Pneumonia
Reading File
Finding Sources
Searching PubMed
"pneumonia" AND "community-acquired"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks to compose a thorough answer. Let me put it all together.
Pneumonia
Definition & Classification
Pneumonia is an infection of the alveolar (gas-exchanging) portion of the lung. It is classified by the setting in which it is acquired, since this strongly predicts likely pathogens and guides empiric antibiotic choice:
| Classification | Criteria |
|---|---|
| Community-acquired (CAP) | Acute pulmonary infection in a patient not hospitalized or in long-term care for ≥14 days before presentation |
| Hospital-acquired (HAP) | New infection occurring ≥48 h after hospital admission |
| Ventilator-acquired (VAP) | New infection ≥48 h after endotracheal intubation |
| Healthcare-associated (HCAP) | Hospitalized ≥2 days in last 90 days; nursing home residents; home IV antibiotics; dialysis; wound care; chemotherapy; immunocompromised |
- Tintinalli's Emergency Medicine, Table 65-1
Epidemiology
CAP causes approximately 3 million cases and 1.6 million hospitalizations per year in the United States. Mortality is <5% in outpatients but rises to 12-40% in hospitalized patients, and up to 29% in the sickest (PSI class V). It is the eighth leading cause of death overall and the leading cause of infection-related death in patients over 65.
- Harrison's Principles of Internal Medicine 22E, Chapter 131
Pathophysiology
Organisms reach the lung primarily by aspiration of oropharyngeal secretions (most common) or by inhalation of aerosolized particles. Hematogenous spread (e.g., S. aureus, S. pneumoniae) is less common. Once in the alveoli, bacteria trigger an intense inflammatory response causing:
- Filling of air spaces with exudate and WBCs (consolidation)
- Spread through the bronchial tree and via alveolar pores (Kohn)
- Possible pleural involvement (pleuritic chest pain)
Risk factors include aspiration predisposition (stroke, seizures, NG tube), impaired mucociliary clearance (COPD, smoking), and bacteremia risk (indwelling devices, debilitation).
Causative Organisms
Community-Acquired Pneumonia (most common)
- Streptococcus pneumoniae - most common bacterial cause overall; classic lobar pattern, rusty sputum, rigors
- Atypical organisms (Mycoplasma pneumoniae, Chlamydia pneumoniae, Legionella spp.) - lack cell wall, do not respond to beta-lactams; treated with macrolides or fluoroquinolones
- Haemophilus influenzae - elderly, COPD, immunocompromised
- Staphylococcus aureus - post-viral (influenza), CA-MRSA risk with structural lung disease or healthcare exposure
- Klebsiella pneumoniae - alcoholics, elderly, aspiration risk; classic "currant-jelly sputum" (rarely seen in practice)
- Viruses - influenza A/B, RSV, parainfluenza, adenovirus, SARS-CoV-2
Epidemiologic clues to pathogens (from Harrison's, Table 131-2):
| Exposure / Risk | Consider |
|---|---|
| Alcoholism | S. pneumoniae, oral anaerobes, Klebsiella, M. tuberculosis |
| COPD / smoking | H. influenzae, Pseudomonas, Legionella, S. pneumoniae, Moraxella |
| Structural lung disease (bronchiectasis) | Pseudomonas, Burkholderia, S. aureus |
| Stroke / decreased consciousness | Oral anaerobes, gram-negative enteric bacteria |
| Hotel / cruise ship exposure | Legionella |
| Bird exposure | Histoplasma, Chlamydia psittaci |
| Southwestern US travel | Hantavirus, Coccidioides |
| Exposure to SARS-CoV-2 contacts | SARS-CoV-2 |
Clinical Features
Typical (bacterial) pneumonia:
- Abrupt onset of fever, rigors, pleuritic chest pain
- Productive cough (purulent or rusty sputum)
- Tachypnea, tachycardia, hypoxia
- Exam: dullness to percussion, tubular breath sounds, rales over affected area
Atypical pneumonia:
- More gradual onset, dry cough, constitutional symptoms (headache, myalgias)
- Physical exam findings may be minimal despite extensive chest X-ray changes ("walking pneumonia")
Viral pneumonia:
- Interstitial pattern on imaging (bilateral diffuse infiltrates)
- Hyaline membrane formation histologically
- Limited auscultatory findings on exam
Severity Assessment and Site of Care
Two tools are widely used:
CURB-65 (5 variables, 1 point each)
| Variable | Criterion |
|---|---|
| Confusion | New disorientation |
| Urea | BUN >7 mmol/L (>19 mg/dL) |
| Respiratory rate | ≥30 breaths/min |
| Blood pressure | Systolic ≤90 or diastolic ≤60 mmHg |
| Age | ≥65 years |
- Score 0: outpatient (30-day mortality ~1.5%)
- Score 1-2: consider inpatient (unless age alone drives the score)
- Score ≥3: high mortality (~22%), consider ICU
PSI (Pneumonia Severity Index)
Uses 20 variables (age, comorbidities, labs, physical findings) to assign risk class I-V. More accurate than CURB-65 but harder to calculate at the bedside. Mortality by class: I (0.1%), II (0.6%), III (2.8%), IV (8.2%), V (29.2%).
ICU admission criteria (ATS/IDSA minor criteria)
Direct ICU admission for septic shock or need for mechanical ventilation. Consider ICU/high-monitoring unit if ≥3 of the following:
-
Respiratory rate ≥30/min
-
PaO2/FiO2 ≤250
-
Multilobar infiltrates
-
Confusion/disorientation
-
BUN ≥20 mg/dL
-
Leukopenia (WBC <4,000)
-
Thrombocytopenia (<100,000)
-
Hypothermia (<36°C)
-
Hypotension requiring aggressive fluid resuscitation
-
Harrison's Principles of Internal Medicine 22E, Chapter 131
Treatment
Initial therapy is empirical since the causative organism is rarely identified at presentation. Coverage is guided by severity, comorbidities, and risk for drug-resistant organisms (MRSA, Pseudomonas).
Outpatient CAP (no comorbidities)
- Macrolide (azithromycin, clarithromycin) OR
- Doxycycline
Outpatient CAP (with comorbidities: cardiac/pulmonary/hepatic/renal disease, diabetes, alcoholism, malignancy, asplenia)
- Respiratory fluoroquinolone (levofloxacin 750 mg/day x5d; moxifloxacin 400 mg/day) OR
- Beta-lactam (amoxicillin-clavulanate 2 g twice daily or 3rd-gen cephalosporin) plus macrolide/doxycycline
Inpatient (non-ICU)
- Beta-lactam + macrolide OR
- Respiratory fluoroquinolone monotherapy
Inpatient (ICU)
- Beta-lactam + azithromycin OR beta-lactam + respiratory fluoroquinolone
- Add MRSA coverage (vancomycin or linezolid) if: prior respiratory isolation of MRSA, or recent hospitalization + IV antibiotics
- Add Pseudomonas coverage if: structural lung disease, prior Pseudomonas isolation, or recent hospitalization + IV antibiotics
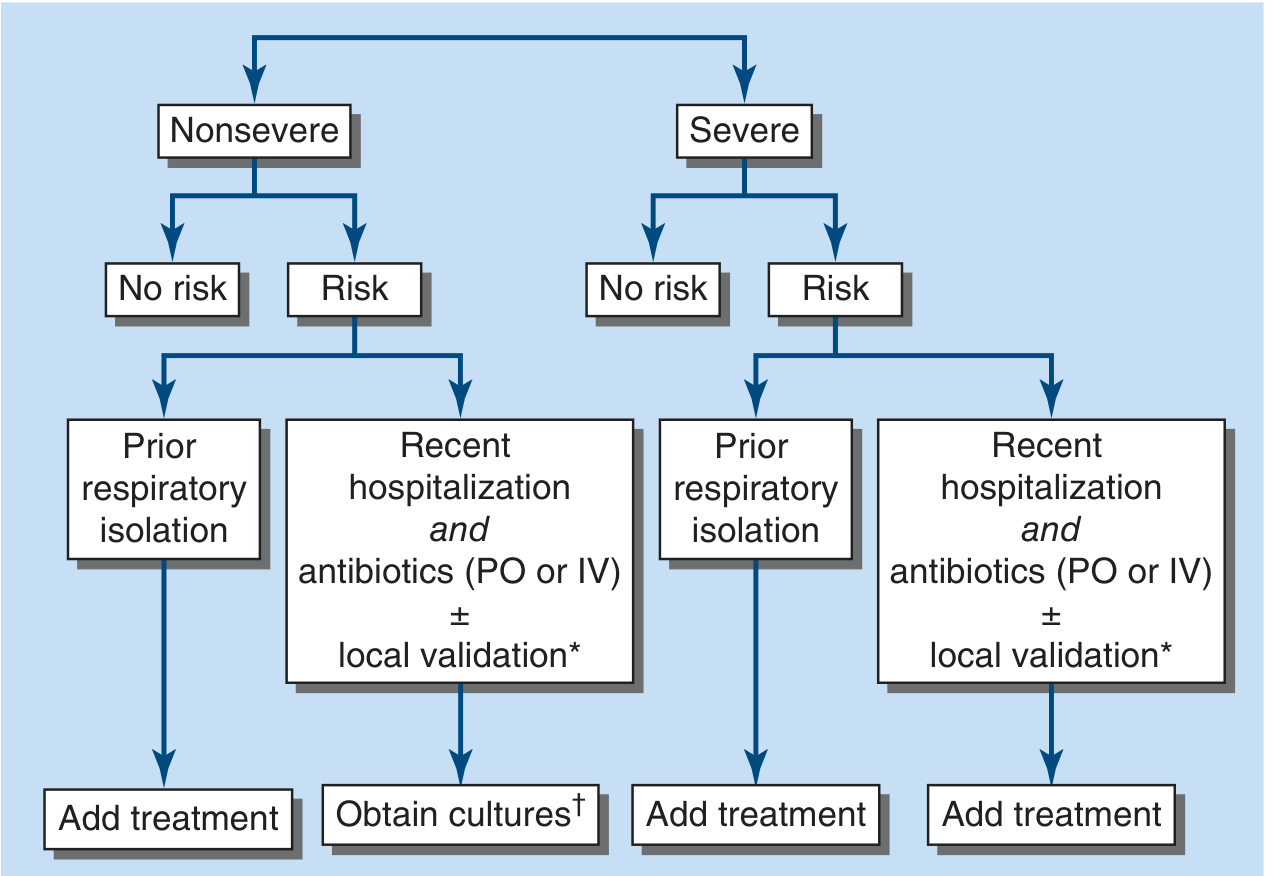
FIGURE: ATS/IDSA algorithm for assessing inpatient MRSA and Pseudomonas aeruginosa risk in CAP (Harrison's Principles of Internal Medicine 22E)
Atypical agents
Because Mycoplasma, Chlamydia, and Legionella lack a cell wall, beta-lactams are ineffective. Use macrolides or respiratory fluoroquinolones. Note: macrolide-resistant Mycoplasma is increasing globally (up to 95% in China, 5-13% in the US). - Tintinalli's Emergency Medicine, Chapter 65
Aspiration pneumonia
Routine anaerobic coverage is not needed unless:
- Poor dentition
- Lung abscess present
- Necrotizing pneumonia (treat 3-12 weeks with systemic antibiotics)
Antibiotic Resistance - Key Points
- S. pneumoniae: resistance to beta-lactams via altered penicillin-binding proteins; increasing macrolide resistance
- CA-MRSA: risk in post-influenza, structural lung disease; associated with Panton-Valentine leukocidin (PVL) causing severe necrotizing infection - must be recognized early
- ESBLs / gram-negatives: fluoroquinolone-resistant E. coli increasing; ESBL-producers warrant carbapenem consideration
- Fluoroquinolone caution: CDC recommends reserving for patients failing first-line therapy, documented resistance, or contraindications to alternatives; contraindicated in myasthenia gravis
Recent Evidence (2024-2026)
- A 2025 meta-analysis (PMID 40107661) identified key risk factors for drug-resistant pathogens in CAP, supporting targeted antibiotic selection based on individual patient risk profiles.
- A 2025 Lancet Respiratory Medicine analysis (PMID 39892408) examined adjuvant corticosteroids in CAP, finding benefit in select subgroups (particularly those with high inflammatory markers) but not all patients.
- A 2024 meta-analysis in Pediatric Pulmonology (PMID 39239917) confirmed lung ultrasound is at least as accurate as chest X-ray for diagnosing CAP in children, supporting its growing use to reduce radiation exposure.
Sources: Harrison's Principles of Internal Medicine 22E (Chapter 131), Tintinalli's Emergency Medicine (Chapter 65), Fishman's Pulmonary Diseases and Disorders (Chapter 122), Jawetz, Melnick & Adelberg's Medical Microbiology 28E (Chapter 48)
This is a shared conversation. Sign in to Orris to start your own chat.