Whathappens if bilirubin is 38 mg/dl due to jaundice caused by viral hepatitis
severe hyperbilirubinemia viral hepatitis outcomes
Bilirubin of 38 mg/dL in Viral Hepatitis - What It Means Clinically
Understanding the Level
What Is Happening Pathophysiologically
- Massive hepatocellular necrosis - Viral destruction of hepatocytes overwhelms the liver's capacity to process bilirubin
- Intrahepatic cholestasis - Inflammation disrupts the canalicular transport proteins (especially MRP2/ABCC2)
- Impaired conjugation - Reduced functional hepatocyte mass means less bilirubin conjugation
- Possible progression to acute liver failure (ALF) - At 38 mg/dL, the liver is under extreme stress
Clinical Consequences and Complications
Direct Signs of Severe Jaundice
- Deep yellow-orange to greenish skin and scleral icterus
- Dark ("tea-colored" or "Coca-Cola") urine from bilirubinuria (conjugated bilirubin is water-soluble and excreted in urine)
- Pale/clay-colored stools from reduced bile flow into intestine
- Intense pruritus from bile salt deposition in skin
Systemic Complications (Acute Liver Failure Spectrum)
| Complication | Mechanism |
|---|---|
| Hepatic encephalopathy | Failure to clear ammonia and other neurotoxins; ranges from confusion (Grade 1-2) to coma (Grade 3-4) |
| Coagulopathy (INR > 1.5) | Impaired synthesis of clotting factors (I, II, V, VII, X) - spontaneous bleeding risk |
| Hepatorenal syndrome | Reduced renal perfusion; kidney failure without intrinsic kidney disease |
| Cerebral edema | From ammonia toxicity; leading cause of death in ALF |
| Hypoglycemia | Impaired hepatic glycogenolysis and gluconeogenesis |
| Metabolic acidosis / lactic acidosis | Impaired lactate clearance |
| Infections / sepsis | Compromised Kupffer cell function and immune defense |
| Ascites | Portal hypertension + hypoalbuminemia |
| Electrolyte imbalances | Hyponatremia, hypokalemia are common |
Bilirubin Itself at This Level
- Cross the blood-brain barrier if albumin-binding capacity is overwhelmed, causing bilirubin encephalopathy (though this is more clinically relevant in neonates; in adults the BBB is more protective unless severely disrupted)
- Cause renal tubular injury - contributes to hepatorenal syndrome
- Exert oxidative stress on red blood cells and other tissues
Prognostic Significance
Management Priorities
- ICU admission - Close monitoring of neurological status, hemodynamics, renal function
- Assess for ALF - Check INR, factor V, ammonia, creatinine, blood glucose, pH
- Specific antiviral therapy if applicable:
- Hepatitis B: nucleos(t)ide analogues (entecavir/tenofovir)
- Herpes simplex hepatitis: acyclovir
- Hepatitis A/E: mostly supportive
- N-acetylcysteine (NAC) - Commonly used in non-acetaminophen ALF (hepatitis B, idiosyncratic) especially with Grade 1-2 encephalopathy
- Manage encephalopathy - Lactulose, rifaximin, low-protein diet, intracranial pressure monitoring if severe
- Treat coagulopathy - FFP if active bleeding; avoid prophylactic correction as it masks the INR trend
- Renal replacement therapy if hepatorenal syndrome develops
- Emergency liver transplant evaluation - The most definitive treatment if the liver fails to recover
Which Hepatitis Virus Matters
| Virus | Severity Likelihood at This Bilirubin |
|---|---|
| Hepatitis A | Can cause severe cholestatic hepatitis; rarely fulminant (~0.5% mortality overall, higher in elderly) |
| Hepatitis B | Can cause fulminant hepatitis, especially in coinfection with delta (HDV) |
| Hepatitis C | Rarely causes fulminant disease acutely |
| Hepatitis E | Most dangerous in pregnancy - can reach very high bilirubin with 15-25% maternal mortality |
Bottom Line
- Harrison's Principles of Internal Medicine 22E, p. 2678
- Goldman-Cecil Medicine, p. 1623
- Miller's Anesthesia 10e, p. 8641
Can it be cured
acute viral hepatitis severe jaundice outcomes survival
Can Bilirubin of 38 mg/dL from Viral Hepatitis Be Cured?
The Good News: Most Viral Hepatitis Can Resolve
"Most persons with acute hepatitis (especially hepatitis A, B, and E) recover spontaneously and do not require specific antiviral therapy."
Recovery Chances by Virus Type
| Virus | Can It Be Cured? | Notes |
|---|---|---|
| Hepatitis A | Yes - almost always | Self-limiting. No antiviral exists, but the immune system clears it fully. Even severe cases usually resolve in 4-8 weeks. No chronic form. |
| Hepatitis B (acute) | Yes - ~99% of healthy adults recover | Spontaneous clearance in most cases. If severe (like this case), antivirals (entecavir or tenofovir) are added to prevent progression to full liver failure. |
| Hepatitis C (acute) | Curable with treatment | Only 15-20% clear spontaneously. But modern Direct-Acting Antivirals (DAAs) achieve 95-100% cure rates. Early treatment is now recommended. |
| Hepatitis E | Usually yes | Self-limiting in immunocompetent people. Dangerous in pregnancy (15-25% maternal mortality) and immunocompromised patients. |
What "Cured" Actually Means Here
Path 1 - Spontaneous Recovery (Best case)
Path 2 - Antiviral Treatment + Recovery
- Goldman-Cecil recommends entecavir (0.5 mg/day) or tenofovir started before acute liver failure develops
- This prevents progression and allows the liver to recover
- Treatment does NOT make Hepatitis B chronic
Path 3 - Liver Transplant (if liver fails)
What Determines Whether This Patient Recovers
- How early treatment is started - starting antivirals for Hep B before liver failure is the critical window
- INR (clotting ability) - if INR stays below 1.5, recovery is likely. If it rises rapidly, the liver is losing its synthetic function
- Presence of encephalopathy - if the patient is confused or drowsy, this indicates rising ammonia and impending failure
- Patient age and pre-existing liver disease - a previously healthy young person has far better odds than someone with underlying cirrhosis
- Renal function - kidney failure alongside liver failure (hepatorenal syndrome) worsens prognosis significantly
What Should Be Done Right Now
- ICU-level monitoring - watch INR, ammonia, creatinine, blood glucose daily
- Identify the virus - anti-HAV IgM, HBsAg, HBeAg, anti-HCV, anti-HEV
- Start entecavir or tenofovir if Hepatitis B confirmed with severe features
- Start DAA therapy (e.g., sofosbuvir + velpatasvir) if acute Hepatitis C
- Supportive care - IV fluids, high-calorie feeds, avoid all liver-toxic drugs
- Liver transplant team on standby - register the patient at a transplant center early, do not wait until the liver fully fails
Timeline for Recovery (If No Failure)
- Bilirubin typically peaks then begins falling over 2-4 weeks
- Most patients with Hep A/B are clinically well within 4-8 weeks
- Liver enzymes normalize by 3-6 months
- The person can return to a completely normal life with a fully functioning liver
- Harrison's Principles of Internal Medicine 22E, p. (Acute Viral Hepatitis section)
- Goldman-Cecil Medicine International Edition, Hepatitis B Treatment section
What if direct bilirubin is 16 mg/dl and indirect bilirubin is 23 mg/dl and what are the physical features observed in the patient
Direct 16 mg/dL + Indirect 23 mg/dL = Total 39 mg/dL
First: What This Pattern Tells You
| Fraction | Value | % of Total | Normal |
|---|---|---|---|
| Direct (conjugated) | 16 mg/dL | 41% | < 0.3 mg/dL |
| Indirect (unconjugated) | 23 mg/dL | 59% | < 1.0 mg/dL |
| Total | 39 mg/dL | 100% | < 1.2 mg/dL |
Why Indirect Bilirubin Is Dominant: Possible Explanations
1. Massive Hepatocellular Necrosis (Hepatic Cause)
"When hepatocytes necrose, the liver's ability to conjugate bilirubin is impaired, and the level of unconjugated bilirubin rises in the blood."
2. Superimposed Hemolysis (Prehepatic component)
3. Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency + Viral Trigger
Physical Features Observed in This Patient
Skin and Eye Changes
- Deep yellow-orange jaundice of skin, mucous membranes - at 39 mg/dL this is profound, visible even in dark-skinned individuals
- Scleral icterus (yellowing of the whites of the eyes) - often the earliest and most striking sign; remains yellow even after skin starts clearing
- Yellow tinge of the oral mucosa and under the tongue
- Skin may have a greenish hue if direct bilirubin component causes long-standing cholestasis
Urine and Stool Changes
| Feature | Finding | Why |
|---|---|---|
| Urine color | Dark yellow to amber-brown ("tea colored") | Conjugated bilirubin (the 16 mg/dL direct fraction) is water-soluble - excreted in urine |
| Urine bilirubin dipstick | Positive | Due to conjugated fraction |
| Urobilinogen in urine | Elevated | Increased bilirubin load reaches gut, more urobilinogen reabsorbed |
| Stool color | Pale/light brown but NOT fully acholic (clay-colored) | Some bile still reaching gut; fully clay stools suggest pure obstruction |
Note: In pure hemolysis (prehepatic jaundice), urine bilirubin is negative because only unconjugated bilirubin is present (it binds albumin and is not filtered). Here, because direct bilirubin is also elevated, urine will be bilirubin-positive.
Signs of Hemolysis (from the high indirect fraction)
- Pallor - anemia from red cell destruction
- Splenomegaly - spleen enlarges as it destroys damaged red blood cells
- Tachycardia - compensating for anemia
- Fatigue and breathlessness - from low hemoglobin
Signs from Liver Disease / Viral Hepatitis
- Hepatomegaly - enlarged, tender liver on right upper quadrant palpation
- Right upper quadrant tenderness - from liver capsule stretch and inflammation
- Anorexia, nausea, vomiting - from hepatic inflammation and cytokine release
- Fever - active viral infection (common in early hepatitis A, E)
- Fatigue, malaise - one of the earliest symptoms
- Loss of taste for cigarettes/alcohol - classic early symptom of hepatitis
- Splenomegaly - can occur in hepatitis from portal hypertension or viral activation of the spleen (especially EBV/CMV)
Pruritus (Itching)
- Present but may be less severe than in pure obstructive jaundice - pruritus is mainly caused by bile salts deposited in skin, which is more pronounced when direct (conjugated) bilirubin dominates
- At 16 mg/dL direct bilirubin, moderate-to-severe pruritus is expected - scratch marks (excoriations) may be visible on skin
Neurological Signs (from the very high indirect bilirubin)
- Unconjugated bilirubin binds albumin in blood. At very high levels, the albumin-binding capacity becomes saturated and free unconjugated bilirubin can cross the blood-brain barrier
- In adults, the BBB is more resistant than in neonates, but at these extreme levels, especially if albumin is low (as in sick hepatitis patients), neurological effects are possible:
- Drowsiness, confusion (may overlap with hepatic encephalopathy from ammonia)
- Altered consciousness
- Clinically, it becomes difficult to separate bilirubin toxicity from ammonia-driven encephalopathy at this stage
Signs of Acute Liver Failure (if present)
- Asterixis ("liver flap") - involuntary flapping tremor of outstretched hands; sign of encephalopathy
- Fetor hepaticus - musty, sweet-smelling breath from mercaptans (sulfur compounds) the diseased liver cannot clear
- Bruising and bleeding - from coagulopathy (nose bleeds, gum bleeding, easy bruising)
- Ascites - fluid in abdomen, causing distension and shifting dullness on percussion
Summary: Direct vs. Indirect - What Each Component Tells Clinically
| Direct (16 mg/dL) - Conjugated | Indirect (23 mg/dL) - Unconjugated |
|---|---|
| Dark urine, bilirubin-positive dipstick | Pallor from hemolytic anemia |
| Pruritus (bile salts in skin) | Splenomegaly |
| Suggests hepatocellular injury OR bile duct component | Suggests failed conjugation OR active hemolysis |
| Light/pale stools | Normal or near-normal stool color |
What Investigations Should Be Ordered
- Peripheral blood smear - look for fragmented red cells (schistocytes), spherocytes, or bite cells (G6PD)
- Reticulocyte count - elevated in hemolysis
- LDH and haptoglobin - LDH elevated, haptoglobin low in hemolysis
- Coombs test (Direct Antiglobulin Test) - positive in immune-mediated hemolysis (Hep A, EBV)
- G6PD screen - especially in at-risk populations
- Serum albumin - low albumin raises risk of free unconjugated bilirubin crossing BBB
- INR, ammonia, creatinine - assess for acute liver failure
- Viral serology - anti-HAV IgM, HBsAg, anti-HCV, anti-HEV, EBV/CMV titers
Bottom Line
- Tintinalli's Emergency Medicine, Jaundice Pathophysiology section
- Henry's Clinical Diagnosis and Management by Laboratory Methods, Derangements of Bilirubin Metabolism
- Maingot's Abdominal Operations, Clinical Presentation of Jaundice
What specialist should be shown
Which Specialists Should This Patient See?
1. Hepatologist (Liver Specialist) - THE PRIMARY DOCTOR
- They are the expert in viral hepatitis - identifying the virus, staging the severity, and directing treatment
- They decide whether antivirals (entecavir/tenofovir for Hep B, DAAs for Hep C) should be started
- They assess MELD score and determine if the liver is heading toward failure
- They coordinate the entire treatment team
- As Harrison's confirms: "The cornerstone of management is meticulous intensive care" - the hepatologist leads this
- Liver biopsy if needed
- Prescribe antivirals
- Monitor for progression to acute liver failure
- Serial bilirubin, INR, and ammonia tracking
2. Intensivist (ICU Specialist) - EQUALLY URGENT
- Hemodynamic instability (low blood pressure from liver failure)
- Airway protection if encephalopathy worsens
- Mechanical ventilation if needed
- Cerebral edema monitoring and management
- Fluid and electrolyte balance
- Prevention of sepsis and infection - a leading cause of death in liver failure
3. Hematologist - FOR THE HIGH INDIRECT BILIRUBIN
- Diagnose the cause of hemolysis (G6PD deficiency, autoimmune hemolytic anemia from Hep A/EBV, microangiopathic processes)
- Manage severe anemia - the patient may need blood transfusion
- Assess coagulopathy from a blood perspective
- Rule out disseminated intravascular coagulation (DIC)
- If G6PD-triggered: identify and stop all offending drugs immediately
4. Nephrologist (Kidney Specialist) - IF RENAL FUNCTION DROPS
- Monitors creatinine, urine output, and electrolytes
- Initiates renal replacement therapy (dialysis/CRRT) if hepatorenal syndrome develops
- Helps manage fluid overload and electrolyte imbalances (hyponatremia is common)
5. Liver Transplant Surgeon / Transplant Team - MUST BE NOTIFIED EARLY
"Liver transplantation is resorted to with increasing frequency, with excellent results, in patients with fulminant hepatitis."
6. Infectious Disease Specialist - IF VIRUS NOT YET IDENTIFIED
- If the specific hepatitis virus is not confirmed, they help identify uncommon causes (EBV, CMV, HSV, dengue, leptospirosis - all can cause severe hepatitis with high bilirubin)
- They guide antiviral choices
- They manage superinfections (bacterial infections are common in liver failure patients)
- They are especially important if hepatitis E is suspected in pregnancy or immunocompromised patients
7. Neurologist - IF ENCEPHALOPATHY DEVELOPS
- The high indirect bilirubin (23 mg/dL) plus ammonia from liver failure can both affect the brain
- A neurologist helps distinguish hepatic encephalopathy from bilirubin toxicity or other causes
- EEG monitoring may be needed in comatose patients
- Intracranial pressure monitoring guidance
Summary: Who to See and When
| Priority | Specialist | When to Involve |
|---|---|---|
| 1 - Immediate | Hepatologist | Right now - primary doctor |
| 1 - Immediate | Intensivist / ICU | Admit to ICU now |
| 2 - Urgent | Hematologist | Within hours - for high indirect bilirubin workup |
| 2 - Urgent | Transplant Team | Notify now, evaluate within 24 hours |
| 3 - As needed | Nephrologist | If creatinine rises or urine output drops |
| 3 - As needed | Infectious Disease | If virus unidentified or superinfection suspected |
| 4 - If develops | Neurologist | If confusion, seizures, or coma appear |
Where Should the Patient Be?
- Admission to a tertiary hospital (one that has hepatology, ICU, and liver transplant services under one roof)
- ICU-level monitoring at minimum
- Proximity to a liver transplant center - if not already there, transfer immediately
- Harrison's Principles of Internal Medicine 22E - Acute Viral Hepatitis, Fulminant Hepatitis sections
- Goldman-Cecil Medicine - Acute Liver Failure Management
What if the patient doesn't hae hepatitis
What If It's Not Hepatitis? - Full Differential Diagnosis
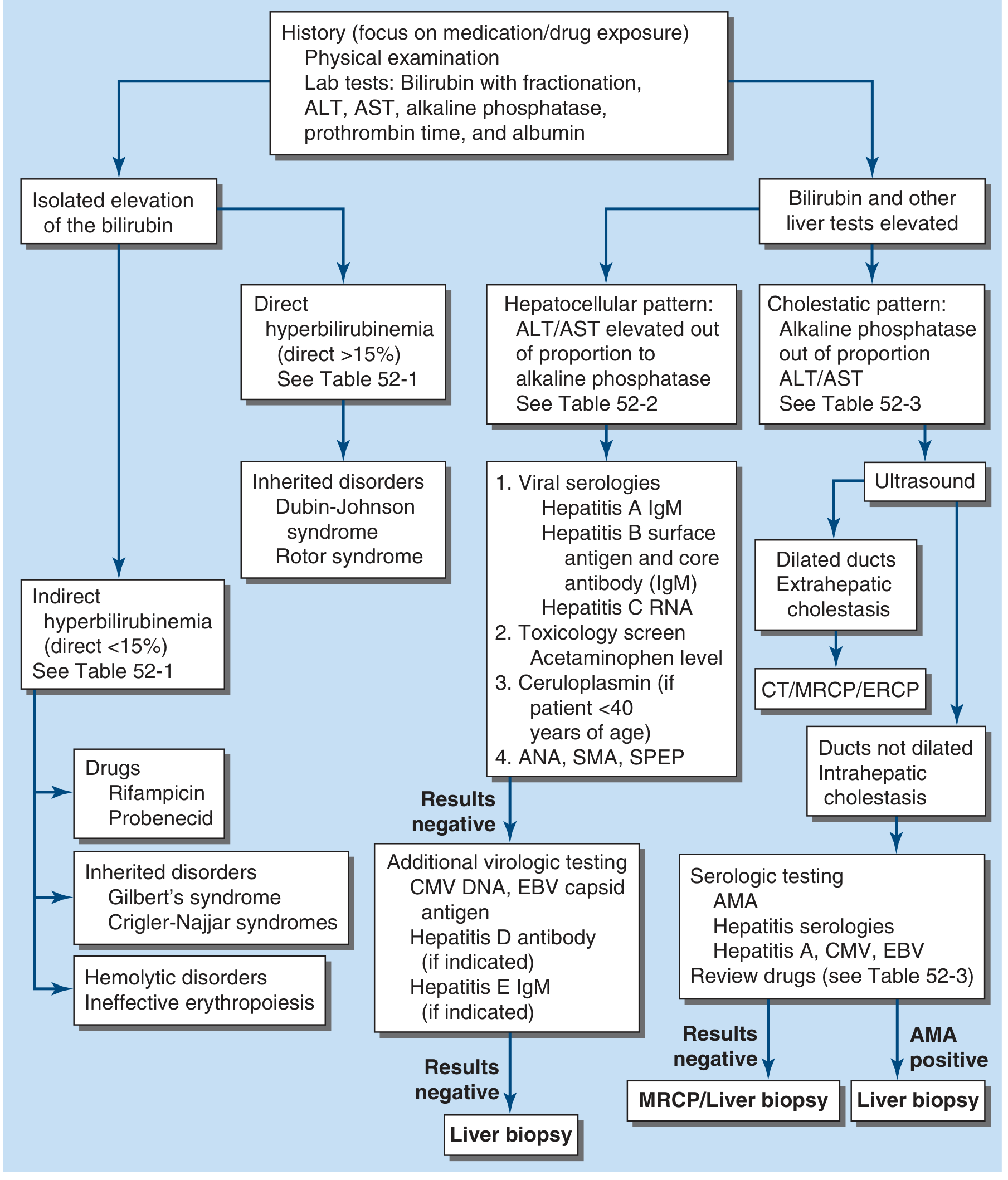
Understanding the Pattern First
"Unconjugated hyperbilirubinemia is present when the direct fraction is <15% of the total serum bilirubin."
Category 1 - PREHEPATIC Causes (Indirect bilirubin dominant)
A. Hemolytic Disorders
| Condition | Key Features |
|---|---|
| Sickle cell disease (crisis) | Acute bone/joint pain, acute chest syndrome, prior sickling episodes, African/Mediterranean descent |
| Thalassemia | Chronic anemia, Mediterranean/Asian origin, splenomegaly since childhood |
| Hereditary spherocytosis | Family history, spherocytes on blood smear, splenomegaly |
| G6PD deficiency | Triggered by drugs, infections, fava beans; bite cells on smear; common in males |
| Pyruvate kinase deficiency | Rare, chronic hemolytic anemia |
| Condition | Key Features |
|---|---|
| Autoimmune hemolytic anemia (AIHA) | Positive Coombs test, can be triggered by drugs, lymphoma, lupus |
| Microangiopathic hemolytic anemia (MAHA) | Schistocytes on smear; seen in HUS, TTP, DIC |
| Hemolytic-uremic syndrome (HUS) | Triad: hemolysis + renal failure + thrombocytopenia |
| Thrombotic thrombocytopenic purpura (TTP) | Pentad: above + fever + neurological changes |
| Paroxysmal nocturnal hemoglobinuria (PNH) | Dark morning urine, venous thrombosis, cytopenias |
| Malaria | Travel history, fever spikes, Plasmodium in blood smear |
| Babesiosis | Tick exposure, similar to malaria |
B. Ineffective Erythropoiesis
- Megaloblastic anemia (B12 or folate deficiency) - red cell precursors destroyed in bone marrow before reaching circulation
- Myelodysplastic syndrome (MDS)
- Indirect bilirubin elevated because abnormal red cells are destroyed before release
C. Increased Bilirubin Load (not hemolysis)
- Massive blood transfusion - transfused cells break down rapidly
- Resorption of a large hematoma - breakdown of red cells from internal bleeding releases bilirubin
- Rhabdomyolysis - muscle breakdown releases myoglobin and can indirectly raise bilirubin
Category 2 - HEPATIC Causes (Both fractions elevated)
| Cause | Key Clues |
|---|---|
| Drug-induced liver injury (DILI) | Any new medication in past 3-6 months; paracetamol/acetaminophen overdose is #1 in the West |
| Alcoholic hepatitis | Heavy alcohol use, AST:ALT ratio >2:1, tender liver |
| Autoimmune hepatitis | Young to middle-aged women, positive ANA/SMA/anti-LKM antibodies |
| Wilson's disease | Age <40 years, neuropsychiatric symptoms, Kayser-Fleischer rings in eyes, low ceruloplasmin |
| Non-alcoholic fatty liver disease (NAFLD) | Obesity, diabetes, metabolic syndrome |
| Ischemic hepatitis ("shock liver") | Recent hypotension, heart failure, or cardiac arrest; very high AST/ALT (>1000) |
| Budd-Chiari syndrome | Hepatic vein thrombosis; right upper quadrant pain, ascites, hypercoagulable states |
| Leptospirosis | Animal/water exposure, fever, muscle pain, renal failure (Weil's disease) |
| Dengue fever | Tropics, mosquito bite, thrombocytopenia, rash |
- Rifampicin, probenecid, atazanavir (HIV drug)
- Some cephalosporins and penicillins
Category 3 - POSTHEPATIC (Obstructive/Cholestatic) Causes
| Cause | Key Clues |
|---|---|
| Choledocholithiasis (gallstone in bile duct) | Colicky right upper quadrant pain, fever, Charcot's triad (pain + fever + jaundice) |
| Pancreatic cancer | Painless jaundice (classic), weight loss, elderly, Courvoisier's sign (palpable non-tender gallbladder) |
| Cholangiocarcinoma | Bile duct cancer; weight loss, itching, elevated CA 19-9 |
| Primary sclerosing cholangitis (PSC) | Often with inflammatory bowel disease; beaded bile ducts on MRCP |
| Primary biliary cholangitis (PBC) | Middle-aged women, intense pruritus, positive anti-mitochondrial antibodies (AMA) |
| Pancreatitis | Upper abdominal pain radiating to back, elevated lipase/amylase |
| Ampullary carcinoma | Cancer at head of pancreas/Ampulla of Vater |
Category 4 - GENETIC/INHERITED Conditions (Isolated bilirubin elevation, no liver damage)
| Condition | Fraction Elevated | Bilirubin Level | Notes |
|---|---|---|---|
| Gilbert's syndrome | Indirect only | Usually <6 mg/dL | Very common (3-7% of population); worsens with fasting, stress, illness |
| Crigler-Najjar type I | Indirect only | >20 mg/dL | Severe; neonates; absent glucuronyl transferase; often fatal |
| Crigler-Najjar type II | Indirect only | 6-25 mg/dL | Milder; adults can survive; treated with phenobarbital |
| Dubin-Johnson syndrome | Direct only | Mild | Benign; asymptomatic; defect in MRP2 transporter |
| Rotor syndrome | Direct only | Mild | Benign; defect in OATP1B1/1B3 transporters |
How to Work It Out Systematically
| Test | What It Tells You |
|---|---|
| ALT, AST | High = hepatocellular injury |
| Alkaline phosphatase (ALP) | High = cholestatic/obstructive cause |
| Albumin + prothrombin time (PT/INR) | Low albumin = chronic disease; prolonged PT = severe liver dysfunction |
| Peripheral blood smear | Schistocytes (MAHA/TTP), spherocytes, sickle cells, malaria parasites |
| Reticulocyte count | High = hemolysis or blood loss |
| LDH + haptoglobin | LDH high + haptoglobin low = hemolysis |
| Coombs test (DAT) | Positive = autoimmune hemolysis |
| Ceruloplasmin (if <40 years) | Low = Wilson's disease |
| ANA, SMA, anti-LKM | Positive = autoimmune hepatitis |
| Abdominal ultrasound | Dilated bile ducts = obstruction; gallstones; liver texture |
| MRCP or CT abdomen | Detailed biliary and pancreatic imaging if ultrasound inconclusive |
Bottom Line
- Hemolytic crisis (sickle cell, G6PD, AIHA, TTP/HUS) - most likely cause of very high indirect bilirubin
- Drug-induced liver injury - if ALT/AST are elevated
- Obstructive jaundice (gallstone, pancreatic mass) - if ALP is elevated
- Wilson's disease - if patient is under 40 with neuropsychiatric symptoms
- Crigler-Najjar type II - if all other tests are completely normal
- Harrison's Principles of Internal Medicine 22E, Chapter 52 - Evaluation of Jaundice
Autoimmune hepatitis in young women
autoimmune hepatitis young women diagnosis treatment
Autoimmune Hepatitis (AIH) in Young Women
What Is It?
"A chronic, progressive disorder with features that include a genetic predisposition, an association with other autoimmune diseases, the presence of autoantibodies, and therapeutic responsiveness to immunosuppression."
Why Young Women?
- HLA haplotypes DR3 and DR4 - genetic predisposition
- 40% of patients have a family history of autoimmune disease
- 20% have or will develop another autoimmune disease (e.g. thyroiditis, rheumatoid arthritis, celiac disease, ulcerative colitis)
- The immune system of young women is inherently more reactive - same reason most autoimmune diseases (lupus, thyroiditis, MS) predominantly affect women
Types of AIH
| Feature | Type 1 | Type 2 |
|---|---|---|
| Who | Young-middle aged women; most common in North America | Children and teenagers; up to 20% adults |
| Key antibodies | ANA (67%) + Anti-smooth muscle antibody/ASMA (87%) + Anti-SLA/LP (25-35%) | Anti-LKM-1 (cytochrome P450 2D6) + Anti-LC-1 + Anti-SLA/LP |
| Frequency | Most common (>80% of cases) | Less common; more aggressive in children |
| Severity | Variable | Often more severe in children |
Symptoms - What the Patient Feels
Common Symptoms
- Progressive fatigue - often the first and most prominent symptom
- Jaundice - relapsing and remitting yellow discoloration of skin/eyes
- Amenorrhea (absent periods) - a classic and distinctive sign in young women; the chronic inflammation disrupts the hypothalamic-pituitary-gonadal axis
- Infertility - closely linked to amenorrhea
- Arthralgia (joint pains) - migratory, non-destructive
- Anorexia, nausea, abdominal pain
- Weight loss
Silent Disease (25% of cases)
- Completely asymptomatic - discovered only when routine blood tests show elevated liver enzymes (ALT/AST)
Severe Presentation (rare but important)
- Acute liver failure - AIH can present as fulminant hepatitis indistinguishable from viral hepatitis
- Up to 40% 6-month mortality if untreated
Physical Signs on Examination
| Sign | What It Means |
|---|---|
| Jaundice + scleral icterus | Active hepatitis |
| Hepatomegaly | Enlarged, often tender liver |
| Splenomegaly | Portal hypertension - suggests cirrhosis may be developing |
| Spider nevi | Dilated capillaries on skin (neck, chest, face) - sign of chronic liver disease |
| Palmar erythema | Red palms - chronic liver disease |
| Cushingoid features | If already on steroid treatment |
| Caput medusae | Distended abdominal veins - late sign of portal hypertension |
| Ascites | If cirrhosis has developed |
Laboratory Findings
| Test | Finding in AIH |
|---|---|
| ALT, AST | Elevated (often 5-50x normal) |
| Bilirubin | Elevated in active disease |
| Alkaline phosphatase | Usually normal or mildly raised (unlike biliary diseases) |
| Albumin | Low in advanced disease |
| IgG (immunoglobulin G) | Markedly elevated - a hallmark sign; often 2x upper limit of normal |
| ANA | Positive (titre ≥1:40) in Type 1 |
| Anti-SMA (ASMA) | Positive in Type 1 - more specific than ANA |
| Anti-LKM-1 | Positive in Type 2 |
| Anti-SLA/LP | Highly specific for AIH (present in both Type 1 and 2) |
| INR/PT | Prolonged if significant liver dysfunction |
Histology (Liver Biopsy) - The Gold Standard
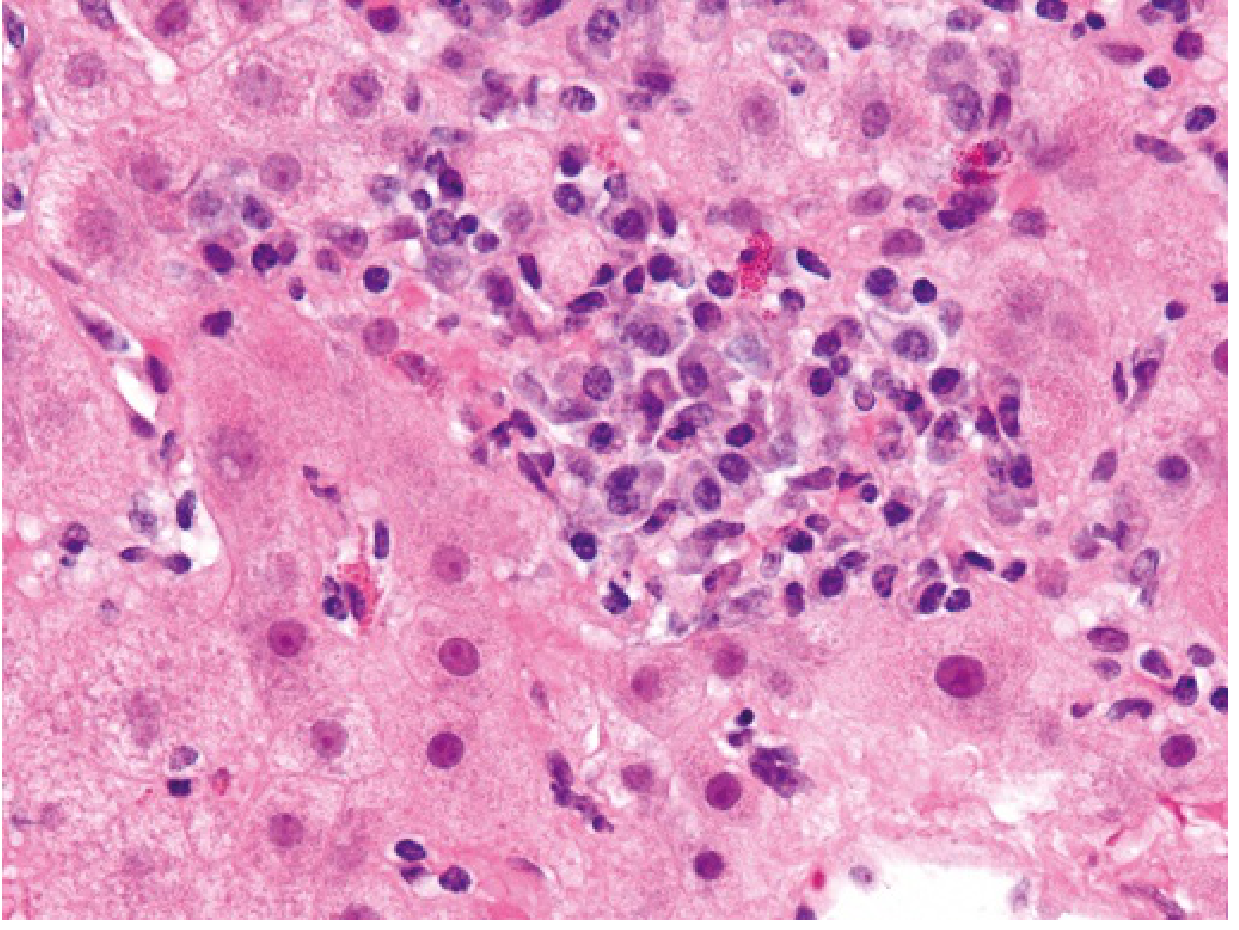
- Interface hepatitis - inflammation at the border of portal tract and liver parenchyma; lymphocytes and plasma cells invade and destroy hepatocytes
- Plasma cell predominance - plasma cells (antibody-producing immune cells) dominate the inflammatory infiltrate - highly characteristic
- Hepatocyte "rosettes" - circular arrangement of regenerating hepatocytes around a dilated canaliculus
- Bridging/confluent necrosis - in severe cases, bands of necrosis connecting portal tracts
- Cirrhosis in late stage - up to 30% already have cirrhosis at diagnosis
How Is It Diagnosed? (Simplified Scoring System)
| Criterion | Points |
|---|---|
| Female sex | +2 |
| Elevated IgG (>1.1x upper limit) | +1 to +2 |
| ANA or SMA titre ≥1:40 | +1 |
| ANA or SMA titre ≥1:80 | +2 |
| Anti-LKM-1 positive | +2 |
| Compatible liver histology | +1 |
| Typical histology | +2 |
| Viral hepatitis excluded | +2 |
Treatment
First-Line Treatment
- Starting dose: Prednisolone 40-60 mg/day, tapered gradually
- Azathioprine 50-150 mg/day added to allow steroid dose reduction
- Budesonide (a topical corticosteroid) can be used instead of prednisolone in non-cirrhotic patients - less systemic side effects
- Remission in ~80-90% of patients
Response Timeline
- Symptoms improve first (weeks)
- Lab values normalize (months - usually 12-24 months)
- Histological resolution takes longest (3-6 months after lab remission)
Sustained remission:
- 80% maintain remission off treatment if histology is normal after therapy
- But 50% relapse within 6 months of stopping treatment if liver biopsy still shows inflammation
Second-Line (if steroids fail or intolerable side effects)
- Mycophenolate mofetil (MMF)
- Cyclosporine
- Tacrolimus
Liver Transplant
- For decompensated end-stage disease or fulminant AIH
- 10-year survival post-transplant: 75%
- Recurrence in transplanted liver: 20% of cases
- Requires lifelong immunosuppression post-transplant
Special Consideration: AIH in Pregnancy
- Amenorrhea resolves with successful treatment - fertility returns
- Azathioprine is safe in pregnancy - should NOT be stopped
- 33% of patients experience a disease flare after delivery (postpartum flare)
- Risks include: preterm birth, fetal growth restriction
- Women with well-controlled AIH can have successful pregnancies
- Women with cirrhosis have higher complication rates
Prognosis
| Scenario | Outlook |
|---|---|
| Treated early, no cirrhosis | Excellent - near-normal life expectancy |
| Cirrhosis present at diagnosis | Good if treated - remission still achievable in 90% |
| Untreated | Poor - 40% mortality within 6 months in severe cases |
| Post-liver transplant | 10-year survival 75%; recurrence 20% |
Summary: The Classic Young Woman with AIH
A woman in her 20s-30s presenting with fatigue, relapsing jaundice, absent periods, and joint pains. Blood tests show elevated ALT/AST, very high IgG, positive ANA and anti-SMA. Viral hepatitis screen is negative. Liver biopsy shows interface hepatitis with plasma cell predominance. She responds dramatically to prednisolone + azathioprine.
- Robbins & Kumar Basic Pathology, Autoimmune Hepatitis section
- Henry's Clinical Diagnosis and Management by Laboratory Methods, Chapter 55
- Tietz Textbook of Laboratory Medicine 7th Ed, p. 2007
- Creasy & Resnik's Maternal-Fetal Medicine, Autoimmune Hepatitis in Pregnancy
- 2025 British Society of Gastroenterology Guidelines for AIH (PMID 40169244 - most current guidelines)
Can drug induced liver injury happen if a patient is having antibiotics for sinusitis
antibiotic drug-induced liver injury DILI sinusitis
Can Antibiotics for Sinusitis Cause Drug-Induced Liver Injury?
The Key Fact
"Currently, the most common agent implicated as causing DILI in the United States and in Europe is amoxicillin-clavulanate (most frequent brand name: Augmentin)."
Which Sinusitis Antibiotics Can Cause DILI?
| Antibiotic | Used For | Liver Injury Type | Risk Level |
|---|---|---|---|
| Amoxicillin-clavulanate (Augmentin) | Sinusitis, chest infections | Mixed hepatocellular + cholestatic (most common) | Highest among antibiotics |
| Ciprofloxacin | Resistant/severe sinusitis | Hepatocellular - looks like viral hepatitis | Moderate |
| Levofloxacin | Severe sinusitis | Cholestatic - can cause vanishing bile duct syndrome | Moderate |
| Trimethoprim-sulfamethoxazole (Co-trimoxazole) | Sinusitis alternative | Hepatocellular + hypersensitivity (fever, rash, eosinophilia) | Moderate |
| Azithromycin/erythromycin | Atypical infections | Cholestatic | Low-moderate |
| Doxycycline/minocycline | Atypical sinusitis | Can mimic autoimmune hepatitis | Low but insidious |
| Nitrofurantoin | UTI (not sinusitis, but similar antibiotic class concern) | Chronic hepatitis mimicking autoimmune hepatitis | Notable |
How Amoxicillin-Clavulanate Causes Liver Injury
- Unpredictable - cannot be predicted from blood tests before starting the drug
- Not dose-dependent in the traditional sense
- Rare (affects roughly 1 in 2,500 to 1 in 100,000 users)
- Not the patient's fault - it is an individual immune system response
- The clavulanate component (added to protect amoxicillin from bacterial resistance) appears to potentiate the liver toxicity
- Amoxicillin alone is much less toxic - clavulanate somehow sensitizes the liver
- The liver injury is thought to be immune-mediated - certain HLA haplotypes (HLA-DRB1) are strongly associated with susceptibility
- The liver damage affects both hepatocytes AND bile ducts - hence "mixed" pattern
What Makes This Tricky - The Delayed Onset
"Because hepatotoxicity may follow amoxicillin-clavulanate therapy after a relatively long latency period, the liver injury may begin to manifest after the drug has been withdrawn."
- Patient takes a 7-10 day course of Augmentin for sinusitis
- They finish the course and feel better from the sinus infection
- 1 to 6 weeks later they develop jaundice, fatigue, and dark urine
- By this time, many doctors - and patients - may not connect it to the antibiotic they finished weeks ago
Symptoms of Antibiotic-Induced DILI
- Fatigue and malaise - often the first sign
- Jaundice - yellow skin and eyes, may be prolonged
- Dark urine - tea-colored (conjugated bilirubin being excreted)
- Pale/clay-colored stools - bile not reaching the gut
- Pruritus (itching) - from bile salt deposition in skin; can be intense
- Nausea and anorexia
- Right upper quadrant discomfort
- Rash - uncommon with amoxicillin-clavulanate, but may occur with co-trimoxazole
- High fever
- Marked aminotransferase elevations (ALT/AST are high but usually <10x normal unless hepatocellular type)
The Vanishing Bile Duct Syndrome - A Serious Complication
"On occasion, amoxicillin-clavulanate, like other cholestatic hepatotoxic drugs, causes permanent injury to small bile ducts leading to the so-called 'vanishing bile duct syndrome.' Initially liver injury is minimal except for severe cholestasis; however, over time, histologic evidence of bile duct abnormalities is replaced by a paucity and eventual absence of discernible ducts."
Minocycline and Doxycycline - A Special Warning
"Nitrofurantoin may cause chronic hepatitis of varying severity but indistinguishable from autoimmune hepatitis... A similar disease pattern can be observed with minocycline, which is used repeatedly for the treatment of acne in teenagers."
What Doctors Should Do (And What Patients Should Know)
If a patient on antibiotics for sinusitis develops jaundice:
- Stop the antibiotic immediately - the most important step
- Tell the prescribing doctor about the antibiotic - even if it was finished weeks ago
- Do not re-prescribe the same antibiotic - re-exposure risks a faster, more severe reaction
- Test liver enzymes (ALT, AST), ALP, bilirubin, and INR
- Rule out viral hepatitis (usually negative)
- Most cases resolve spontaneously after stopping the drug (weeks to months)
- Monitor until liver tests normalize
Two Important Types of Injury Pattern
| Pattern | ALT/AST | ALP | Bilirubin | Most Common Cause |
|---|---|---|---|---|
| Hepatocellular | Very high (>5x) | Normal or mildly raised | Elevated | Ciprofloxacin, co-trimoxazole |
| Cholestatic | Mildly elevated | Very high (>2x) | Elevated + jaundice | Amoxicillin-clavulanate, levofloxacin |
| Mixed | Both elevated | Both elevated | Elevated | Amoxicillin-clavulanate |
Bottom Line
- Harrison's Principles of Internal Medicine 22E - Liver Injury Caused by Drugs, Amoxicillin-Clavulanate Hepatotoxicity section
- Goldman-Cecil Medicine - Drug-Induced Liver Injury, Epidemiology section
T a patient is having jaundice due to drug induced liver injury the conjugated bilirubin is 23 mg/dl and unconjugated bilirubin is 16 mg/dl what are the steps of treatment
drug-induced liver injury DILI management treatment guidelines
Treatment of DILI with Conjugated 23 mg/dL + Unconjugated 16 mg/dL = Total 39 mg/dL
Understanding This Pattern First
| Fraction | Value | % of Total | Pattern |
|---|---|---|---|
| Conjugated (direct) | 23 mg/dL | 59% | Dominant |
| Unconjugated (indirect) | 16 mg/dL | 41% | Elevated too |
| Total | 39 mg/dL | - | Mixed/cholestatic |
Step-by-Step Treatment Protocol
STEP 1 - STOP THE OFFENDING DRUG IMMEDIATELY (Most Critical Step)
"Other than stopping treatment with the offending drug, no specific treatments are usually recommended for idiosyncratic drug-induced liver injury."
- Identify and immediately discontinue the causative drug
- If the patient is on multiple medications, all suspected hepatotoxic agents must be stopped
- Do NOT re-challenge with the same drug - re-exposure causes faster and more severe injury
- Even drugs recently completed (within weeks) should be identified - amoxicillin-clavulanate can present after the course ends
STEP 2 - ASSESS SEVERITY AND RISK STRATIFY
| Test | Why |
|---|---|
| ALT, AST | Degree of hepatocellular injury |
| Alkaline phosphatase (ALP) | Degree of biliary injury - expected to be high in cholestatic DILI |
| INR / PT | If prolonged, indicates synthetic liver failure - danger sign |
| Serum albumin | Low = chronic or severe liver injury |
| Serum creatinine | Hepatorenal syndrome risk |
| Blood glucose | Hypoglycemia in liver failure |
| Serum ammonia | Encephalopathy risk |
| FBC / blood count | Look for eosinophilia (hypersensitivity reaction to drug) |
STEP 3 - DECIDE: INPATIENT OR OUTPATIENT?
- INR > 1.5
- Encephalopathy (confusion, drowsiness)
- Rising creatinine
- Hypoglycemia
- Rapid rise in bilirubin
- Normal INR
- Alert and oriented
- Normal renal function
- Stable or falling bilirubin after drug stopped
STEP 4 - SPECIFIC ANTIDOTE (If Applicable)
| Drug Cause | Specific Antidote |
|---|---|
| Acetaminophen (paracetamol) overdose | N-acetylcysteine (NAC) - 140 mg/kg IV loading dose, then 70 mg/kg every 4 hours - must be given early |
| Valproate toxicity | IV Carnitine - 100 mg/kg IV over 30 minutes (max 6g), then 15 mg/kg every 4 hours - for valproate-induced ammonia elevation |
| Leflunomide, cholestyramine-responsive drugs | Cholestyramine - 8g orally 3 times daily for 11 days - accelerates removal of lipophilic drugs with long half-lives |
| All other antibiotics/idiosyncratic DILI | No specific antidote - supportive care only |
STEP 5 - TREAT THE CHOLESTASIS AND PRURITUS
| Treatment | Dose | Purpose |
|---|---|---|
| Cholestyramine (bile acid resin) | 4-8g orally 2-3x/day | Binds bile salts in gut, reduces pruritus |
| Ursodeoxycholic acid (UDCA) | 10-15 mg/kg/day | Protects bile duct cells, promotes bile flow, reduces cholestasis |
| Rifampicin | 150-300 mg/day | Reduces pruritus by inducing bile acid metabolism (use cautiously - hepatotoxic itself) |
| Naltrexone | 25-50 mg/day | Opioid antagonist for severe pruritus |
| Antihistamines | Chlorphenamine etc. | Symptom relief for pruritus |
Note: Cholestyramine also helps remove the offending drug from enterohepatic circulation if it undergoes biliary excretion.
STEP 6 - CONSIDER CORTICOSTEROIDS (Selective Use)
"Corticosteroids (typically starting with the equivalent of 40 mg prednisone daily with subsequent titration and tapering according to the patient's response) are often administered if the drug-induced liver injury mimics autoimmune hepatitis OR if the liver injury is progressing towards liver failure, especially if clinical signs of hypersensitivity (fever, rash, and peripheral eosinophilia) are present."
- Liver injury is progressing despite stopping the drug
- Features of hypersensitivity: fever + rash + eosinophilia (seen with sulfonamides, phenytoin)
- DILI pattern mimics autoimmune hepatitis (positive ANA, anti-SMA)
- Minocycline or nitrofurantoin-induced hepatitis (commonly causes AIH pattern)
STEP 7 - SUPPORTIVE CARE
| Issue | Management |
|---|---|
| Nutrition | High-calorie diet; IV glucose if unable to eat |
| Hydration | IV fluids if dehydrated/vomiting |
| Avoid all hepatotoxic drugs | No paracetamol, no NSAIDs, no alcohol, no herbal remedies |
| Vitamin K | 10 mg IV if INR elevated (tests if prolonged PT is from malabsorption vs liver failure) |
| Fat-soluble vitamins | Deficiency in prolonged cholestasis (Vitamins A, D, E, K not absorbed without bile) |
| Encephalopathy management | Lactulose + low protein diet if ammonia rises |
| Antiemetics | Ondansetron for nausea |
| Rest | Reduce physical activity; avoid strenuous exercise |
STEP 8 - SERIAL MONITORING
- Bilirubin trend - should start falling after stopping drug (may take weeks)
- ALT/AST - should fall ≥50% within 30 days of stopping drug (positive prognostic sign per RUCAM scoring)
- INR - any rise signals worsening synthetic function
- Creatinine - watch for hepatorenal syndrome
- Patient mental status - any confusion = encephalopathy
- Wrong diagnosis (rule out biliary obstruction by ultrasound)
- Vanishing bile duct syndrome (liver biopsy)
- Progression to acute liver failure
STEP 9 - LIVER TRANSPLANT EVALUATION (If Deteriorating)
- Encephalopathy (Grade 2+)
- INR > 1.5 and rising
- Rising creatinine
- Hypoglycemia
- Refractory coagulopathy
STEP 10 - RECOVERY EXPECTATION
| Type | Recovery Timeline |
|---|---|
| Cholestatic DILI (like amoxicillin-clavulanate) | Bilirubin may stay elevated for weeks to months; full normalization can take 3-6 months |
| Hepatocellular DILI | Usually faster recovery - 4-8 weeks |
| Vanishing bile duct syndrome | Can cause permanent cholestasis; may need liver transplant |
| Uncomplicated cholestatic | ~95% make full recovery after drug stopped |
Summary Flowchart
DILI Confirmed (Conjugated 23 + Unconjugated 16 mg/dL)
│
├── STEP 1: STOP the drug → IMMEDIATELY
├── STEP 2: Assess severity → INR, ALT, creatinine, ammonia
├── STEP 3: Admit to hospital (bilirubin 39 mg/dL = severe)
├── STEP 4: Specific antidote? (NAC for paracetamol; carnitine for valproate)
├── STEP 5: Treat cholestasis → cholestyramine, UDCA for pruritus
├── STEP 6: Corticosteroids? → Only if hypersensitivity features or AIH-like
├── STEP 7: Supportive care → fluids, nutrition, vitamin K, avoid all hepatotoxins
├── STEP 8: Monitor weekly → bilirubin, INR, ALT, creatinine
└── STEP 9: Transplant referral if worsening despite drug withdrawal
- Goldman-Cecil Medicine International Edition - Drug-Induced Liver Injury, Treatment section (p. 1593)
- Harrison's Principles of Internal Medicine 22E - Liver Injury Caused by Drugs
- 2024 Chinese Guidelines for Diagnosis and Treatment of DILI (PMID 38402364 - most current international practice guideline)