circulatory system from grays full chapter
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Nervous system from grays full chapter
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from the Nervous System chapter of Gray's Anatomy for Students. Here is the full chapter presentation:
Nervous System - Gray's Anatomy for Students
- Gray's Anatomy for Students, Chapter 1 (The Body) & Chapter 2 (Back)
Overview and Structural Divisions
The nervous system is divided two ways:
Structurally:
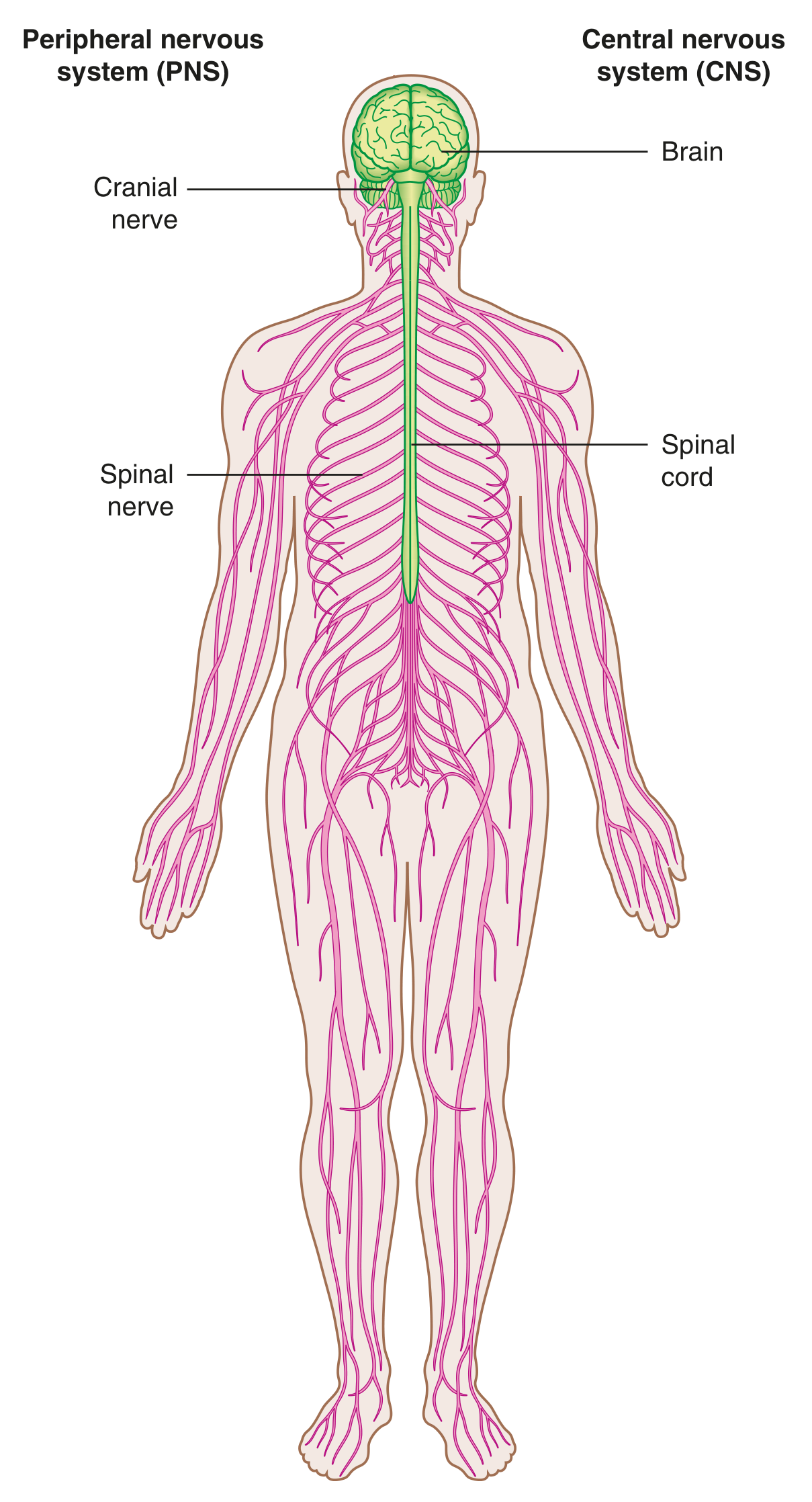
- Central Nervous System (CNS) - brain and spinal cord (both develop from the neural tube)
- Peripheral Nervous System (PNS) - all nervous structures outside the CNS; connects CNS to the body; develops from neural crest cells and outgrowths of the CNS. Includes spinal nerves, cranial nerves, visceral nerves and plexuses, and the enteric system.
Functionally:
- Somatic part - innervates skin and skeletal muscle (structures from somites); concerned with the external environment
- Visceral part - innervates organ systems, smooth muscle, and glands; concerned with the internal environment
Central Nervous System
Brain
The brain has three major parts:
- Cerebral hemispheres - outer gray matter (cell bodies), inner white matter (axonal tracts/pathways), and ventricles (CSF-filled spaces)
- Cerebellum - two lateral lobes plus a midline portion
- Brainstem - classically includes the diencephalon, midbrain, pons, and medulla; in common usage "brainstem" usually refers to midbrain, pons, and medulla only
Spinal Cord
The spinal cord occupies the superior two-thirds of the vertebral canal. It is roughly cylindrical with a central canal and is circular to oval in cross-section. It runs within a bony canal formed by aligned vertebral arches (the vertebral canal), from the first cervical vertebra (CI) to the last sacral vertebra (SV). The canal also contains blood vessels, connective tissue, fat, and proximal spinal nerve roots.
Meninges
Three connective tissue coverings surround and protect the brain and spinal cord:
| Layer | Position | Character |
|---|---|---|
| Dura mater | Outermost | Thickest layer |
| Arachnoid mater | Against inner surface of dura | Intermediate |
| Pia mater | Adherent to brain/spinal cord surface | Innermost |
The subarachnoid space lies between the arachnoid and pia mater and contains cerebrospinal fluid (CSF).
Functional Subdivisions of the CNS
The CNS functionally divides into somatic and visceral parts. The somatic part innervates skin and most skeletal muscle; the visceral part innervates organ systems, smooth muscle, and glands in peripheral regions.
Somatic Part of the Nervous System
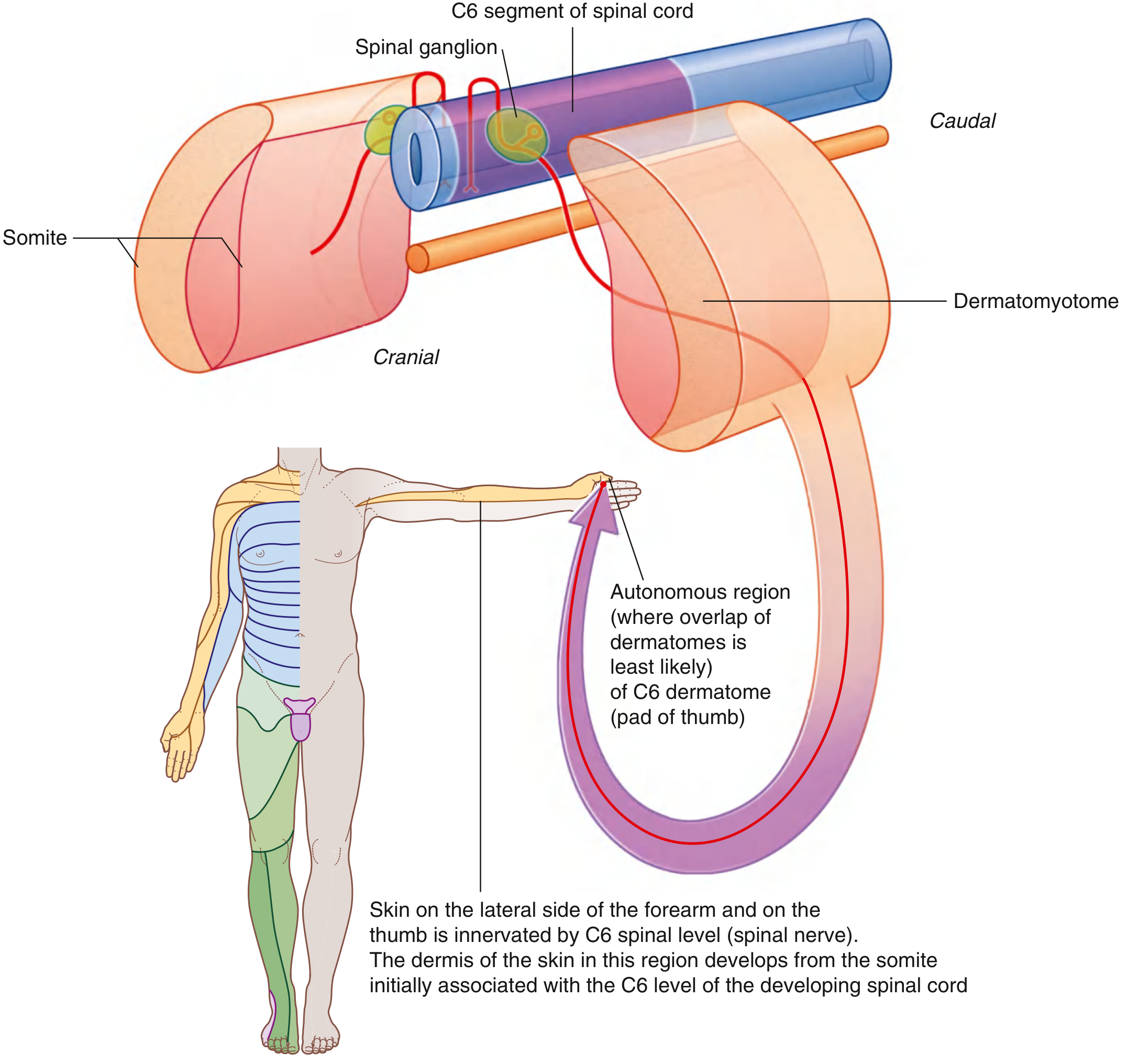
Somatic nerves arise segmentally along the developing CNS in association with somites - blocks of paraxial mesoderm arranged segmentally on each side of the neural tube.
Part of each somite (the dermatomyotome) gives rise to skeletal muscle and dermis of the skin. Cells migrate:
- Anteriorly - form muscles of limbs and trunk (hypaxial muscles) and associated dermis
- Posteriorly - form intrinsic back muscles (epaxial muscles) and associated dermis
Neural crest cells differentiate into sensory neurons, extending:
- Medial processes into the posterior spinal cord
- Lateral processes into the differentiating dermatomyotome
Neurons within the spinal cord are motor neurons; those from neural crest cells are sensory neurons.
Somatic Sensory Fibers (Somatic Afferents / GSAs)
Carry conscious sensory information from peripheral body regions to the CNS. These fibers can be very long, extending from peripheral sensory receptors to the dorsal horn of the spinal cord. Sensory neuron cell bodies form sensory ganglia (clusters of sensory nerve cell bodies located outside the CNS).
Somatic Motor Fibers (Somatic Efferents / GSEs)
Carry information from the CNS to skeletal muscles. Cell bodies sit in the spinal cord, and their axons extend to the muscle cells they innervate.
Dermatomes
Because somite-derived dermis occupies a precise location, somatic sensory fibers from that somite enter the posterior spinal cord at a specific level and become part of one spinal nerve.
A dermatome = the area of skin supplied by a single spinal cord level (or by a single spinal nerve on one side).
There is overlap between adjacent dermatomes. However, each dermatome has an autonomous zone - a region least likely to have overlap - which can be tested clinically to localize spinal cord or nerve lesions.
Myotomes
Somatic motor nerves from a specific somite emerge at the corresponding anterior spinal cord level and travel in the same spinal nerve as the sensory fibers from that level.
A myotome = the portion of skeletal muscle innervated by a single spinal cord level (or by a single spinal nerve on one side).
Myotomes are harder to test clinically because most skeletal muscles develop from more than one somite and are therefore innervated by more than one spinal cord level. Key clinical examples:
| Movement | Primary spinal levels |
|---|---|
| Shoulder joint muscles | C5, C6 |
| Elbow muscles | C6, C7 |
| Hand muscles | C8, T1 |
Visceral Part of the Nervous System
The visceral nervous system has both motor and sensory components:
- Sensory - monitors changes in viscera
- Motor - regulates activities of the viscera (smooth muscle, cardiac muscle, glandular epithelium)
The visceral motor component is the autonomic nervous system (ANS), which has two parts:
| Feature | Sympathetic | Parasympathetic |
|---|---|---|
| Origin | Thoracolumbar cord (T1-L2) | Brainstem (CN III, VII, IX, X) and sacral cord (S2-S4) |
| Ganglion location | Paravertebral chain or prevertebral | In or near the target organ wall |
| Distribution | Peripheral regions AND viscera | Viscera only |
| "Fight or flight" | Yes | No (rest and digest) |
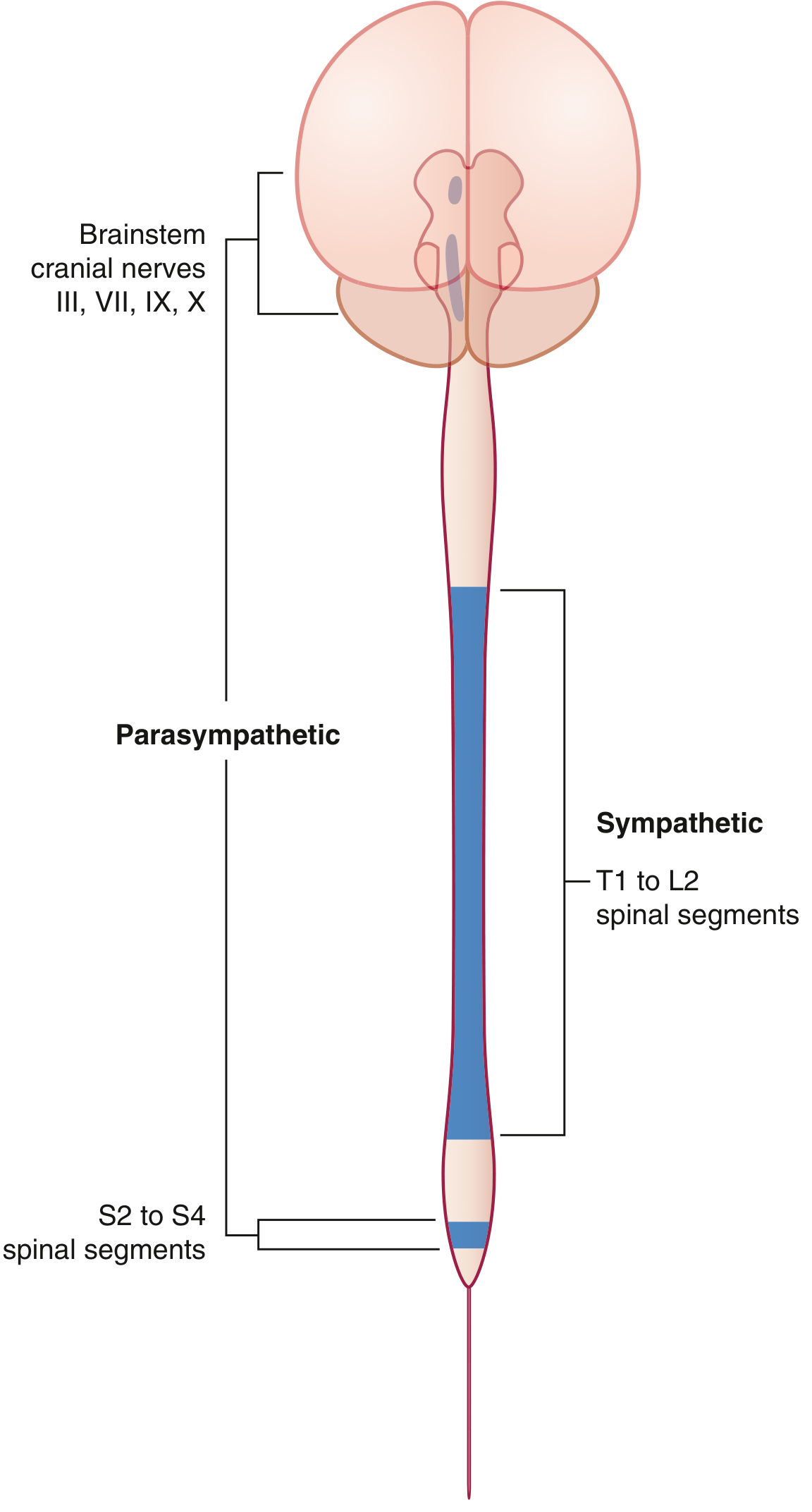
Sympathetic System
The sympathetic division leaves the thoracolumbar spinal cord (T1-L2) with somatic components of those spinal nerves.
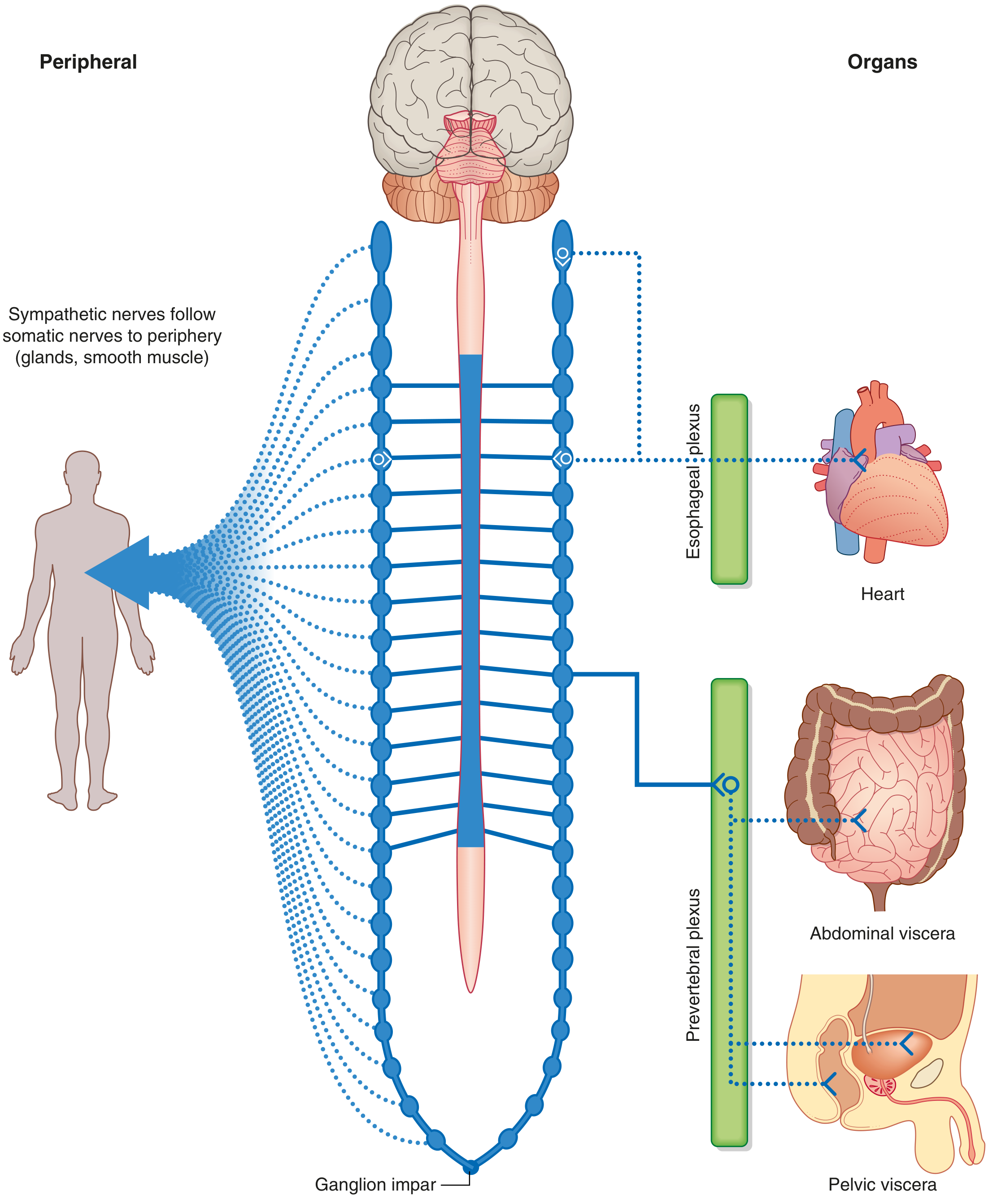
On each side, a paravertebral sympathetic trunk extends from the base of the skull to the coccyx, where both trunks converge at the ganglion impar. The trunks are anterior to the anterior rami and connect to them.
Pathway of preganglionic sympathetic fibers:
- Leave the spinal cord in anterior roots from T1-L2
- Enter spinal nerves, pass through anterior rami
- Enter the sympathetic trunk via white rami communicantes (myelinated, appear white)
From there, preganglionic fibers take one of four pathways:
- Synapse in the paravertebral ganglion at the same level - postganglionic fibers return to the anterior ramus via gray rami communicantes (unmyelinated), distributed to periphery in spinal nerves (to sweat glands, arrector pili muscles, blood vessel smooth muscle)
- Ascend in the trunk to synapse at a higher ganglion (serving cervical and upper thoracic regions)
- Descend in the trunk to synapse at a lower ganglion (serving lumbar and sacral regions)
- Pass through the trunk without synapsing - form splanchnic nerves that travel to prevertebral ganglia (celiac, superior mesenteric, etc.) to synapse there, with postganglionic fibers then distributed to abdominal and pelvic viscera
Parasympathetic System
Parasympathetic preganglionic fibers originate from two regions:
1. Brainstem (cranial outflow - CN III, VII, IX, X):
- CN III, VII, IX - preganglionic fibers synapse in one of four ganglia near branches of CN V; postganglionic fibers travel with CN V branches to: salivary glands, mucous glands, lacrimal gland, pupillary constrictor, ciliary muscle
- Vagus nerve [X] - most extensive parasympathetic nerve; provides visceral branches to plexuses of thoracic and abdominal viscera (heart, lungs, GI tract to the mid-colon)
2. Sacral cord (S2-S4):
- Preganglionic fibers form pelvic splanchnic nerves, entering pelvic extensions of the prevertebral plexus
- Distributed to pelvic and abdominal viscera mainly along blood vessels
- Postganglionic neurons sit in the walls of the target organs
- Targets include inferior abdominal viscera, pelvic viscera, and erectile tissue arteries
Both sympathetic and parasympathetic pathways use a two-neuron chain: preganglionic (CNS) → synapse in ganglion → postganglionic → target organ.
Exception: In the gastrointestinal tract, parasympathetic preganglionic fibers synapse directly on neurons of the enteric system (no separate postganglionic parasympathetic neuron in the pathway).
Visceral Sensory Innervation (Visceral Afferents)
Visceral sensory fibers generally travel alongside visceral motor fibers.
Fibers accompanying sympathetic fibers:
- Enter the spinal cord at similar levels to the motor output, though may enter at higher or lower levels (e.g., cardiac pain fibers can enter above T1)
- Primarily detect pain
Fibers accompanying parasympathetic fibers (CN IX, X, and S2-S4):
- CN IX - chemoreceptors and baroreceptors in walls of major neck arteries; receptors in pharynx
- CN X - cervical viscera, thoracic vessels and viscera, abdominal viscera
- S2-S4 - pelvic viscera and distal colon
- These primarily relay information about normal physiological status and reflex activities
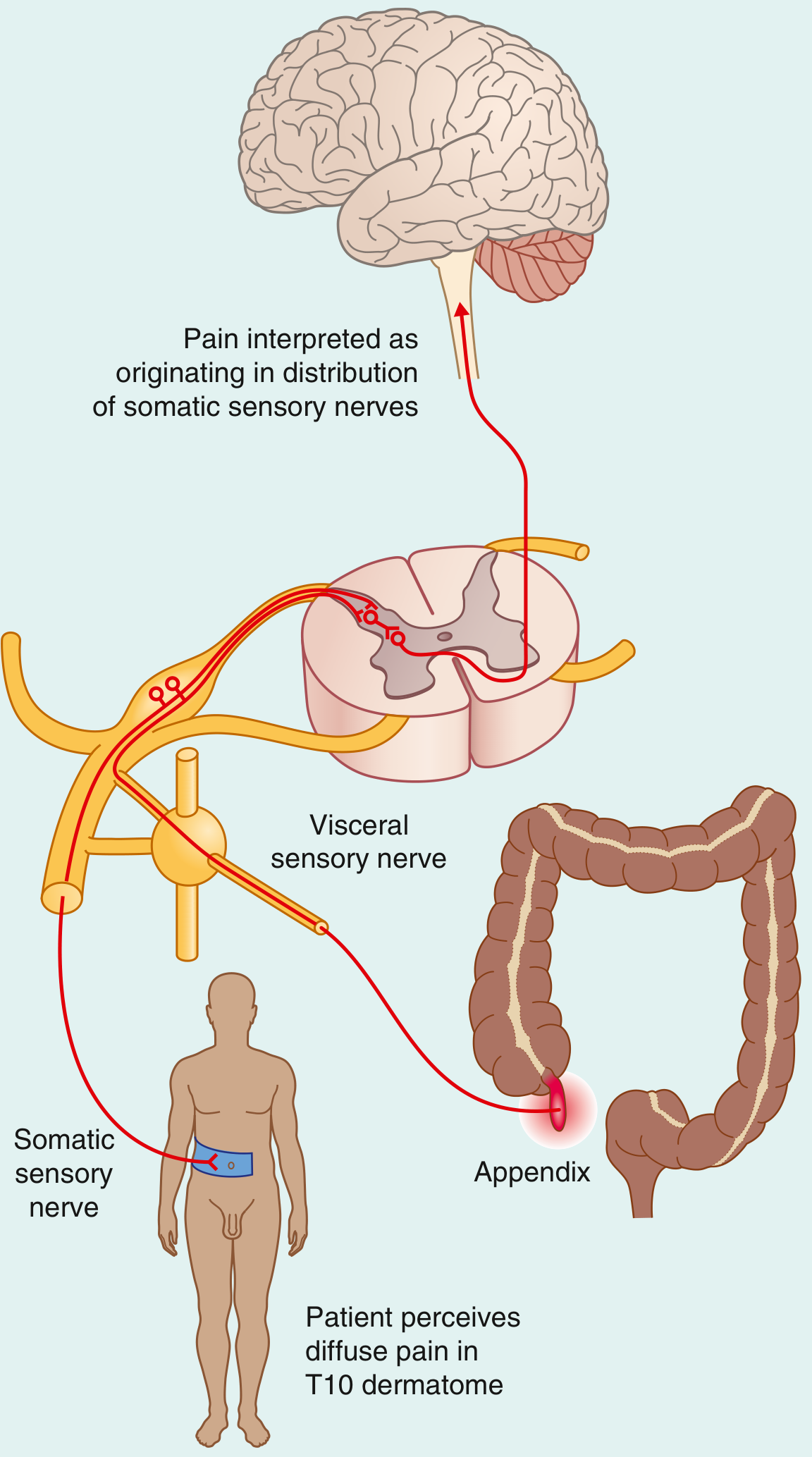
Referred Pain
Because visceral sensory pain fibers enter the spinal cord at the same level as somatic sensory fibers from specific dermatomes, the brain misinterprets visceral pain as coming from that dermatome (skin area) rather than from the organ itself.
Classic example - Appendicitis:
- Inflamed appendix stimulates visceral sensory fibers that enter at T10
- Pain is referred to the T10 dermatome (umbilical region)
- Pain is diffuse and colicky (each peristaltic wave triggers it)
- Later, when the appendix contacts the parietal peritoneum (innervated by somatic nerves), pain localizes to the right iliac fossa and becomes constant - this somatic pain overrides the referred visceral pain
The Enteric System
The enteric nervous system is a semi-independent division of the visceral nervous system located in the walls of the gastrointestinal tract. It contains:
- Collections of neurons in the walls of the GI tract
- Intrinsic circuits capable of regulating gut function independently of CNS input
- Connections with both sympathetic and parasympathetic fibers
Protection of the Nervous System
The CNS is protected by several layers:
- Bony encasement - skull (brain) and vertebral column (spinal cord)
- Meninges - three connective tissue layers (dura, arachnoid, pia)
- CSF - fills the subarachnoid space and central canal; acts as a hydraulic shock absorber
- Blood-brain barrier - tight junctions between CNS capillary endothelial cells restrict passage of many substances
The vertebral canal (formed by aligned vertebral arches from CI to SV) houses the spinal cord and its protective membranes. The canal also contains blood vessels, connective tissue, fat, and proximal spinal nerve roots.
Summary Table: Somatic vs. Visceral Nervous System
| Feature | Somatic | Visceral |
|---|---|---|
| Structures innervated | Skin, skeletal muscle | Smooth muscle, cardiac muscle, glands, viscera |
| Sensory concern | External environment | Internal environment |
| Motor control | Voluntary | Largely involuntary (ANS) |
| Motor pathway | Single neuron (CNS to effector) | Two neurons (pre- and postganglionic) |
| Pain perception | Well-localized | Diffuse, often referred |
| Motor subdivisions | - | Sympathetic (T1-L2) + Parasympathetic (cranial + S2-S4) |
Source: Gray's Anatomy for Students (ISBN 9780323934237), Chapter 1: The Body - Nervous System section (pp. 47-65)
circulatory system from general anatomy full chapter with diagrams
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Here is the full Circulatory System chapter from the THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System (ISBN 9781626237186), presented with all diagrams.
Circulatory System
THIEME Atlas of Anatomy: General Anatomy and Musculoskeletal System
Overview: The Cardiovascular System as an Organ System
The cardiovascular system is classified under the Viscera group of organ systems, alongside:
- Hemolymphatic system
- Endocrine system
- Respiratory system
- Digestive system
- Urinary system
- Reproductive system
The heart and blood vessels form a closed, pressurized circuit that delivers oxygen and nutrients to every tissue and removes metabolic waste products.
Section 1.6 - Early Embryonic Circulation and the Development of Major Blood Vessels
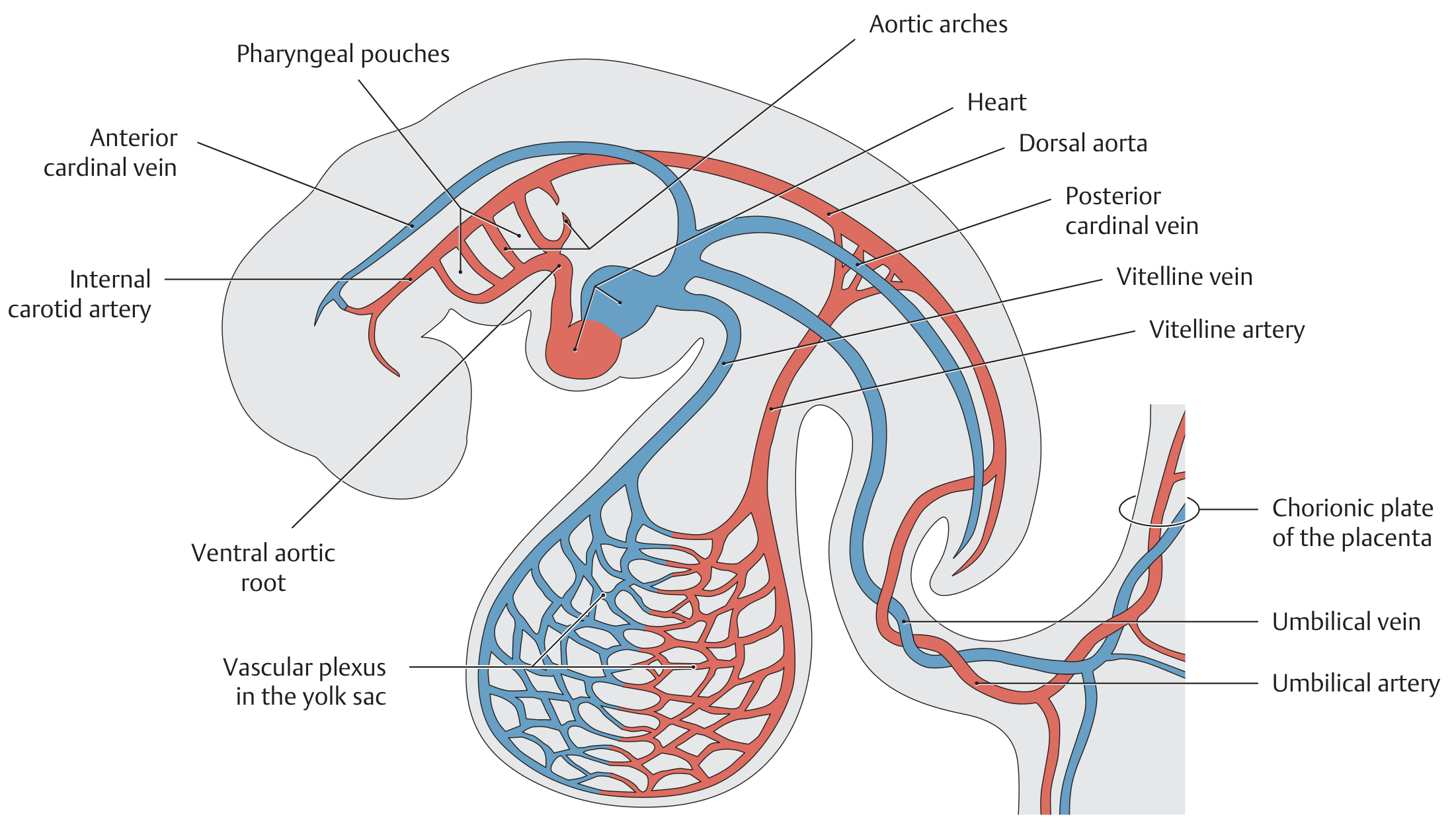
A. Circulatory System of a 3- to 4-Week-Old Human Embryo
The cardiovascular system is the first organ system to become functional in the embryo. By 3-4 weeks, a well-functioning two-chambered heart is already pumping blood through three distinct circulatory systems:
- Intraembryonic systemic circulation - ventral and dorsal aorta, branchial arch and aortic arches, anterior and posterior cardinal veins
- Extraembryonic vitelline circulation - omphalomesenteric arteries and veins (supplying the yolk sac)
- Placental circulation - umbilical arteries and veins (connecting to the placenta)
At this stage, the vascular pathways still show a largely symmetrical arrangement.
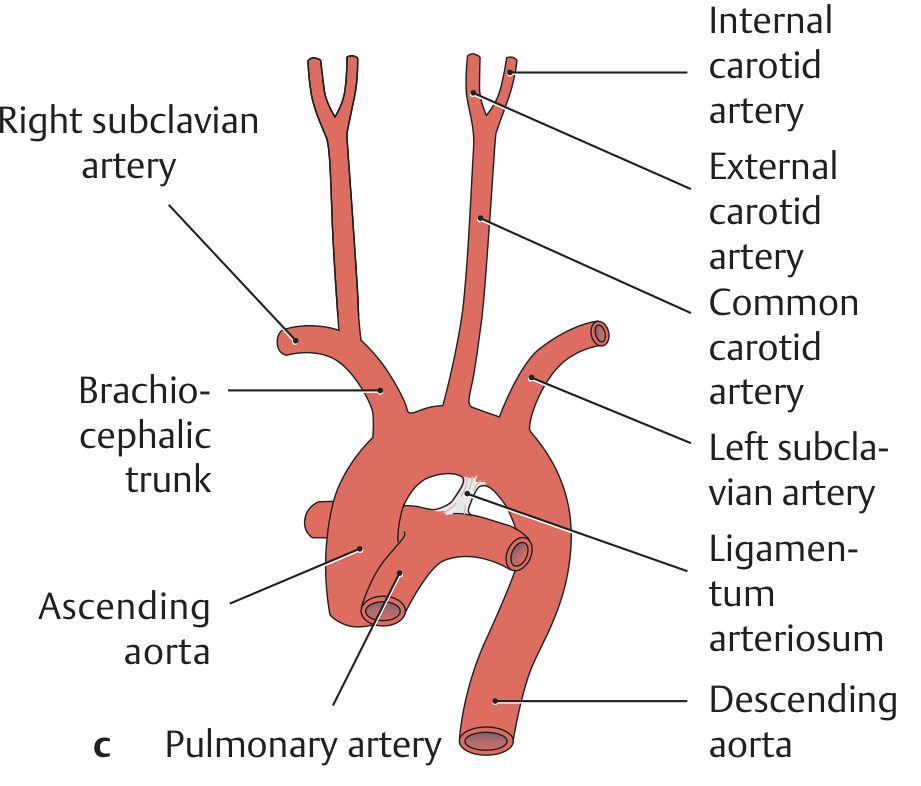
B. Development of the Arteries Derived from the Aortic Arch
a. Initial stage (4-week embryo, ventral view):
An artery develops in each pharyngeal arch, proceeding craniocaudally. These arteries arise from the paired ventral aortic roots, course through the mesenchyme of the pharyngeal arches, and open into the initially paired dorsal aorta. Six aortic arches form in sequence - they are not all present simultaneously (while the 4th arch is forming, the 1st two are already regressing). Development proceeds so that the original symmetry is lost in favor of a left-sided predominance.
b. Regression and persistence of aortic arches:
| Aortic Arch | Fate |
|---|---|
| 1st and 2nd arches | Regress on both sides |
| 3rd arch | Forms common carotid artery + proximal internal carotid artery (both sides) |
| 4th arch (left) | Becomes the definitive aortic arch |
| 4th arch (right) | Becomes the proximal right subclavian artery |
| 5th arch | Regresses on both sides |
| 6th arch | Forms the pulmonary artery trunk and the ductus arteriosus |
| 7th segmental artery | Forms the left subclavian artery |
c. Adult variants:
- Typical branching pattern (77%): brachiocephalic trunk + left common carotid + left subclavian arise separately from the arch
- Second most common (13%): left common carotid also arises from the brachiocephalic trunk
- Right-sided aortic arch: ~0.1%
- Duplicated aortic arch: ~0.1%
C. Development of the Cardinal Venous System (Weeks 5-7 to Birth)
Up until the 4th week, three paired venous trunks return blood to the heart: the vitelline, umbilical, and cardinal veins. The cardinal venous system at this stage has anterior, posterior, and common cardinal veins.
Between weeks 5 and 7, three additional cardinal systems form:
Supracardinal veins:
- Replace the posterior cardinal veins
- Receive blood from the intercostal veins
- Form the future azygos system (azygos and hemiazygos veins)
Subcardinal veins:
- Develop to drain the kidneys
- Right subcardinal vein → middle part of the inferior vena cava
- Transverse anastomosis → left renal vein
- Distal left subcardinal vein persists as a gonadal vein (testicular or left ovarian vein)
Sacrocardinal veins:
- Develop during formation of the lower limbs
- Transverse anastomosis → left common iliac vein
Key transverse anastomoses:
- Between anterior cardinal veins → future left brachiocephalic vein
- Right anterior + common cardinal veins → superior vena cava
- Left common cardinal vein → coronary sinus (venous drainage of the heart)
D. Development of the Vitelline and Umbilical Veins
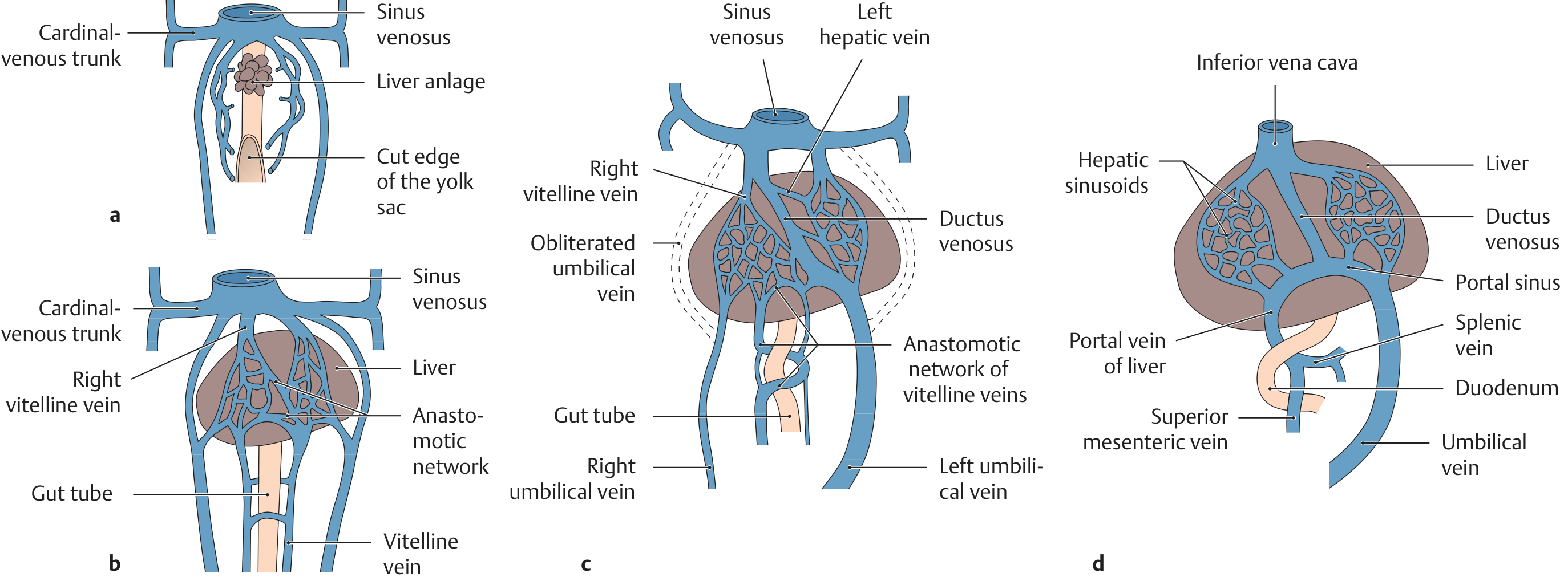
Key structures and their adult derivatives:
| Embryonic Structure | Adult Structure |
|---|---|
| Right umbilical vein | Regresses completely |
| Left umbilical vein | Ligamentum teres hepatis |
| Ductus venosus | Ligamentum venosum |
| Distal right vitelline vein | Portal vein |
| Proximal right vitelline vein | Posthepatic inferior vena cava |
Section 2.2 - Structural Organization: Body Cavities and the Heart
The heart is housed in the pericardial cavity - an enclosed serous cavity within the thorax. The pericardial cavity is lined by a serosa with two layers:
- Visceral layer (epicardium) - directly invests the heart
- Parietal layer - lines the outer wall of the pericardial sac
The thoracic cavity also contains the two pleural cavities (one per lung). The heart lies in the mediastinum, a connective-tissue space between the two pleural cavities.
Section 4.1 - The Arteries of the Lower Limb
Overview of Arterial Segments
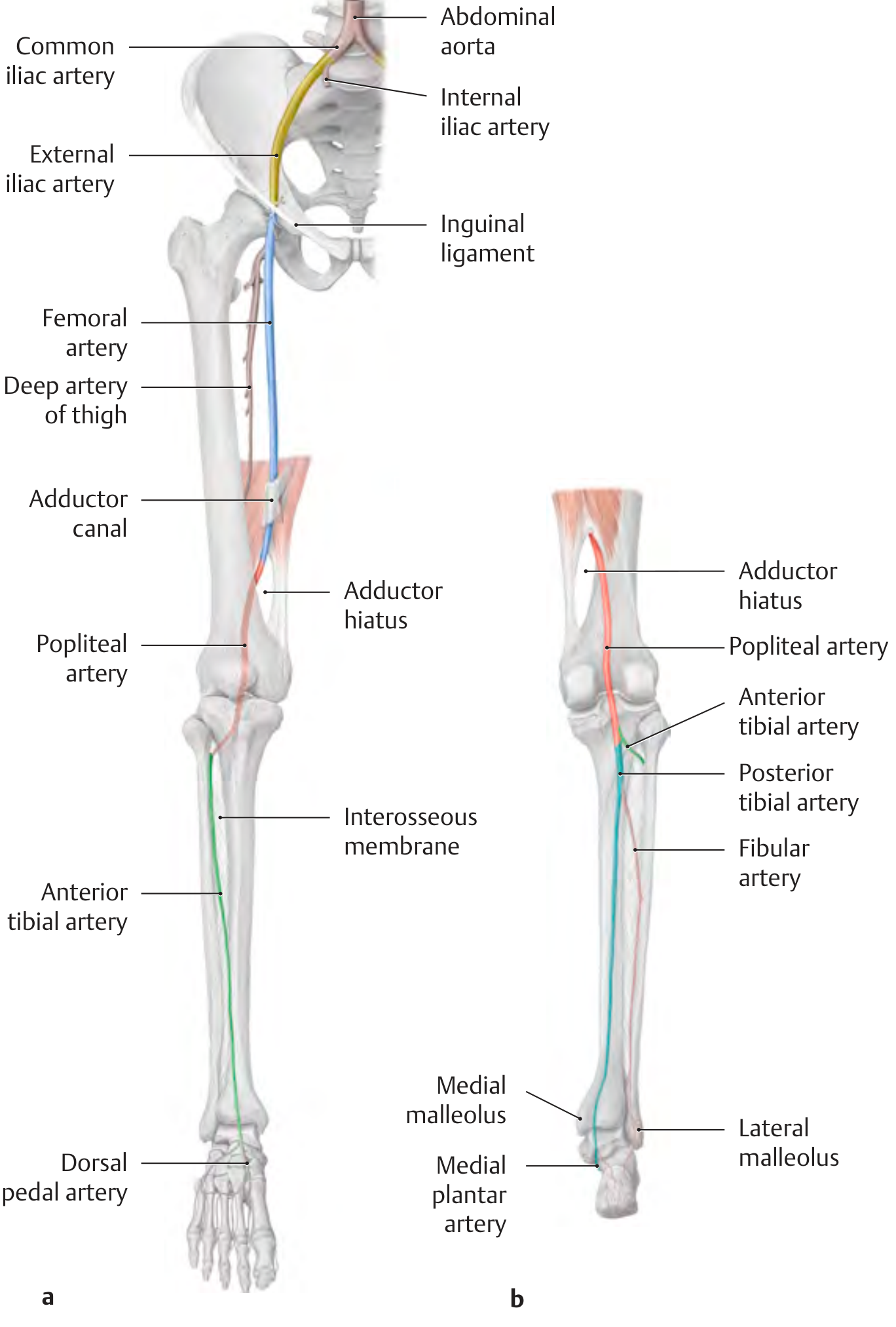
Arterial Segments in Detail
External iliac artery:
Arises with the internal iliac artery from the common iliac artery. Descends along the medial border of psoas major through the lacuna vasorum. Becomes the femoral artery at the level of the inguinal ligament.
Femoral artery:
Continuation of the external iliac artery. Runs down the medial thigh to the adductor canal, through which it passes from anterior to posterior. Exits through the adductor hiatus to become the popliteal artery.
Popliteal artery:
Runs from the adductor hiatus through the popliteal fossa to the popliteus muscle, dividing at the inferior border of popliteus into its terminal branches.
Anterior tibial artery:
Enters the extensor compartment at the upper border of the interosseous membrane. Descends between tibialis anterior and extensor hallucis longus. Continues distally as the dorsal pedal artery on the dorsum of the foot.
Posterior tibial artery:
Direct continuation of the popliteal artery. Enters the flexor compartment and passes behind the medial malleolus, dividing into medial and lateral plantar arteries. Also gives rise to the fibular artery.
Branch Summary Tables
Branches of the external iliac artery:
- Inferior epigastric artery
- Cremasteric artery
- Artery of the round ligament of the uterus
- Pubic branch
- Deep circumflex iliac artery
Branches of the femoral artery:
- Superficial epigastric artery
- Superficial circumflex iliac artery
- Superficial and deep external pudendal arteries
- Deep artery of the thigh (profunda femoris): medial/lateral circumflex femoral arteries + perforating branches
- Descending genicular artery
Branches of the popliteal artery:
- Posterior tibial recurrent artery
- Medial and lateral superior genicular arteries (form the arterial anastomotic network of the knee)
- Sural arteries
- Middle genicular artery
- Medial and lateral inferior genicular arteries
Branches of the anterior tibial artery:
- Anterior tibial recurrent artery
- Anterior lateral and medial malleolar arteries
- Dorsal pedal artery (with lateral tarsal, arcuate, dorsal metatarsal, and dorsal digital branches)
Branches of the posterior tibial artery:
- Fibular artery (with perforating branch and calcaneal branches)
- Medial plantar artery
- Lateral plantar artery (forms the plantar arch with the deep plantar artery)
Section 4.2 - The Veins of the Lower Limb
Overview: Three Venous Systems
The veins of the lower limb are subdivided into three interconnected systems:
| System | Location | % of venous return |
|---|---|---|
| Deep (intermuscular) | Below fascia | ~85% |
| Superficial (epifascial) | Above fascia | ~15% |
| Perforating | Pierce the fascia, connect the two systems | - |
The upright posture places an exceptional load on leg veins, which must work against gravity. Venous valves maintain normal superficial-to-deep direction of blood flow.
Deep Veins of the Lower Limb
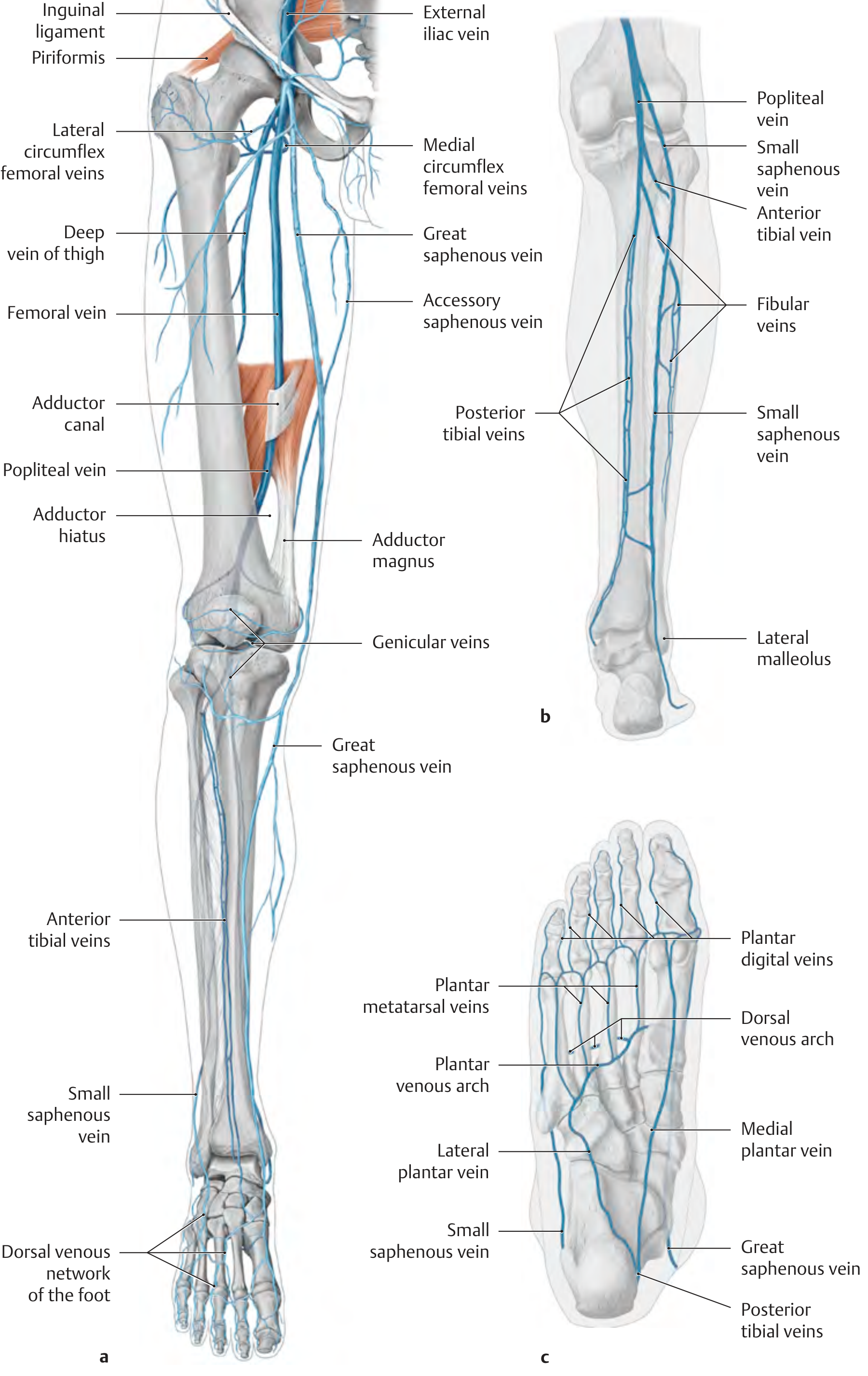
Principal deep veins:
- Femoral vein
- Deep vein of thigh
- Medial and lateral circumflex femoral veins
- Popliteal vein
- Sural veins and genicular veins
- Anterior and posterior tibial veins
- Fibular veins
- Dorsal and plantar metatarsal veins
- Plantar digital veins
Superficial Veins of the Lower Limb
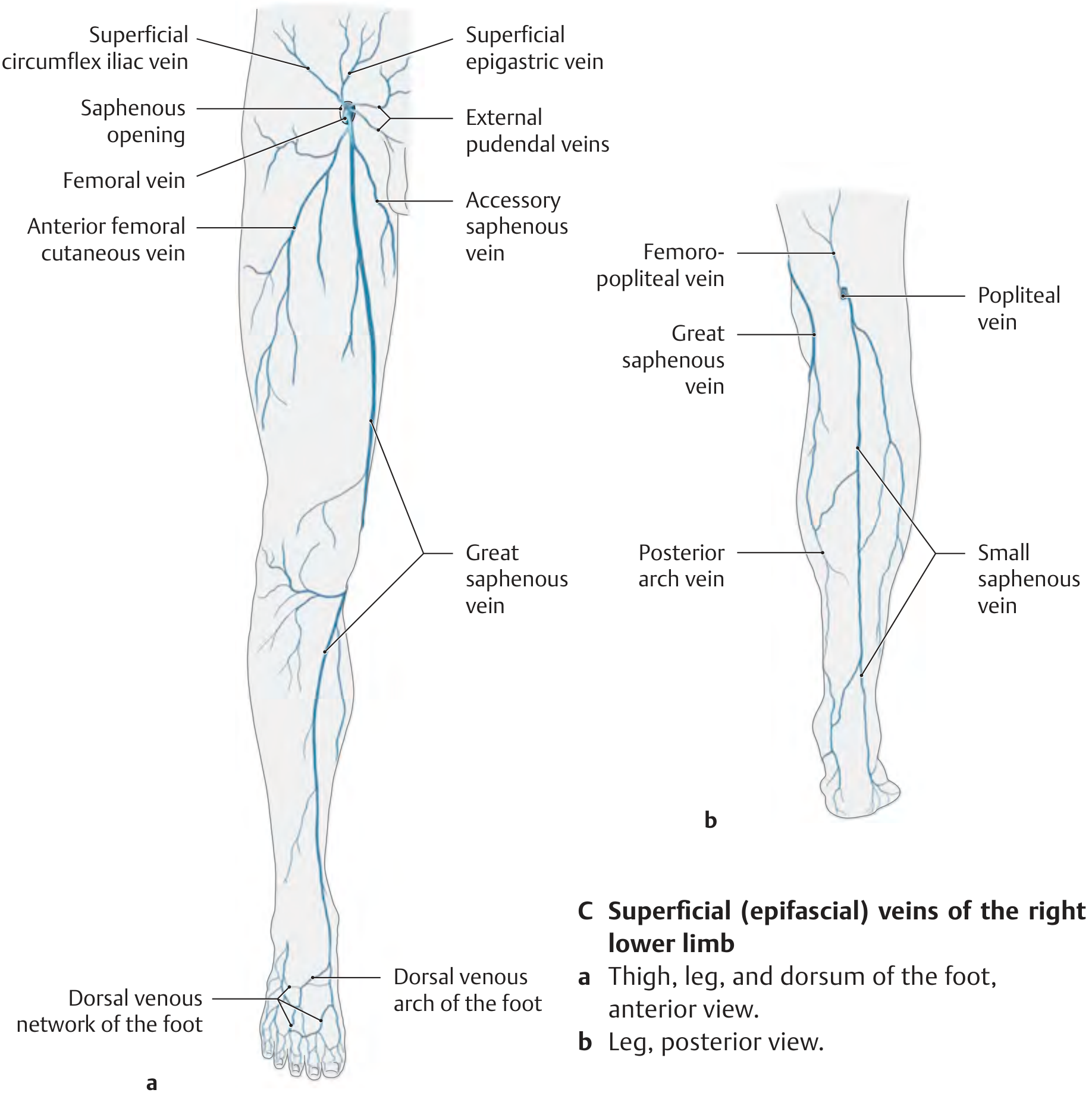
Principal superficial veins:
- Great saphenous vein - longest vein in the body; ascends along the medial thigh and leg; empties into the femoral vein through the saphenous opening
- Accessory saphenous vein
- Posterior arch vein
- Small saphenous vein - ascends along the posterior leg; drains into the popliteal vein
- Femoropopliteal vein
- Dorsal venous network and arch (foot)
- Plantar venous network and arch
- Superficial epigastric, circumflex iliac, and external pudendal veins (at the thigh root)
Perforating (Communicating) Veins
Three clinically important groups connect the deep and superficial systems:
| Group | Location | Connected Veins |
|---|---|---|
| Dodd veins | Medial thigh, middle third (adductor canal level) | Great saphenous ↔ femoral vein |
| Boyd veins | Medial leg, below knee | Great saphenous ↔ posterior tibial veins |
| Cockett veins (I-III) | Medial distal leg (behind medial malleolus) | Posterior arch vein ↔ posterior tibial veins |
Valves in perforating veins normally prevent flow from deep to superficial. Incompetence of these valves causes reversal of flow and varicose disease.
Clinical Box: Varicose Disease of the Superficial Leg Veins
Varicose disease is the most common chronic venous disease, affecting 15% of the adult population.
Classification:
- Spider veins - tiny intradermal varices
- Reticular varices - web-like dilations of small subcutaneous veins
- Great saphenous varicosity - true varicose veins along the great saphenous territory
- Small saphenous varicosity - varicosities along the small saphenous territory
Pathophysiology:
- Primary (idiopathic) varices (75%): Degeneration of the vein wall → incompetence of venous valves → pooling
- Secondary (symptomatic) varices: Chronic occlusion of the deep venous system → incompetence of perforator veins → reversal of flow direction
Acute complications:
- Thrombophlebitis - acute superficial venous system inflammation
- Deep venous thrombosis (DVT) - acute disease of the deep venous system
The Cockett veins are of special clinical importance because the medial distal leg is highly susceptible to venous ulceration when these perforators become incompetent.
Section 4.3 - The Lymphatic Vessels and Lymph Nodes
The lymphatic system of the lower limb mirrors the venous system in organization:
Superficial (epifascial) lymphatic system:
- Collectors follow the course of superficial veins (great and small saphenous)
- Two bundles:
- Anteromedial bundle (runs along great saphenous vein → superficial inguinal lymph nodes) - drains skin and subcutaneous tissue of most of the lower limb
- Posterolateral bundle (runs along small saphenous vein → superficial popliteal lymph nodes) - drains lateral foot and a narrow strip of the calf
Deep (subfascial) lymphatic system:
- Follows the deep veins (popliteal and femoral)
- Drains muscles, joints, and nerves
- Deep popliteal lymph nodes → deep inguinal lymph nodes
Inguinal lymph nodes (the main collecting station):
- Superficial inguinal nodes: arranged horizontally (along the inguinal ligament) and vertically (along the great saphenous vein)
- Deep inguinal nodes: medial to the femoral vein, partly behind the inguinal ligament
Section: Vascular Supply to the Skin (B)
Intact vascular supply is essential for both nutrient delivery to the skin and thermoregulation. All blood vessels lie in the dermis (the epidermis is completely avascular):
Two dermal vascular plexuses:
| Plexus | Location | Function |
|---|---|---|
| Superficial plexus | Border of papillary dermis and reticular dermis | Gives off capillary branches to the papillae and overlying epidermis |
| Deep dermal plexus | Border of dermis and subcutaneous tissue | Larger feeding vessels |
Vertical vessels connect the two plexuses. A dermatome (skin graft device) can cut through the dermis between these two plexuses to harvest a split-thickness skin graft - used to cover large wounds such as burns, since the deep plexus can regenerate the superficial one.
Summary: Key Principles of the Circulatory System
| Concept | Key Points |
|---|---|
| Embryonic origin | Cardiovascular system is first to function; 3 circulatory systems at 3-4 weeks |
| Aortic arch derivatives | 3rd → carotid; 4th left → aortic arch; 6th → pulmonary trunk + ductus arteriosus |
| Venous system development | Cardinal, vitelline, umbilical veins; transverse anastomoses form major adult veins |
| Lower limb arteries | Aorta → common iliac → external iliac → femoral → popliteal → tibial → foot |
| Lower limb veins | Three systems: deep (85%), superficial (15%), perforating (connecting) |
| Key superficial veins | Great saphenous (medial, drains inguinal), Small saphenous (posterior, drains popliteal) |
| Perforating veins | Dodd (thigh), Boyd (proximal leg), Cockett (distal leg - clinical importance) |
| Varicose disease | 15% adult prevalence; primary (valve degeneration) vs secondary (deep venous obstruction) |
| Lymphatic drainage | Parallels venous: anteromedial bundle → inguinal nodes; posterolateral bundle → popliteal nodes |
| Skin vasculature | Two plexuses in dermis; split-thickness grafting uses the plane between them |
Source: THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System (ISBN 9781626237186), Sections 1.6, 2.2, 4.1, 4.2, 4.3
This is a shared conversation. Sign in to Orris to start your own chat.