctly identifies methemoglobin, carboxyhemoglobin, and true SaO2 |
| Spectroscopy of blood | Identifies methemoglobin and sulfhemoglobin when cause is unclear |
| CXR | Pulmonary vs. cardiac cause |
| ECG | Congenital/structural cardiac disease |
| Echocardiography | Right-to-left shunts, structural defects |
| FBC | Polycythemia, anemia context |
- Tintinalli's Emergency Medicine, p. 471
Management Principle
-
Administer supplemental oxygen to all patients with central cyanosis.
-
Failure to improve with O2 suggests: impaired circulation (shock), abnormal hemoglobin (methemoglobinemia - treat with IV methylene blue), or pseudocyanosis.
-
Treat the underlying cause.
-
Tintinalli's Emergency Medicine, p. 471
Vital capacity
Vital Capacity
Definition
- Fishman's Pulmonary Diseases and Disorders, p. 576
Lung Volumes and Capacities - The Framework
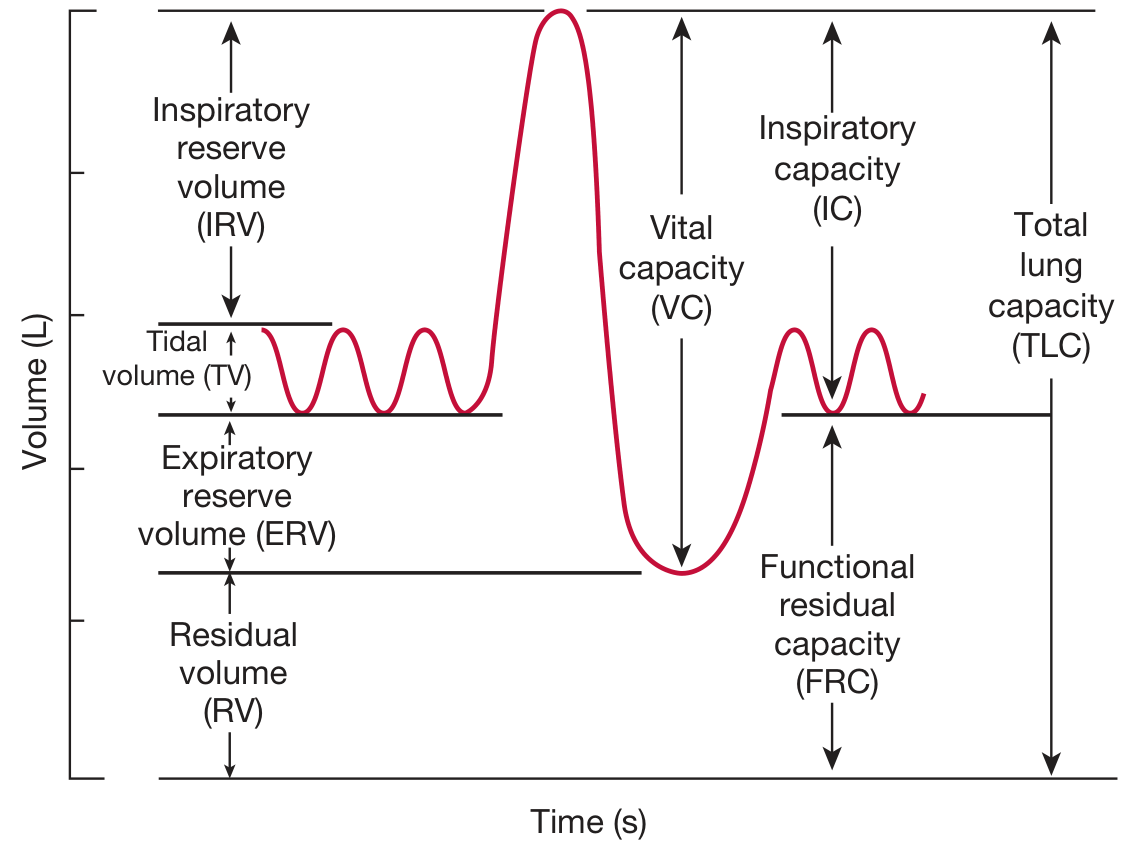
The Four Basic Lung Volumes (do not overlap)
| Volume | Symbol | Definition | Normal Value |
|---|---|---|---|
| Tidal Volume | TV (VT) | Air moved in/out during quiet breathing | ~500 mL |
| Inspiratory Reserve Volume | IRV | Extra air inspired above TV with maximal effort | ~3000 mL |
| Expiratory Reserve Volume | ERV | Extra air expired below TV with maximal effort | ~1200 mL |
| Residual Volume | RV | Air remaining after maximal expiration; cannot be measured by spirometry | ~1200 mL |
The Four Capacities (each = sum of 2 or more volumes)
| Capacity | Symbol | Components | Normal Value |
|---|---|---|---|
| Inspiratory Capacity | IC | TV + IRV | ~3500 mL |
| Vital Capacity | VC | IRV + TV + ERV (= IC + ERV) | ~4700 mL |
| Functional Residual Capacity | FRC | ERV + RV | ~2400 mL |
| Total Lung Capacity | TLC | VC + RV (all four volumes) | ~5900 mL |
- Costanzo Physiology 7th Edition, p. 200
Vital Capacity in Detail
- Larger body size / height
- Male sex
- Physical conditioning / athletic training
-
Increasing age
-
Female sex (relative to males)
-
Obesity
-
Restrictive lung diseases
-
Extrapulmonary restriction (see below)
-
Barash Clinical Anesthesia 9e, p. 1133
-
Costanzo Physiology 7th Edition, p. 201
Forced Vital Capacity (FVC)
- Fishman's Pulmonary Diseases and Disorders, p. 585
FVC Maneuver
- Patient inspires maximally to TLC
- Forceful, rapid, complete expiration into a spirometer (to RV)
- Normally completed within 6 seconds (in obstruction, may continue 10-12 s)
FEV1 and the FEV1/FVC Ratio - Clinical Core
| Parameter | Definition | Normal Value |
|---|---|---|
| FEV1 | Volume forcibly expired in the first second | ~80% of FVC |
| FEV1/FVC | Fraction of FVC expired in 1 second | ~0.80 (80%) |
| FEF25-75% | Mean flow over the middle 50% of FVC | Sensitive for small airway disease |
FVC and FEV1 in Disease
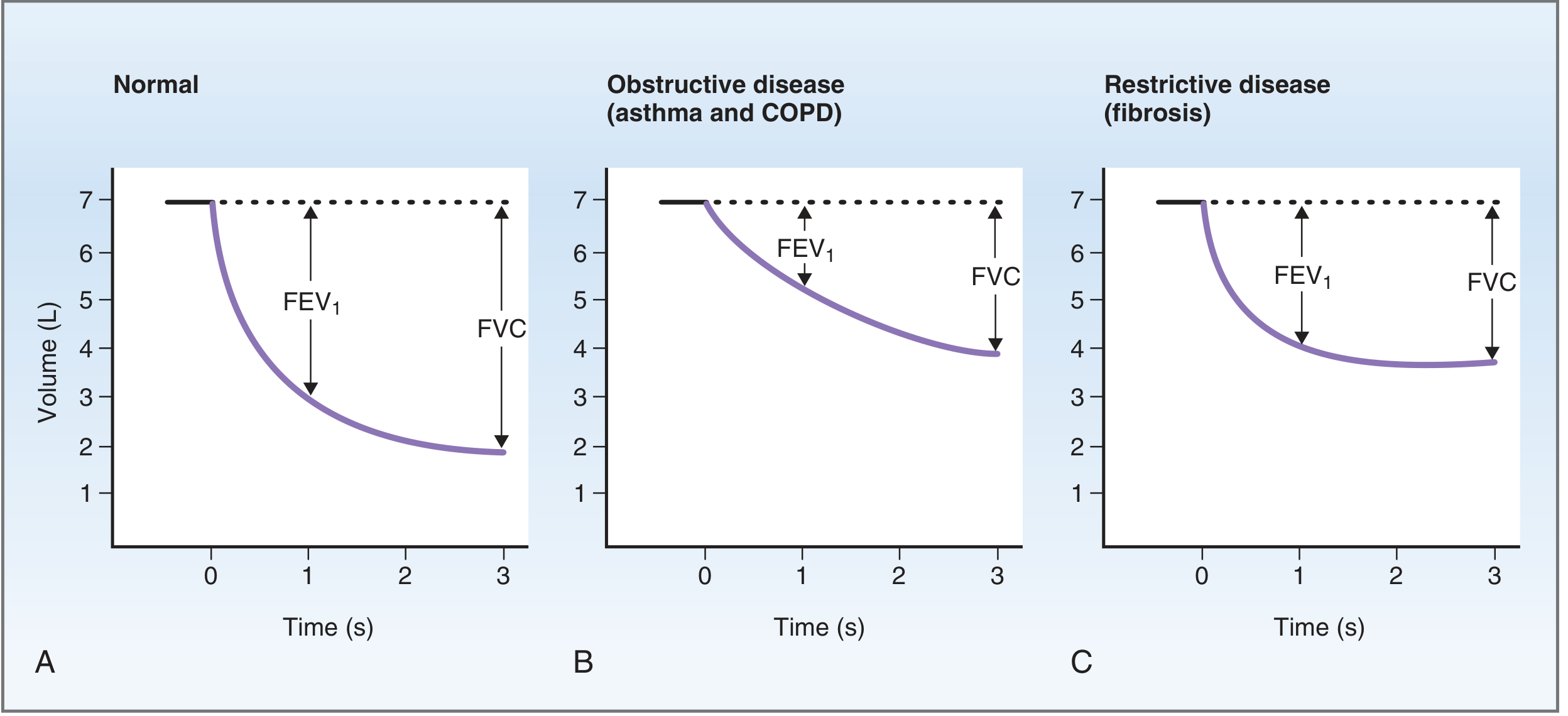
| Pattern | FVC | FEV1 | FEV1/FVC | Examples |
|---|---|---|---|---|
| Normal | Normal | Normal | ~0.80 | - |
| Obstructive | Decreased | Decreased more | < 0.70 (decreased) | Asthma, COPD, emphysema |
| Restrictive | Decreased | Decreased less | > 0.80 (normal or increased) | Pulmonary fibrosis, pleural effusion |
-
In severe asthma, FEV1/FVC can fall below 20%.
-
In obstruction, the FVC curve is prolonged and flattened; in restriction, it is steep but low in volume.
-
Costanzo Physiology 7th Edition, p. 203
-
Guyton and Hall Textbook of Medical Physiology, p. 534
Clinical Significance of Vital Capacity
- Deep breathing ability
- Effective coughing (critical for airway clearance)
- Ability to sustain ventilation (relevant in neuromuscular disease)
Causes of Reduced Vital Capacity
- Pulmonary edema, atelectasis
- Pulmonary fibrosis / interstitial lung disease
- Pneumonia
- Emphysema (gas trapping reduces ERV)
- Pleural effusion
- Pneumothorax
- Pregnancy / large ascites
- Obesity (diaphragm elevation)
- Respiratory muscle weakness (e.g., Guillain-Barre, myasthenia gravis, muscular dystrophy)
- Quadriplegia / spinal cord injury
Critical threshold: FVC < 15 mL/kg is associated with increased risk of postoperative pulmonary complications and may indicate need for ventilatory support. This level is most often seen in quadriplegia or severe neuromuscular disease.
- Barash Clinical Anesthesia 9e, p. 1133-1134
Bedside Estimation
Summary
| Feature | Value |
|---|---|
| VC formula | IRV + TV + ERV (or TLC - RV) |
| Normal VC | ~4.6-4.8 L (~60 mL/kg in adults) |
| FEV1/FVC normal | ~0.80 (80%) |
| Obstructive pattern | FVC ↓, FEV1 ↓↓, FEV1/FVC ↓ |
| Restrictive pattern | FVC ↓, FEV1 ↓, FEV1/FVC normal/↑ |
| Measured by | Spirometry |
| RV not measured by spirometry | FRC and TLC also require plethysmography or helium dilution |
Atrial septal defect
Atrial Septal Defect (ASD)
Definition
- Sabiston Textbook of Surgery 21e, p. 2563
Embryological Basis
- Septum primum grows down, partially closing the ostium primum
- Before complete closure, ostium secundum opens posteriorly in septum primum
- Septum secundum grows to cover ostium secundum, leaving the foramen ovale (a right-to-left channel in fetal life due to high pulmonary pressures)
- At birth: lung expansion drops pulmonary pressure → left atrial pressure exceeds right → foramen ovale closes
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 503
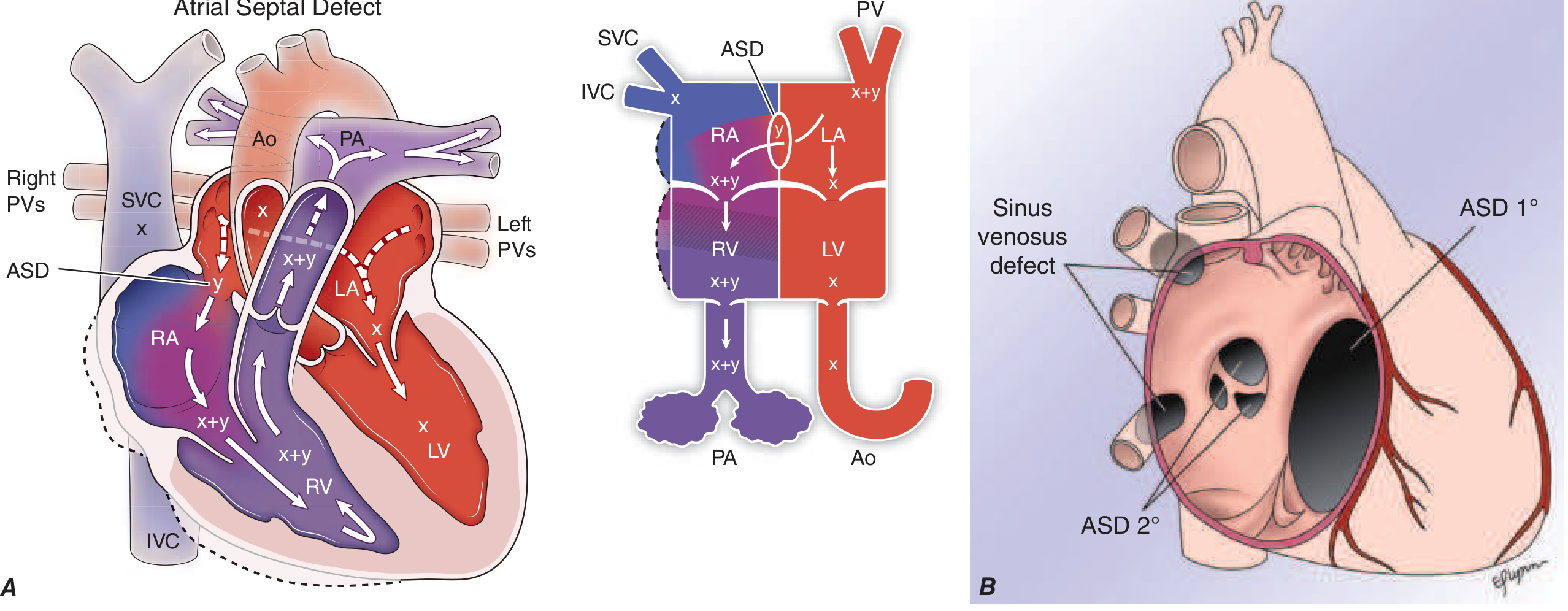
Classification / Types
| Type | Frequency | Location | Associated Anomalies |
|---|---|---|---|
| Secundum ASD | ~90% | Fossa ovalis region (center of atrial septum); deficient septum secundum | Usually isolated; can be multiple/fenestrated |
| Primum ASD | ~5% | Adjacent to AV valves (AV canal defect) | Always associated with AV valve abnormalities (cleft mitral valve); often + VSD |
| Sinus venosus defect | ~5% | Near SVC-atrial junction (superior) or IVC-atrial junction (inferior) | Associated with anomalous pulmonary venous return (right upper PV to SVC) |
| Coronary sinus defect | Rare | Opening between coronary sinus and LA | - |
Important distinction: A patent foramen ovale (PFO) is NOT a true ASD - it is persistence of the flap valve of the fossa ovalis without a true septal deficiency. PFO persists in up to 20-25% of adults and does not cause right heart dilation. It has no resting shunt and is not detectable clinically, but can allow paradoxical embolism if right atrial pressures transiently rise.
- Harrison's Principles of Internal Medicine 22E, p. 2114
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 504
Pathophysiology
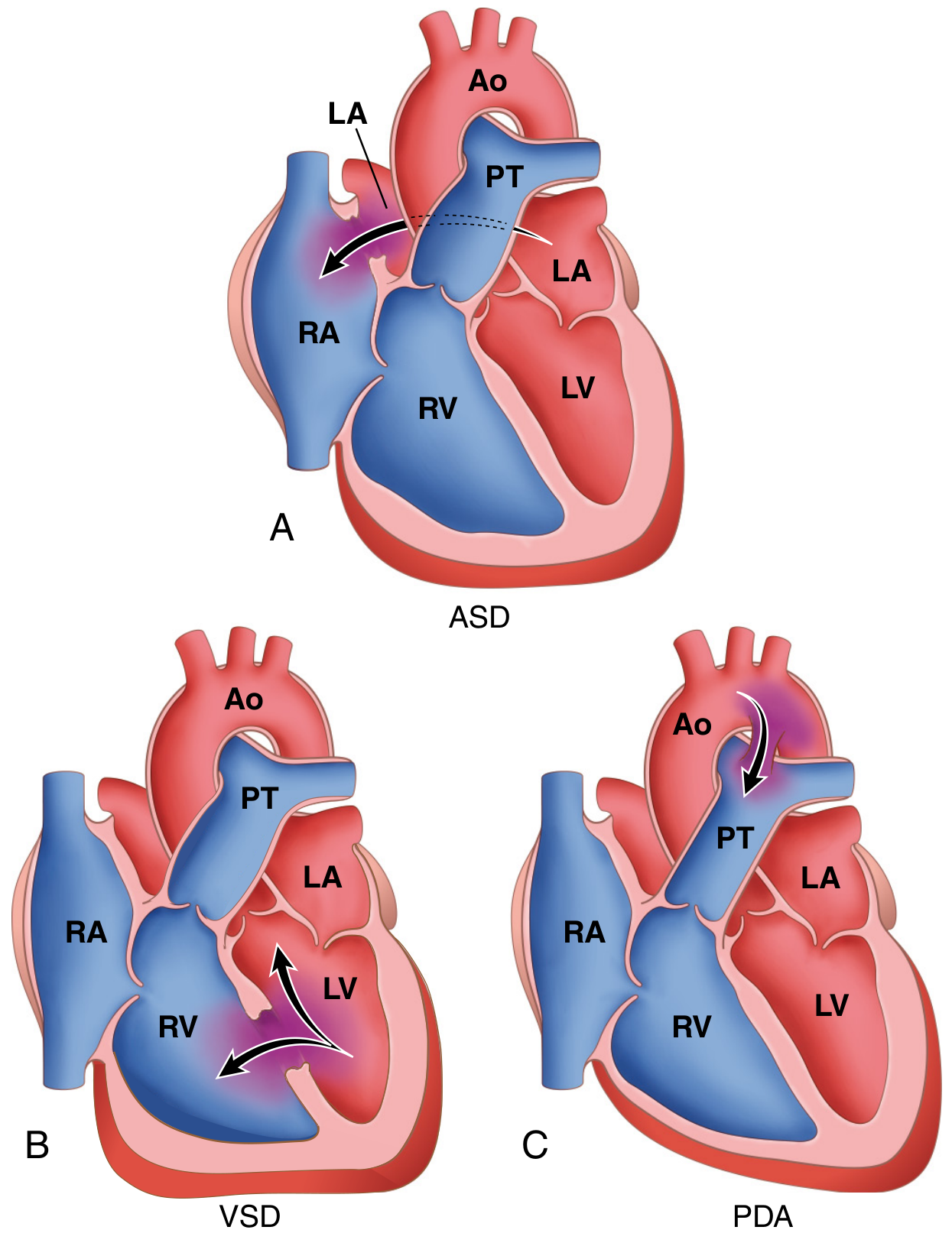
Left-to-Right Shunt
- Pulmonary vascular resistance < systemic vascular resistance
- Right ventricular compliance is greater than left ventricular compliance
Consequences of Chronic L→R Shunting
- Right heart volume overload - RA and RV dilate
- Increased pulmonary blood flow - pulmonary artery dilation
- Atrial arrhythmias (AF, flutter) from RA enlargement
- Pulmonary arterial hypertension - in ~10% of unrepaired ASDs
- Eisenmenger syndrome - rare; when pulmonary hypertension causes shunt reversal to R→L, producing cyanosis
Significant Shunt Threshold
- Harrison's Principles of Internal Medicine 22E, p. 2113
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 504
Clinical Features
Symptoms
- Childhood: Often asymptomatic; occasional exercise intolerance or frequent respiratory infections
- Adults: Dyspnea on exertion, exercise intolerance, fatigue, palpitations
- Late/advanced: Right heart failure, atrial fibrillation, syncope, stroke (from paradoxical embolism)
- Aging factors: DM, hypertension, and atherosclerosis reduce LV compliance, worsening L→R shunt with age
Physical Examination
| Finding | Mechanism |
|---|---|
| Wide, fixed splitting of S2 | Hallmark sign. Increased venous return equalizes phasic changes; RV overload + increased PA capacitance delays P2 regardless of respiratory cycle |
| Soft midsystolic ejection murmur (2nd LICS) | Increased flow across pulmonary valve (pulmonary flow murmur), NOT flow through the ASD itself |
| Mid-diastolic murmur (lower LSB) | Increased flow across tricuspid valve (only with large shunts) |
| Right ventricular heave | Left parasternal area - due to RV volume overload |
| Palpable pulmonary artery | 2nd LICS pulsation with large shunts |
| Elevated JVP, peripheral edema | Late, with right heart failure |
- Goldman-Cecil Medicine, p. 985
- Harrison's Principles of Internal Medicine 22E, p. 2113
Investigations
ECG
- Incomplete right bundle branch block (rSr' pattern in V1/V2) - characteristic finding, from RV volume overload
- Right axis deviation
- Right atrial enlargement (tall P waves)
- Prolonged PR interval (especially primum ASD)
- Atrial fibrillation or flutter (in older/advanced cases)
Chest X-Ray
- Pulmonary vascular plethora (increased pulmonary vascular markings bilaterally)
- Dilated main pulmonary artery and branches
- Right atrial and right ventricular enlargement
- Small aortic knuckle (reduced systemic output)
Echocardiography (Diagnostic Gold Standard)
- Transthoracic echo (TTE): Identifies secundum and primum ASDs; RV dilation; estimates PA pressures by Doppler
- Transesophageal echo (TEE): Required for sinus venosus defects and device sizing; agitated saline contrast (bubble study) demonstrates shunt
- Provides shunt ratio estimation (Qp/Qs)
Cardiac Catheterization
-
"Step-up" in oxygen saturation at the right atrial level (confirms L→R shunt)
-
Precise Qp/Qs measurement and pulmonary vascular resistance
-
Indicated when PA hypertension is suspected or non-invasive data are inconclusive
-
Goldman-Cecil Medicine, p. 986
Management
Indications for Closure
- Right heart dilation (with or without symptoms) - primary indication
- Qp/Qs ≥ 1.5 with attributable symptoms or signs
- In patients >40 years old: closure improves functional status and survival even with symptoms and large shunts
- Paradoxical embolism risk (prior stroke with PFO/ASD)
Contraindication
- Severe, irreversible pulmonary hypertension (Eisenmenger syndrome) - closure is harmful as it removes the "pop-off" valve
1. Transcatheter (Percutaneous) Device Closure
- Now preferred for secundum ASDs - currently accounts for >60% of all ASD interventions
- Suitable for centrally located defects up to ~3.5 cm with adequate tissue rims
- Amplatzer septal occluder (nitinol mesh) most widely used; placed under fluoroscopic + echocardiographic guidance
- Avoids sternotomy and cardiopulmonary bypass
- Limitations: Large defects, inadequate rims, anomalous pulmonary veins, or associated cardiac lesions requiring repair
- Complications: Device erosion through atrial wall/ascending aorta (rare but serious), conduction disturbances, endocarditis
2. Surgical Closure
- Required for: primum ASDs, sinus venosus defects, coronary sinus defects, large secundum ASDs unsuitable for devices, or when concomitant repairs needed
- Methods: direct suture closure, autologous pericardium patch, or prosthetic patch on cardiopulmonary bypass
- Very low mortality; postoperative survival comparable to general population
- Minimally invasive surgical approaches increasingly used
Timing
-
Most centres recommend closure before school age for significant defects
-
Earlier closure prevents pulmonary vascular disease; however, small ASDs may close spontaneously (less common than in VSD)
-
Sabiston Textbook of Surgery 21e, p. 2563-2564
-
Harrison's Principles of Internal Medicine 22E, p. 2114
-
Goldman-Cecil Medicine, p. 986
Prognosis
- Small ASDs with minimal shunting: excellent prognosis, may not require intervention
- Surgically/percutaneously closed before pulmonary hypertension develops: life expectancy approaches that of the general population
- Unrepaired large ASDs: progressive right heart failure, atrial arrhythmias, pulmonary hypertension
- Eisenmenger syndrome (R→L shunt reversal): median survival ~40-45 years; managed medically with pulmonary vasodilators
ASD vs. PFO - Key Comparison
| Feature | ASD | PFO |
|---|---|---|
| True septal defect | Yes | No (flap valve incompetence) |
| Resting shunt | Yes | No (only with ↑ RA pressure) |
| Right heart dilation | Yes | No |
| Murmur / fixed S2 split | Yes | No |
| Prevalence | ~1/700 births | ~25% of adults |
| Main complication | RHF, PAH | Paradoxical embolism / cryptogenic stroke |
- Harrison's Principles of Internal Medicine 22E, p. 2114
Components of tetralogy of fallot
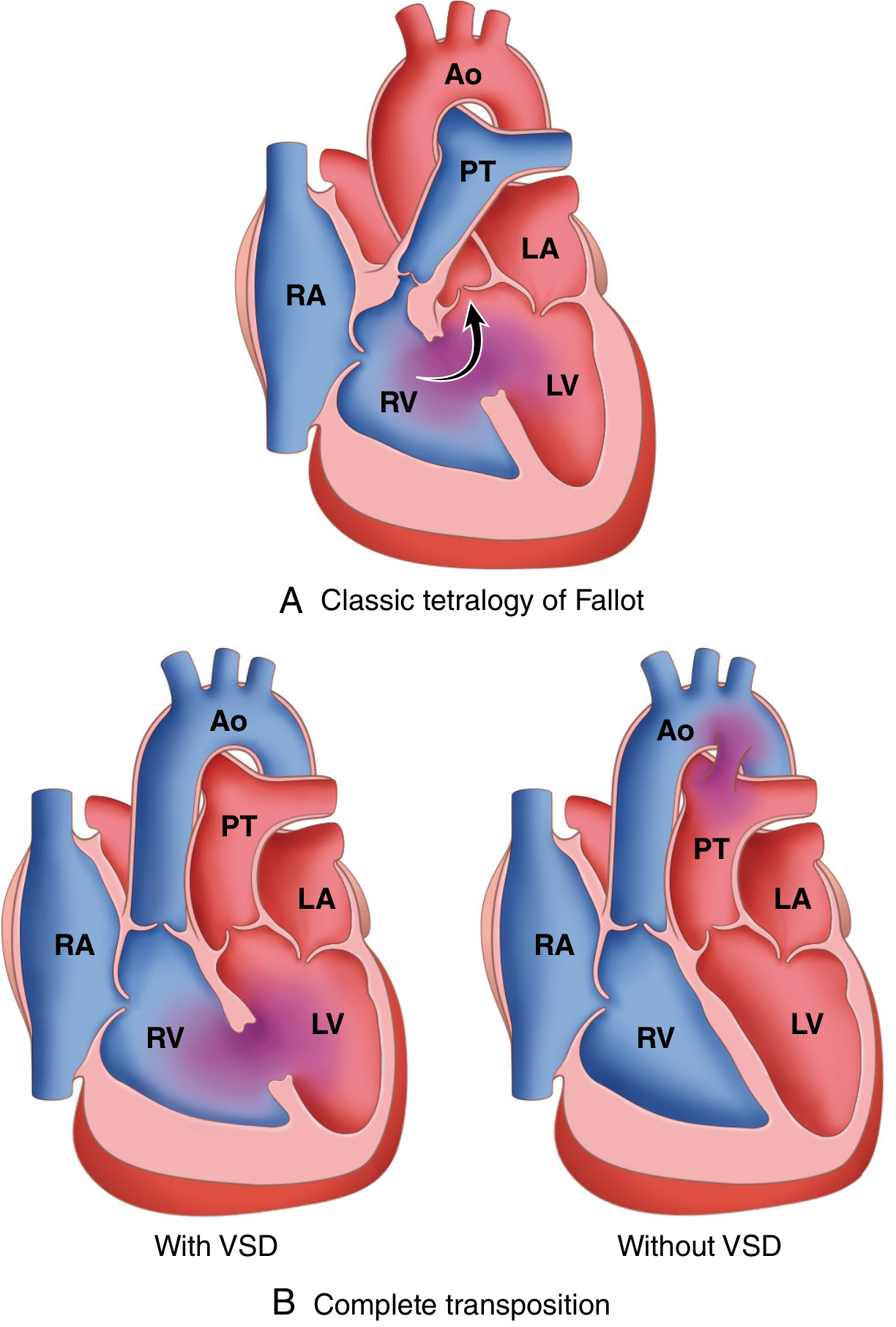
Tetralogy of Fallot (TOF)
Overview
The Four Components
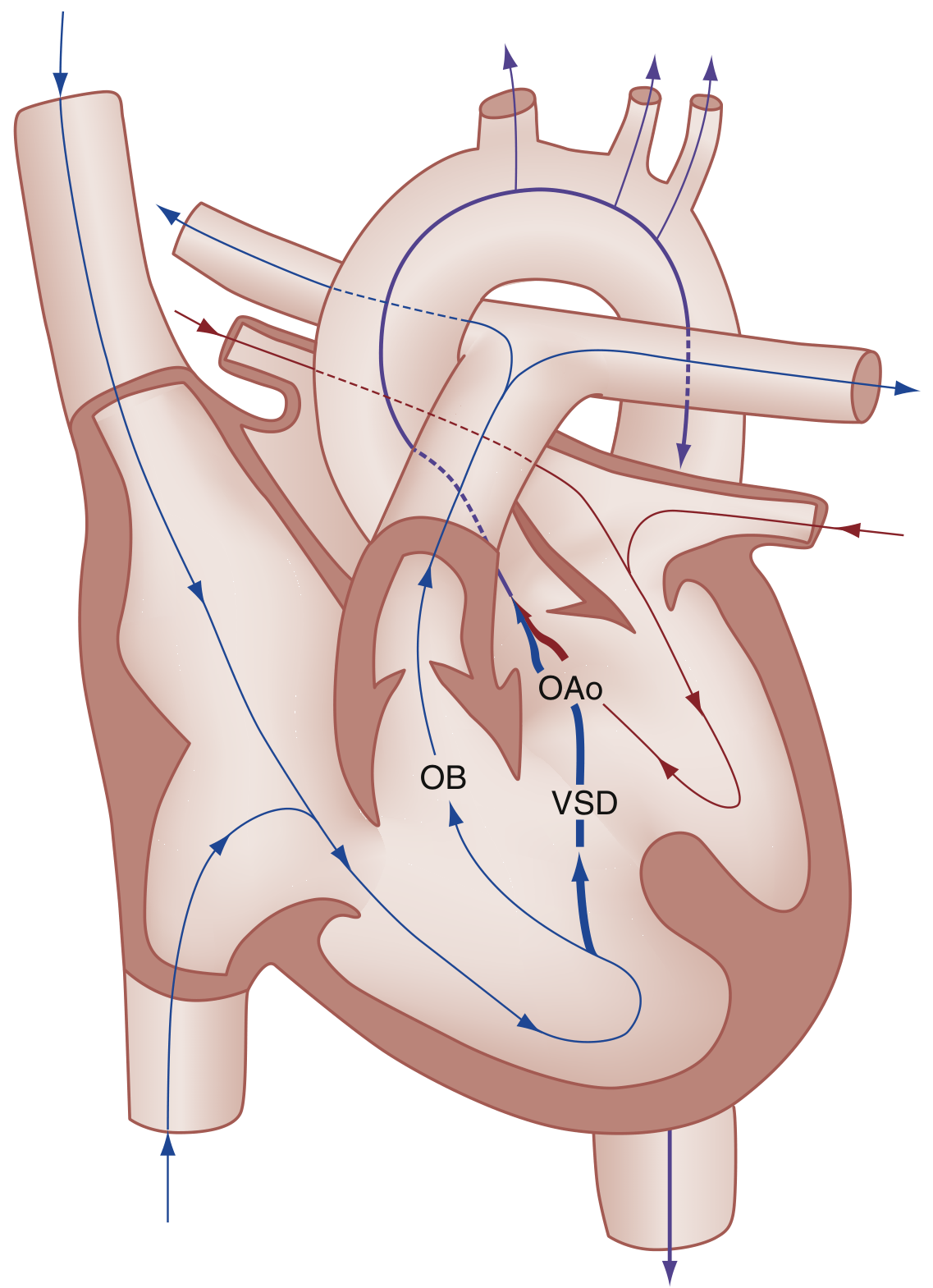
1. Ventricular Septal Defect (VSD)
- A large, unrestrictive, misaligned VSD - the aortic valve sits at its superior border
- Located in the perimembranous/subaortic region
- Results directly from the malaligned infundibular septum failing to close the interventricular communication
- The VSD is typically large enough that pressures in both ventricles are equal ("non-restrictive")
- Acts as the conduit for the right-to-left shunt
2. Right Ventricular Outflow Tract (RVOT) Obstruction - Pulmonary Stenosis
- Most often due to subpulmonic (infundibular/subvalvular) stenosis - narrowing of the muscular outflow tract below the pulmonary valve
- May also involve the pulmonary valve itself (valvular stenosis) in addition
- In the most severe form: pulmonary atresia - no forward flow to pulmonary arteries; survival depends on a PDA or bronchial collateral vessels
- The degree of RVOT obstruction is the single most important determinant of the severity of cyanosis and clinical presentation
- The pulmonary trunk is typically small/hypoplastic
3. Overriding Aorta (Dextroposition of the Aorta)
- The aorta is displaced anteriorly and to the right, so it straddles the VSD, receiving blood from both the right and left ventricles
- In a normal heart, the aorta arises entirely from the LV; in TOF, it "overrides" the ventricular septum
- The degree of override is variable - from mild to >50%
- Directly caused by the anterior malalignment of the infundibular septum
- Results in mixing of oxygenated and deoxygenated blood in the systemic circulation
4. Right Ventricular Hypertrophy (RVH)
-
Secondary to the other three defects - not a primary developmental anomaly
-
RVH develops because the RVOT obstruction causes chronic pressure overload on the right ventricle
-
The VSD equalizes pressures between ventricles, so RV systolic pressure = LV systolic pressure = systemic pressure
-
Macroscopically: the heart is enlarged and classically boot-shaped (coeur en sabot) due to prominent RVH lifting the cardiac apex, with a concave pulmonary artery segment
-
Importantly, RVH protects the pulmonary vasculature from pressure overload (the stenosis acts as a barrier) - so unlike Eisenmenger's, pulmonary vascular disease is not a feature of TOF
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 505-506
-
Rosen's Emergency Medicine, p. 3210
Embryological Basis
- Anterior shift → narrows the RVOT (causing stenosis)
- Anterior shift → displaces the aorta rightward (causing override)
- Anterior shift → VSD forms because the septum no longer aligns with the membranous septum
- RVH → develops secondarily from the pressure load
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 505
- The Developing Human - Clinically Oriented Embryology, p. 847
Summary Table: The Four Components
| Component | Nature | Mechanism | Clinical Impact |
|---|---|---|---|
| VSD | Large, perimembranous, subaortic | Primary - infundibular malalignment | Conduit for R→L shunt; equalizes ventricular pressures |
| RVOT obstruction | Subpulmonic/infundibular stenosis ± valvular PS ± pulmonary atresia | Primary - infundibular malalignment | Drives R→L shunt; severity determines degree of cyanosis |
| Overriding aorta | Aorta straddles VSD, receives blood from both ventricles | Primary - infundibular malalignment | Mixed blood enters systemic circulation |
| RVH | Concentric hypertrophy of RV walls | Secondary - pressure overload from RVOT obstruction | Boot-shaped heart on CXR; protects pulmonary vasculature |
Pathophysiology of Cyanosis
- Degree of RVOT obstruction (increases R→L shunting)
- Systemic vascular resistance (SVR) (fall in SVR worsens R→L shunting)
"Pink Tet" vs Classic TOF
| Feature | Pink Tet (Acyanotic TOF) | Classic (Cyanotic) TOF |
|---|---|---|
| RVOT obstruction | Mild | Moderate-severe |
| Shunt direction | Left-to-right (like isolated VSD) | Right-to-left |
| Cyanosis at birth | Absent | Present or develops early |
| Clinical course | May develop cyanosis later as RV grows | Cyanotic from birth or infancy |
Associated Anomalies
- Right-sided aortic arch - present in ~25% (an important associated finding)
- Atrial septal defect (ASD) - creating a "pentalogy of Fallot" if both present
- Anomalous origin of the left coronary artery (from RCA crossing RVOT - surgically important)
- Partial anomalous pulmonary venous return
Tet Spells (Hypercyanotic/Hypoxic Spells)
- Knee-to-chest position (increases SVR - most important first step)
- Supplemental oxygen
- Morphine 0.1-0.2 mg/kg IV/IM (reduces infundibular spasm and hyperpnea)
- Sodium bicarbonate (1 mEq/kg IV) for metabolic acidosis
- Ketamine (maintains/increases SVR)
- Propranolol 0.1-0.2 mg/kg (reduces infundibular spasm)
- Phenylephrine 0.01-0.02 mg/kg IV (pure vasoconstrictor, increases SVR)
- Rosen's Emergency Medicine, p. 3211
Investigations
| Test | Findings in TOF |
|---|---|
| CXR | Boot-shaped heart ("coeur en sabot") - RVH + concave pulmonary segment; decreased pulmonary vascular markings; right aortic arch in 25% |
| ECG | Right ventricular hypertrophy, right axis deviation |
| Echocardiography | Diagnostic - defines all 4 components, RVOT severity, coronary anatomy |
| Cardiac MRI | Gold standard for post-repair follow-up; quantifies pulmonary regurgitation and RV volumes |
| Cardiac catheterization | Pre-op when PA anatomy uncertain or coronary anomaly suspected |
Management
- Definitive treatment: Complete surgical repair - VSD patch closure + RVOT reconstruction (transannular patch to enlarge outflow tract), typically in early infancy
- Staged palliation: For severe cyanosis with very narrow RVOT or hypoplastic pulmonary arteries - modified Blalock-Taussig (BT) shunt (subclavian artery to pulmonary artery) as a bridge to full repair
- PGE1 infusion: For neonates with severe RVOT obstruction or pulmonary atresia - maintains ductal patency to preserve pulmonary blood flow
-
Pulmonary regurgitation (most common) → progressive RV dilation → may require pulmonary valve replacement
-
Residual RVOT obstruction or VSD
-
Ventricular arrhythmias and sudden cardiac death (due to RV dilation/fibrosis)
-
Aortic root dilation
-
Grainger & Allison's Diagnostic Radiology, p. 303
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 506
Darw a normal ecg and lable
A detailed, clean medical diagram of a single normal ECG (electrocardiogram) complex on graph paper background. Show one complete cardiac cycle with clear labels pointing to each component: P wave (atrial depolarization), PR interval, PR segment, QRS complex with individual Q wave, R wave, and S wave labeled, ST segment, T wave (ventricular repolarization), U wave (small, after T wave), QT interval, and RR interval. Include normal time and voltage measurements on the axes (horizontal: 0.04 sec per small square, 0.2 sec per large square; vertical: 0.1 mV per small square, 0.5 mV per large square). The baseline (isoelectric line) should be clearly shown. Use a clean white/light background with a standard red/pink ECG grid. All labels should be in clear black text with arrows pointing to the correct part of the waveform. Medical textbook style illustration.
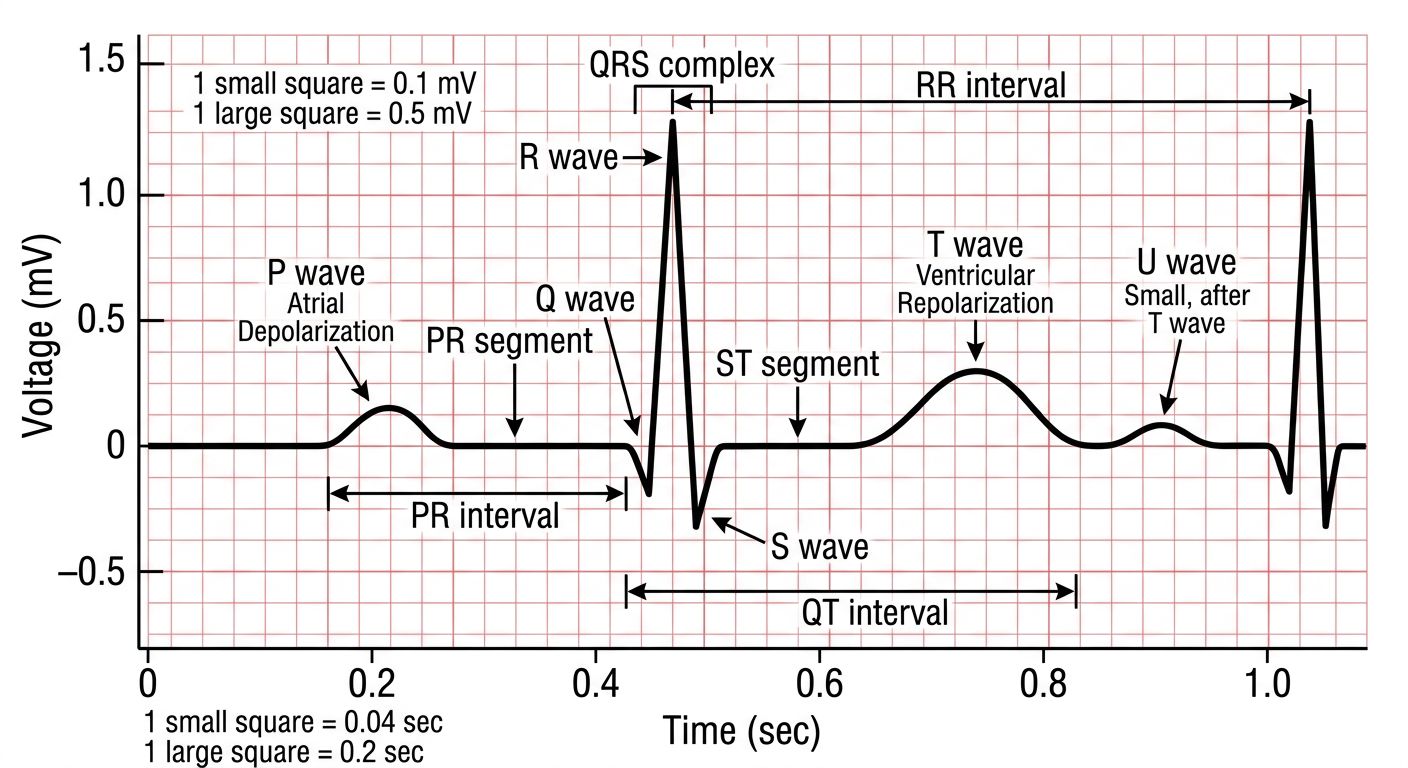
- P wave - small upright deflection; represents atrial depolarization (SA node → atria)
- Q wave - first small downward deflection of the QRS; septal depolarization
- R wave - tall upward spike; ventricular depolarization
- S wave - downward deflection after R; completion of ventricular depolarization
- T wave - broader upright wave after QRS; ventricular repolarization
- U wave - small wave after T (not always visible); possibly Purkinje repolarization
| Measurement | Normal Value | Represents |
|---|---|---|
| PR interval | 0.12 - 0.20 sec | AV node conduction time |
| QRS duration | < 0.12 sec (< 3 small squares) | Ventricular depolarization |
| QT interval | 0.36 - 0.44 sec (rate-dependent) | Total ventricular electrical activity |
| ST segment | Isoelectric (flat) | Early ventricular repolarization |
| PR segment | Isoelectric | Atrial repolarization + AV conduction |
- Horizontal: 1 small square = 0.04 sec; 1 large square = 0.2 sec
- Vertical: 1 small square = 0.1 mV; 1 large square = 0.5 mV
- Paper speed: 25 mm/sec
Bronchiectasis
Bronchiectasis
Definition
- Robbins & Kumar Basic Pathology, p. 455
Pathogenesis
Obstruction / Infection
↓
Impaired mucociliary clearance
↓
Mucus retention + bacterial colonisation
↓
Inflammatory cell recruitment
↓
Cytokines, proteases, bacterial toxins → bronchial wall destruction
↓
Airway dilation + peribronchial fibrosis
↓
Further impaired clearance → perpetuating cycle
- Bronchial obstruction - impairs secretion clearance → superimposed infection → inflammatory destruction
- Bronchial wall damage - direct necrotizing infection destroys wall structural components
- Parenchymal fibrosis (traction bronchiectasis) - maturing fibrous tissue adjacent to airways retracts and pulls bronchi open
- Grainger & Allison's Diagnostic Radiology, p. 155
- Robbins & Kumar Basic Pathology, p. 455
Causes / Aetiology
Post-Infectious (most common worldwide)
| Organism/Condition | Notes |
|---|---|
| Tuberculosis | Leading cause in endemic areas; post-TB bronchiectasis a major cause of morbidity |
| Bacterial pneumonia | Staphylococcus aureus, Klebsiella spp., Pseudomonas |
| Necrotizing/suppurative pneumonia | Direct destruction of bronchial walls |
| Pertussis, measles (in childhood) | Classic post-viral/post-bacterial |
| SARS-CoV-2 | Advanced bronchiectasis reported post-COVID-19 pneumonia |
Congenital / Hereditary
| Condition | Mechanism |
|---|---|
| Cystic fibrosis | Abnormally viscid mucus + secondary infection → widespread severe bronchiectasis |
| Primary ciliary dyskinesia (immobile cilia syndrome) | Autosomal recessive; defective cilia → impaired mucociliary clearance → persistent infections. Associated with situs inversus (Kartagener syndrome) and male sterility |
| Immunoglobulin deficiency (common variable immunodeficiency, X-linked agammaglobulinaemia) | Recurrent bacterial infections → localized or diffuse bronchiectasis |
| Alpha-1-antitrypsin deficiency | Protease-antiprotease imbalance |
Airway Obstruction
- Foreign body aspiration (localized, single segment)
- Endobronchial tumour
- Mucus impaction (e.g., ABPA - allergic bronchopulmonary aspergillosis)
- Atopic asthma, chronic bronchitis (proximal)
Other Causes
-
Rheumatoid arthritis (30% prevalence on CT - often clinically silent)
-
Inflammatory bowel disease
-
Post-lung transplant (obliterative bronchiolitis)
-
Young's syndrome
-
Recurrent aspiration
-
Robbins & Kumar Basic Pathology, p. 455
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 1699
Pathological Types (Morphological Classification)
| Type | Description | CT appearance |
|---|---|---|
| Cylindrical (tubular) | Uniform, regular airway dilation; airways fail to taper | Parallel "tram lines"; signet ring sign |
| Varicose | Non-uniform, irregular, serpiginous (beaded) dilation | Beaded/irregular bronchial lumen |
| Cystic (saccular) | Progressive ballooning into large cysts; most severe form | Cluster of cysts; air-fluid levels; string of cysts |
- Grainger & Allison's Diagnostic Radiology, p. 155
Macroscopic and Microscopic Pathology
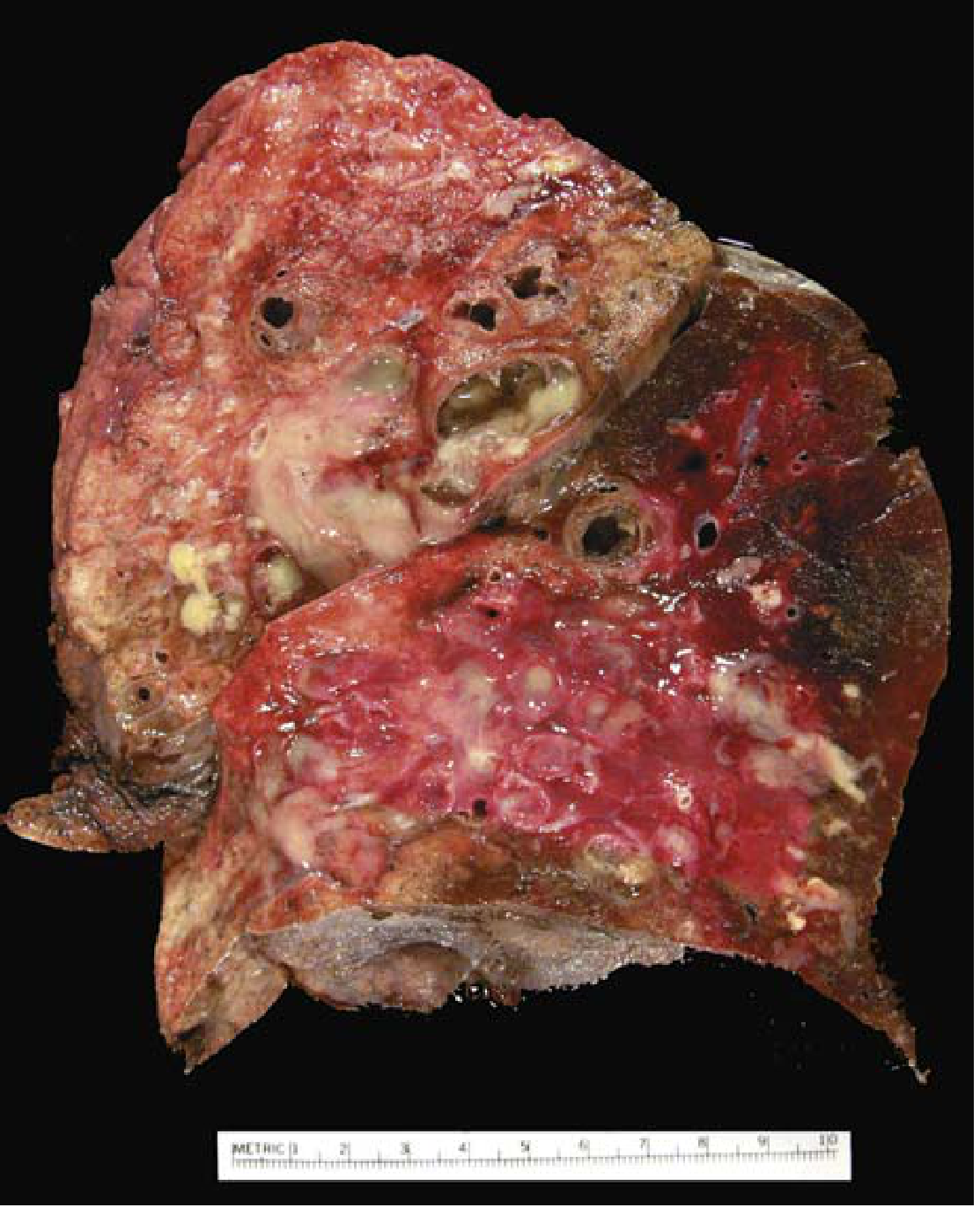
Macroscopic
- Airways dilated up to 4x their normal diameter
- Can be traced almost to the pleural surface (in health, bronchioles cannot be followed within 2-3 cm of pleura)
- Lower lobes predominantly affected bilaterally (most vertical air passages)
- Localized disease when caused by obstruction or aspiration
- Airways filled with mucopurulent or purulent material
Microscopic
-
Active phase: Intense acute and chronic inflammatory exudate within bronchial/bronchiolar walls; desquamation of lining epithelium; ulceration
-
Mixed bacterial flora: staphylococci, streptococci, H. influenzae, Pseudomonas aeruginosa, anaerobes
-
Chronic/healing phase: Fibrosis of bronchial walls; peribronchial fibrosis; goblet cell metaplasia; abscess cavity formation in severe cases
-
Complete epithelial regeneration is unusual - structural damage persists
-
Robbins & Kumar Basic Pathology, p. 455-456
Clinical Features
Symptoms
| Symptom | Details |
|---|---|
| Chronic productive cough | Cardinal symptom; ≥30 mL/day of mucopurulent or purulent sputum (sometimes foul-smelling) |
| Haemoptysis | Ranges from blood-streaked sputum to massive (from erosion of bronchial arteries) |
| Dyspnoea | Proportional to extent of disease |
| Rhinosinusitis | Frequently associated (particularly in cystic fibrosis, PCD) |
| Recurrent respiratory infections | Episodic exacerbations precipitated by URTI or new pathogens |
| Fever, malaise, weight loss | During infective exacerbations |
Signs
- Coarse crepitations (crackles) over affected areas - characteristically change with coughing and postural drainage
- Wheeze (from airway secretions or associated bronchoconstriction)
- Digital clubbing - in chronic severe bronchiectasis
- Signs of associated conditions (e.g., rheumatoid arthritis changes)
- In advanced disease: features of cor pulmonale (right heart failure from chronic hypoxia)
Complications
| Complication | Notes |
|---|---|
| Massive haemoptysis | Bronchial artery embolization required |
| Cor pulmonale | From chronic hypoxaemia in severe widespread disease |
| Respiratory failure | Hypoxaemia + hypercapnia |
| Amyloidosis (secondary/AA) | Rare complication of chronic suppurative disease |
| Brain abscess | Rare now with modern treatment |
- Robbins & Kumar Basic Pathology, p. 456
- Murray & Nadel's Textbook of Respiratory Medicine, p. 875
Investigations
Chest X-Ray
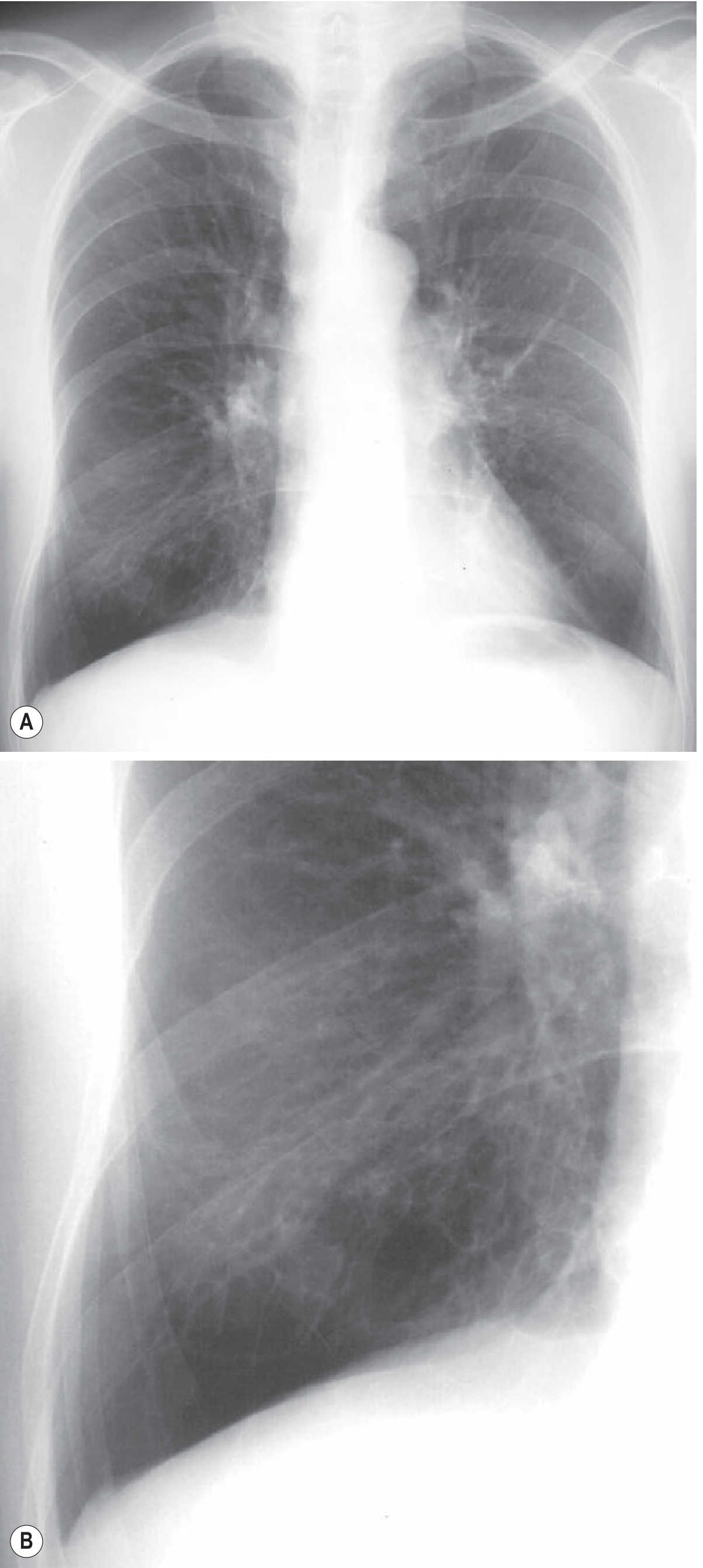
- Tram lines - thickened bronchial walls seen as parallel lines (bronchi viewed longitudinally)
- Ring shadows - dilated bronchi seen end-on; poorly defined rings or curvilinear opacities
- Tubular opacities - mucus-filled dilated bronchi (gloved-finger shadows)
- Air-fluid levels - in cystic/saccular bronchiectasis
- Increased bronchial wall thickening; lower lobe predominance in idiopathic disease
- Overinflation in CF; atelectasis/volume loss in localized disease
HRCT Chest (Gold Standard)
| CT Sign | Description |
|---|---|
| Signet ring sign | Bronchial internal diameter > diameter of adjacent pulmonary artery branch (like a signet ring - thick ring = bronchus; small dot = artery) |
| Lack of tapering | Bronchi fail to narrow as they travel peripherally |
| Bronchi within 1 cm of pleura | Normal bronchioles invisible this close to pleura |
| Bronchi abutting mediastinal pleura | Abnormal peripheral extension |
| Mucus plugging | Lobulated glove-finger-shaped opacities |
| Beaded bronchi | Varicose type |
| String of cysts / cluster of cysts | Cystic type; may contain air-fluid levels |
| Tree-in-bud | Associated bronchiolitis |
- Grainger & Allison's Diagnostic Radiology, p. 155-156
Pulmonary Function Tests
- Obstructive pattern most common (FEV1/FVC reduced)
- Restrictive pattern in severe fibrotic disease
- Mixed pattern possible
Microbiological Investigations
- Sputum culture (routine and AFB): identify colonizing/infecting organisms
- Common pathogens: H. influenzae, P. aeruginosa (associated with worse prognosis), S. aureus, Moraxella catarrhalis
- Sputum for NTM (non-tuberculous mycobacteria)
Aetiological Investigations (to identify the underlying cause)
- Serum immunoglobulins (IgG, IgA, IgM) - immunodeficiency
- Sweat chloride / CFTR gene testing - cystic fibrosis
- Nasal mucosal biopsy / ciliary beat frequency - primary ciliary dyskinesia
- Serum IgE, RAST for Aspergillus, total IgE - ABPA
- Alpha-1-antitrypsin level
- Autoantibodies (RF, ANA) - connective tissue disease
Management
Conservative / Medical
- Chest physiotherapy with postural drainage - essential; the basis of long-term management
- Active cycle of breathing techniques, oscillatory devices (Flutter, Acapella)
- Mucolytics (nebulized hypertonic saline, DNase in CF)
- Antibiotics guided by sputum culture and sensitivities
- H. influenzae: amoxicillin or co-amoxiclav
- Pseudomonas aeruginosa: ciprofloxacin (oral) or IV antipseudomonal penicillin/cephalosporin
- Duration typically 14 days (longer than standard pneumonia)
- Long-term macrolide therapy (azithromycin 3x/week) - reduces exacerbation frequency and improves lung function (anti-inflammatory + antibiotic effects)
- Inhaled antibiotics (tobramycin, colistin) for Pseudomonas-colonized patients
- Inhaled β2-agonists - improve mucociliary clearance and reverse bronchoconstriction
- Useful in patients with associated airflow obstruction
- Minor haemoptysis: usually managed with antibiotics
- Massive haemoptysis: bronchial artery embolization (interventional radiology)
- Annual influenza vaccine
- Pneumococcal vaccine
Surgical
-
Reserved for localized bronchiectasis not responding to medical treatment
-
Lobectomy or segmentectomy of the most severely affected lobe
-
Low mortality in carefully selected patients
-
Lung transplantation - for end-stage bilateral bronchiectasis (e.g., CF)
-
Robbins & Kumar Basic Pathology, p. 456
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 875
Summary
| Feature | Detail |
|---|---|
| Definition | Irreversible bronchial/bronchiolar dilation from wall destruction |
| Key mechanism | Obstruction + infection vicious cycle |
| Most common cause (worldwide) | Post-TB / post-infectious |
| Most common cause (congenital) | Cystic fibrosis |
| Cardinal symptom | Chronic productive cough (>30 mL/day purulent sputum) |
| Imaging gold standard | HRCT chest |
| Pathognomonic CT sign | Signet ring sign; lack of bronchial tapering |
| CXR sign | Tram lines, ring shadows |
| Common pathogens | H. influenzae, P. aeruginosa, S. aureus |
| Core treatment | Airway clearance + antibiotics for exacerbations |
| Long-term prevention | Macrolide therapy (azithromycin) |
| Distribution | Lower lobes bilateral (idiopathic); upper lobes in CF/TB |
Diagram
A clean medical educational diagram showing the three morphological types of bronchiectasis side by side, comparing them to a normal bronchus. Four panels arranged horizontally: Panel 1 - Normal bronchus: smooth tapering tube that narrows progressively towards the periphery, with thin walls, labeled "Normal". Panel 2 - Cylindrical (tubular) bronchiectasis: uniformly dilated bronchus that does not taper, maintains same diameter throughout, with slightly thickened walls, labeled "Cylindrical (Tubular)". Panel 3 - Varicose bronchiectasis: irregular, non-uniform dilation with alternating areas of dilation and constriction giving a beaded or string-of-pearls appearance, labeled "Varicose". Panel 4 - Cystic (saccular) bronchiectasis: progressive ballooning into large rounded sac-like dilations at the ends of bronchi, like clusters of grapes or cysts, labeled "Cystic (Saccular)". Each panel shows cross-sectional and longitudinal view. Use clear labels, arrows, and light blue/pink color scheme. Include a severity arrow below showing increasing severity from cylindrical to cystic. Medical textbook illustration style, white background.
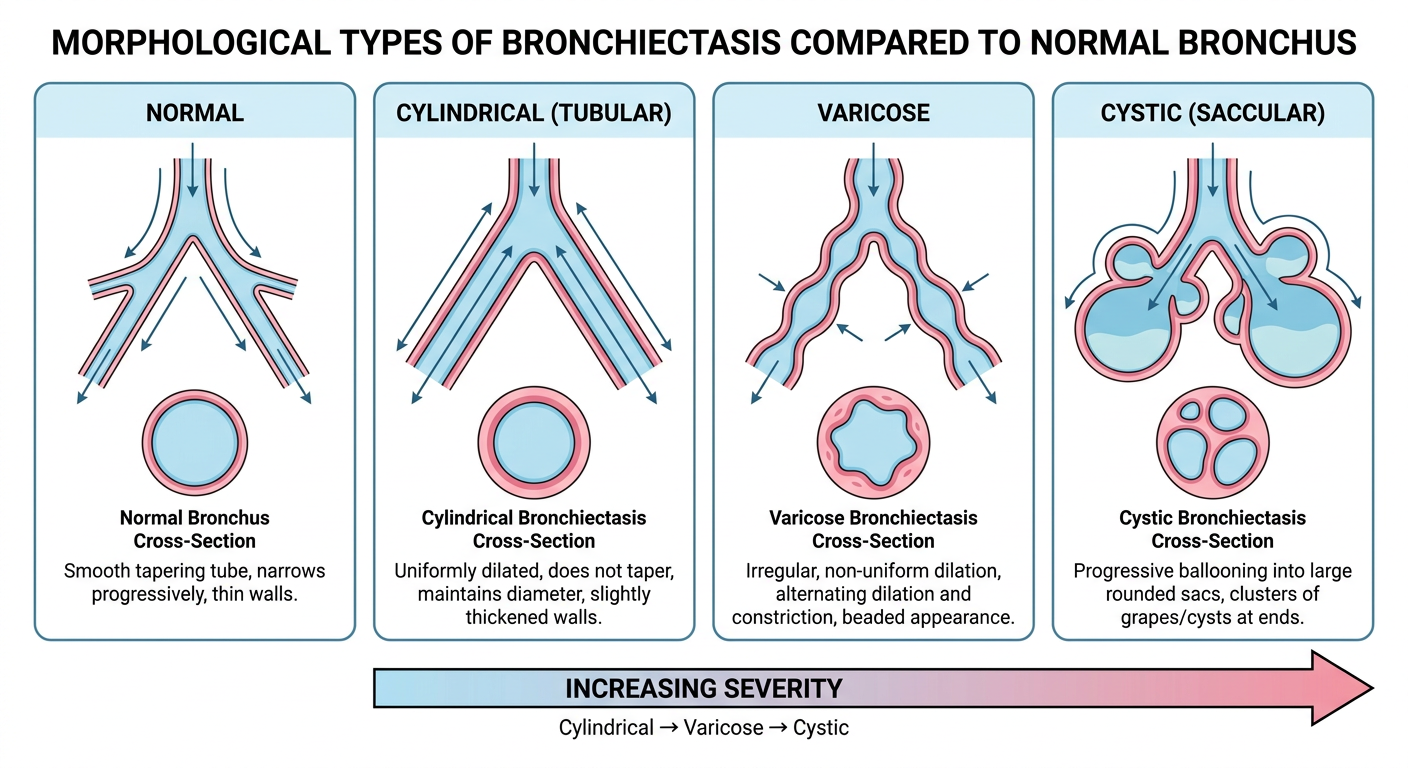
| Type | Key Feature | Severity | CT Appearance |
|---|---|---|---|
| Normal | Smooth, progressive tapering toward periphery | - | Normal tapering bronchi |
| Cylindrical | Uniform dilation, no tapering; parallel walls | Mild | Tram lines; signet ring sign |
| Varicose | Irregular, beaded/non-uniform dilation | Moderate | Beaded bronchial lumen |
| Cystic (Saccular) | Progressive ballooning into large sac-like cavities | Severe | Clusters of cysts; air-fluid levels |
Cor pulmonae